
Abstract
Background
Indoor navigation within closed facilities has been subject of studies with different application areas, particularly in recent years (e.g. the navigation requirements of people or the location of objects). Hospitals are of specific interest in this regard as the multitude of technical equipment used is potentially interfering with navigation systems.
Objective
This research examines relevant studies regarding Indoor Positioning Systems (IPS) in hospitals and IPS that are designed for hospitals and in preparation for implementation, by investigating the respective technologies, techniques, prediction-improving methods, evaluation results, and limitations of the IPS.
Methods
To gather current and future IPS in hospitals, the methodology of a Scoping Review was used. The study has been conducted by applying the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Framework to the context of IPS in hospitals. The results and limitations concerning current and future IPS in hospitals were gathered and structured by using a highly cited evaluation framework for IPS.
Results
Thirty-eight studies were considered for this research. The IPS technologies investigated were Bluetooth Low Energy (n = 17), Wireless-Fidelity (n = 10), Hybrids (n = 4), Radio-Frequency Identification (n = 4), Ultra-Wideband (n = 1), Infrared (n = 1) and ZigBee (n = 1).
Conclusions
This study presents current and future IPS in hospitals. For future IPS research and IPS in hospitals, the theoretical implications contribute to our knowledge about IPS technologies, techniques, prediction-improving methods, evaluation results and limitations during testing/implementing IPS in hospitals. As practical implications, the insights of this study can be used by developers to improve IPS and by hospitals to facilitate IPS implementation.
Keywords
Introduction
The rapid development of various electronic services, such as Internet of Things, 1 over the past decade, has resulted in a multitude of innovations. Two of them are the navigation of individuals and the localization of objects within buildings. The use of those innovations in hospitals is of special importance, especially under consideration of pandemic crises and needs for isolation.2,3 Because health measures are highly complex and handled individually, 4 it is important to use the already scarce resources efficiently and to avoid redundant activities.4–6 Indoor Positioning Systems (IPS) as measures to track people and objects 7 should help to ensure that no resources for redundant activities in this context are raised, for example, finding the right room or important objects, such as respirators. Since hospitals have a unique environment concerning radiation and electromagnetic fields, for example, X-Ray and high-frequency fields, those circumstances are especially relevant for IPS in hospitals as they influence the IPS measures.7,8 Additionally, they confine the adaptability of challenges of other IPS research (e.g. shopping malls), as they do not use medical devices that emit radiation, like for example, X-Ray7,8 which underpins the practical relevance of this study. From a theoretical point of view, system implementations in hospitals are known to be costly9,10 and the success of an IT intervention depends as much on the implementation as on the system itself, 11 which also supports the need for this study. Thereby, the aim of this research is to provide a Scoping Review about (a) objectives of IPS in hospitals; (b) IPS technologies for hospitals; (c) their localization techniques; (d) their prediction-improving methods and (e) to evaluate the IPS concerning the criteria: (i) accuracy, (ii) availability, (iii) cost, (iv) energy efficiency, (v) latency/delay, (vi) precision, (vii) reception range, (viii) robustness and (ix) scalability. Then, the insights of this study can be used practically, for example, to determine an appropriate IPS for a hospital as well as theoretically, for example, (a) to facilitate the implementation of an IPS and to keep the costs therefore low as well as; (b) to avoid pitfalls during the development of a new IPS by considering the limitations of the existing and future IPS for hospitals. Consequently, this study is relevant for the following stakeholder groups: (i) researchers who investigate the adoption, diffusion, and evaluation of information technologies (IT) for hospitals, (ii) IT developers for hospitals as well as (iii) hospital management that try to determine an appropriate IPS for their hospital.
Accordingly, this paper is structured as follows: the section “Conceptual Background” describes the concept of IPS in hospitals. The section “Method” represents the Scoping Review methodology as well as the search strategy and standardized data extraction form for IPS research in hospitals. Section “Results” reflects the outcome of this study, presenting technologies, techniques, prediction-improving methods, evaluation results and limitations of current and future IPS in hospitals. Section “Discussion” evaluates the outcomes, while the section “Conclusion” represents the implications and limitations of this study (for a better understanding, see Figure 3). For additional information concerning the limitations of current and future IPS in hospitals, see Appendix (A).
