
Abstract
Objectives
Indoor navigation systems (indoor positioning systems) can improve orientation for patients in hospitals and help employees to track assets. Many hospitals would like to implement indoor positioning systems but do not know how. To support them in doing this, and to gain knowledge about the requirements for indoor positioning system implementation, our research identifies the design criteria relevant to indoor positioning system implementation projects.
Methods
A design science research process is built to design and evaluate an artifact. For this, five indoor positioning system developers and five hospital IT management representatives from various hospitals and companies in Germany are interviewed. Further, controlled experiments are conducted in Germany, using an ultrasound-based indoor positioning system.
Results
We determined and tested indoor positioning system functions, evaluated indoor positioning system performance criteria, and identified the operating conditions in hospitals. Our results show that indoor positioning system functions should provide a benefit to a hospital's daily operations, that some performance criteria are more important than others, and that operating conditions are important, e.g., radiation.
Conclusion
As a theoretical contribution, we show how design science research can be applied to the context of indoor positioning systems in hospitals. In addition, we make a practical contribution in that our propositions can be used for future indoor positioning system developments.
Keywords
Introduction
Indoor positioning systems (IPSs) are important forms of information in hospitals as they allow visitors, patients, and doctors to better travel through space, thus reducing navigation times, avoiding unnecessary detours, and contributing to an increase in hygiene. 1 Improved navigation is especially important for hospitals that experience many non-frequent visitors and patients, have technical devices spread throughout the hospital, have large building structures, and have changeable layouts as rooms are booked for different purposes. While IPS is available for use, the overwhelming majority of hospitals have not installed an IPS, though many are interested in doing so. 2 However, alongside the issue of finances, a critical problem is how to implement the system into a hospital environment. 3
Existing research on IPSs has shown that several evaluation criteria have to be considered when IPSs are developed and maintained.3,4 Additionally, previous studies have carried out case studies of IPSs in hospitals
5
and identified the requirements of stakeholders.1,6 Thus, existing knowledge can be used to design and develop an artifact according to design science research7,8 that aims to facilitate future IPS implementations. Based on the above, we pose the following research question: Which factors are relevant to design and demonstrate an artifact that facilitates future IPS implementations?
To address our research question, we apply the design science research process based on Peffers et al. 8 and the design science project grid according to vom Brocke et al. 9 to the context of IPSs in hospitals. Our results show that the functions, performance criteria evaluation, and operating conditions of IPSs are important to consider for implementation projects in hospitals. Thus, we contribute to theory and practice by proposing an artifact that shows that design science research is applicable to the context and also defines certain requirements for IPSs in hospitals.
The remainder of the paper is organized as follows: The ‘Theoretical background’ section describes the theoretical background of our study, the ‘Method’ section outlines the method used for our research, the ‘Demonstration’ section describes the application scenario, and the ‘Results’ section presents the results. The ‘Discussion’ section discusses the results and the limitations of our work. Finally, the ‘Conclusion’ section describes implications and future research directions.
Theoretical background
Indoor positioning systems
IPSs determine the location of an individual or asset through an algorithm that analyzes specific signals. To do so, several technologies can be used, such as satellite-based, magnetic-based, sound-based, vision-based, or radio frequency-based IPSs. While every technology has its own advantages and disadvantages (for detailed information on this, see3,4), radio frequency-based approaches, such as Bluetooth low energy (BLE) or wireless-fidelity (Wi-Fi) are widespread, since radio frequency signals can be processed by various devices.3,4 Further, more recent technologies than BLE and Wi-Fi, such as LoRa, are used to investigate their sufficiency for indoor positioning purposes. 10 LoRa is a low-bandwidth, low-power, and long-range wireless wide-area network that is popular for Internet-of-Things purposes that is accessible by various devices. 11 Additionally, studies state that LoRa performs better for IPS purposes than Wi-Fi and BLE do.10,11 Alongside the technology used, the algorithm of an IPS employs various methods for determining position, such as using the strongest signal (received signal strength indication (RSSI)) or by measuring angles from phase differences of the signal. Additionally, IPSs can be either device-based or monitor-based, with device-based systems typically used for navigation and monitor-based systems for tracking. 3
IPS evaluation
Liu et al. 4 and Zafari et al. 3 identified key criteria for evaluating IPSs: accuracy, availability, cost, energy efficiency, latency/delay, precision, reception range, robustness, and scalability. Accuracy, measured in meters (m), refers to the degree of location measurement precision. Availability is determined by whether existing hardware, such as smartphones, can process the signals used by the IPS or if additional hardware, such as tags, is required. Low cost is desirable, with few or no additional hardware needed for proper IPS operation. Energy efficiency is important to prevent draining device batteries. Latency/delay should be less than one second to ensure real-time location tracking. Precision describes how well IPSs fulfill their intended tasks. Reception range should be greater than 10 m to ensure adequate signal coverage. Robustness is critical, with the IPS expected to remain functional even if certain measurement points fail. Scalability should be tested with multiple devices and operating systems. These criteria are important for assessing IPS performance.
