
Abstract
Objective
In this article, we investigate how chronic noncommunicable disease (CND) patients evaluate the medical service, and what obstacles exist in this process, which is useful for hospitals to improve efficiency and enhance patient satisfaction.
Methods
Based on the total number of CND patients in China, 7 CNDs were selected as the evaluation objects, and then selected the Haodaifu website as the data source, crawled 15,682 medical service reviews, then the 9 themes were analyzed by the LDA theme model. The evaluation index system of six indicators was constructed based on quality management theory. The binary long short-term memory model was used to analyze the sentiment, and the entropy-valued, TOPSIS and gray correlation model was implemented for medical service quality evaluation; the barrier model was used to find out the key factors limiting medical services.
Results
(a) Hypertension was rated at a good level in the degree of gray correlation closeness, bronchitis was rated at a low level and the rest were at an intermediate level. (b) The first two overall barriers were the hospitalization process and registration services which occupy about 30%, respectively. This implies that hospitals should focus on providing registration services and inpatient settings in the future.
Conclusion
To promote hospitals to provide better services for patients with CNDs and improve patient satisfaction with medical care. And it is necessary to optimize medical services fundamentally by optimizing the inpatient process and improving the registration process to improve efficiency.
Keywords
Introduction
Since the reform and opening up in 1978, China's population has experienced a remarkable shift in health and disease patterns, with chronic noncommunicable diseases (CNDs) such as cardiovascular diseases, malignant tumors, chronic respiratory diseases, diabetes and mental illnesses replacing infectious diseases as the leading causes of death and disability in the population. The situation of CNDs prevention and control is becoming increasingly serious. A distinctive feature of CNDs is that their incidence increases significantly with age, 1 and the rapid aging of the population has led to a dramatic increase in the number of people vulnerable to CNDs. China has experienced rapid demographic shifts and rapid economic development over the past three decades, and the current serious aging problem in China has led to a rapid health shift in the population and a large increase in the number of patients with CNDs. According to the China Health and Wellness Statistical Yearbook in 2019, the number of diabetes discharges from public hospitals in China reached 2,241,100, hypertension discharges reached 1,334,400 and cerebrovascular disease discharges reached 6,539,500. In 2020, for the first time, the number of discharges from public hospitals in China for all types of CNDs declined due to the COVID-19 epidemic, with 2,196,600 discharges for diabetes, 1,106,500 discharges for hypertension and 5,925,600 discharges for cerebrovascular disease in 2020. Yet it is not just in China; the incidence of CNDs is a major global public health challenge. In the United States, approximately 60% of adults meeting the criteria for multiple morbidities have increased significantly over the past three decades. 2 Half of Canadian adults have at least one CNDs and a quarter have multiple diseases. 3 CNDs have become a global problem today.
In terms of assessing the quality of medical services, it is easy to see that the doctor–patient relationship has become a red-hot social concern, based on the reports in recent years.4–6 The main cause of doctor–patient problems is patients’ dissatisfaction with hospital treatment services, which can have negative effects on physicians. 7
Although existing research has proposed hospital service satisfaction surveys, 8 it only considers patients’ final feelings about the services they received, which means they ignore the patient's feelings about the whole process. Most hospitals only pay attention to the final effect of medical treatment, but ignore the satisfaction of the whole medical service process, resulting in the satisfaction survey obtained by the hospital deviates from the expectations of the public.9,10 Thus, it becomes imperative to conduct a comprehensive assessment of the entire medical service process's quality. Analyzing the assessment results helps identify problematic aspects of the medical service process, offering a microscopic perspective to enhance patient satisfaction.
Second, patients with CNDs and their families experience many different kinds of stress during their illness and treatment.11,12 Patients endure discomfort for years to survive, and treatment for most CNDs is lifelong, requiring frequent visits to hospitals for treatment in addition to the financial cost pressures incurred. 13 Therefore, whether the hospital improves good medical care in the process can have a great impact on patients with CNDs. It is essential to have a proper understanding of the services provided by hospitals for patients with CNDs and to optimize the management of hospitals.
Third, with the advancement of technology and the progress of the era, traditional methods of conducting healthcare service surveys have become inadequate in meeting the diverse research needs of various sectors, including the broader society, research institutions, decision-makers and scholars. This indicates the necessity for updating and refining research methodologies to gain a more comprehensive and in-depth understanding of all aspects of healthcare services. This adjustment is essential to align with the current societal expectations and demands for increasingly complex and diversified healthcare services. The advent of online medical service evaluations has empowered patients to assess and share their treatment experiences through the internet, addressing various medical challenges. This digital platform serves as a valuable resource by providing users with essential medical information, thereby alleviating the dilemma of limited access to healthcare-related knowledge. Patients’ evaluations contribute to the identification and enhancement of areas lacking in the quality of care, fostering transparency in healthcare service and addressing concerns related to the lack of openness and clarity in medical practices. Additionally, online assessments empower individuals, allowing them to actively participate in their healthcare decisions, ultimately promoting patient satisfaction and advancing the overall development of medical care.
Due to the nature of healthcare service quality, the questionnaire approach makes it difficult for patients to evaluate the quality of healthcare services accurately and reasonably, and there are limitations in evaluating patient satisfaction alone. Therefore, it is necessary to use text mining and sentiment analysis methods to identify service quality issues from text comments affecting patients, in that, this can give us a more comprehensive understanding of patient's needs in terms of service quality. The study is therefore data-driven and exploratory.
To close these knowledge gaps, this study examined two research questions: (a) What is the satisfaction of patients with chronic diseases in health care delivery? (b) What are the constraints in the process of healthcare delivery for different chronic diseases?
We focused on seven prevalent chronic diseases in China to address the following questions, considering the substantial number of patients affected by these conditions. To determine the concerns of patients, we employed the Latent Dirichlet Allocation (LDA) topic classification method. Subsequently, sentiment analysis was conducted using the binary long short-term memory (BiLSTM) model to analyze the gathered data. To assess the quality of healthcare, we combined the TOPSIS and gray correlations methodologies. Additionally, we calculated barrier factors for each indicator to comprehensively evaluate the quality of healthcare services for chronic diseases.
