
Abstract
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited kidney disease in adults. As a social media platform, YouTube has tremendous potential to both support and hinder public health efforts. The aim of this study was to assess the reliability and quality of the most viewed English-language YouTube videos on ADPKD.
Methods
A YouTube search was conducted on 3 August 2023, using the keyword ADPKD disease and the top 200 videos were analyzed for relevance. Videos in the “Short” category that were duplicates, were not in English, were not audio or visual, and contained advertisements were excluded. Two reviewers divided the 159 included videos into groups based on their source and content.
Results
In 106 (66.7%) of the 159 videos, general information about the disease was given, 58 (36.5%) discussed medical treatment, 11 (6.9%) discussed surgical treatment, 30 (18.9%) included patient images and radiological images, and eight (5%) discussed the genetic and pathological features of the disease. Additionally, 16 (10.1%) videos fell into the “other” category. According to the Journal of the American Medical Association, Quality Criteria for Consumer Health Information and Global Quality Scale scoring systems, videos uploaded by health associations and foundations received the highest scores (3 (1–4), 54 (28–70), 4 (1–5), respectively).
Conclusion
Academic institutions and other official health organizations such as Health Associations/Foundations need to use YouTube more effectively to disseminate accurate, reliable and useful health-related information to society.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is a multisystem disorder characterized by multiple bilateral renal cysts and associated cysts in other organs such as the liver, pancreas, and arachnoid membranes. 1 ADPKD is the most common inherited kidney disease in adults. 2 According to the 2022 Turkish Society of Nephrology Registry Report, ADPKD accounts for 3.78% of newly initiated hemodialysis patients and 4.14% of all hemodialysis patients as of 2022. 3 Mutations in PKD1, located on the 16th chromosome, are found in approximately 85% of patients, while mutations in PKD2, located on the fourth chromosome, are found in the remaining 15%. 4 Clinical symptoms typically begin between the ages of 30 and 50, and end-stage kidney disease develops in approximately 50% of patients by the age of 70. 5 Important clinical symptoms of this disease include kidney enlargement, flank pain, hematuria, urinary system and cyst infections, arterial hypertension, nephrolithiasis, and renal insufficiency, which manifest as a result of the disease.
The internet, especially in the last 20 years, has become an increasingly popular tool for obtaining health information. 6 According to the literature, 79% of adults use the internet as a source of health information. 7 YouTube™, originally established as a video-sharing platform in 2005, has been shown to be the most common video-sharing platform and the second most popular website worldwide after Google. 8 While YouTube™ serves as a media channel to promote education and awareness, it may provide inaccurate content and misleading information since it does not undergo an evaluation process and is not regularly updated.9,10 YouTube™ videos have been the subject of research in a variety of medical specialties and for numerous diseases.11–13
The aim of our study is to assess the accuracy adequacy, quality, and reliability of English-language video content related to ADPKD available on YouTube™.
Materials and methods
Videos on YouTube™ (http://www.youtube.com) were searched on 3 August 2023, using the keyword “autosomal dominant polycystic kidney disease.” The videos were sorted in order of relevance on the YouTube™ video list. The first 200 videos in English were reviewed over a 10-day period. The number of videos was limited to 200 because studies have shown that more than 90% of internet consumers tend to review videos in the first few pages of search results. 14 During the YouTube™ search, advertisements, duplicate videos, non-English videos, nonaudio videos, and videos in the “shorts” category were excluded. After these exclusions, a total of 159 videos were included in the study. Our study is a prospective, digital media-based, observational study.
Video characteristics, quality, and reliability analysis
Two independent nephrologists viewed and analyzed the videos. Both nephrologists were unaware of each other's evaluations. The characteristics of the YouTube™ videos were recorded, including the length of each video, the number of views, the number of likes, the number of comments, the duration, and the number of months since upload. Profiles of the upload sources were also recorded.
The videos were categorized based on the sources that uploaded them into six categories: doctors, hospitals, medical websites, health associations or foundations, media channels such as radio/television, and patients (Table 1).
Groups of videos.

Videos were further categorized based on their content into six groups: general information, medical treatment, surgical treatment, patient images/radiological images, genetic/pathological features, and other topics (such as dietary treatment, psychological treatment, pain management, and kidney transplantation) (A video could have multiple types of content, so the ratios and percentages were reported as higher than the total number of videos) (Table 1).
