
Abstract
Objective
While there is a rise in mobile health (mHealth) usage and evidence of improved patient care, its widespread acceptance and adoption are limited. User engagement is a major determinant in successful implementation of mHealth. However, there is limited understanding of doctors’ challenges in adopting mHealth in their clinical practice. This study explored the perception and experiences of primary care doctors (PCDs) in adopting mHealth with their patients.
Methods
A qualitative study was conducted using semi-structured interviews with 20 primary care doctors (4 family medicine specialists, 15 family medicine trainees, and 1 medical officer) in Malaysia. PCDs were purposively sampled based on gender, ethnicity, age groups, professional position and years of experience. All interviews were audio-recorded and transcribed verbatim. The qualitative analysis was performed using a thematic analysis.
Results
Five themes emerged from this study: (1) perceived benefits of adopting mHealth with patients, (2) doctors’ approaches to facilitating mHealth use and adoption, (3) identifying credible mHealth resources, (4) selecting patients to adopt mHealth, (5) privacy concerns when delivering mHealth.
Conclusion
Despite positive perception of mHealth use in improving patient care, PCDs face significant challenges in adopting mHealth with patients. To address these barriers, targeted interventions should be developed to enhance PCDs’ knowledge, skills, and confidence in integrating mHealth in their clinical practice. We need to find ways to provide support for PCDs in mHealth adoption, particularly in resource-limited settings.
Introduction
Mobile health (mHealth) is defined as medical and public health practice supported by mobile devices, and other wireless devices. 1 It holds a promising role in addressing the challenges faced in primary care settings caused by a lack of workforce and increased workload on the primary healthcare system. 2 mHealth initiatives have been growing in the past decades because of high smartphone penetration, technological advancement, improving internet coverage and growing acceptance of digital interventions. mHealth technology enables remote monitoring of chronic conditions, assists physicians with clinical diagnosis and decision-making processes, promotes changes in patient behaviour, provides patient education, and improves communication between healthcare services and patients. 3 Literature has showed the effectiveness of mHealth interventions in improving disease management, adherence, 4 quality of life, 5 and function. 6
Despite the advantages of mHealth, widespread acceptance and adoption are limited, especially in resource-limited countries. 7 Many factors influence the adoption of digital health interventions, spanning macro- (health policy), meso- (healthcare organization), and micro- (individual) levels. 8 Low user engagement is one of the major barriers in mHealth adoption. 9 Studies have reported factors influencing patient adoption of mHealth from patients’ perspectives.10,11 There is a knowledge gap for exploring doctors’ perceptions on their adoption of mHealth in clinical practice. Doctors’ acceptance and how they integrate mHealth into their clinical practice are critical to ensure successful adoption and sustainability.
A systematic review by Jacob et al., 2020 reported the social (e.g. senior management and hospital support), organizational (e.g. infrastructure, workload and workflow fit) and technological factors (e.g. ease of use, perceived usefulness, technical issues of the mobile technology) that influenced doctors’ adoption of mHealth tools, however most studies included originating from high-income countries, reveals a scarcity of research on mHealth adoption from the doctors’ perspective, especially in resource-limited countries. 12 This geographical and economic bias has resulted in a significant gap in understanding the unique challenges faced by doctors in resource-limited settings. Doctors in resource-limited countries struggle with issues like insufficient training, a lack of culturally adapted mHealth tools and technical difficulties in the field. 13 In contrast, healthcare systems in high-resource countries have achieved more seamless integration of mHealth into patient care.14,15 Addressing these disparities requires an in-depth understanding of doctors’ clinical experiences and perceptions of mHealth, as this knowledge is valuable in developing targeted interventions to promote equitable mHealth adoption and utilization.
Research examining doctors’ attitudes towards mHealth adoption reveals a notable discrepancy: while doctors are supportive of mHealth with patients, most do not recommend or prescribe mHealth to their patients.16,17 Similarly, a study in Malaysia showed that primary care doctors use mHealth to support their clinical decision-making, help make a clinical diagnosis but rarely adopt mHealth with patients to improve patient education and support self-care. 18 It has been found that 98.4% of the Malaysian population owned a smartphone in 2023, 19 yet the adoption of mHealth is not common. To address these research gaps, this study focuses on exploring primary care doctors’ perceptions and experiences in adopting mHealth with their patients. Understanding their perspectives and real-life clinical experiences in adopting mHealth can inform strategies to improve mHealth adoption in primary care settings.