The study's key innovations and contributions are as follows:
Targeted evaluation: Recognizing the variations in access to care processes and experiences across different disease types, we tailored the evaluation of medical services for chronic diseases accordingly. This approach enhances the specificity and relevance of the evaluation content, aiding hospitals in delivering improved services for patients with chronic conditions. Theoretical model and index selection: Our study builds upon the “structure–process–outcome” theoretical model,
14
which is pre-established, and leverages the results of LDA thematic analysis for classification. This framework ensures a comprehensive assessment of healthcare services for chronic diseases. Improved sentiment analysis: Existing sentiment analysis techniques primarily focus on e-commerce platforms, potentially leading to inaccurate results when applied to health websites. In our study, we propose a sentiment analysis approach using the BiLSTM model, incorporating a manually selected supervised learning model to enhance accuracy.
By uncovering the attitudes of chronically ill patients toward healthcare, this study surpasses previous research, contributing to a more comprehensive understanding of the quality of healthcare services provided to this population.
Literature review
Our work is closely related to the flow of literature on online reviews, topic analysis, service quality and quality models.
Online review and topic modeling
Online reviews have important implications in the medical field. Firstly, they provide a platform for patients to share their medical experiences and opinions so that other patients can benefit from the experiences of others. This helps build a community where patients can exchange information about doctors, hospitals and treatments. Secondly, healthcare-related online reviews guide patients in choosing a healthcare provider. By learning about the satisfaction and dissatisfaction of other patients, patients can more wisely choose a doctor or healthcare provider that suits their needs. In addition, these reviews provide a feedback channel for healthcare practitioners to know how patients feel and feel about their services. This helps healthcare organizations and practitioners to improve the quality of their services and increase patient satisfaction.
For topic analysis, most studies on social media topic evolution are based on parametric topic models, which are mainly developed by LDA. 15 Gao Huiying addresses the problems of semantic sparsity and insufficient co-occurrence information in LDA topic models for medical review topic mining and proposes a CO-LDA model based on the combination of word co-occurrence analysis and LDA topic models. 16 Gonzalez used LDA probabilistic topic modeling to understand the importance and reproducibility of women's urinary tract infection experiences. 17 Shah, AM's text mining approach based on a combination of SentiNet and LDA uncovered potential topics in high- and low-risk disease categories, revealing new insights into what patients value and what they dislike when consulting their physicians. 18
Although there have been research studies on online reviews in the health domain for topic analysis and satisfaction, for example, Zhai and Yunkai used text mining for index extraction and satisfaction analysis of online reviews to quantitatively assess user satisfaction with mHealth applications, confirming that users are satisfied with the quality of service and content of mHealth applications and less satisfied with the quality of management and technology. 19 Jia used machine learning for topic modeling and opinion mining of user-generated content from postnatal care centers on the Internet. 20
However, patients with chronic illnesses who require frequent medical care lack access to quality care in this area. Our research begins with patients with chronic conditions because they differ from other diseases. Based on the vast number of patients with chronic diseases, the long disease cycle and the characteristics of not easy to cure, hospitals must optimize the medical process to improve the efficiency of services to treat chronic patients better.
Service quality
The Medical Quality Management Measures (2016) issued by the Chinese Health and Family Planning Commission defines medical quality as the extent to which medical institutions and their medical personnel, in the course of clinical treatment, provide medical care to patients by strictly implementing the requirements of professional ethics as well as treatment norms, given the current level of medical technology, capabilities and conditions. 21
The widely used model for measuring healthcare quality is the three-step framework, structure–process–outcome, proposed by Donabedian. 14 This model suggests that healthcare quality encompasses the combination of structure, process and outcome, aiming to provide patients with the most suitable healthcare with minimal risks and costs, thus achieving the best possible state of health. Various scholars have explored specific evaluation models for service quality, such as data envelopment analysis (DEA) analysis method 22 ; KANO model 23 ; SERVQUAL model 22 and SERVVPERF model. 24
In the realm of online reviews and service quality, Chen analyzed the impact of perceived service quality and disconfirmation on patients’ emotional responses and reviewed efforts through online reviews. 25 Kim used online reviews for LDA topic modeling to derive determinants of hotel service quality based on Korean hotel rating. 26 Xiao studied text reviews of luxury hotels using latent semantic analysis and Kano modeling to understand customers’ concerns and expectations regarding service attributes, effectively applying quality engineering diagnostic techniques to online review analysis. 27 Bai proposed a hotel service quality measurement model based on sentiment analysis of online reviews and a multi-attribute approach. 28 However, these existing studies focus more on hotels rather than healthcare service evaluations, highlighting a significant gap in combining online reviews and healthcare quality assessments.
Building upon the results of previous studies, it is crucial to assess the quality of healthcare services provided during medical visits. However, to the best of our knowledge, there is a lack of studies that specifically examine the quality and challenges associated with accessing care for patients with chronic diseases. Therefore, our research aims to fill this gap by identifying the barriers encountered by patients with chronic conditions when seeking medical care. Furthermore, we strive to conduct a preliminary analysis of how hospitals can enhance their services for this particular group of patients. By addressing these aspects, we aim to contribute valuable insights to the field and promote improvements in healthcare delivery for individuals with chronic diseases.
Based on the findings of these studies, it is essential to measure the quality of healthcare services during medical visits. However, to our knowledge, no studies have specifically considered the quality and challenges related to access to care for patients with chronic diseases. Our research endeavors to identify barriers that patients with chronic conditions face when seeking medical care and provide a preliminary analysis of how hospitals can improve services for this patient population.
Materials and methods
This section describes the framework of data collection methods, data cleaning/pre-processing, text mining analysis methods and quality evaluation. The schematic framework (Figure 1) shows the methodological structure of this study.