Related work
Wichmann 5 presented a scoping review of IPS approaches in hospitals. After gathering existing IPS technologies, Wichmann 5 evaluated 38 IPSs concerning their performance in hospital settings and highlighted several objectives for IPSs in hospitals. A selection of these is shown in Table 1.
Objectives of indoor positioning systems (IPSs) in hospitals based on Wichmann. 5

To ensure that our analyses are current, we further report on two more recent studies that were not included in the scoping review of Wichmann. 5 First, Vladislav and Marina 23 developed a Wi-Fi-based IPS using RSSI to determine position. They aimed to solve the problem of high noise in RSSI measures by using a probabilistic-based method and a neural network method. Second, we consider the study of Booranawong et al., 24 who also developed a Wi-Fi-based IPS. They investigated this using two reference nodes in order to track in real time a moving target in an indoor corridor of a hospital building. Further, several prior studies have determined user requirements concerning IPSs in hospitals. First, Anagnostopoulos et al. 6 gathered navigational needs and requirements of hospital staff in Geneva University Hospital as a use case. As the most important requirements, their participants proposed that IPSs should be easy to use and provide benefits to daily work in the hospital. 6 Second, Wichmann and Leyer 1 surveyed hospital visitors and employees concerning their intention to use IPSs in hospitals, as well as their requirements of IPSs. They determined that both hospital visitors and employees intended to use IPSs in hospitals. Further, Wichmann and Leyer 1 supported the proposition of Anagnostopoulos et al. 6 that hospital employees have to find benefits to daily hospital work in order to regularly use IPS. Combining these factors—i.e., IPS objectives, industry approaches, and user requirements—comprise the basis of design functions for IPSs in hospitals. Alongside IPS functions and performance evaluation, Zafari et al. 3 stated that the operating conditions of IPSs should be considered. Specifically, they referred to the need to improve IPS algorithms to suppress multipath effects and noise (e.g., as different sources of radiation/magnetic waves in one building might influence IPS signals). IPSs in hospitals should address such issues.3,4
Method
Design science research
Originating from engineering and sciences of the artificial, 25 the design science research paradigm was introduced to information systems by Hevner et al. 7 in 2004. Design science research seeks to enhance human knowledge by providing guidance for creating innovative artifacts and design knowledge to solve real-world problems. In 2006, Peffers et al. 8 contributed to the field by providing a process for design science research that stems from certain use cases in which design science has been used to develop an artifact. This design science process is illustrated in Figure 1.

Design science research process according to Peffers et al. 8
In the meantime, design science research has become an important method for the development of information systems. 8 While there have been various design science research projects, they are categorized as contributing to either (1) design entities, (2) both design entities and design theory, or (3) design theory without addressing a design entity in the same project. 9 Further, and for new design science research projects, a grid was introduced to report on those projects. 9 Concerning this grid, vom Brocke et al. 26 proposed six core dimensions of a design science research project that have to be addressed: (a) problem, (b) research process, (c) solution, (d) input knowledge, (e) concepts, and (f) output knowledge. vom Brocke et al. 26 proposed several suggestions for correctly reporting on design knowledge. First, design science research projects must be positioned properly. This means that they should explicate the relevant problem focused on in the research, as well as the solution being designed or investigated, and evaluate how the problem and solution are related. Second, design science research projects must be grounded sufficiently in existing research. Processes for and results of searches on contexts related to the contribution must be reported, while the knowledge gained should be defined as either propositional or prescriptive in terms of design theory or design entities. Third, aligning of the design science research project is important. The project needs to be transparent and the authors should ensure that it is appropriate by explaining the rationale of the design process. Fourth, design science research projects must include clarification of how they advance prior knowledge. Specifically, authors should discuss the projectability of, fitness of, and confidence in the comparability of their design knowledge to similar projects, and to better understanding directions for future research. 26
Design science research process for IPSs in hospitals
As proposed by Peffers et al., 8 the design science research process is sufficient to develop artifacts. Thus, we design a process for IPSs in hospitals as the overall method for this study, using the six process steps according to Peffers et al. 8 to evaluate an artifact—i.e., requirements for IPSs in hospitals. To do so, we use the evaluation methods for design science research proposed by Hevner et al., 7 meaning that we conduct expert interviews to improve IPS evaluation criteria determined by related work3–5 as an artifact. Further, we evaluate the artifact via controlled field experiments.7,27
Problem identification and motivation
Researchers must prove that the problem in question is of general importance and that there is a clear benefit of the artifact.7–9 Concerning IPSs in hospitals, the demand for such systems is high 2 and, though IPSs are being used in some hospitals,3–5 this use is not extensive. 2 Nonetheless, IPSs can provide certain benefits to hospitals, such as improving hygiene, facilitating daily work, and improving navigation processes, 5 which is why their implementation should be pursued.2,5
Objectives of a solution
For artifacts to be successful, a sufficient number objectives for the solution provided by the artifact should be defined.7,8 We thus refer to IPS functions, performance criteria evaluation, and operating conditions as important criteria for IPSs in hospitals, based on meta-analyses.3,4 Accordingly, we aim to design an artifact that provides evaluated IPS functions, performance criteria, and operating conditions to facilitate future IPS implementation.