Methods
This qualitative study used a semi-structured interview method. We used an interpretive description approach to inductively explore the understanding of the perceptions, experiences and challenges of primary care doctors (PCDs) in adopting mHealth with their patients. Interpretive description is an inductive analytic approach used to investigate and understand a clinical phenomenon of interest by capturing the emerging themes and patterns within subjective perceptions. This approach allows us researchers, to explore the meanings and explanations that could inform changes in clinical practice. 20 We reported the findings of this study as per the Consolidated Criteria for Reporting Qualitative Studies (COREQ) (Supplementary material).
The study was conducted in a public primary care clinic located within a university hospital setting between December 2020 and March 2021. The clinic, a fee-subsidized clinic, is in the urban city of Kuala Lumpur, Malaysia. It has a total of 61 primary care doctors: 38 clinical trainees, 23 family medicine specialists and 3 service medical officers. We included primary care doctors who had been actively practicing in this clinic for at least 6 months. We used a maximum variation sampling method to purposively sample participants from different gender, ethnicity, age groups, professional position, and years of experience. This sampling method allowed researchers to obtain a heterogeneous sample and have a better understanding on the mHealth adoption phenomenon. 21 Recruitment was stopped when data saturation was reached, where no new themes emerged from additional interviews. A study by Braun et al. (2021) reported that 12–16 interviews were adequate to reach data saturation for thematic analysis. 22 Figure 1 shows the flowchart of recruitment.
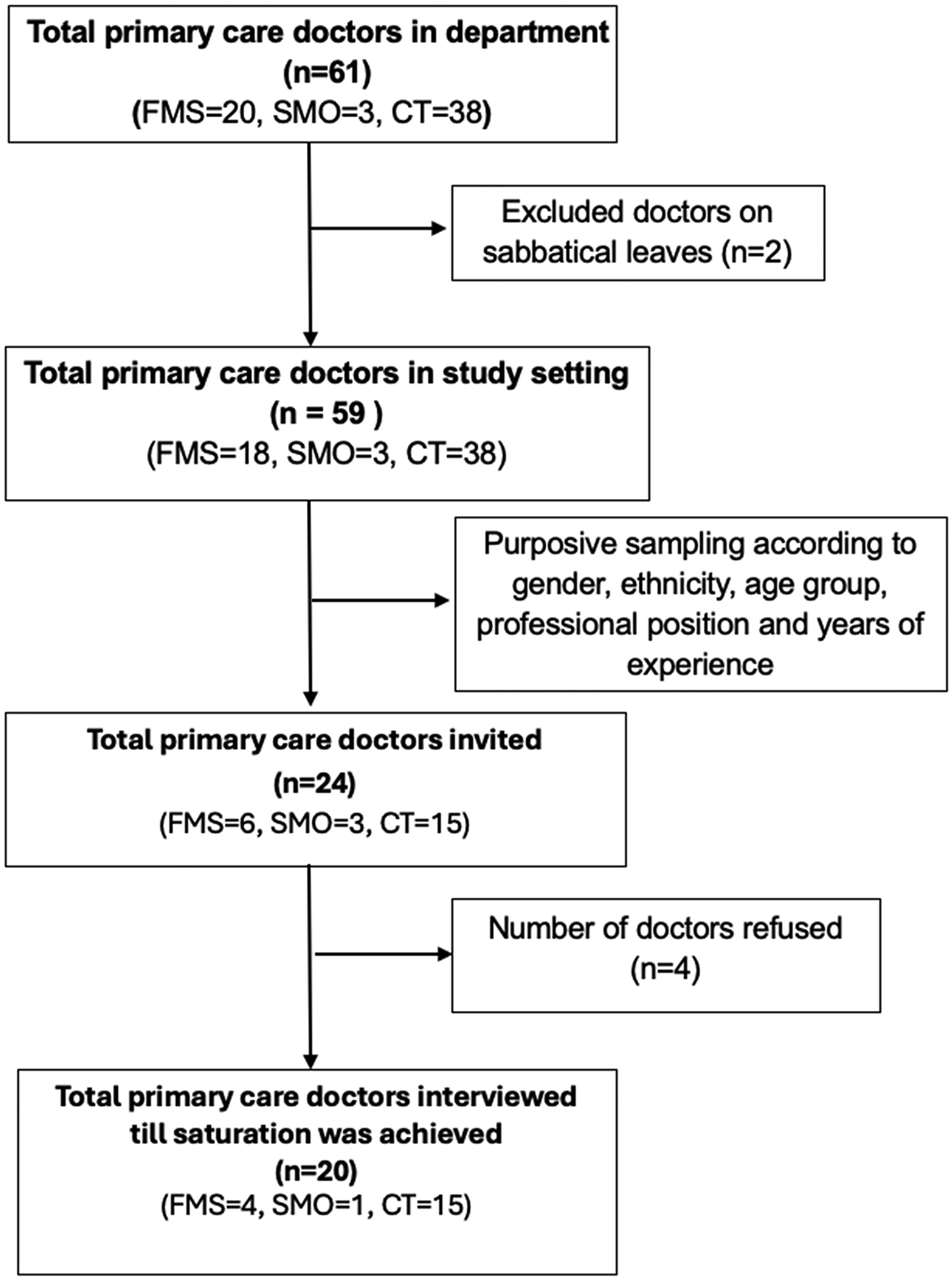
Flowchart for recruitment. FMS, family medicine specialist; SMO, service medical officer; CTs, clinical trainees.