A schematic framework of text data analysis method.
Figure 1 illustrates the three phases involved in the study. In the first phase, data acquisition was carried out by selecting the Haodaifu website as the data source. The information was collected using the Octopus Collector and Python. In the second phase, the test data obtained in the first phase underwent pre-processing to prepare it for the final analysis. The third phase focused on data analysis. Initially, the LDA model was utilized to determine the number of topics present in the text data. Subsequently, the BiLSTM model was employed for sentiment analysis, generating sentiment values ranging from 1 to 0. Once the numerical data was obtained, each indicator was calculated to evaluate the quality. An unquantified matrix was constructed, followed by obtaining the Euclidean distance and gray correlation. These two sets of data were then combined to derive the gray correlation evaluation. Finally, obstacle factor analysis was conducted based on the obtained data.
Data collection and pre-processing
Research context
The data for our study was sourced from the Haodaifu website (www.haodf.com), which was established in 2006 and is one of China's leading internet medical platforms. The website boasts over 10,000 registered and certified hospitals, 820,000 doctors and 230,000 public hospital doctors. Haodaifu provides a range of services, allowing doctors to operate their “online clinics” for remote consultations, while patients can seek specialist advice from the comfort of their homes. The platform also offers features such as online prescriptions, online pharmacies, medicine delivery and the ability to access doctors’ outpatient information online.
Additionally, the Haodaifu platform facilitates finding doctors based on hospitals and specific diseases. Users can search for relevant conditions on the website, which will automatically recommend specialists. Filtering options are available based on geographical region, speciality and the doctor's professional level. The platform provides comprehensive doctor information, including profiles, ratings and patient reviews. The reviews are publicly available and include details regarding the type of disease, subjective satisfaction with the treatment and attitude, as well as a comprehensive description of the condition, treatment process and recovery progress.
Given its status as one of China's leading Internet medical platforms, Haodaifu possesses an extensive pool of doctors and patient resources. The reviews on the platform are considered highly reliable. To maintain authenticity, the platform requires patients to register using their real names and submit proof of their visit, such as registration slips, medical records and examination sheets. Patients are also required to agree to the Terms of Publication, ensuring the accuracy of the published content and assuming responsibility for their comments. Furthermore, Haodaifu conducts manual reviews for each evaluation submitted.
Moreover, Haodaifu employs technical mechanisms to monitor assessments in real-time. Any abnormalities, such as an excessive number of positive reviews for a particular doctor or a large volume of evaluations originating from the same device or IP address within a short timeframe, trigger a “warning” queue. In such cases, the platform conducts a more stringent manual review of all evaluations associated with the doctor. Instances of “cheating” are severely penalized, and in serious cases, all reviews may be cleared, or even services may be suspended. If the platform receives feedback from patients suggesting that they were coerced or influenced to provide reviews, a manual review of all doctor reviews is immediately initiated to ensure that patients submit appraisals knowingly and willingly. These measures guarantee that the reviews are unbiased and provide reliable data for our study. The reviews are substantive, can be categorized according to diseases, and meet the data requirements for our research.
The population suffering from chronic diseases in China is very large. According to the 2021 China Cardiovascular Health and Disease Report, the number of people with hypertension is about 245 million. Next, the number of people with diabetes increased from 90 million to 140 million, an increase of 56%, of which about 72.83 million, or 51.7%, are undiagnosed. According to the World Health Organization, the prevalence of gastric disease in the population is as high as 80%. There are 120 million patients with gastrointestinal diseases in China, and the prevalence of chronic gastritis is about 30%. The number of patients with chronic bronchitis is 10–20 million, including 7 million children. Secondly, according to the World Health Organization (WHO), the anemia rate among Chinese residents aged 6 years and above is 9.7%, with 5.0% and 17.2% among children aged 6–11 years and pregnant women, respectively. Finally, the China Rheumatoid Arthritis Development Report 2020. The report shows that according to preliminary estimates, there are about 5 million patients with rheumatoid arthritis in China, with an average age of onset of only 45 years. The average age of onset of Ginseng disease is 60 years old, and the number of patients has exceeded 3 million. In addition to tumors and cardiovascular diseases, Parkinson's disease has become a common disease among middle-aged and elderly people. From this, we can see that hypertension in cardiovascular diseases, chronic bronchitis in respiratory diseases, chronic diseases in differential diseases, Parkinson's disease in neurological CNDs, diabetes in endocrine diseases, rheumatoid arthritis in rheumatic diseases and personality anemia in mathematics have a large patient base. Therefore, these seven diseases were selected for investigation.
Data collection
We use Octopus Collector to collect reviews from the Haodaifu website. First, we search for the relevant disease and then recommend the relevant specialist according to the disease, and then click on the specialist's homepage to collect the reviews given by the patients seen by the specialist. However, the number of reviews for each disease varies greatly depending on the patient base, so the number of reviews also varies. We have collected as many reviews as possible, with a total of 16,372 reviews.
The collected data were then pre-processed, firstly by de-duplication and removing comments with a length of less than six Chinese characters. After that, we used the Jieba word splitting database to split the words and then combined it with the Harbin deactivation thesaurus to remove meaningless stop words, expressions, punctuation and numbers, followed by white space removal. The last step is to conclude words with similar meanings in the thesaurus, to complete the semantic deduplication and integration. After the above data preprocessing, noise data interfering with service quality evaluation is reduced.
Text mining approaches
Establishing LDA topic model
This study uses LDA to extract latent themes from review text data and define themes as quality evaluation dimensions. LDA is an unsupervised machine learning technique that can be used to identify latent topic information in large document collections or corpus. It uses the bag of words approach, which treats each document as a vector of word frequencies and thus transforms textual information into numerical information that can be easily modeled. This model was first proposed by BLEI et al. in 2003,
29
and the concept and idea of the LDA model. It is a three-layer Bayesian probabilistic model containing words, topics and documents, and the process of document generation is shown in Figure 2.
Step 1: In the Dirichlet distribution α, sample the topic distribution θd of document d. Step 2: In the topic distribution θd, sample to obtain the nth topic zdn of document d. Step 3: In the Dirichlet distribution β, sample the word distribution ∅k of topic k. Step 4: From the word distribution ∅k, sample the word wdn.
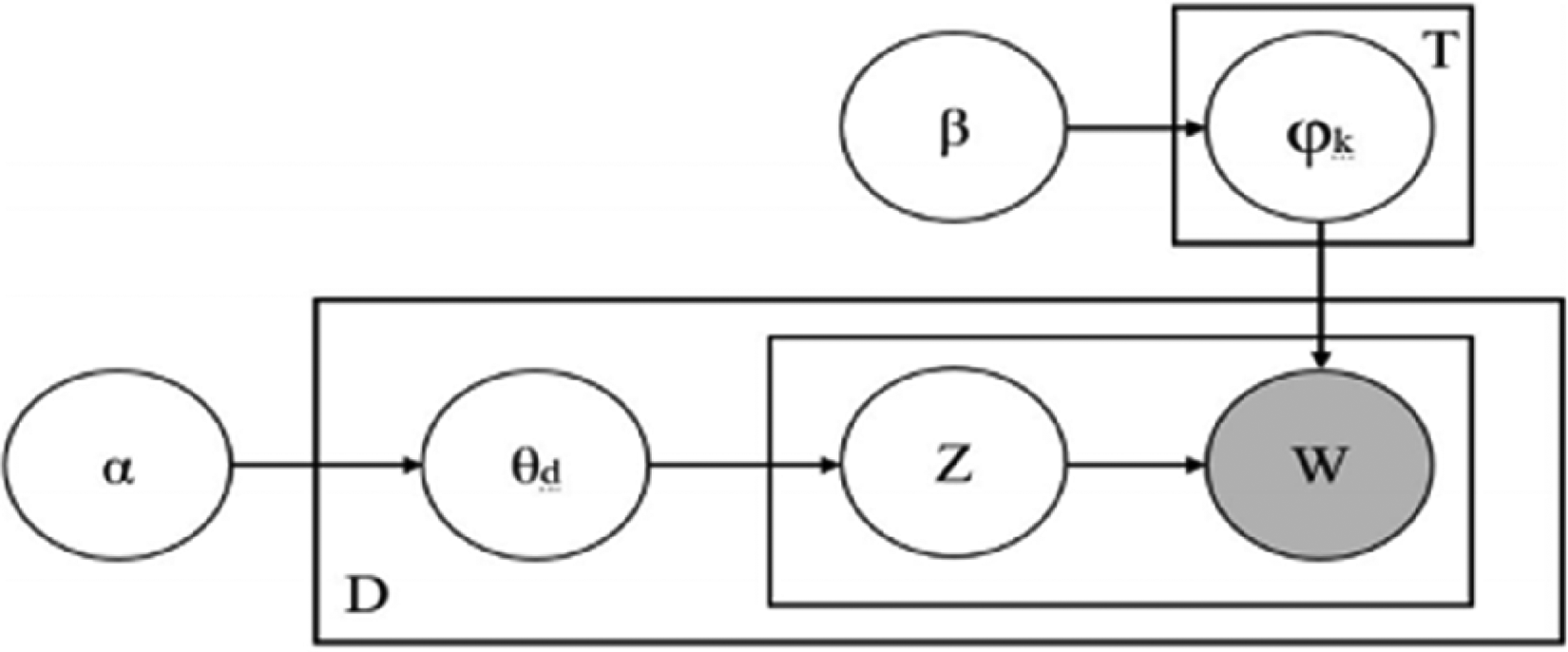
LDA model generation process.
The hyperparameters α and β are set as symmetric Dirichlet priors with values of 50/T and 0.01, respectively. The number of iterations for Gibbs sampling is 100, and the document contribution threshold ε is set to 1/k.
BiLSTM sentiment analysis
For text review sentiment analysis, it is common practice to classify review texts into positively inclined sentiment reviews neutral sentiment reviews, and negatively inclined sentiment reviews to determine the sentiment direction of the review. Text sentiment analysis is divided according to text granularity into three levels of study: chapter level, sentence level and phrase level. Through the length statistics in medical evaluation, it is found that user reviews are short, so this article chooses to mine the sentiment tendency of review texts from the sentence level. At present, text sentiment analysis is mainly divided into sentiment analysis based on sentiment lexicon, sentiment analysis based on machine learning, and sentiment analysis based on deep learning. Since the sentiment analysis in sentiment dictionaries is built based on e-commerce reviews, there will be a large error for sentiment analysis of medical service reviews with dictionaries. After comprehensive consideration, this article selects deep learning, which is the BiLSTM model to Classify sentiment.
BiLSTM is a two-way recurrent neural network that takes all words of a whole sentence as input and takes into account the contextual information of the text so that the information is transmitted in both forward and backward directions.30,31
As shown in Figure 3, BiLSTM is a combination of forward LSTM and backward LSTM. As shown in Figure 4, the LSTM model consists of the input character Xt at time t, the cell state Ct, the temporary cell state Ct, the hidden layer state ht, the forget gate ft, the memory gate it and the output gate ot. It delivers useful information for subsequent computations by discarding useless information and memorizing new information. The calculation process is divided into the next four steps:
Calculate the forget gate and select the information to be forgotten: Calculate the memory gate and temporary unit state: Calculate the current cell state: Calculate the current state of the output gate and hidden layer:







BiLSTM network structure.

Internal structure of LSTM.
In the formula: W and b are the weights and biases in neurons, respectively; the subscripts f, i and c are the forget gate, input gate and output gate, respectively; * represents the scalar product of two vectors.
There are two types of emotions: positive and negative. Emotion scores were categorized as 0 and 1, where 0 indicates negative and 1 indicates positive. We counted the emotion scores of patient reviews on each perceptual dimension; finally, the average scores of positive and negative emotions were calculated as the final emotion score of the index.
Quality evaluation
At present, the commonly used methods for evaluating the quality of medical services include TOPSIS, SERVQUAL service quality model, principal component analysis (PCA), fuzzy comprehensive evaluation (FCE), entropy weighting (EW), gray correlation analysis (GRA), hierarchical analysis (AHP), etc.32–38 Among them, TOPSIS (Technique for Order Preference by Similarity to Ideal Solution) method is a multi-objective decision analysis method proposed by Hwang and Yoon to obtain the optimal solution by approximating the ideal solution. The principle is that the weighted normalization matrix is constructed based on the weighted normalization process of the original data to form the normalization matrix. The maximum and minimum values of each index are used to find out the positive and negative ideal solutions of the evaluation object, and the optimal value of each evaluation index is the positive ideal solution, and the worst value is the negative ideal solution. Then calculate the distance of each evaluation index to the positive and negative ideal solutions, and find out their closeness to the positive ideal solution. Then the evaluation objects are ranked by their closeness to the optimal solution. The solution that is closest to the positive ideal solution and farthest from the negative ideal solution is the optimal solution, while the opposite is the worst solution, thus helping us to make the best choice. The degree of correlation is to describe the degree of correlation between different factors, and the degree of correlation between different objects is often different. It only reflects the distance relationship between the positions of the data curves. Gray relation analysis (GRA) is a method to describe the degree of correlation. The main idea is to construct geometric shapes for the selected reference series and the compared series and to explain their correlation degree by comparing the similarity of the shapes, essentially analyzing the correlation degree of the curves. The gray correlation analysis model has the following characteristics: the gray correlation analysis method is simple to operate, the quality of the research sample requires a low degree, does not require the provision of too much data about the sample or the data of a regular sample, and is suitable for systems where the information is not very clear and does not require the data to have an obvious distribution pattern, but the results obtained are very effective and solve the subjective judgment results. The method has strong applicability and wide application, showing great practical application value. Gray correlation analysis is based on the degree of geometric similarity between the family of curves constituted by the sequence of each evaluation index and the sequence constituted by the reference sequence, and its response is the strength of association. The purpose is to evaluate the degree of overall fit of hospital quality to the ideal state.
The purpose of this article is to evaluate the degree of overall fit between the evaluation of hospital quality and the ideal state, so the TOPSIS method is combined with the gray correlation analysis to measure the gray correlation closeness of the chronic disease medical service process. The main calculation formula is as follows:
Step 1: entropy weighting method
Firstly, the results xij obtained according to the BiLSTM model are normalized. Since all indicators are positive term indicators, the treatment is as follows:

In entropy method, the entropy value is obtained by analyzing the dispersion degree of the data, and then the entropy value is used to calculate the weight of the index. The entropy value is then used to calculate the weight of the index. Therefore, the entropy method is chosen to assign weights to the indicators.
The dispersion of the indicator data is first calculated to find the entropy value of the indicator as:

In equation (8), ej is the entropy value of the indicator, and then the entropy value of the indicator is used to find the weight of the indicator as:

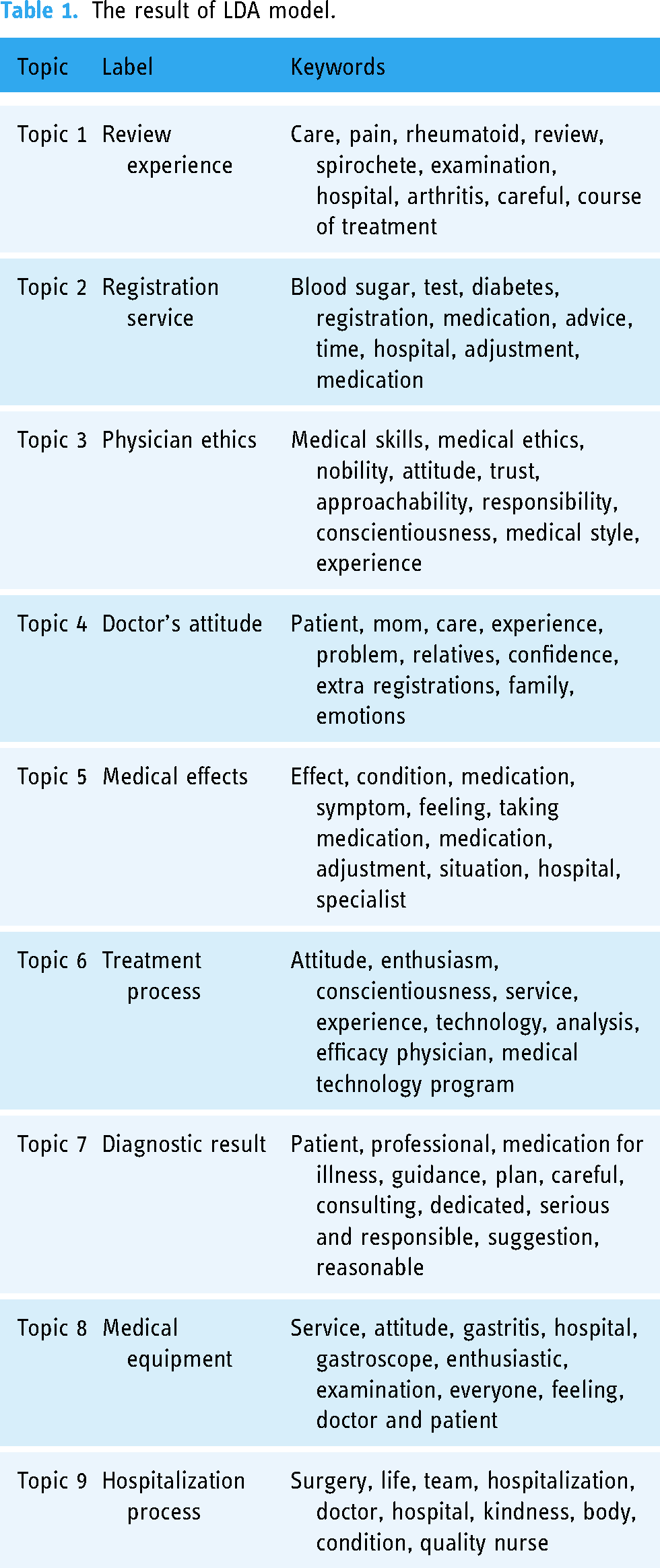
In equation (9), wj is the weight of the index and the specific weights are shown in Table 1.

The result of LDA model.
In equation (10),
Step 2: euclidean distance
The best combination yj+ and the worst combination yj− of each indicator in the seven CNDs service quality evaluation indicator to be evaluated is first determined, as shown in equations (11) and (12). Then calculate the Euclidean distance from the sample to the positive ideal solution and the negative ideal solution. As shown in equation (13) and equation (14),



Step 3: gray correlation degree
The maximum value of 



Step 4: degree of gray correlation closeness
Firstly, the Euclidean distance from the sample to the ideal solution and the grayscale correlation between the sample and the ideal solution are dimensionless.






Step 5: barrier degree evaluation model
In order to further identify the weak points of CNDs in the diagnosis and treatment process, the obstacle degree model is used to evaluate the obstacle factors of CNDs in the diagnosis and treatment process, which is calculated by the formula:
In equation (26), ϑij is the standard value of the original data obtained by the extreme value method of the three-level indicator, vj is the weight determined by the entropy value method of indicator j, ∈j is the indicator of the specific barrier degree of each disease and the sum of the barrier degrees of all indicators for each disease is 1.
Results analysis
LDA model
In this article, LDA topic model is used for topic mining. The LDA model's importance is determining the number of potential topics and naming the issues. This article uses the coherence value to determine the optimal number of cases for LDA.
This article tested 1–30 topic values and performed coherence curve fitting for the number of topics, as shown in Figure 5. Based on the results in the figure, nine topics were identified as the best solutions. Each of the nine topics is different; each document has a topic and a specific subject word and probability corresponding to each topic. The topic with the highest probability is taken as the document's topic. The right area of Figure 6 shows the top 30 words with the most frequent occurrences. You can place the mouse on the corresponding Topic and display the top 30 related words under different topics. Then, the topics are named according to the associated documents of reading medical service quality.

The result of coherence value.

The result of the LDA model.
In Topic 1, the keywords such as pain, rheumatoid, review, spirochete, examination, hospital, arthritis, careful and course of treatment suggest a focus on reviewing experiences. Considering the characteristics of chronic diseases, such as long duration and relatively low cure rates, this topic is labeled “Review Experience.”
Moving on to the next topic, keywords such as test, registration, medication, time, hospital and adjustment indicate a discussion on registration services. Therefore, this topic is named “Registration Service.”
The words medical skills, medical ethics, nobility, attitude, trust, approachability, responsibility, conscientiousness, medical style and experience are closely related to physician ethics. Thus, this topic is appropriately labeled “Physician Ethics.”
In Topic 4, high-probability feature words such as patient, confidence, family, additional registrations and emotions indicate a discussion about patients’ experiences with doctors and their attitudes. Hence, this topic is defined as “Doctor Attitude.”
For Topic 5, the keywords medication, symptom, feeling, taking medication, medication adjustment and situation suggest a focus on medical effects. Therefore, this topic is named “Medical Effects.”
Furthermore, words like attitude, enthusiasm, conscientiousness, service, experience, technology, analysis, efficacy, physician and medical technology program are associated with the treatment process. Thus, this topic is labeled “Treatment Process.”
In the subsequent topic, keywords such as patient, professional, medication for illness, guidance, plan, careful, consulting, dedicated, serious, responsible, suggestion, reasonable and diagnostic result indicate a discussion about providing diagnosis and reasonable treatment suggestions. This topic is named “Diagnostic and Treatment Suggestions.”
The following topic focuses on concerns related to service, attitude, gastritis, hospital, gastroscope, enthusiasm, examination, everyone, feeling, doctor and patient. After reviewing relevant indexes and considering medical quality evaluation information, it was decided to label this topic “Medical Equipment.”
Finally, Topic 9, with high-probability feature words like surgery, hospitalization and quality nurse, is closely related to the hospital process. Thus, this topic is appropriately named “Hospital Process.”
Based on the analogy, the results of the medical service quality topics are divided into nine categories, as summarized in Table 1.
Number of comments on different chronic diseases and corresponding themes
Based on the outcomes of the LDA model classification, we have systematically analyzed the quantity of comments across various chronic diseases and their distribution within different thematic categories, as illustrated in Table 2.
Number of comments on different chronic diseases and corresponding themes.