The quality assessment of the videos was conducted using the Journal of the American Medical Association (JAMA) criteria, 15 the DISCERN (Quality Criteria for Consumer Health Information) scale 16 and the Global Quality Scale (GQS). 17
JAMA score
The JAMA scoring system is a well-known quality assessment tool that can be used to evaluate information obtained from health-related websites. It consists of four criteria (authorship, references, copyright, currency), each with a possible score of 1, and the total possible score is 4. A score of four indicates the highest quality. 15
DISCERN scale
The DISCERN scale was developed for patients and information providers to judge the quality of information. It consists of fifteen questions and an overall quality rating. It has three sections that evaluate reliability (section 1), the quality of information on treatment options (section 2), and the overall quality of information (section 3). The first section has eight questions, the second section has seven questions and the third section provides a general rating. Each question is scored on a five-point scale (1–5). If a quality criterion is fully met, it is scored as 5 and if not met at all, it is scored as 1. If a criterion is partially met, it is scored between 2 and 4, depending on the assessors’ judgment. The total DISCERN score is calculated by summing the scores for the first 15 questions. It can be categorized as excellent (63–75), good (51–62), fair (39–50), poor (27–38), and very poor (<27). 16
GQS score
The GQS is a five-point scale (1–5) used to measure the quality, flow, and usefulness of a video. In this scale, four or five points indicate high quality, three points indicate moderate quality, and one or two points indicate low quality. 17
Statistical analysis
For the evaluation of data, the Statistical Package for Social Sciences Version 25.0 program was used for statistical analysis. Categorical data were reported as frequencies (percentages) and counts. Numeric variables that exhibited a normal distribution were presented as mean ± standard deviation, while those that did not follow a normal distribution were presented as median (minimum–maximum). The distribution characteristics of numeric variables were assessed using the Kolmogorov–Smirnov or Shapiro–Wilk tests. Given that there were more than two groups to be compared, and the numeric variables did not follow a normal distribution, the Kruskal–Wallis test was used to compare the groups. The Bonferroni “post hoc” correction method was employed for pairwise comparisons. Spearman's test was conducted for correlation analysis. Interrater agreement was assessed using the kappa coefficient. The level of statistical significance was set at p < .05, and findings were also interpreted as p < .01 and p < .001 when appropriate.
Ethical approval
Publicly available YouTube™ videos were analyzed, and there was no involvement of human participants or animals in the study; therefore, ethical approval was not required, as is the case in other similar YouTube™ research studies.
Results
A total of 159 videos were analyzed. Video characteristics are summarized in Table 2. Out of these, 106 (66.7%) videos provided general information about the disease, 58 (36.5%) discussed medical treatment, 11 (6.9%) discussed surgical treatment, 30 (18.9%) included patient images and radiological images, and 8 (5%) discussed the genetic and pathological features of the disease. Additionally, 16 (10.1%) videos fell under the “other” category. The majority of videos (n = 59, 37.1%) were uploaded by medical websites (Figure 1).

Videos by upload source.
General features of videos.

*DISCERN: Quality Criteria for Consumer Health Information; JAMA: Journal of the American Medical Association, GQS: Global Quality Scale.
When comparing video durations based on their sources, a statistically significant difference was observed among the groups (p = .017). Pairwise group comparisons revealed that this difference stemmed from the Hospital and Associations/Foundations (p = .033), Medical Website and Associations/Foundations (p = .021) groups. Videos uploaded by Associations/Foundations had the longest median duration at 46 min (range: 2–72 min).
Objective evaluation of video content
When comparing video quality scores using JAMA, GQS, and DISCERN scores, Cohen's kappa coefficients were 0.883, 0.887, and 0.885, respectively. Significantly higher scores were obtained by videos uploaded by Associations/Foundations when assessed according to their sources (p < .001) (JAMA median score: 3 (1–4), DISCERN median score: 54 (28–70), GQS median score: 4 (1–5)) (Figure 2).