Design and development
Liu et al. 4 proposed that IPSs can be helpful in emergency situations and departments, and Zafari et al. 3 stated that healthcare in general can greatly benefit from this technology. For instance, Zafari et al. 3 stated that IPSs are very important for treatment management in hospitals; for example, physicians could receive an alert message if a patient is in urgent need of help. However, while both studies stated that healthcare services can greatly benefit from IPSs, they did not outline specific functions for IPSs in this regard. Thus, we aim to determine these functions for IPSs in hospitals.
To evaluate IPS performance, Liu et al. 4 proposed several metrics by surveying existing systems. These metrics include accuracy, precision, complexity, robustness, scalability, and cost. Liu et al. 4 used these criteria to report on IPSs that use different technologies, such as Wi-Fi, BLE, and Infrared. Later, Zafari et al. 3 used these variables to perform a more recent survey of IPSs. They used some of the metrics proposed by Liu et al. 4 and added availability, energy efficiency, reception range, and latency/delay. They then evaluated IPSs using these metrics, similar to Liu et al. 4 More recently, to evaluate IPSs in hospitals, Wichmann 5 combined the criteria of Liu et al. 4 and Zafari et al. 3 Thus, to design and test new IPSs in hospitals, the following criteria should be used: (1) accuracy, (2) availability, (3) cost due to additional hardware, (4) energy efficiency, (5) latency/delay, (6) precision, (7) reception range, (8) robustness, and (9) scalability concerning devices (9a) and operating systems (9b).1,3,4
To evaluate performance criteria, controlled experiments7,27 and expert interviews7,28,29 are appropriate methods in design science research. Some performance criteria are more important than others due to the particular context of implementation in hospitals, 3 which we investigated using expert interviews. 28 These interviews were semi-structured, following the recommendations of Zowghi and Coulin 28 for requirement elicitation. The survey used (see Appendix) is mostly based on prior research. We used recommendations from Fishbein and Ajzen 30 for intention to use IPSs. Further, we investigate IPS evaluation criteria proposed by Liu et al. 4 and Zafari et al. 3 Additionally, we examine the IPS functions outlined by Wichmann. 5 To do so, we interview five IPS developers from different companies and five representatives of hospital IT management from different hospitals, all in Germany (henceforth referred to as “experts”). The selection process followed a convenience sampling approach, in which we contacted experts and included those who were willing to dedicate time to the interviews. Participants had two or more years of experience in their job. Additionally, we obtained verbal consent of our participants to use their statements for this study.
Further, to address the IPS evaluation criteria, we followed the procedure proposed by Wichmann. 5 Thus, we conducted controlled field experiments using the propositions of Rozum et al. 31 and Gerber and Green. 27 The experiment was conducted in Germany. We report on the respective criteria as follows: (1) Accuracy refers to the level of precision in localization results, measured in meters. (2) Availability is determined by whether the IPS utilizes signals that are readily available on common devices, such as smartphones. (3) To ensure a low cost of operation, no additional hardware should be necessary to run the IPS. (4) Energy efficiency is important for IPS performance, as the system should be designed to protect device batteries. (5) The latency/delay of the IPS should be less than one second to minimize localization errors and ensure real-time tracking. (6) Precision is concerned with the (relative) consistency of the system, as it measures the variation in its performance over multiple trials (vs. accuracy, which shows the [absolute] values of the mean distance errors of the IPS in meters). (7) Reception range indicates the range of the signal emitted by reference points, such as routers, and should be greater than 10 m. Higher ranges may result in lower accuracies but also lower costs, and vice versa. (8) To ensure robustness, IPSs should be designed to avoid errors and maintain operation even in the event of malfunctions. (9) Scalability is important so that it is easy to add new tasks or devices to the IPS. Testing with multiple devices (9a) and operating systems (9b) is recommended. 5 Alongside their evaluation of IPSs in hospitals, Zafari et al. 3 outlined the challenges of indoor localization and suggested solutions for this. They stated that IPS developers should not rely on techniques that improve IPS performance based on machine learning, since this will not improve IPS technologically. Instead, IPS developers should ensure that IPSs are robust, energy efficient, and use existing hardware infrastructure, such as Wi-Fi. 3 Further, IPS developers should consider environmental dynamics that have to be determined for certain contexts, such as hospitals. For example, multipath signals and noise have to be considered—e.g., by investigating radiation within the implementation environment. Further, IPSs are known to be error-prone if walls within the indoor environment are reinforced—e.g., using metal. 3 Hence, the operating conditions must be determined by addressing experts and their knowledge concerning these conditions using appropriate methods, such as expert interviews.3,4,7,28,29 The overall design science research process that we adopted according to Peffers et al. 8 is shown in Figure 2.