Conceptual background
For indoor positioning purposes, respective systems are necessary. These systems are dedicated to ascertain a specific position of an asset or individual and/or to track them. 12 Thereby, a localization technique determines the position of a mobile client (e.g. the tag attached to the wheelchair in the middle of Figure 1 as well as the tablet on the left-hand side and the wristband on the right-hand side) by utilizing a set of reference points (e.g. the routers in Figure 1) within a specific area 13 by using several technologies (e.g. Wireless-Fidelity [Wi-Fi] or Bluetooth Low Energy [BLE]). The technique (such as triangulation that is illustrated by the three circles next to the right router in Figure 1 or trilateration as represented by the triangle in Figure 1 below the left router) utilizes (a) specific signal(s) of the respective technology (such as the Received Signal Strength Indication [RSSI]). 14 If desired, prediction-improving methods can be used to improve the performance of the IPS, for example, by using filters. 15 In accordance with the implementation of the system, it can be used to support several tasks in a hospital, such as to track insulin pumps, 16 to track patients in the emergency department 17 or to reduce waiting times and redundant activities. For a better understanding, Figure 1 represents an exemplary functional setup for an IPS in a hospital.

Methods
As the methodology for this research, the Scoping Review approach by Arksey and O’Malley 23 was used. It is dedicated to “map” the relevant literature in the field of interest 23 and provides a search strategy, a standardized data extraction form and a risk of bias assessment. 24 This study examines IPS in hospitals to solve in-hospital IPS tasks. As the sole restriction, the published articles had to be in English. No publication date limitations were imposed. This search was applied to the literature databases Scopus (determined time frame: 2006–2020), IEEE (Institute of Electrical and Electronics Engineers/1994–2020) and AISeL (Association for Information Systems Electronic Library/2005–2017). The research was conducted from January 2020 to February 2021, with the last search run on 01 March 2021. The study was concluded from March to August 2021. Accordingly, the search strategy is presented 24 :
The following terms were used to conduct the search process: hospital, clinic, indoor navigation, indoor localization and object localization. The search queries for the databases AISeL, IEEE and Scopus are presented in A-1. Then, the studies were evaluated and determined as “relevant” or “not relevant” by a three-step investigation. First, the abstracts of the studies were reviewed, and they had to match the following first-order inclusion criteria:
The environment of the research is, at least, one hospital.
AND The study addresses the aim of navigating or tracking individuals through the hospital.
AND/OR The research addresses the aim of localizing objects in the hospital.
Second, duplicates that were determined through different databases were removed. Third, the studies were analyzed in-depth. Therefore, relevant studies had to match the following second-order inclusion criteria:
The IPS was tested and/or implemented in a real hospital scenario or designed for a hospital use case and is therefore in preparation to be implemented in a hospital scenario. The IPS determines the position of an object and/or a person by a localization technique (e.g. trilateration). For example, an IPS that gives directions due to a location that the user must determine manually (e.g. by selecting it as the own position) is considered irrelevant for this research. If the IPS is dedicated to navigate robots through hospitals, the respective study is considered irrelevant. Concerning the fact that the localization of robots has to be much more precise than those of people, since significantly more environmental factors, such as obstacles, have to be considered, this leads to higher costs for robot IPS than for more convenient IPS.
25
As costs are important to evaluate IPS (see section “Methods”), considering robot IPS would have caused a bias within the IPS evaluation results.