Distribution of video quality scores to video sources. (a): JAMA Score. JAMA: Journal of the American Medical Association. (b): DISCERN Score. DISCERN: Quality Criteria for Consumer Health Information. (c): GQS Score. GQS: Global Quality Scale.
In terms of JAMA scores, there was a statistically significant difference among groups when comparing video sources (p < .001). Pairwise group comparisons revealed that this difference originated from the media channels and hospitals (p = .008), media channels and associations/foundations (p < .001), medical websites and hospitals (p < .001), medical websites and associations/foundations (p < .001), and doctors and hospitals (p < .001) groups.
Regarding DISCERN scores, there was a statistically significant difference between groups when comparing video sources (p < .001). In pairwise group comparisons, this difference was found between doctors and hospitals in favor of the hospitals (p = .013), between doctors and association/foundations in favor of the associations/foundations (p < .001), between media channels and associations/foundations in favor of the associations/foundations (p = .001), and between medical websites and associations/foundations in favor of the associations/foundations (p < .001) and between the hospitals and the associations/foundations in favor of the associations/foundations (p = .032).
Regarding GQS scores, there was a statistically significant difference between groups when comparing video sources (p < .001). In pairwise group comparisons, this difference was found to be in favor of the associations/foundations between the media channels and the associations/foundations (p = .001), in favor of the associations/foundations between the doctors and the associations/foundations (p < .001), in favor of the associations/foundations between the medical websites and the associations/foundations (p < .001) and in favor of the associations/foundations between the hospitals and the associations/foundations (p = .025).
The DISCERN score was examined separately for its three parts, and the groups were compared in this respect according to their sources. Results by DISCERN score sections are given in Table 3. A statistically significant difference was found between video sources in terms of DISCERN reliability (p < .001). In pairwise group comparisons, this difference was found to be between the media channels and the medical websites in favor of the medical websites (p = .024), between the media channels and the associations/foundations in favor of the associations/foundations (p < .001), between the doctors and the associations/foundations in favor of the associations/foundations (p < .001), and between the medical websites and the associations/foundations in favor of the associations/foundations (p < .001) and between the hospitals and the associations/foundations was found to be in favor of the associations/foundations (p = .039). A statistically significant difference was found between video sources in terms of DISCERN treatment (p < .001). In pairwise group comparisons, it was determined that this difference was in favor of the hospitals between doctors and hospitals (p = .014), in favor of the associations/foundations between doctors and associations/foundations (p < .001), and in favor of the associations/foundations between medical websites and associations/foundations (p = .001).
Comparison of parts of the DISCERN score according to video sources.

Kruskal Wallis. The results of the pairwise group comparison are given in the text.
DISCERN: Quality Criteria for Consumer Health Information.
A statistically significant difference was found between video sources for DISCERN quality (p < .001). In pairwise group comparisons, it was determined that this difference was in favor of the hospitals between the doctors and the hospitals (p = .023), in favor of the associations/foundations between the doctors and the associations/foundations (p < .001), and in favor of the associations/foundations between the medical websites and the associations/foundations (p = .002). Videos from associations/foundations had significantly higher DISCERN median reliability scores: 26, treatment scores: 20, and quality scores: 3 compared to other video sources.
When examining the correlation between JAMA, GQS, and DISCERN scores: A very strong correlation was found between DISCERN total score and GQS score (r2 0.827, (0.71–0.99 very strong correlation), p < .001), a good correlation was found between DISCERN total score and JAMA score (r2 0.686, (0.30–0.70 good correlation), p < .001), a good correlation was found between GQS score and JAMA score (r2 0.700, (0.30–0.70 good correlation), p < .001).
Regarding numerical variables related to video characteristics, such as video duration, view count, comment count, and like count, and their correlation with JAMA, DISCERN, and GQS scores: There was a correlation between video duration and JAMA, DISCERN, and GQS scores, while no correlation was found between other video characteristics (Table 4). These findings suggest that video quality scores are correlated with each other and that video duration is a factor that correlates with these quality scores.
Correlation analyses between JAMA, DISCERN and GQS scores and video features.
