
Abstract
Objective
The patient–provider relationship is critical for achieving high-quality care and better health outcomes. During the COVID-19 pandemic, primary care practices rapidly transitioned to telehealth. While telehealth provided critical access to services for many, not all patients could optimally utilize it, raising concerns about its potential to exacerbate inequities in patient–provider relationships. We investigated technical and workforce-related barriers to accessing telehealth and the impacts on patient–provider relationships for vulnerable populations.
Methods
Qualitative, semi-structured interviews from May 2021 to August 2021 with 31 individuals (medical directors, physicians, and medical assistants) working at 20 primary care practices in Massachusetts, North Carolina, and Texas. Thematic analysis to better understand how barriers to using telehealth complicated patient–provider relationships.
Results
Interviewees shared challenges for providers and patients that had a negative effect on patient–provider relationships, particularly for vulnerable patients, including older adults, lower socio-economic status patients, and those with limited English proficiency. Providers faced logistical challenges and disruptions in team-based care, reducing care coordination. Patients experienced technological challenges that made accessing and engaging in telehealth difficult. Interviewees shared challenges for patient–provider relationships as commonly used telephone-only telehealth reduced channels for non-verbal communication.
Conclusion
This study indicates that barriers to virtual interaction with patients compared to in-person care likely led to weaker personal relationships that may have longer-term effects on engagement with and trust in the healthcare system, particularly among vulnerable patient groups. Additional support and resources should be available to primary care providers to optimize telehealth utilization.
Introduction
The patient–provider relationship has long been shown to be critical for fostering interpersonal trust and reducing inequities in health outcomes.1–8 Ultimately, research shows that trust in the patient–provider relationship is associated with improved treatment adherence 9 and better health outcomes.6,10,11 Patient satisfaction and trust in their physicians are fostered when providers care for patients’ interests, have good interpersonal skills, are seen as a reliable source of information, respect patient confidentiality, and utilize non-verbal communication, such as warmth and listening.12–16 However, studies show poorer quality of communication between providers and vulnerable populations, leading to worse outcomes, including care discontinuity, patient dissatisfaction, inadequate shared decision-making, and a higher financial burden for patients and society at large.16–20 However, nearly all of this research has focused on patient–provider interactions during in-person visits.
The evolution of telehealth has been a dynamic journey, shaped by advances in technology and changes in healthcare delivery models in the last two decades.21–26 Telehealth services are provided through synchronous (e.g. video or phone consultations and live chats), asynchronous (e.g. email and messages), and remote monitoring of health conditions (e.g. wearable devices) 27 across various medical disciplines, such as primary care, psychiatry, and maternal health.21,26,28–33 However, the uptake of telehealth before the pandemic has been limited due to policy regulations in the United States.34,35 The COVID-19 pandemic led to rapid uptake of telehealth, increasing use by 300% 36 serving as a vital tool for delivering healthcare while minimizing the risk of virus transmission. Quantitative studies on telehealth during the pandemic show lower use among vulnerable groups.37–39 We define vulnerable populations according to the definition by the Centers for Disease Control and Prevention as populations disproportionately affected by disasters and adverse events (e.g. low-income, limited English proficiency, racial and ethnic minorities, and the elderly). 40 Documented patient- and provider-level barriers to accessing telehealth services include digital literacy, technology, and broadband access, limited data plans, older age, and provider satisfaction with telehealth.39,41–44 Due to patient-level barriers, most of these populations have received telehealth services using telephone-only modality,39,41,42 potentially impacting the quality of communication between patients and providers. While some clinicians and patients have shared personal narratives of challenges in establishing an emotional connection with patients over telehealth,45–47 little empirical work to date has examined the critical but harder-to-measure impacts of telehealth expansion, such as how telehealth, particularly, telephone-only modality, changed patient–provider relationships for established patients and creating patient–provider relationships with new patients.29,30 Particularly given underlying differences in the quality of interpersonal communication between providers and patients from vulnerable populations, the rapid uptake of telehealth may negatively impact the patient–provider relationship for these groups. For example, patients and providers need access to reliable internet connections and devices, which may present barriers for some individuals, especially those in underserved or rural areas. Moreover, telehealth may limit the ability to fully send and receive non-verbal cues, potentially impacting the depth of understanding between patients and providers.