Design science research process for indoor positioning systems (IPSs) in hospitals (adapted from Peffers et al. 8 ).
Demonstration
To demonstrate our design artifact and to evaluate and generate new or improved IPS functions, performance criteria evaluations, and operating conditions, we present several methods that are appropriate for evaluation. To do so, we apply the design science research project grid from vom Brocke et al. 9 to the context of IPSs in hospitals. This grid is shown in Figure 3.
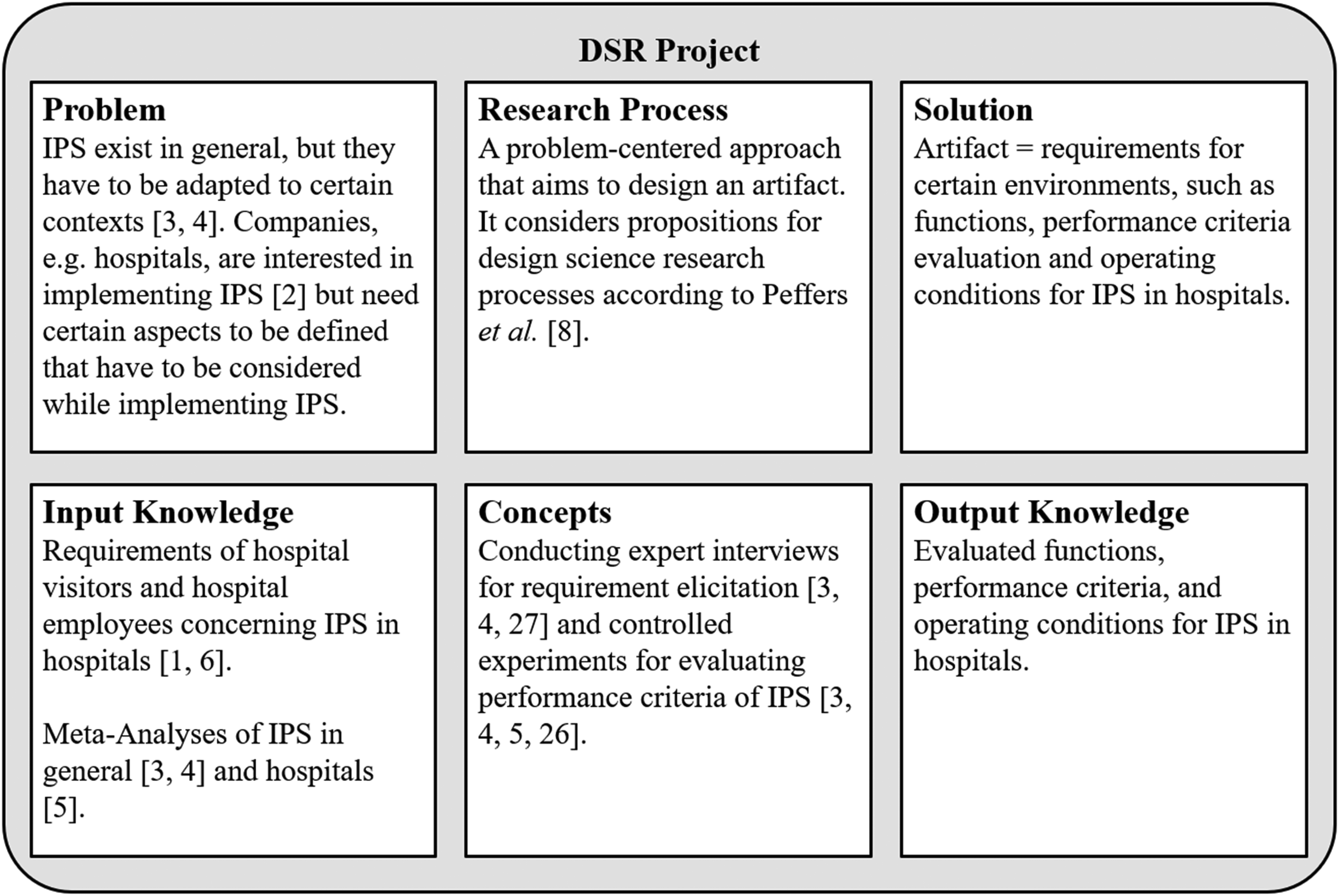
Design science research project grid for indoor positioning systems (IPSs) in hospitals (adapted from vom Brocke et al. 9 ).
IPS functions
First, we deduce IPS functions using the IPS objectives provided by Wichmann 5 and case studies.32–34 To do so, we use propositions for explication concerning narrow context analysis as defined by Mayring. 35 Table 2 provides our proposed functions.