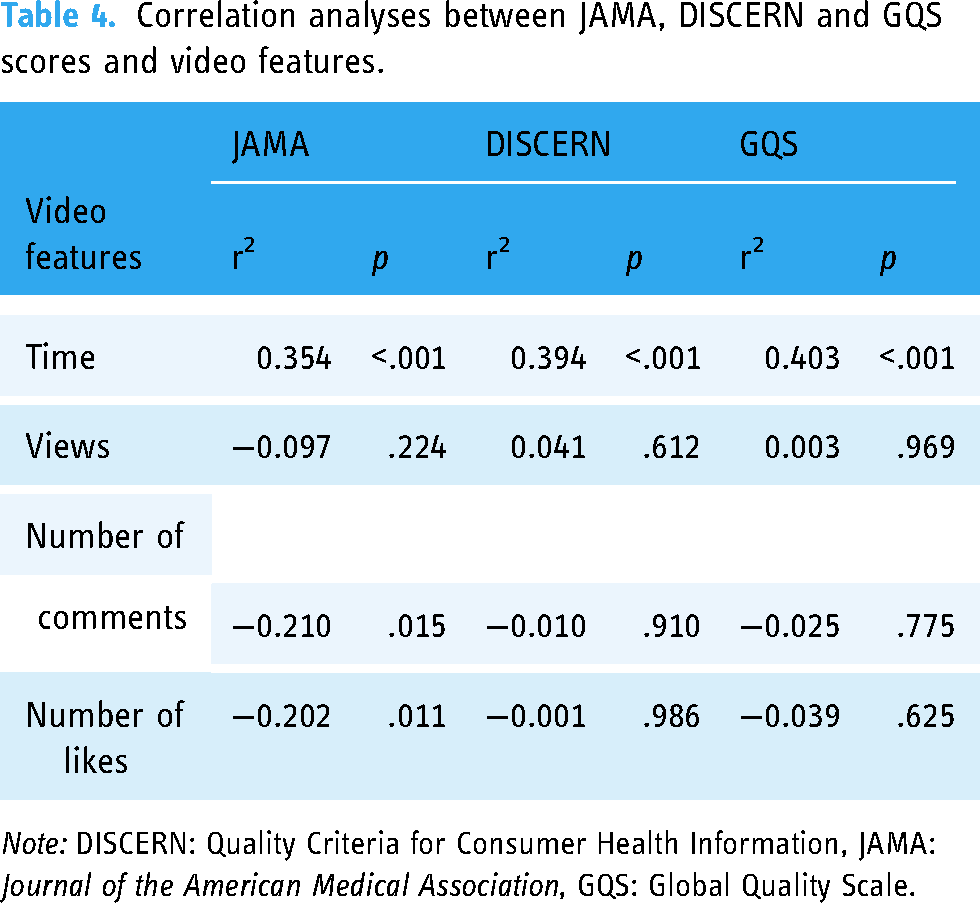
Note: DISCERN: Quality Criteria for Consumer Health Information, JAMA: Journal of the American Medical Association, GQS: Global Quality Scale.
Discussion
The internet significantly contributes to how people communicate and obtain information. It has been reported that people often turn to the Internet as their primary source of health information before seeking advice from a doctor. 18 When we looked at health literacy online in a study conducted in various countries in Europe in 2020; almost 60% of those who had used the Internet during the 12 months reported using it to search for health information. There was however considerable cross-country variation, with the highest use being observed in the Netherlands (73%), Sweden (70%), and Denmark (70%), and the lowest in Malta (49%) and Romania (47%). 19
YouTube™, as an online video-sharing platform, offers the significant advantage of being readily accessible at any time. While YouTube™ provides free content, its lack of an evaluation process for accuracy and currency means that it can also present inaccurate information. 20 Therefore, individuals should pay closer attention to videos shared through official and academic channels.
YouTube™ was first used as a data source in research by Keelan et al. in 2007 in their study on vaccination. 21 Regarding ADPKD, the first YouTube™ study was published by Lambert et al. in May 2023. 22 Our study represents the first comprehensive investigation utilizing YouTube™ as a data source for ADPKD.