The abstracts and full texts were reviewed by the author and one reviewer independently of each other, that is, blinded, to determine whether research will be included in this study or not. The reviewer is not an author as he did it as part of his job, however, not a subordinate of the author. To report on the differences of this independent procedure (and for risk of bias assessment 24 ) the Cohen's kappa coefficient 26 was used. Thereby, a kappa value of .526 was determined that represents a moderate agreement between the author and the reviewer, according to McHugh 26 Subsequently, disagreements between the author and the reviewer concerning the first- and second-order inclusion criteria that were applied to the studies were solved by consensus. The author then performed the evaluation of the included studies, leading to the results (see Tables 1 to 3) and limitations (see A-3 to A-11) of this study. To collect the data, a standardized extraction form 24 was designed (based on the Cochrane Consumers and Communication Review Group's data extraction template 27 that was adapted for IPS research purposes based on23,28,29 by the author). The datasheet contains: database; publication year; author(s); title; duplicate-check; abstract/first-order inclusion criteria: 1. hospital, 2. tracking/navigating individuals, 3. object localization; conference/journal details; in-depth analysis/second-order inclusion criteria: brief summary; 1. tested/implemented in hospital scenario, 2. live-determination of position, 3. no robot navigation; relevant to be included in review? (author + reviewer); notes (author); exclusion criteria/consensus between author and reviewer; study design; results: evaluation framework results; limitations; notes for results/limitations (author). For a better understanding, Figure 2 reflects the study selection process of the author. The study selection process of the reviewer will be provided as additional data for this research. (Available online).


Research process.
Objectives of the relevant IPS studies for hospitals.
Technologies, techniques, and prediction-improving methods of IPS in hospitals.

Extended Version of Signal Strength Path Loss Model.
Evaluation results of IPS in hospitals.
For appropriate evaluation of IPS in hospitals and to gather the participants (P), interventions (I), comparators (C), outcomes (O) as well as the study designs (S), the PICOS approach as part of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework guidelines according to Liberati et al. 31 was used. To specify the participants (P), the term “hospital” represents a specific location where individuals receive medical care for a certain amount of time. 59 This definition specifically includes integrated and additional business segments of a hospital, such as an elderly care center, but excludes medical care interventions at alternating locations, for example, integrated home care. 60 To determine the study design of relevant research (the “S” in PICOS approach 31 ), design evaluation methods according to Hevner et al. 61 were used, who distinguished between: observational- (case- and field studies); analytical- (statistic-, architecture-, and dynamic analyses as well as optimization); experimental- (controlled experiment or simulation); testing- (functional- or structural testing); or descriptive (informed arguments and scenarios) methods as study design. Accordingly, this research considers studies that: a) describe the implementation of an IPS and different scenarios to test the IPS and therefore fulfill the requirement of a “case study” according to Hevner et al. 61 ; b) represent experiments 61 that were conducted in a hospital or in an environment that was specifically prepared to illustrate a hospital (e.g. prepared university labs to simulate an emergency department waiting hall in a hospital 32 ); as well as c) simulated systems, 61 whose development was clearly related to a hospital scenario, for example, a system to prevent the kidnapping of newborns 40 or to call nurses in case of emergency. 37 As comparatives (C), the IPS were sorted using criterion sampling methods62,63 to determine the practical aim of the respective IPS (see Table 1). Additionally concerning the technical IPS concepts, characteristics were derived from Liu et al. 28 and Zafari and Leung 29 who proposed a highly cited evaluation framework for IPS. Therefore, the systems were sorted concerning: 1) the technology of the IPS (e.g. Wi-Fi, BLE); 2) the localization technique (e.g. RSSI) as well as; 3) prediction-improving methods that enhance the IPS accuracy. To evaluate the IPS (as “outcomes” as the “O” of the PICOS approach28,29,31), defined relevant criteria therefore. They are: (i) accuracy, (ii) availability, (iii) cost due to additional hardware, (iv) energy efficiency, (v) latency/delay, (vi) precision, (vii) reception range, (viii) robustness, as well as (ix) scalability.28,29 In this research, those aspects are used to distinguish the relevant IPS for hospitals, as evaluation results were gathered according to the evaluation parameters of from Liu et al. 28 and Zafari and Leung 29 and expected and unexpected limitations of those investigations are assigned to the respective parameters. Although the results are demonstrated in Tables 1 to 3, detailed explanations of the limitations in accordance with the evaluation characteristics are presented in the appendix (see A-3 to A-11). First, the respective IPS accuracy (declared in meters) helps to compare the relevant studies among themselves by presenting the exactitude of the localization results (declared in meters)28,29 (see A-3). Second, availability refers to whether the system utilizes techniques that do not need additional hardware, instead utilizes signals (e.g. Wi-Fi, BLE) that are already available on common devices (e.g. smartphones) 29 (see A-4). Third, IPS setups should require no or minimal additional costs due to additional hardware28,29 (see A-5). Fourth, to protect device batteries, the IPS should be energy efficient28,29 (see A-6). Fifth, the latency/delay of the IPS should be low to reduce the possibility of localization errors 29 (see A-7). Sixth, whereas the accuracy considers the (absolute) values of the mean distance errors, the precision represents the (relative) consistence of the system instead, as it reveals the variation of its performance over many trails 28 (see A-8). Seventh, the reception range refers to the range of the signal that is emitted by reference points (e.g. routers) and received by devices (e.g. smartphones), as higher ranges often lead to lower accuracies but also lower costs and vice versa28,29 (see A-9). Eighth, the IPS should be robust in terms of system failures and dysfunctions because of new tasks for the respective IPS 28 (see A-10). Ninth, the scalability of the IPS should be high, so that new tasks/areas of implementations (e.g. asset tracking/hardware stores) can be easily processed by the system 29 (see A-11). Furthermore, Figure 3 represents the overall research process of this study.