We developed an interview guide (Supplementary material, Table S1) based on the Decomposed Theory of Planned Behaviour by Taylor and Todd (1995b). 23 We used the behaviour-centred framework to assess the behaviours of the primary care doctors, exploring their views, experiences, barriers and facilitators. The framework comprises of three main components (attitude, subjective norm and perceived behavioural control) which influence an individual's intention to use or adopt a resource. This framework integrates aspects of the Technology Acceptance Model (TAM), predicts user intentions by considering factors such as perceived usefulness, ease of use, social influence, and facilitating conditions. We obtained the list of primary care doctors from the clinic. Eligible participants were approached via email and phone messaging. Subsequently, participants who fulfilled the inclusion criteria were invited to participate in this study. An appointment for the online interview was made at a date and time that was convenient for the participants. All the interviews were conducted virtually via the Microsoft Team application due to COVID-19 pandemic restrictions. After explaining about the objectives and nature of this study using a participant information sheet, informed consent from participants who agreed to participate in this study was obtained. Participants were assured that they could withdraw from the study at any time.
During the interviews, researchers explained the scope of mHealth, which includes applications and websites for patient use and patient education, teleconsultation, telemonitoring, patient decision tools, appointment apps, navigation apps and professional websites for doctors. The participants were asked to describe their views on adopting any mHealth with patients, experiences they have encountered when adopting mHealth with their patients and how their previous experiences influenced the adoption of mHealth with patients. IGV (MBBS) with a background of being a junior doctor, perceived mHealth as being beneficial to both doctors and patients. IGV has attended trainings on qualitative research methodology and has experience in conducting and publishing qualitative research. HML (PhD), CJN (PhD) and YKL (PhD) are academicians and experienced qualitative researchers. They regularly conduct trainings on qualitative research methods. The first two pilot interviews were conducted by IGV under the supervision of HML. The interview guide was revised with more open-ended questions to be able to prompt more responses to doctors’ views and experiences to adopting mHealth with their patients. All subsequent interviews were conducted independently by IGV. All interviews were conducted between participant and researcher only. All the interviews were conducted in English, lasted for 30–60 minutes and notes were taken throughout the interviews. The transcripts were not returned to the participants. All interviews were video- and audio-recorded and stored in a single encrypted laptop. The video recordings were not used for the analysis. We stopped the recruitment when data saturation was reached where no new themes emerged from interviews.
Data analysis
All the recordings were transcribed and checked by the researcher (IGV) herself. A thematic analysis approach was used to analyse the data.22,24 Firstly, two researchers (IGV and HML) read and re-read the first two transcripts to familiarize themselves with the interview content. The transcripts were then coded by two researchers (IGV and HML) independently. Researchers IGV, HML and CJN met to discuss the codes and develop a coding framework (Supplementary material, Table S2). Subsequently, IGV coded the remaining transcripts. All the researchers (IGV, HML and CJN) met regularly to discuss codes and discrepancy. After coding, researchers sorted and merged the codes to form categories and subsequently themes from the data. The themes were then reviewed with another researcher (LYK) in the team. Atlas.ti version 8 was used to manage and analyse the qualitative data (Atlas.Ai).
Results
A total of 20 participants (4 family medicine specialists, 15 family medicine trainees, and 1 medical officer) participated in the interviews (Table 1). The participants’ practice experiences in primary care clinics ranged from 4 to 23 years of experience.