Remarkably, diabetes stands out with the most substantial number of comments, totaling 3075. Following closely, both Parkinson’s disease and chronic gastritis exhibit considerable engagement, garnering 3166 and 3075 comments, respectively. In contrast, bronchitis records the fewest comments, amounting to a modest 403.
Quality evaluation results
After obtaining the above indicators, a three-step framework for measuring healthcare quality was relied on, proposed by Donabedia 14 : structure–process–outcome. Three levels of hierarchy were established for the indicators and the evaluation was based on the secondary indicators among them. The attribute with the highest weight in the results of the weighting method is Materials, which indicates the importance of the adequacy of hospital supplies in the delivery of chronic care. The following two attributes are Quality of treatment and Diagnosis coincidence rate, which show that the diagnosis and treatment of CNDs greatly affect the patients’ evaluation of hospital services and doctors should have a good service attitude. Table 2 shows the weighted standardized rating values and indicator attributes of each indicator.
Combining Euclidean distance and gray correlation, the results of gray correlation closeness were obtained, as shown in Table 3. Combining the hospital service quality criteria in Table 4, it can be seen that hypertension is rated at a reasonable level, bronchitis is rated at a low level and the rest are at a medium stage. This indicates that patients communicated a general perception about having an excellent hypertensive medical experience while bronchitis patients expressed poor experiences during their visits.
Index system, weight, and index attributes.

The result of gray-associated posting progress.

In terms of specific indicators, hypertension scored as expected in terms of supplies with the highest score of 0.8571, which is at the premium level. Bronchitis also scored at the lowest level of 0.1429, indicating that there is much room for improvement in the material aspect of the bronchitis visit. However, in terms of the medical process, all the scores were at the good stage except for rheumatoid arthritis and chronic anemia, which were at the intermediate stage. In the treatment effectiveness score, there was little difference in the scores for each chronic disease. The highest score was for hypertension and the lowest score was for bronchiectasis, 0.6687 and 0.3313, respectively, indicating that there were no major differences in treatment effectiveness for these seven CNDs. The quality of treatment scores showed the same trend, with little difference in the scores for each disease, the highest being 0.5384 for diabetes and the lowest being 0.4616 for rheumatoid arthritis. In terms of diagnostic compliance rate, all were in the medium stage except for diabetes (0.6615) and hypertension (0.6610) which were in the good stage. This indicates that the diagnostic compliance rate for diabetes and hypertension is high. As for physicians’ attitudes, all CNDs were in the moderate stage, indicating that there was no significant difference among CNDs in terms of physicians’ attitudes.
In summary, there are not many significant imbalances in the medical care of CNDs. However, the imbalances in the indicators are particularly prominent in the materials and medical process.
Barriers to health care quality in these seven chronic conditions were diagnosed using the Barrier Diagnostic Model to identify resistance factors affecting quality levels. And Table 5 is the gray correlation closeness classification criteria. As shown in Table 6, the top two overall barriers were the Hospitalization process (B122) and Registration service (A121) alternately ranked first. And they accounted for a large proportion, with an average of more than 30%. This indicates that in chronic disease medical services, hospitalization and registration process have a greater barrier to the level of quality of treatment for chronic disease patients, which means that hospitals should focus on providing registration services and an inpatient environment to improve the quality of the medical process and pay attention to the actual needs of patients when improving medical service facilities in the future. In addition to these two, Medical equipment (A111), Review experience (B111) and Diagnostic result (C111), the three obstacle factors, are also large, in the same rotation of the seven CNDs fourth five or six. This indicates that there is room for strengthening in these three areas. The least significant barriers were the doctor's attitude (C122) and the course of treatment (B121), indicating that patients had good experiences in these two aspects of the quality process.
Gray correlation closeness classification criteria.

Medical service barrier factor.