In this study, we examine the impact of telehealth, particularly the telephone-only modality and its barriers to patient–provider relationships with a critical eye toward vulnerable populations. We use qualitative data from interviewees at primary care practices to elucidate the complex interdependency of provider- and patient-level barriers to telehealth utilization and their subsequent impact on the patient–provider relationships.
Data and methods
We collected and analyzed cross-sectional, semi-structured qualitative interviews with providers and staff at primary care practices to understand the barriers to utilizing telehealth and how those barriers affect the patient–provider relationship. This design enabled us to explore and describe the lived experiences of providers, administrators, and leaders as they transitioned to telehealth during the COVID-19 pandemic. We purposively sampled practices in North Carolina, Massachusetts, and Texas, seeking variation in healthcare infrastructure and state policies (e.g. Medicaid expansion) relevant to the pandemic and telehealth. Within each state, we sought variation by rural versus urban location, independent versus health-system affiliated practices, and safety net (serving low-income patients) versus non-safety net practices. This sampling strategy allowed us to deliberately choose participants based on specific characteristics or criteria relevant to maximizing the diversity needed to capture the experiences of practices serving vulnerable populations. The study was deemed exempt by the Institutional Review Boards at the University of North Carolina. Since this research presented no more than minimal risk of harm to interviewees and did not involve procedures for which written consent is normally required, verbal consent was deemed sufficient by the IRB. All data security protocols required by the Institutional Review Board for qualitative data were followed, including de-identification of data and storage in a password-protected environment.
We recruited individuals at practices via email and phone outreach. We contacted 148 primary care provider organizations in three states, of which 19 declined to participate, 20 accepted to participate and others did not respond. To capture different perspectives within a given practice, we requested interviews with up to three individuals at each practice: a medical director, a clinician, and a medical assistant. Verbal consent was obtained at the beginning of the interview
We conducted content analysis and coded transcripts using NVivo 11 software. We used a hybrid approach to coding our data. 48 First, we developed the codebook deductively or a priori based on the domains of inquiry in the interview guide and existing literature, then we added codes inductively as new themes highlighting challenges with telehealth emerged in the data. The final codebook included 15 parent codes and 40 child codes, 12 of which were related to telehealth. For this study, we used data coded under the telehealth codes. Two research team members (GM and MA) independently coded the first four transcripts to assess the adequacy of the codebook. All members met regularly to establish agreement about the appropriate application of codes. Overall, agreement was strong, with most disagreements concerning the length of surrounding text coded. This iterative process led to minor changes to the codebook. For example, the code technology was interpreted as the technology used for telehealth by one coder and technology on the patient and provider sides, including highlights and barriers to using telehealth. After discussion, several sub-codes were added to the technology code to capture all the dimensions of telehealth technology in our data. One team member (MA) then coded all transcripts. The team discussed uncertainties that arose during the coding process to maintain agreement on definitions, interpretations, and emergent themes and how they might be influenced by the individual team member's positionality. The coder used reflexivity and memoing to critically examine and reflect on their own positionality throughout the analysis process that came from implementation science and clinical background. The interpretation was discussed with other research team members for validation.
Results
Our sample included 20 diverse primary care practices, varying by practice type, rurality, safety-net status (serving primarily low-income populations), and 31 interviewees with various roles within those practices (Table 1). Overall, 19 of 20 practices implemented telehealth at the beginning of the pandemic. Before the pandemic, 40% of practices had some telehealth infrastructure, but that uptake was minimal due to a lack of reimbursement. Interviewees reported that during the first few months of the pandemic, 80–90% of their visits were provided via telehealth, which gradually dropped to 10–30% between May and August 2021, roughly 12–18 months since the beginning of the pandemic. Of telehealth visits, interviewees reported that 50–80% of telehealth consults were telephone-only, without video.
Characteristics of primary care practices and participants in the sample.

Note. Rural versus urban designation was determined based on the Federal Office of Management and Budget categorizations.