Participants’ demography (n = 20).

FMS are primary care physicians who supervise and train the FMT and SMO; FMTs are clinical trainees under the 4-year Masters of Family Medicine Program; SMOs are medical officers who provide clinical service in the clinic.
Five themes emerged regarding the use of mHealth by the primary care doctors: perceived benefits of adopting mHealth with patients, doctors’ approaches to facilitating mHealth use and adoption, identifying credible mHealth resources, selecting patients to adopt mHealth, and privacy concerns when delivering mHealth.
Theme 1: Perceived benefits of adopting mHealth with patients
Doctors expressed a positive view of mHealth as beneficial for patient self-care and empowerment. Doctors observed patients gained a better understanding of their health conditions by improving patients’ knowledge about diseases and treatments using mHealth. I find the patients actually appreciate it (mHealth) and they understand better, and it also conveys my message to them clearer. [P2,36-year-old, family medicine trainee]
Using mHealth for self-monitoring provided patients with the autonomy to manage their diseases themselves, rather than waiting for their next doctors’ visits. Doctors acknowledged that using mHealth can enhance patient–doctor communication. They found it easier to advise and convince patients with the assistance of mHealth, which also indirectly shortened consultation times. Doctors expressed that using mHealth as a disease monitoring tool facilitates discussion between doctors and patients. …in disease monitoring, it's self-empowerment for the patients as well. (For example) Sugar monitoring, you’re encouraging self-management of the patient. [P11, 36-year-old, family medicine specialist] When patient has this app where they do it as a routine monitoring and they come for their follow up, they can just show us the app and then we can interpret the results, and it helps to facilitate a more proper discussion between the physician and the patient. [P1, 26-year-old, family medicine trainee]
Theme 2: Doctors’ approaches to facilitating mHealth use and adoption
There is a significant variation on how different doctors recommend or prescribe mHealth to their patients. Figure 2 describes a range of approaches and related levels of effort in adopting mHealth with their patients. Some doctors who were busy and had limited time during consultation would merely ‘tell’ their patients about the available mHealth resources and information during consultations or point out the resources that they would like patients to read after their appointments (minimal effort). I'll open on the spot the website on allopurinol and gout, and just tell them this is gout, and this is allopurinol's function. I'm not giving A to Z the info, I'm just saying. [P17, 35-year-old, family medicine trainee]
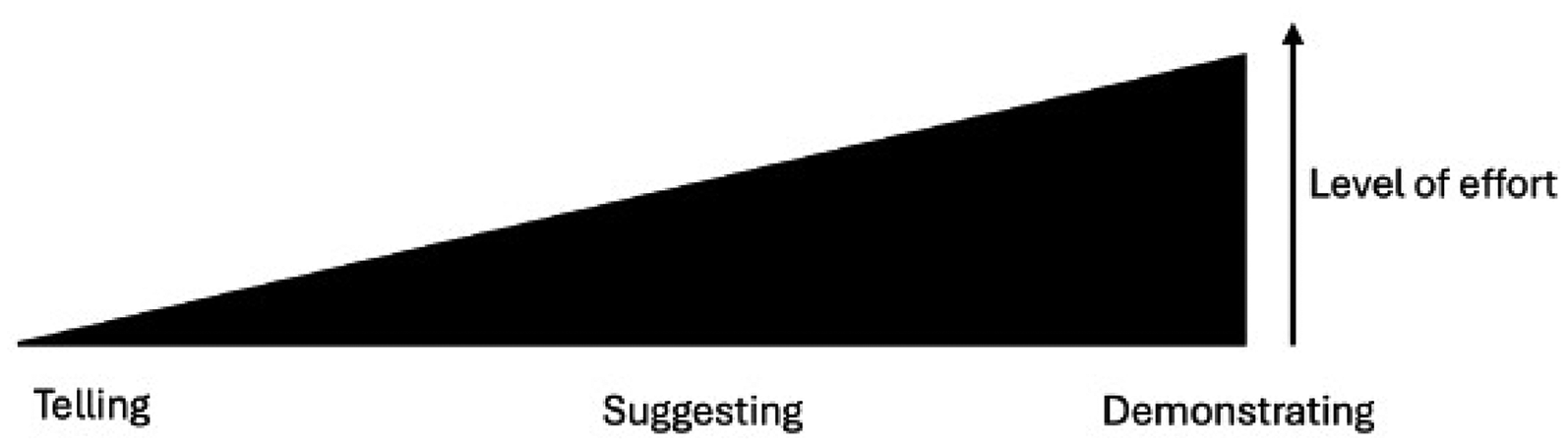
Range of approaches and levels of effort in adopting mHealth with patients.