Results
The search of AISeL, IEEE and Scopus database provided 404 results. After adjusting for duplicates, 82 articles were removed. Additionally, 219 studies were discarded, as they did not meet the title and abstract criteria defined in the section “Methods”. The remaining 103 articles were reviewed in-depth and checked whether they fulfill the inclusion criteria. Thereby, 65 studies were excluded, as they were neither dedicated, nor tested or simulated in a hospital scenario (n = 43), the position determination of the IPS was not live (n = 12), or the IPS was dedicated to robot navigation (n = 10). Hence, a total of 38 studies was included in the review.
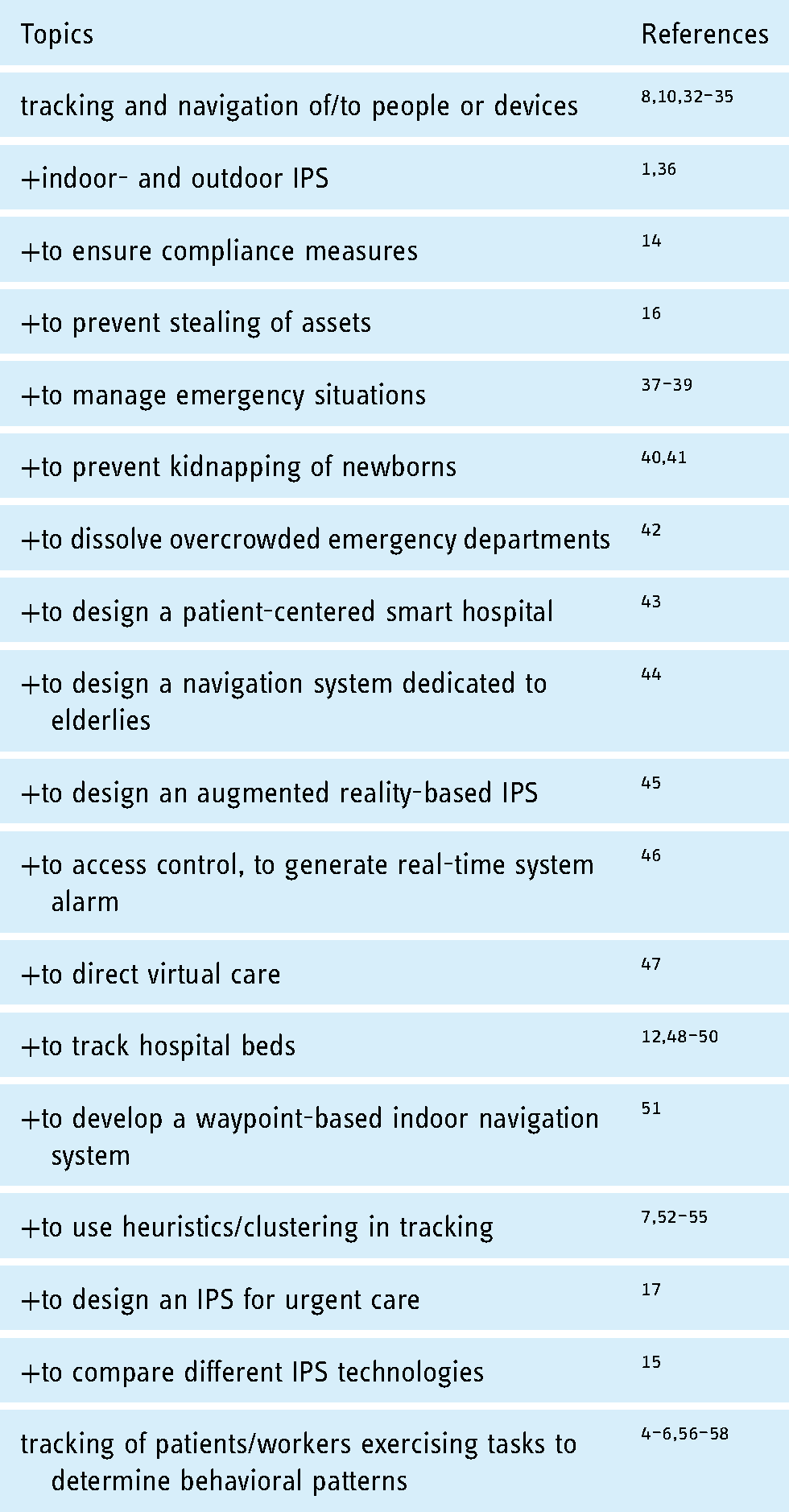
To gather the results, the PICOS approach was used. A detailed depiction of the participating (P) hospitals is presented in A-2. For the interventions (I), the following Table 1 presents the research objectives of the relevant studies to encounter localization-related problems in hospitals. As expected, all studies considered the tracking and navigation of/to people or devices, with some studies tackling more granular issues (e.g. to prevent the kidnapping of newborns/to track patients/workers exercising tasks to find behavioural patterns).