Functions for indoor positioning system (IPSs) in hospitals (derived from Wichmann 5 ).

IPS performance criteria evaluation
We conducted controlled field experiments according to Gerber and Green 27 using an ultrasound-based IPS (as this type of IPS is quite precise, according to Zafari et al. 3 ) on two floors of a university building. For the experiments, the commonly used devices LG G8S ThinQ, HUAWEI Mate 8, and Sony Xperia X Compact, which have different built-in loudspeakers, were used. During the experiments, we tested two different scenarios concerning the loudspeakers (see “references nodes” in Zafari et al. 3 ). First, we used seven speakers to determine position. Second, we disabled three of them (see Figure 4). For position determination, we used acoustic signals from the loudspeakers and fingerprinted their RSSI (see3,4) as the localization technique. The fingerprinting was divided into two phases: An online phase in which fingerprinting mapping data were collected with a Huawei smartphone by traveling the hallways of each floor (i.e., eight times in total); and an offline phase, where the validation was realized. In the offline phase, the relative cross-correlation data (as the relevant IPS signal) were stored together with the position data that were acquired by the RPLidar 3 and Intel Camera T265 (see Figure 4). During the experiments, the cross-correlation was performed between the audio data that were recorded via smartphone and 27 IPS reference signals. Then, a vector was constructed from those 27 reference signals and three X-, Y-, and Z-positions were stored as fingerprint-mapping data. Accordingly, the IPS requires that the premises are pre-measured (e.g., via digital building maps) for proper operation. In the online phase, cross-correlation between the audio signals recorded by the smartphone and the 27 reference IPS signals was performed. Then, a “k nearest neighbor” (k = 1) algorithm (see 3 ) was used to determine the k IPS positions that were nearest in terms of fingerprint to the recently recorded audio. Further, weighting was applied to the k IPS signals to receive weighted IPS signal results and to improve IPS accuracy. 3 The experimental setup is similar to that used by Rozum et al. 31
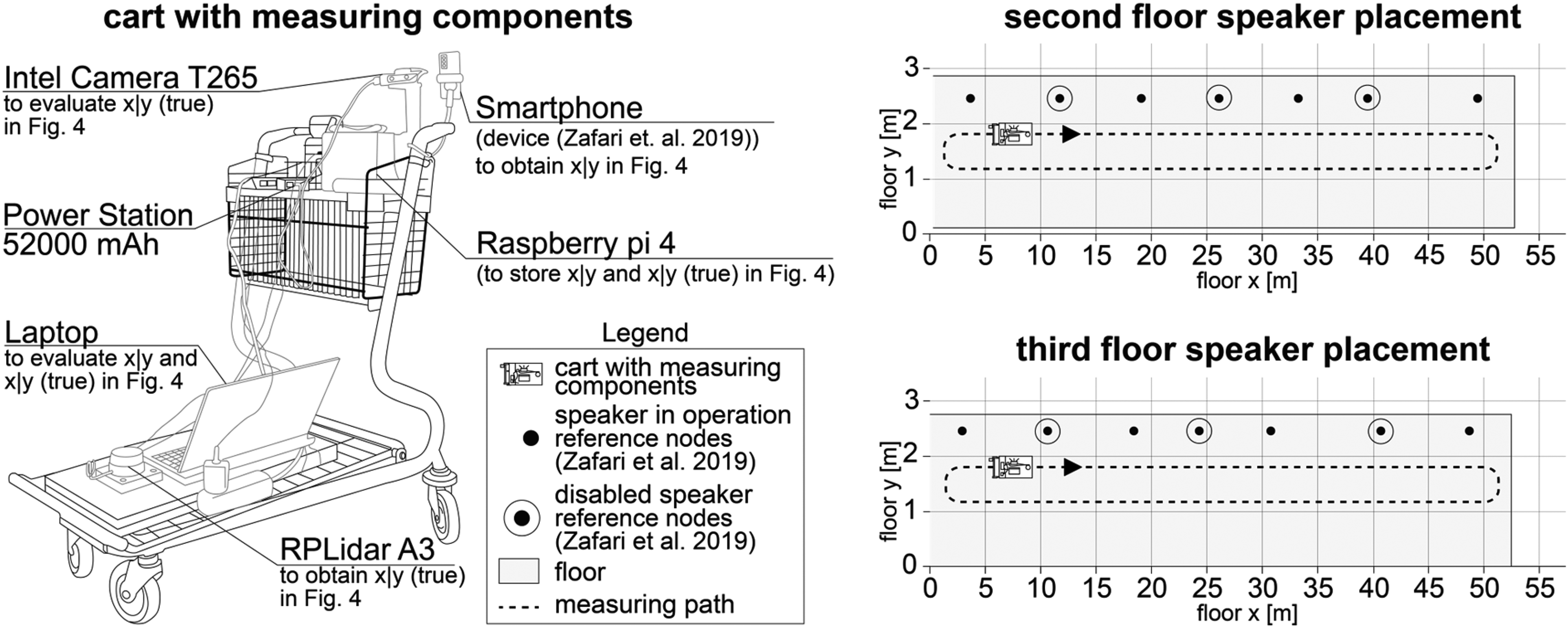
Experimental setup of ultrasound-based indoor positioning system (IPS).