Some doctors invested more effort in suggesting mHealth resources to their patients, tailored to patients’ specific health conditions, expecting patients will adopt them. Some took extra steps by providing patients with written link and resources to access (medium effort). I refer to the phone and write it. I just YouTube and then write the link or the name of the video that they have to search for. I don't go step by step. [P6, 35-year-old, family medicine trainee]
A few doctors invested more time during consultations, took additional efforts and initiatives by demonstrating to patients on how to use the mHealth resources during clinic consultations. They provided step-by-step guidance, starting from downloading or searching for the mHealth apps and resources, to effectively utilizing them for patient benefit. One doctor even compiled a list of patient resources and shared it with patients to facilitate easier access. Some doctors proactively sought feedback from patients after they used mHealth tools (maximal effort). I collect brochures and leaflets in a soft copy. I have a compilation of PDFs in my drive, in which I usually create a shortened link, and then whenever a patient comes, who fits the criteria for me to use the leaflets, I just pass them the link. [P5, 32-year-old family medicine trainee]
Theme 3: Identifying credible mHealth resources
Doctors face difficulty in finding high quality mHealth resources and are uncertain about its credibility which contributed to the challenges in adopting mHealth during their clinical consultations. Doctors pointed out that the abundance of available resources complicated their search for reliable and mHealth resources. And I, I think I am not aware of any app that we can offer to patients. So, I have not been offering here. [P20, 39-year-old, family medicine specialist] I myself also don't know whether the apps are real and then is it evidence-based medicine or not, so I kind of afraid to suggest who knows they give the wrong info and then the patient trust and then I get into trouble, I because I’m the one who suggested. [P16, 34-year-old, family medicine trainee]
Besides reliability, localization was also raised as doctors described that some of the mHealth resources failed to align with local cultural norms. Their concerns about the reliability and credibility of mHealth resources available for patient use led to hesitation in adopting mHealth with patients. Ah yes, we never had any app that is Malaysia-based to be widely used. So, if you have a Malaysian in-house apps, then maybe everyone can start using and the information we (doctors) are going to give is more of a Malaysian-based and local community-based. [P17, 35-year-old, family medicine trainee]
Some doctors suggested that training and continuous medical education (CME) could address these challenges by improving awareness and knowledge of available mHealth for patient use. Such training would increase their confidence in recommending and adopting mHealth effectively with patients. Well, you know, we can have teaching sessions, we have CMEs… if primary care physician whose interest is in this (mHealth), and who knows a lot of mobile health to be shared and recommended to patients, then probably can have a session or just write down a list for us to go through. [P20, 39-year-old family medicine specialist]
Theme 4: Selecting patients to adopt mHealth
While it was generally easier to adopt mHealth with younger patients, doctors mentioned that they would frequently use mHealth with older patients on the condition that they were tech-savvy and had higher literacy levels. Nevertheless, doctors noted that patients who were highly motivated to learn about mHealth were willing to use it regardless of their age. Doctors also took into account patients’ family support when considering mHealth adoption. Doctors recommended mHealth use in older patients who have good family support in helping patients navigate the adoption process. Of course, the age, you do know that younger (patients), they are more tech-savvy, they will know how to use their phone well, but the more important thing is whether they have awareness. If elderly patients have a good health awareness, it will not be a problem…. They will automatically learn how to use mobile apps, be it the elderly patients. [P1, 36-year-old family medicine trainee] I think there are some elderly patients who have support at home, those with children. I write on a piece of paper and then let them show the piece of paper to their children so that they can help them to look up these materials. [P20, 39-year-old, family medicine specialist]
Theme 5: Privacy concerns when delivering mHealth
Doctors expressed worries about the potential breach of their own personal information when demonstrating mHealth to patients when using their own mobile devices. For example, they pointed out the possibility of receiving personal message notifications and calls when demonstrating a health app or websites. We are scrolling through the mobile phone to them, we have some WhatsApp messages coming in and then someone calls … discouraged me from showing and revealing my personal things to them (patients). [P17, 35-year-old, family medicine trainee]
Doctors also expressed concerns regarding patient privacy particularly when adopting mHealth with people living with HIV (PLHIV). For instance, a doctor who used their personal mobile phones for teleconsultation through voice call with PLHIV to discuss treatment options, voiced worries about the potential leak of patients’ personal data and confidentiality breaches during the call. Thus, they have a specific phone to speak to PLHIV during their consultations as an act in protecting patients’ confidentiality. For example, we do have specific phones for retroviral disease patients, so everything is confidential. [P16, 34-year-old, family medicine trainee]
Discussion
Our study uncovered practical experiences and challenges PCDs encountered when adopting mHealth with patients. Our findings revealed substantial gaps in the knowledge and skills of PCDs concerning the adoption of mHealth with their patients, particularly identifying credible mHealth resources and practicing effective ways to deliver mHealth. While there are concerns about patient data privacy, our study surfaced doctors’ personal privacy issues during the process of delivering mHealth.