Mixed service coverage area means that primary care practices have multiple locations in both rural and urban counties.
Safety-net practices are the primary care practices serving primarily low-income, uninsured or underinsured populations.
We found three interconnected themes in our data related to challenges in implementing and utilizing telehealth and how they impacted the patient–provider relationship. First, technical and workflow challenges associated with telehealth influenced how clinicians provided care. Second, the delivery of telehealth services was constrained by infrastructure on the patient's end, further complicating the provider and patient experience. Lastly, telehealth requires a fundamentally different way of communicating with patients, with a dampening effect on the quality of patient–provider relationships. We find that telehealth, primarily telephone-only, creates a thinner interaction between patients and providers, straining the relationship and increasing the need for trust while reducing avenues to establish and maintain trust.
Workflow challenges of telehealth disrupted practices’ care for patients
Telehealth complicated the provision of care for participating practices, impacting the patient–provider experience, particularly for rural and low-income patients. Transitioning to telehealth during the pandemic created multiple challenges for participating practices, including technological challenges consuming provider time at the expense of time spent in patient visits; destabilizing team-based care; and rendering auxiliary care (e.g. social workers and interpreters) more challenging (Table 2).
Themes, subthemes, and representative quotes for workflow and technical challenges faced by providers and patients.

Interviewees described challenges with technology on both the practice and patient sides at the onset of the pandemic. At the practice level, many interviewees described using multiple telehealth platforms to find the one appropriate for their practice and patients. Initially, practices used platforms that were convenient to use but later shifted to ones that were HIPAA compliant, compatible with their electronic health record systems, and better fit with their operating budget. Changing platforms meant providers and patients were frequently learning about newer platforms. More pressingly, many reported struggling with basic hardware and software issues. While some organizations provided more support for telehealth, particularly large practices or health systems, all interviewees reported it took additional work and time to ensure patients could successfully use telehealth services. With changing platforms, patient education about using telehealth had to be revisited. Medical assistants and front desk staff provided most of this patient support at the beginning of the visit. This was particularly acute for patients at safety net practices. A provider at a safety-net practice described, “they [staff] try to get the patient in the tele-visit. And if the patient has problems, they'll get on the phone and just spend a lot of time…” In some instances, this work, along with the pre-work needed for visits, was done by the providers, reducing the time for the clinical encounter. In addition, interviewees described pressure to use video (as opposed to phone-only) for telehealth, which was frustrating for some providers because the technology seemed to be beyond many patients.
Before the pandemic, team-based care was widely used in primary care settings to address the needs of patients.33–39 However, the transition to telehealth impacted how clinical teams worked and their effectiveness for patients. First, team-based care required efficient communication between team members. Before the pandemic, medical assistants or nurses would walk to the physician's office to convey issues concerning patients. This ability to communicate in real-time on an as-needed basis was disrupted because of how telehealth workflows were set up. With reduced communication and coordination among the care team, team-based care broke down, and individual encounters between patients and providers became higher stakes.
Relatedly, interviewees described struggles to access their auxiliary staff during telehealth encounters. For example, during in-person visits, a patient would walk to the front desk to schedule follow-up appointments, or team members could send the patient to a co-located social worker when needed. During telehealth encounters, these routines were disrupted, leaving patients needing to fill the gaps. Similarly, accommodating team members critical to more vulnerable populations, such as behavioral health specialists, during telehealth visits was challenging.
All of these factors that impacted clinics’ workflow reduced the ability of practices to deliver the same quality of care through telehealth compared to in-person, with particular disruption for more vulnerable patient groups.
The delivery of telehealth services was constrained by infrastructure on the patient's end
In addition to challenges providers faced in setting up telehealth, interviewees described challenges their patients faced in accessing telehealth services, particularly elderly patients, low-income rural patients, and patients with limited English proficiency.