IPS operating conditions
To evaluate IPSs in their respective contexts, Liu et al. 4 and Zafari et al. 3 proposed considering the operating conditions particular to each IPS. In particular, metals and liquids are known to significantly influence IPS signals.3,4 Thus, we aimed to verify such propositions for IPS in hospitals, and to determine further operating conditions that are important by conducting expert interviews using propositions for requirement elicitation. 28
Results
To present the results of our application scenario as a demonstration of the design science research process, 8 we evaluated our design artifact using various methods. Hence, we performed controlled field experiments following the recommendations of Gerber and Green. 27 Further, we conducted expert interviews considering the propositions of Zowghi and Coulin 28 for requirement elicitation.
Evaluation of controlled field experiments
The controlled field experiments 27 were conducted with three different smartphones on two different floors. As disabling three loudspeakers led to IPS failure, we are not able to provide results for this experiment. In the following section, the results for all seven speakers are described, beginning with IPS accuracy in Figure 5.

Experimental results for ultrasound-based indoor positioning systems (IPS).
In Figure 5, the green and red lines represent the actual distance that was ascertained by the Intel camera T265. The blue and orange lines describe the signals measured by the respective smartphones. The descriptives for Figure 5 are presented in Table 3. Root mean square error (RMSE) represents the standard deviation of the actual position measured by the tracking camera. The x accuracy refers to the length of the floor and y accuracy to the width. As two floors with speakers were considered, the accuracy percentage concerning the correct prediction of the respective floor over the total distance covered was also measured. Additionally, the overall performance of the experiment was determined.
Descriptives concerning experimental results for ultrasound-based IPS.

IPS: indoor positioning system; RSSI: received signal strength indication; RMSE: root mean square error.
Further, we evaluated our experiments using the enhanced evaluation criteria for IPS. We achieved an overall accuracy of 1.69 m using Gaussian filters. As we used ultrasonic audio for position determination that is processible by various smartphones, availability was good. Since we had to use loudspeakers for our controlled experiments, which might not be installed in all hospitals, we reported an additional cost. We are not able to report on energy efficiency, as our controlled experiments were performed in the early stages of our IPS development. The transmission of the ultrasound audio was latency-free, as it was issued continuously, resulting in low latency/delay. Regarding precision, the task for the IPS was to identify the correct floor, at which it succeeded for 99.9% of the experiment's distances. The reception range was low, as the loudspeakers were placed less than 10 m from each other (see Figure 4). The robustness was determined to be poor, as blocking the microphone of the smartphone (e.g., due to an incoming a phone call or carrying the smartphone in a pocket) led to excessive decreases concerning accuracy. As we used different smartphones for the experiments, scalability was high, but all of them were Android-based, resulting in a low scalability. Table 4 provides an overview of our results with regard to these criteria, compared to other studies evaluated by Wichmann, 5 Islam et al. 11 Vladislav and Marina, 23 and Booranawong et al. 24
Enhanced evaluation of IPS in hospitals.

IPS: indoor positioning system; BLE: bluetooth low energy; Wi-Fi: wireless-fidelity.
Evaluation of expert interviews
Evaluation of IPS functions
In order to evaluate our IPS functions, we asked our experts to assess whether each function needed an interface to another system that was not administered by the IPS. Table 5 provides an overview of the functions and assessments of our experts.
Evaluated functions for indoor positioning system (IPS) in hospitals.

Our experts stated that those functions that need interfaces might be cost-intensive to develop and hard to implement. Thus, they recommended avoiding implementing those functions that need interfaces in the first place, and instead focusing on those functions that do not require interfaces and thus are rather easy to implement. Therefore, our experts stated that IPSs in hospitals should contain the following functions as standard: A warning/alert function,16,40 a function for barrier-free navigation that also takes visually impaired people into account, 3 an emergency call function, 16 and functions that are specially adapted to the needs of older people (such as larger fonts). 19 From a technological point of view, the IPS should allow push messages. 18 Integrating contact-tracing functions 1 was deemed less important by all experts.