In this study, doctors perceived mHealth as beneficial to their patients. mHealth was useful for patients’ self-care, empowerment and patient–doctor communication. Similarly, a study in France showed that primary care doctors believed mHealth to be beneficial to their patients as it strengthened patients’ involvement in managing health. 25 Doctors have positive attitudes towards mHealth use in promoting patients’ self-care especially in lifestyle modification and treatment monitoring. 16 A qualitative study by Sze et al. conducted among Singaporean primary care doctors showed that PCDs share a positive view that increasing interactions between doctors and patients via virtual consultations improves communications. 26 Online health information access by patients via mobile phones could enhance the patient–doctor relationship through fostering shared decision-making. 26
Our study revealed an interesting practice on how PCDs deliver mHealth to their patients, highlighting a wide variation of approaches and efforts in adopting mHealth. This phenomenon may result from varying attitudes among PCDs towards the adoption of mHealth with patients. Our findings echoed a study by Schroeder et al., 2023 which showed that some doctors perceived motivating patients to use mHealth as not being their responsibility; while they were willing to offer mHealth tools, they were hesitant to invest more time and effort in persuading patients or demonstrating the app functions during consultations. 27 Another study found that doctors’ variable approaches to delivering mHealth were influenced by patients’ digital literacy, patients’ receptiveness to use mHealth and time constraints during consultations. 28 Our study highlighted the need to enhance support for PCDs to effectively integrate mHealth into clinical practice. Evidence from a scoping review suggested that identifying committed support staff as change agents and offering technical support and supervision are critical implementation strategies to improve mHealth adoption in resource-limited settings. 7 For instance, involving nurses or allied staff to assist when patients agree to use mHealth but require further guidance could alleviate PCD's time constraints. Such measures could reduce inefficiencies and improve the delivery of mHealth interventions in clinical practice.
PCDs in our study encountered challenges in identifying credible and culturally adapted mHealth resources for patients, uncovering a knowledge gap and a lack of confidence of PCDs in accessing, evaluating and prescribing mHealth resources. Our findings aligned with other studies showing limited awareness and unfamiliarity with evidence-based mHealth resources as barriers to mHealth adoption.29,30 These findings emphasized the need for strategies to support PCDs in adopting mHealth with patients, such as training programs on evaluating mHealth apps using standardized assessment tools, developing a repository of credible mHealth resources for common diseases in primary care and increasing the dissemination of evidence-based and culturally adapted mHealth initiatives.
Our study highlighted the privacy concerns PCDs encountered when implementing mHealth in a resource-limited setting where formal mHealth infrastructure is lacking and PCDs resort to using personal devices to bridge gaps in delivering mHealth services. PCDs expressed their uneasiness about having to use their personal phones to show the apps to patients. Our findings echoed a systematic review showing that providing teleconsultation services using personal mobile phones increased the risk of privacy and confidentiality breaches, especially in vulnerable populations. 31 To mitigate these risks, healthcare institutions should ensure access to secure telehealth platforms and designated infrastructure, while also providing training for doctors on data protection and privacy measures. In resource-limited settings, it is crucial to find ways for mHealth integration which minimizes privacy risks for both patients and healthcare providers. 32 Clear guidelines for the use of personal devices for clinical care are essential for upholding patient confidentiality and privacy.