According to the interviewees, elderly patients either did not have access to laptops and smartphones or did not know how to use them. Moreover, interviewees described setting up a telehealth visit with video was complicated for most of them. However, use of phone-only visits had critical implications for elderly patients. For example, medical assistants described how limited access to video or other technology (e.g. patient portals) put the onus of writing down any medication changes on elderly patients. A medical assistant described, “You don't know what they're writing down. So, we would have a lot of callbacks…” Interviewees described identifying strategies to address these challenges, which were more effective for some patients than others (Table 3). Interviewees described elderly patients who had multiple telehealth visits became more comfortable over time; however, only those elderly patients with access to technology and adequate cognitive capacity could more efficiently use telehealth over time with this additional support from the practice staff and care team.
Strategies used by primary care providers to improve patient access to video-based telehealth when possible.

Interviewees also described challenges in delivering telehealth to patients with limited internet or cellphone access, such as rural populations with limited broadband access; low-income patients with limited data or minutes on cellular service; and homeless patients unable to access a cell phone or internet connection. Clinics tried a variety of strategies to overcome these challenges, such as offering drive-through telehealth services, Wi-Fi access in clinic parking lots, and volunteer-based networks for populations with any electronic instability. (Table 3)
Interviewees from practices serving ethnically diverse populations described their challenges of communicating with patients with limited English proficiency (LEP) via telehealth. Interviewees described the inability to comprehend Spanish over the phone, which necessitated video visits.
Taken together, patients’ ability to access telehealth services created challenges for vulnerable subgroups, such as elderly patients, rural patients with limited broadband or cell service, and patients with LEP. While some clinics deployed strategies to overcome challenges, the data suggest that the loss of the physical space for a patient visit with a provider posed challenges that disproportionately affected vulnerable subgroups, impacting patient–provider relationships.
Telehealth and patient–provider relationships
The shift to telehealth led to technical and workflow challenges for providers and patients, culminating in impacts on the patient–provider relationship. Three critical factors emerged in our data. First, telephone-only visits removed essential dimensions of the face-to-face interaction between patient and provider. Second, telehealth had a particularly deleterious impact on developing patient–provider relationships for new patients. Third, telehealth hampered trust for both patients and providers. (Table 4)
Impact of workflow and technical challenges on patient–provider relationship.
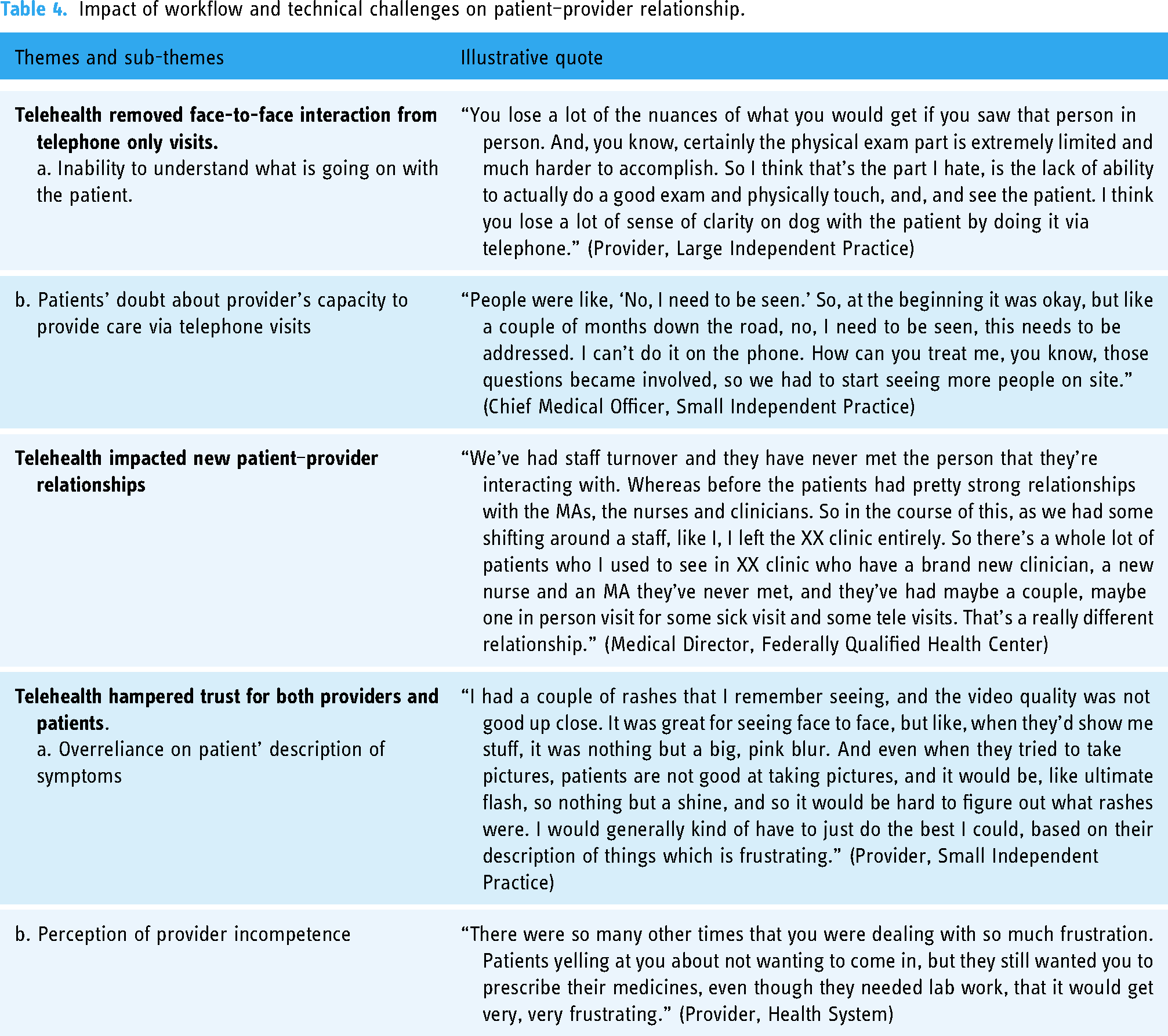