ADPKD is the most common hereditary kidney disorder and a frequent cause of end-stage kidney disease. Enlarging kidney cysts and accompanying hypertension, liver cysts, intracranial aneurysms, and extrarenal manifestations such as heart valve disease, demonstrate the systemic nature of the disease. 2 Treatment of the disease involves supportive measures such as dietary adjustments to regulate salt and protein intake, excessive fluid intake, hypertension management, and control of kidney stones. However, the final stages of the disease may require dialysis and transplantation. 23
In the literature, the scoring systems most commonly used in the video evaluation process are primarily DISCERN, JAMA, and GQS systems. In our study, we also utilized these scoring systems. The median DISCERN, JAMA, and GQS scores for the videos were 35 (poor quality), 1 (poor quality), and 2 (poor quality), respectively. These results indicate that YouTube™ videos about ADPKD are generally of low quality. When quality scores were examined separately according to video sources, videos uploaded by health associations/foundations received significantly higher scores than other video sources (p < .001) (JAMA median score: 3 (1–4), DISCERN median score: 54 (28–70), GQS median score: 4 (1–5)). Additionally, it was observed that videos from health associations/foundations had significantly longer durations than the other video sources. A positive correlation was found between video duration and JAMA, DISCERN, and GQS scores. It should be noted that, especially as video duration increases, video quality increases, but viewer interest and viewing rate may decrease. When examining the correlation between scoring systems, it was found that there is a very strong correlation between the DISCERN total score and the GQS score (r2 0.827) a good correlation between the DISCERN total score and the JAMA score (r2 0.686), and a good correlation between the GQS score and the JAMA score (r2 0.700). This suggests that scoring systems can be used interchangeably.
When the sources of video uploads are examined, it is observed that the majority (n: 59, 37.1%) of the videos are uploaded by medical websites. In another YouTube™ study that evaluated the association/foundations between COVID-19 and dialysis, universities, health associations, and government institutions were the primary sources of video content (n: 14, 40%). 11 In another YouTube™ study evaluating Anakinra injections, the majority of videos (n: 29, 56.9%) were uploaded by physicians. 24 It is noteworthy in our study that there is a scarcity of patient-generated videos (n: 2, 1.3%). This situation can be attributed to the low level of patient knowledge and awareness about the disease, as mentioned in a study by Doğan et al. 25
Videos uploaded by reliable sources such as health associations/foundations often contain useful and high-quality information about diseases. Videos uploaded from various sources can sometimes contain incorrect information. 26 Patients should be encouraged to carefully review the information sources on YouTube™. The nephrology community should be vigilant about incorrect information about ADPKD that patients may be exposed to on YouTube™. Physicians should correct any misinformation during their discussions with patients. Nephrology associations/foundations and communities can collaborate with social media channels to evaluate video content uploaded about ADPKD and other relevant diseases, thereby providing more accurate information to the public. They can also take the initiative to remove videos containing misleading information on social media platforms. Politicians and government officials may plan to establish fact-checking centers that check the quality and reliability of YouTube videos.
Limitations
Our study has several limitations. Subjectivity and observer-dependent nature of the scoring methods used in video quality assessment, relatively small sample size and exclusion of non-English videos are the most obvious limitations of our study. Using the full name of the disease, “autosomal dominant polycystic kidney disease” instead of the term “polycystic kidney disease” as the search term, may have caused us to evaluate some relevant videos. Also sorting and cross-sectionally examining videos according to relevance may result in not encompassing all videos on YouTube™ which is a dynamic platform. Additionally, the absence of information about the demographic characteristics of the viewers and the impact of these videos on their lives stands out as another limitation.
Conclusion
Health associations/foundations, academic institutions, and other official health organizations, especially health associations/foundations, should consider using YouTube™ to deliver accurate, reliable, and useful health-related information to the public. Currently, social media content intended to alleviate people's health concerns should also be closely monitored for misleading information.
Footnotes
Acknowledgments
I would like to thank my brother Alper Selen for providing technical support in the writing of this article.
Contributorship
concept or design: TS and OM; acquisition of data: TS; analysis or interpretation of data: OM and TS; drafting of the article: TS and OM; critical revision for important intellectual content: OM and TS. All authors had full access to the data, contributed to the study, approved the final version for publication, and took responsibility for its accuracy and integrity.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
We confirm that such approval is not needed as we did not conduct research on human subjects. Informed consent was not necessary for all of the analysis data to be publicly available from the website. User agreement of video platforms was obtained by video platforms before users uploaded the video.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
T.S.