CNDs are characterized by insidious onset, long duration and persistent and complex etiology. And the patients have high demands on the treatment process. In the process of improving the quality of medical services, hospitals should consider the needs of patients and effectively improve the quality of medical services.
Discussion
In this study, we performed topic analysis and sentiment analysis based on LDA topic model and BiLSTM model, and then quality analysis was performed on the obtained sentiment values. By collecting patients’ online reviews on Haodaifu website, we studied the evaluation of the quality of hospital services for seven CNDs with the following main findings.
Topic analysis
Through LDA topic identification, it was found that the evaluation of these seven CNDs can be divided into nine dimensions, which are review experience (Topic 1), registration service (Topic 2), physician Ethics (Topic 3), doctor's attitude (Topic 4), medical effect (Topic 5), treatment process (Topic 6), diagnostic result (Topic 7), medical equipment (Topic 8) and hospitalization process (Topic 9).
For Review experience (Topic 1), CNDs are characterized by a long duration of illness and a tendency to flare up. Therefore, it is inevitable for patients with CNDs to return to the clinic. Psychological studies on patients with CNDs show that patients with CNDs are more likely to be depressed due to long-term pain.39,40 Therefore, it is necessary for the hospital to provide good service during the return visit, improve the quality of service and increase patient satisfaction.
In Topic 2 registration service, because of the huge number of patients with CNDs,41,42 there is a shortage of medical resources in many large and small cities. Therefore, whether the number can be registered is also known as a major problem for patients with CNDs to see a doctor. This requires hospitals to optimize the process of seeing a doctor and to upgrade and improve the hospital's appointment system. 2 This will help solve the problem of difficult registration, improve the quality of medical services and optimize the use of medical resources.
In terms of physician ethics, the doctor–patient relationship has become a hot issue. Doctors are prone to role tensions and conflicts in their professional role-playing, which are essentially tensions and conflicts of interest within and between the roles they undertake. 43 The issue of role ethics is a major problem facing the development of medical ethics in contemporary China. The aging characteristics of Chinese society, the proliferation of difficult diseases caused by the deterioration of the ecological environment and the frequent occurrence of disharmony brought about by doctor–patient disputes, require physicians to be more aware of their role in the development of medical ethics. This requires doctors to accumulate professionalism in their work practice, cultivate ethics in the responsibility of the times and enhance communication in equal dialogue to avoid doctor-patient conflicts. 44
The next topic doctor's attitude was found in a study that patients with CNDs are prone to psychological states such as depression and anxiety,39,45,46 which therefore place high demands on the doctor’s attitude during the treatment process. It has also been shown that when doctors’ attitudes are positive, patients have higher evaluations of doctors’ enthusiasm, competence and ethical dimensions, indicating that patients generally believe in doctors’ competence, but they not only seek cheap and high-quality treatment but also look forward to doctors’ attention. This indicates that doctors should be friendly and enthusiastic in the treatment process. 47
In terms of treatment effect, although many CNDs have a very long duration, which can reach more than 5 years, some patients with CNDs even need lifelong medication to control their conditions. Most CNDs are not curable and pain can only be controlled by long-term medication.48–51 Many patients still have great hope for the treatment effect and can relieve the disease and pain through treatment. And according to patient satisfaction surveys, patients are most concerned with technical factors, that is, the quality and effectiveness of care, when they seek care. Technical competence is the basis of medical services provided by medical institutions. 52 Similarly, the symptoms of most CNDs are not obvious, specifically minor pain or insomnia and dreaminess, which requires a great deal of diagnostic accuracy from the doctor. The longer a diagnosis is delayed, the more pain it will cause the patient, which requires increased diagnostic accuracy when diagnosing CNDs.
In the case of medical equipment for CNDs, the average value of “medical equipment” indicates the patients’ concern about the hardware facilities of the medical institution. Medical equipment reflects patients’ signs and monitors their physical condition, an essential factor in patient satisfaction. 53 At the same time, funding for facilities and equipment is correspondingly low. 54 In the context of the variety and complexity of CNDs, this places new demands on the facilities and equipment of medical institutions and requires increased investment in hospital equipment. 55
Patients with CNDs experience psychological trauma during hospitalization, which can affect the quality of survival. 56 Medical and nursing staff should take measures to improve the post-traumatic growth of hospitalized chronic disease patients, thus enhancing their quality of survival.57–59
The analysis of the characteristics of CNDs, such as stable disease status, inconspicuous symptoms, long disease duration and recurrence, shows that patients with CNDs value the diagnosis, the overall process in the hospital and the doctor's attitude more in the treatment process. It shows that most patients hope that the doctor will bring a friendly attitude in the treatment process to confirm the diagnosis and treatment in a good and fast way.60,61
Using the classification results of the LDA model, we analyzed the emotions commented on by patients under each quality indicator dimension. We concluded that the vast majority of patients’ emotional tendencies are positive. Most of these positive emotions originate from gratitude to the doctor for the relief of the illness and the compliments of the doctor's medical skills. This is similar to the findings of the patient satisfaction surveys, which showed a strong effect of physician-related factors on treatment outcomes. 62 However, most of the existing negative emotions stem from the following problems: first of all, the attitude of some doctors can be impatient. 63 At the same time, there are power imbalance between doctors and patients, and sometimes doctors may criticize patients, and patients will have distrustful emotions 64 ; secondly, due to the chronic illnesses that are prolonged and complicated in their causes are boring for most patients; these emotions will be brought to the evaluation of medical treatment 65 ; finally, the high number of patients with CNDs makes hospitals too popular, with complex registration and endless queuing times, which primarily affects the medical experience.
Sentiment and service quality evaluation orientation analysis
Based on the sentiment score values, a quality model was applied to evaluate their quality. The closeness of the gray correlation shows that diabetes evaluation scores are the highest, indicating that among these seven diseases, diabetes patients have a good experience in medical visits. This finding is similar to the results of previous studies. 66 It may be that the symptoms of diabetes are not evident and severe at the beginning of the disease. In addition, the number of patients with diabetes is significant. Most hospitals have a relatively complete treatment system for it, 67 so the patients’ evaluation of it is also very high. According to previous patient satisfaction surveys, male patients scored higher than female patients on the process of service delivery by the provider, that is, the services provided by the medical staff during the process (including the entire process of medical team inquiry, prescription pricing, drug capture, registration and drug description). 68
In contrast, bronchiectasis has a meager score, especially in the “Materials” category, with a score of only 0.1429. The next lower score is observed in the “Treatment Effectiveness” category. It is possible that bronchitis requires specific medical supplies such as bronchodilators and nebulizers, and the hospital may not adequately provide these specialized equipment, leading to lower ratings in the “Materials” category. The hospital may face challenges in the supply chain, resulting in insufficient availability of both routine and specialized medical supplies, thus impacting overall patient satisfaction with medical services. Given the complexity of bronchitis as a chronic condition, effective treatment may require a more personalized and customized approach. Failure to consider individual patient differences in the treatment plan could also influence the perceived effectiveness of treatment. To enhance satisfaction with medical services for bronchitis patients, hospitals may consider the following improvements:
Ensure that the hospital adequately provides the specific medical supplies required for bronchitis patients to enhance ratings in the “Materials” category. Ensure a smooth supply chain to guarantee an ample supply of various medical materials, improving the overall quality of medical services. Pay closer attention to individual differences among bronchitis patients, offering more personalized treatment plans to improve treatment effectiveness and overall patient satisfaction. This can be achieved through in-depth patient history assessments and regular evaluations.
By implementing these improvements, hospitals can better cater to the unique needs of bronchitis patients, elevate the overall quality of services, and enhance patient satisfaction.
The remaining five diseases are all rated at the medium level, and all have excellent ratings in terms of materials, indicating that most hospitals can meet the material needs of patients in CNDs.
The barriers orientation analysis