As noted above, telehealth visits with video frequently needed to be converted to telephone-only visits due to technical or logistical issues. Interviewees reported dissatisfaction with telephone-only communication because it was much more challenging to ascertain what was happening with the patient. Some interviewees identified limited utility for telephone-only visits, such as follow-up visits. Moreover, interviewees shared that their patients were also frustrated by telephone-only visits and had started questioning clinicians’ capacity to effectively deliver care through telehealth.
Interviewees described additional challenges when seeing a patient over telehealth who was a new patient rather than an established patient. High provider turnover and staffing shortages meant practices and healthcare systems were often shuffling staff between practice locations or hiring new staff to cover patient visits, leading to many visits where a patient was new to a given provider. This perspective was mostly shared by interviewees serving predominantly Spanish and Mandarin–Chinese-speaking patients. A provider at a safety-net practice described, “I'm not fluent in Spanish, but I have a very high percentage of Spanish-speaking patients. So, I bring them into the clinic for their first visit. If somebody is new, I see them in the clinic. And particularly anybody who's using a tramp [interpretation services]. We have probably another eight languages we're seeing patients in, and I bring them all in and do it in person and then after that, I'll do it on the phone or on video. And that seems to help, but having some personal relationships seems really important.” As challenging as telehealth can generally be when there is no prior face-to-face interaction to ground the clinical encounter, telephone-only consults are yet more difficult. 49
Finally, telehealth demanded greater reliance on trust between patients and providers in ways neither were accustomed to. For example, far more so than in in-person clinical encounters, physicians had to depend on the patient's explanation of their symptoms, such as a description of a rash or blood glucose level. For visits by telephone-only, instead of relying on their own visual observations paired with the patient report, physicians had to rely much more heavily on patients’ descriptions of their condition, which requires a greater reliance on patient description than is required during in-person encounters.
At the same time, the inability of physicians and clinical staff to help patients in a telehealth encounter in the same way that was possible in an in-person visit created frustration among patients toward clinic staff. As one physician described, “There were times you were dealing with so much frustration [from patients].” These challenges could create perceptions of provider incompetence and erode patients’ trust, even for patients with whom providers had long-term relationships.
Thus, telehealth stripped away key channels that support trust, such as non-verbal communication, and simultaneously required clinicians to rely on patients to a greater degree than is the norm during in-person encounters.