In our study, PCDs recounted their experiences in patient selection and implementing mHealth with older patients, emphasizing the crucial role of family and peer social support in technology adoption. Social support can increase the motivation of mHealth adoption and enhance technology learning in older patients. 33 When engaging older patients in mHealth use, we should actively identify social support and guidance from younger family members, such as children and grandchildren. This is especially pertinent in Asian contexts, given the prevalence of intergenerational households. 34 Meanwhile, support from allied health providers can be considered for older patients with limited social support. 35 Older patients face challenges with mHealth adoption because of limited digital literacy, complexity of mHealth apps and limited physical capabilities. 36 Our study reported that tech-savviness is one of the factors PCDs considered when selecting patients for mHealth use. While there is a need for increased digital literacy training, it is essential for mHealth app designs to be tailored to the needs of older patients, including the use of larger font sizes, high contrast between text and background, consistent layout, and considerations for cognitive load and interaction. 37 These findings are consistent with other studies that mentioned with good social support from family members and a well-designed application interface, older adults could overcome challenges faced with mHealth and improve the feasibility of mHealth adoption.38,39
The strength of the study was that most of the participants practiced in both hospital-based outpatient clinics and government health clinics as part of their clinical training program. Thus, they have broader and richer experiences of mHealth practice in both settings. This study has several limitations. It was conducted in an urban academic primary care setting where patients and doctors have higher chances in being exposed to mHealth interventions initiated by the university hospital. This led to exploring views and experiences of PCDs who were mHealth users as compared to capturing PCDs’ views of non-mHealth users and the barriers pertaining to PCDs who were not mHealth users. PCDs in this study were from a single primary care setting; however, most of the PCDs have experience practicing in other governmental primary care clinics in urban and suburban regions which improves the transferability of the study findings. Further research can be conducted in rural area and private practices in Malaysia. This study was conducted during the COVID pandemic period when there was an increase in the implementation of mHealth interventions for COVID contact tracing and monitoring which potentially influenced the views and challenges faced by PCDs. The majority of participants in this study were trainees with 10 years or less experience. This is because this study was conducted in an academic-institution-based primary care setting where most doctors are trainees in the primary care medicine department. In Malaysia, the majority of primary care services are provided by doctors and clinical trainees as there are few family medicine specialists in Malaysia (estimated 900). 40 Thus, findings of this study mainly mirror the group of trainees which acts as a setback in minimizing the range of exploration.
Conclusion
This study provided insights into the facilitators and challenges faced by PCDs during the integration of mHealth in real-life primary care practice. Targeted efforts for PCDs on addressing issues, such as privacy concerns and identifying validated mHealth resources, should be considered for effective mHealth adoption with patients. Although PCDs generally support mHealth use with patients, lack of knowledge and support from the healthcare system have influenced their effort and willingness to adopt mHealth. Training is needed to improve healthcare providers’ knowledge and skills in adopting mHealth with patients. Organizational support is essential to improve the technology infrastructure to ensure the privacy of both patients and healthcare providers. Further research should explore effective ways to improve PCDs’ skills and confidence in delivering mHealth and integrating mHealth into clinical consultations.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251347850 - Supplemental material for Exploring primary care doctors’ perceptions and experiences in adopting mHealth with patients: A qualitative study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251347850 for Exploring primary care doctors’ perceptions and experiences in adopting mHealth with patients: A qualitative study by Indra Gayatri Valliyappan, Yew Kong Lee, Chirk Jenn Ng and Hooi Min Lim in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251347850 - Supplemental material for Exploring primary care doctors’ perceptions and experiences in adopting mHealth with patients: A qualitative study
Supplemental material, sj-docx-2-dhj-10.1177_20552076251347850 for Exploring primary care doctors’ perceptions and experiences in adopting mHealth with patients: A qualitative study by Indra Gayatri Valliyappan, Yew Kong Lee, Chirk Jenn Ng and Hooi Min Lim in DIGITAL HEALTH
Footnotes
Acknowledgements
We thank the clinical staff of the Department of Primary Care Medicine, Universiti Malaya Medical Centre for their assistance during data collection.
Ethical considerations
Ethical approval was obtained from the University of Malaya Medical Centre Medical Research Ethics Committee (MREC 2020102–9123).
Author contributions
IGV contributed to the conceptualization, methodology, research tool development, data collection, data analysis and drafting the manuscript. CJN and HML contributed to conceptualization, methodology, research tool development, data analysis, supervision, and critically reviewed and edited the manuscript. YKL contributed to data analysis, supervision and critical review of the manuscript. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Guarantor
HML.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.