The barriers to the established disease access process were analyzed to identify further the factors limiting the quality of the chronic disease access process. The results showed that the two indicators with the highest average obstacles to the quality of the established disease process were the Hospitalization process (B122) and registration service (A121). The percentage of both is high, especially in hypertension, where the indicators hospitalization process and registration service account for 37.6486% and 31.3850%, respectively, which means that hospitals should optimize the inpatient process by streamlining the admission process, increasing the efficiency of admissions and improving the patient admission experience. This can help reduce the number of barriers patients encounter during the admission process and improve the overall efficiency of healthcare delivery. To address the barriers to registration services, hospitals can introduce smarter booking systems, provide online registration services, etc.69,70 In order to reduce the waiting time and cumbersome registration process before seeing a doctor, thereby increasing patient satisfaction. The third indicator is the Medical effect (C112), which accounts for about 15% on average, which is not tiny. This indicates that patients still hope to be treated to alleviate their pain and suffering in medical treatment. Still, due to the irreversible nature of CNDs, most of them need to achieve complete improvement and treatment effects. Therefore, in the quality survey, this indicator has a large proportion of the barrier factor. The following three indicators are medical equipment (A111), review experience (B111) and diagnostic result (C111), ranked 4, 5 and 6, alternating back and forth among the seven diseases, with an average share of between 10% and 5%. This indicates that there is still room for improvement in these three indicators, but overall, patients are satisfied with these three indicators. It is because Patients’ relatively high ratings of medical equipment may be attributed to hospitals’ substantial investments in and provision of advanced and suitable medical equipment. The satisfaction expressed by patients regarding the equipment reflects the hospital's commitment and expertise in delivering quality medical services. Similarly, the favorable rating of the review experience suggests that the hospital provides effective review services during patients’ visits, facilitated by professional healthcare staff and an efficient review process. Moreover, the relatively high satisfaction with the diagnosis indicates the healthcare team's high level of professionalism and accuracy in diagnosing patients, showcasing the hospital's success in confirming disease diagnoses.
The seventh-ranked indicator is Doctor's ethics, which accounts for about 1.5% of the total, indicating that doctors and patients can maintain a good relationship in the treatment process and have fewer doctor-patient conflicts. The last two indicators are Doctor's attitude (C122) and the course of treatment (B121), which account for less than 1%, meaning that patients are satisfied with the treatment process and the doctor's attitude.
Academic contribution
In contrast to existing studies, our research delves into the evaluation of Medical Services by patients with CNDs, presenting a wealth of new findings that enrich the scholarly landscape in this domain.
Our study unravels nuanced patterns in the assessment of various CNDs, revealing a favorable rating for hypertension, a lower rating for bronchitis, and the remaining CNDs falling within an intermediate range. This detailed differentiation enhances our understanding of patient perceptions across diverse chronic conditions, providing a more comprehensive view for healthcare practitioners and policymakers.
A distinctive aspect of our research lies in the identification and prioritization of specific barriers within the medical service evaluation process. Notably, the hospitalization process and registration services emerge as the foremost obstacles, each contributing to approximately 30% of the identified barriers. This precise identification equips hospitals with actionable insights, offering a strategic roadmap to enhance overall service quality and patient satisfaction.
Our methodology adopts a holistic approach, integrating advanced techniques such as the LDA theme model, BiLSTM sentiment analysis, and quality management theory to construct a robust evaluation index system. The incorporation of entropy-valued, TOPSIS, and gray correlation models represents a methodological advancement, providing a comprehensive framework for the nuanced assessment of medical service quality.
Emphasizing the hospitalization process and registration services as primary barriers, our study goes beyond the mere identification of challenges. It provides targeted recommendations for hospitals, offering practical solutions to optimize efficiency and elevate patient satisfaction. These specific insights act as a valuable guide for healthcare institutions striving to enhance the overall quality of medical services for CNDs patients.
In conclusion, our research not only underscores the importance of evaluating medical services for CNDs patients but also introduces novel insights, methodological advancements and focused recommendations that contribute substantively to the field. As we navigate the intersections of patient experiences and healthcare improvements, our findings pave the way for transformative enhancements in medical services for individuals with CNDs.
Conclusions
Through a comprehensive analysis integrating thematic and sentiment analysis with service quality assessment, this study investigates the evaluation of healthcare services by patients with CNDs. The key findings revolve around the diverse assessment of various diseases, nuanced affective tendencies and the identification of barriers to service quality. In summary, patients with different chronic diseases exhibit varying evaluations, notably with those suffering from hypertension expressing higher satisfaction compared to individuals with bronchiectasis. The prevalence of positive sentiments, rooted in gratitude for therapeutic effects and commendation for medical skills, provides valuable insights for decision-makers aiming to enhance healthcare services. The clear identification of barriers, such as admission and registration processes, underscores the imperative for optimization through the introduction of a smart reservation system and online registration services.
Given the protracted nature of chronic diseases, this study on the Chronic Disease Access Service Quality Survey, coupled with sentiment analysis, offers crucial insights for healthcare stakeholders. To elevate patient satisfaction during hospital visits, strategies include implementing personalized treatment plans, enhancing patient communication and providing psychological support to address the unique challenges faced by patients with chronic illnesses.The introduction of a Smart Appointment System, online registration services, electronic medical records and telemedicine consultations aims to amplify the convenience and efficiency of healthcare services. A comprehensive feedback mechanism, encompassing a real-time patient feedback platform, satisfaction surveys, doctor–patient communication meetings and a transparent complaint-handling process, contributes to continuous improvement.
In conclusion, this research equips decision-makers with pivotal information to enhance healthcare services for patients with chronic diseases. The insights provided empower stakeholders to make informed decisions based on actual data, fostering a continuous improvement cycle for both patients and healthcare organizations.
Limitations and future research
This study possesses several limitations that merit consideration in future research. First, our data were exclusively sourced from a single online platform, potentially introducing selection bias. The comments on the website may predominantly originate from patients willing to share their experiences, leading to a skewed sample. Some patients may be more inclined to share negative experiences, while others may focus solely on positive feedback. Furthermore, variations in patients’ criteria for evaluating medical services could introduce subjective factors, complicating the assessment process. The lack of consistent evaluation standards may pose challenges in comparing and synthesizing comments. Additionally, the inability to ascertain patients’ health status within the website further limits the depth of understanding regarding their overall well-being.
The dimensions are narrow and not comprehensive enough. In the future, we can further emphasize the potential presence of other factors that may affect the evaluation of medical services, such as patients’ perceptions of medical costs, 71 transparency of medical information,72–74 communication skills of doctors,75,76 etc. So future research could develop new methods to measure service quality more effectively and comprehensively. Third, the data collection was limited to seven CNDs and the characteristics of CNDs are quite different from other diseases, so the promotion recommendations cannot be generalized to more diseases. Fourth, the data for this study came only from patient reviews on the Haodaifu website. Therefore, the analysis was only from the patient's perspective, without taking into account the specific situation of the hospital, and may not be able to specifically analyze the shortcomings of the specific hospital. Future studies can obtain data from hospitals and use a combination of internal and external methods to analyze the quality of services provided by hospitals. Lastly, we used the BiLSTM model for sentiment analysis, which may not identify expressions such as sarcasm and irony in some people. In future studies, we suggest that researchers include data from multiple diseases and within the hospital to perform the quality evaluation in the next study.
Footnotes
Acknowledgments
We thank all the participants and all the researchers and collaborators who participated in this study. We thank Dr. Lu Ning (The Second Hospital affiliated of Kunming Medical University, Kunming, China) for helping in this revision. All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Contributorship
Jing Dai contributed to the conception of the study; Fang Lyu crawled the data, analyzed the data and wrote the manuscript; Lin Yu performed the data analyses; Zixuan Zhou performed the data analyses; Yunyu He contributed to the manuscript preparation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The survey was approved by the Medical Ethics Committee of the First People's Hospital of Yunnan Province. Written informed consent to participate in this study was provided by the participant's legal guardian/next of kin. Written informed consent was obtained from the individual(s) and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 71764014).
Guarantor
YH.