Discussion
Our results highlight how telehealth created challenges for providers and patients that ultimately had a negative effect on patient–provider relationships, particularly for vulnerable patients, including older adults, patients with lower socio-economic status, and those with limited English proficiency. Rapid expansion of telehealth resulted in logistical challenges at the practice level, with front-line staff bearing the brunt of this burden and resulting in disruptions in team-based care that particularly affected vulnerable populations, reducing coordination of care and, in some cases, placing additional burdens on patients. At the same time, patients experienced technological challenges that made it difficult to access and engage in telehealth effectively. Finally, rapid telehealth expansion presented unique challenges for patient–provider relationships as the medium reduced channels for non-verbal communication critical to developing and maintaining patient–provider relationships while increasing demands for mutual trust. These relational barriers are particularly critical for health equity, as they present additional challenges to clinical relationships that already suffer from lower-quality in in-person encounters.
Our study extends the literature by demonstrating that while telehealth increases access for some populations, it creates difficulty in establishing patient–provider relationships with vulnerable populations. Telehealth has been used for a variety of health conditions among rural, elderly, and low-income populations across the United States.32,33,50 Several studies have shown better access to care, improved uptake of services, and better provider and patient satisfaction with telehealth.22,32,33,51–53 For example, Choi et al. conducted a study with 121 homebound low-income individuals, ages 50 and above with depression to test the feasibility and acceptability of problem-solving training by comparing video-assisted telehealth, telephone-only training, and in-person training. 32 They showed that the improvement in depression scores was higher with video-assisted telehealth and in-person visits as compared to telephone-only visits. 32 Though important these results are not generalizable to broader population because participants receiving video-assisted telehealth were provided with devices and stable internet connection which is not common among general population. Similarly, a literature review of studies on telehealth in rural areas showed higher acceptability and increased satisfaction among rural patients and that technology was convenient to use. 33 Other patient benefits included time and time for travel. Benefits for healthcare providers included lower in-person staffing utilization, improved physician retention, and satisfaction. 33 However, some of these studies were conducted in controlled settings making it difficult to generalize results to broader population. One of the studies about tele-lactation included in the literature review showed reluctance of mothers to conduct video calls with a provider they had never met before, preference for local breastfeeding resources, and technical issues, and limited Wi-Fi in rural areas. 33
Our study extends the literature on telehealth and equity by providing critical findings on the impact of telehealth on access to and quality of therapeutic encounters. In keeping with recent work,54–57 our findings indicate that telehealth of all modalities (video and telephone-only) hinders team-based care for vulnerable populations, which is critical for developing patient–provider relationships, improving care management, and empowering patients with chronic conditions.58,59 Further, prior studies have shown mixed provider satisfaction with the quality of interaction between patients and providers during telehealth52,60,61 and limited evidence about provider trust in patients, particularly in marginalized and vulnerable populations. 62 Studies have shown a relationship between patient socio-demographic characteristics, such as race or socio-economic status, and variance in physician behavior and treatment offered.63,64 A study conducted by van Ryn and colleagues on 618 patient encounters examined the effect of patient race and socio-economic status on physicians’ attitude toward patients. The study showed physicians tended to perceive African American, and patients from low and middle socio-economic groups more negatively on intelligence, risk behavior, medication adherence, personality, and behavioral tendencies than they did Whites and upper SES patients. 63 Studies have identified several factors affecting the relationship between patient socio-demographic characteristics (such as race or socio-economic status) and variance in physician behavior and treatment.65–69 These include the provider's implicit bias,65,66 cultural competence, 67 communication style, 68 and ability to establish patient rapport. 69 Our study extends the literature by highlighting the potential negative consequences of widespread telehealth use for vulnerable populations who have been shown to experience poorer patient–provider communication during in-person encounters resulting in detrimental effects on health outcomes.16,18–20,70–73 Sub-optimal communication has been shown to be associated with poorer medication adherence, lower patient satisfaction, and worse health outcomes.59,74,75 Vulnerable patients, particularly, elderly, low-income, certain racial and ethnic groups, and those with limited English proficiency have been shown to experience communication gaps with providers as a result of the complex interplay of health literacy, quality of patient–provider relationships, and psychosocial factors such as mistrust in the health system.14,18–20,70,71,76–78 More recent studies have focused on examining disparities in patient–provider communication via telehealth.47,79 A 2020 survey of 932 adult telehealth users over 35 years of age with a history of smoking, chronic obstructive pulmonary disorder, and psychological distress compared satisfaction with patient-centeredness of telemedicine (video-only) consultations for open-endedness, and empathy by rural/urban residence using the Interview Satisfaction Questionnaire. The study showed higher satisfaction with open-endedness and expressed empathy by the telehealth service provider. 79 Our study extends this work by identifying how telehealth, particularly telephone-only modality, can strain the patient–provider relationship by requiring increased trust while reducing communicative channels that are critical to establishing and maintaining trust. Without proactive efforts to build communication skills and address technological barriers, the wide-scale use of telehealth services beyond the pandemic may perpetuate disparities in healthcare access and quality in vulnerable and marginalized communities.