Evaluation of IPS performance criteria
We asked our experts to rank the IPS performance criteria according to importance. Most of the experts agreed that accuracy and availability are most important, and energy efficiency and scalability are less important evaluation criteria. The experts had differing assessments of precision (ranked as more important by the IPS developers, which was disputed by the hospital IT management); cost, latency/delay, reception range, and robustness were also disputed. Further, our experts recommended considering scalability in more detail: scalability should not only be considered by using multiple devices but by using different operating systems as well. Accordingly, we used the enhanced IPS performance criteria to report on our controlled experiments and to evaluate the IPS that were investigated by Wichmann. 5
Evaluation of IPS operating conditions
Regarding operating conditions of IPSs in hospitals, our experts stated that IPS signals could be influenced by radiation/magnetic waves and metallic shields, which are particularly relevant in hospital departments such as radiology, radiotherapy, and nuclear medicine. Basically, our experts argued that requirements for IPSs in hospitals should be determined and applied to IPS implementation projects as early and comprehensively as possible (e.g., with regard to possible structural changes, maintenance cycles, as well as the power supply of the IPS, for which power-over-ethernet should be used). Further, they argued that the generation of personal data by the IPS should be avoided as far as possible. If data have to be generated, a high security standard (e.g., AES-256) should be used. To comply with legal regulations (e.g., the EU-GPDR), the IPS servers should be operated in the same country as the IPS in the hospital. Support for the IPS should be online, remote, and based on both technical- (e.g., help with app crashes) and content- (e.g., missing representations of rooms) related issues. Concerning scalability, our experts recommended considering the most important smartphone operating systems (such as Android and iOS) and Web applications as platforms for the IPS. Further, the IPS should be cloud-based, backward-compatible (e.g., usable with smartphones issued within the last five years), and use responsive designs. In implementing the IPS, intensive testing of the system should be carried out (e.g., crowd testing, friendly user trial, i.e., testing the IPS within a company, but outside the IPS development department). The hospital should also inform its users (patients and hospital staff) about the use of the app.
Discussion
In terms of IPS functions, our expert interviews revealed that interfaces are important when initially implementing IPS in hospitals. Thus, our study contradicts extant research, in that functions such as treatment 36 and inventory management 22 should not be integrated in the initial stages. Nonetheless, considering the great demand for IPS in hospitals, those functions should be considered at later stages when updating an IPS that already has all the priority functions.
Concerning the evaluation criteria for IPS, our results reflect that accuracy and availability are more important, and we thereby confirm the propositions of Zafari et al., 3 who stated that accuracy and availability are fundamental requirements of indoor localization. In contrast, our experts deemed energy efficiency less important, countering the proposition of Zafari et al. 3 that highly accurate localization that is provided in real-time might drain the batteries of user devices, as well as of reference nodes (such as beacons or routers). The contrary propositions are probably related to the facts that, on one hand, the user devices are not of primary importance to our experts and, on the other hand, our experts rely on a power-over-ethernet connection instead of batteries for reference nodes, which has already been adopted by some companies in the IPS market. 32 Further, our experts confirmed the propositions of Zafari et al. 3 in that scalability is less important for localization using mobile devices. It is unsurprising that precision was evaluated differently by our experts, since it provides information about the functions of the IPS, which in turn allow conclusions to be drawn regarding the necessary complexity of the systems to enable the functions. 4 Thus, it is likely that the precision (and the resulting functions of the IPS) makes it easier for the IPS developer to design an optimum IPS for the hospital in question, 4 since, for example, current user requirements1,6 lead to certain functions for IPS.
As for our controlled experiments, our IPS performed similar to other technologies in terms of accuracy, availability, latency/delay, precision, and scalability. However, we used additional hardware, which is why we reported an additional cost. Further, the IPS performed poorly in reception range, robustness, and scalability compared to the IPS in Table 4. To counter high cost, Zafari et al. 3 recommended avoiding additional hardware; however, this is not suitable for our approach as additional reference nodes (such as speakers) are needed to emit acoustic signals. 3 Nonetheless, there is a need to improve our IPS algorithm to increase robustness, 4 and test this using different operating systems (e.g., iOS) to address scalability, as stated by our experts. Additionally, we determined that some studies and technologies, such as Islam et al. 11 using LoRa, performed better in most of our evaluation categories for IPS. Hence, we conclude that either our experimental setup and/or ultrasonic audio as technology are/were not the best solution for IPS investigations. As a major advantage of LoRa compared to ultrasonic audio, just one node is needed for an eight-story building leading to fewer IPS nodes and hence lower costs of LoRa IPSs’. 11
Regarding the operating conditions for IPSs in hospitals, our results support the proposition of Zafari et al. 3 that IPSs are highly dependent on the characteristics of the indoor environment, with our experts referring to the characteristics of hospitals. Further, our results support the need for cloud-based IPS, which Zafari et al. 3 recommended for high processing power and continuous power supply. Our findings also emphasize that compliance with applicable data policies, especially with respect to personal data, is very important, as also noted by Zafari et al. 3
As with any research, our study is subject to limitations. First, while we derived our IPS requirements as an artifact using design science research paradigms, using other methods, such as action research, could lead to different results. Thus, future research should conduct meta-analyses of different methods for requirement elicitation concerning IPS in hospitals. Second, while we interviewed German experts on their opinions of German hospitals, using similar experts from other countries could yield different results, especially where the state of hospital digitalization is different from Germany. Third, concerning our controlled experiments, further investigations could be carried out that focus on the signal processing of our algorithm to increase reception range and reduce the error-proneness of the algorithm, to improve robustness, and to ensure sufficient operation even if three speakers (i.e., reference nodes) are disabled. Fourth, we did not test the system in a quantitative manner, and hence our results are qualitative only. Quantitative analysis should be carried out in future work, especially when including real people in the design tests.