Our findings provide critical guidance to policymakers, payers, administrators, and other key stakeholders. Since the COVID-19 pandemic, telehealth reimbursement policies have shifted from temporary policy waivers to an interest in permanent changes in telehealth policy, making equity considerations critical for decision-making.80,81 If these policy changes become permanent, designing and testing hybrid care models with in-person and complimentary telehealth components may be considered, particularly for vulnerable populations. Telehealth does provide better access in some situations, and more work needs to be done to help practices best incorporate it. Understanding the dynamics highlighted here could inform healthcare organizations on how to better structure telehealth to mitigate the negative implications highlighted in this article. To optimize its utilization, telehealth should be supplemented with additional support and resources to providers. This support can include technical solutions to re-constitute team-based care and re-integrate ancillary services for the telehealth environment and communication training to overcome the barriers of reduced communication channels in telehealth.
This study has several limitations. First, our sample reflects perspectives from primary care organizations from three states, which may limit the application of our results to broader primary care settings. Second, data were collected during the early phases of widespread telehealth implementation, and some of the technology-related barriers may have been addressed since these data were collected. Third, only primary care providers and staff participated in this study; the disparities noted reflect their perspectives alone. Future research should focus on examining the lived experiences of vulnerable populations during telehealth encounters for understanding their perceptions of patient–provider relationships. Lastly, data were collected during the early phases of the pandemic when interviewees were handling constantly changing COVID-19-related policies, which could have led to more recollection of barriers than facilitators. Future research should focus on the facilitators of telehealth adoption and equitable implementation from provider and patient perspectives. Despite these limitations, our study offers critical insights into the mixed utility of telehealth, including its implications for the patient–provider relationship, particularly for vulnerable populations.
Conclusion
While the widespread availability of telehealth may have led to increased access in some populations, this study indicates that barriers to virtual interaction with patients compared to in-person care may weaken patient–provider relationships. This may result in longer-term effects on engagement with and trust in the healthcare system, particularly among vulnerable patient groups. For equitable utilization, telehealth should be supplemented with additional support and resources. These include technical solutions to re-constitute team-based care for the telehealth environment and communication training to overcome the barrier of reduced communication channels in telehealth. This is particularly important for practices serving vulnerable populations, including small practices and health centers with smaller operating budgets and requiring focused support to best serve vulnerable populations.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241233148 - Supplemental material for Advancing equity in challenging times: A qualitative study of telehealth expansion and changing patient–provider relationships in primary care settings during the COVID-19 pandemic
Supplemental material, sj-docx-1-dhj-10.1177_20552076241233148 for Advancing equity in challenging times: A qualitative study of telehealth expansion and changing patient–provider relationships in primary care settings during the COVID-19 pandemic by Monisa Aijaz, Valerie A Lewis and Genevra F Murray in DIGITAL HEALTH
Footnotes
Author Contribution
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was deemed exempt by the Institutional Review Board at the University of North Carolina at Chapel Hill (#21-0085).
Funding
This study was supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under Cooperative Agreement U81HP26495, Health Workforce Research Centers Program as part of an award totaling US$525,465 with 0% financed with non-governmental sources. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government.
Guarantor
MA.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.