Conclusion
This study addresses requirements as an artifact for IPS implementation using design science research as the underlying theory. As requirements, we determined, demonstrated, and evaluated IPS functions, performance criteria, and operating conditions for such systems in hospitals. Thus, we conclude that design science research is appropriate for requirement elicitation concerning IPSs in hospitals. In terms of our controlled experiments, we conclude that our algorithm is sufficient for IPS purposes, as it effectively completed the task of floor prediction, showing comparable accuracy across several smartphones. Nonetheless, other technologies perform better and our algorithm is still error-prone and needs to be further investigated in terms of robustness.
On a theoretical level, our implications for healthcare information systems research are as follows. First, we provide propositions concerning design science processes and project grids regarding how to implement IPS in hospitals. Our insights reveal how both processes and grids can be adapted for IPS purposes and thus could be used in contexts other than hospitals. Second, we contribute to requirement elicitation research in that we show how to use design science research methods to determine requirements for IPS in hospitals. Further, our processes and grids concerning requirement elicitation could be used for other information systems implementation projects in hospitals, such as using virtual reality for rehabilitation measures. Third, we contribute to IPS research by enhancing and evaluating IPS evaluation criteria that can be used for future IPS performance evaluations in various contexts. Fourth, we determine new and verify existing operating conditions for IPS in hospitals that could be important for implementations in other contexts—e.g., museums and hardware stores.
On a practical level, we provide enhanced IPS evaluation criteria, as well as several IPS functions and operating conditions, which hospitals can use to evaluate their IPS. Likewise, IPS developers can benefit from this study by obtaining useful insights from other IPS developers, as well as hospital IT management. Further, both IPS developers and hospital IT management can benefit from insights concerning the requirements for such systems as defined by hospital visitors and employees.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241229148 - Supplemental material for Determining design criteria for indoor positioning system projects in hospitals: A design science approach
Supplemental material, sj-docx-1-dhj-10.1177_20552076241229148 for Determining design criteria for indoor positioning system projects in hospitals: A design science approach by Johannes Wichmann, Thomas Paetow, Michael Leyer, Bisrat Aweno and Kurt Sandkuhl in DIGITAL HEALTH
Supplemental Material
sj-xlsx-2-dhj-10.1177_20552076241229148 - Supplemental material for Determining design criteria for indoor positioning system projects in hospitals: A design science approach
Supplemental material, sj-xlsx-2-dhj-10.1177_20552076241229148 for Determining design criteria for indoor positioning system projects in hospitals: A design science approach by Johannes Wichmann, Thomas Paetow, Michael Leyer, Bisrat Aweno and Kurt Sandkuhl in DIGITAL HEALTH
Supplemental Material
sj-csv-3-dhj-10.1177_20552076241229148 - Supplemental material for Determining design criteria for indoor positioning system projects in hospitals: A design science approach
Supplemental material, sj-csv-3-dhj-10.1177_20552076241229148 for Determining design criteria for indoor positioning system projects in hospitals: A design science approach by Johannes Wichmann, Thomas Paetow, Michael Leyer, Bisrat Aweno and Kurt Sandkuhl in DIGITAL HEALTH
Supplemental Material
sj-csv-4-dhj-10.1177_20552076241229148 - Supplemental material for Determining design criteria for indoor positioning system projects in hospitals: A design science approach
Supplemental material, sj-csv-4-dhj-10.1177_20552076241229148 for Determining design criteria for indoor positioning system projects in hospitals: A design science approach by Johannes Wichmann, Thomas Paetow, Michael Leyer, Bisrat Aweno and Kurt Sandkuhl in DIGITAL HEALTH
Footnotes
Contributorship
JW gathered literature and conceived the study. JW, TP and ML were involved in the development of experiments and interviews. KS participated in the methodological part, while BA performed data analysis. JW and ML reviewed and edited the manuscript while all authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Concerning research ethics, we adhere to the World Medical Association Declaration of Helsinki. While we do not address patients in our study, we nonetheless obtained verbal consent of our interviewees to use their statements for this study.
Funding
The authors disclosed receipt of the following financialsupport for the research, authorship, and/or publicationof this article: The experiments were funded by European Regional Development Fund, project number TBI-V-1-329-VBW-113 at Wismar University of Applied Sciences: Technology, Business and Design.
Guarantor
Supplemental material
Supplemental material for this article is available online.
Appendix
The results and templates of our controlled experiments and expert interviews can be accessed here: https://osf.io/jcs93/?view_only=67e3c4b3e79a46a3b8c21e567098becb.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.