To distinguish between existing IPS, attributes are needed to compare (“C” in PICOS 31 ) the results. Therefore, Liu et al. 28 and Zafari and Leung 29 conducted highly relevant studies to distinguish and evaluate IPS. They state that different localization techniques (such as trilateration, see section “Conceptual Background”) can be utilized by different localization technologies (such as Wi-Fi or Bluetooth).28,29 As the complexity of the algorithm (as the foundation of the localization technique) is more important than the raw choice of technology for IPS purposes, 53 those criterions (localization technology and technique) are used in this research to gather the results following criterion sampling methods.62,63 Then, the criterions are assigned to the taxonomy of smartphone-localization techniques according to Maghdid et al. 64 Additionally, prediction-improving methods are gathered, as they improve the IPS performance 15 and represented in Table 2.
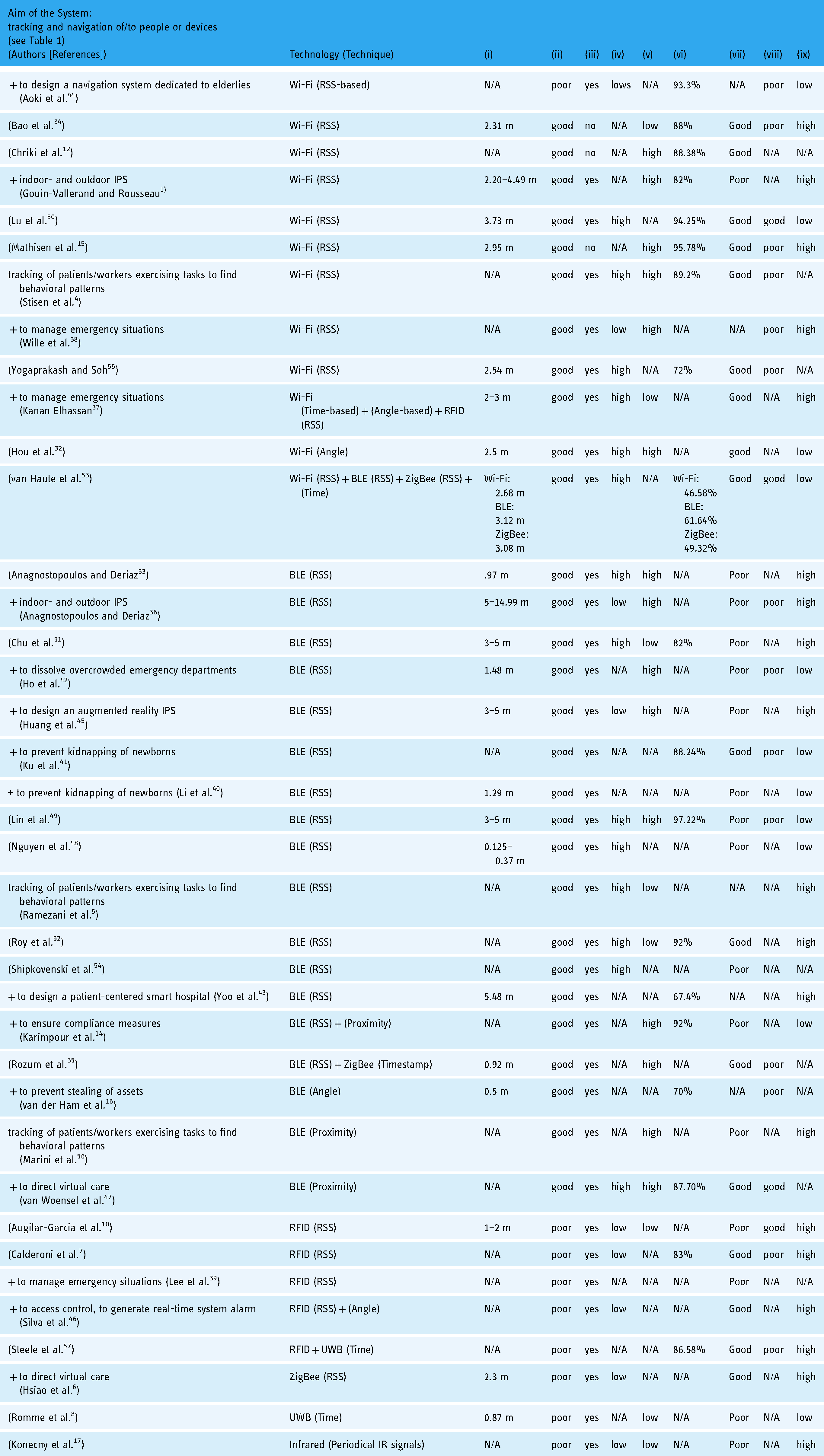
As the outcomes of this research (and of the PICOS approach 31 – “O”), this scoping review reflects current and future IPS in hospitals by determining that Wi-Fi and BLE are the most common technologies used in this context (see Figure 2, Table 2). Furthermore, RSS-based localization techniques are widely used, which is congruent with general IPS research. 29 By considering prediction-improving methods, a variety of approaches exist that improve the IPS accuracy (see Table 2). Concerning the performance of the IPS, evaluation criteria28,29 were used to assess IPS (see section “Methods”) and are presented in the following table. The data for (i) accuracy is either self-reported (in meters) or not available (N/A). The (ii) availability is determined either “good” if the IPS is processable by most of the current smartphones and “poor” if not. The evaluation of (iii) cost due to additional hardware refers to whether additional hardware is used or not. Regarding (iv) energy efficiency, an IPS is either determined “high” if it does not drain batteries or “low” if it does. The (v) latency/delay of the IPS is determined “low” by reacting within milliseconds, otherwise it is considered “high”. (vi) Precision is either self-reported (in percent) or not available (N/A). A (vii) reception range of more than 10 m between the measurement points is considered “good” to keep the (iii) cost low, 29 otherwise it is determined “poor”. (viii) Robustness is either “good” or “poor” (self-reported). For a “high” (ix) scalability of an IPS, it has to been tested with multiple devices, otherwise it is determined “low”. If criteria were not addressed by the study sufficiently, they were considered not available (N/A). The evaluation results of IPS in hospitals are shown in Table 3.
Concerning the limitations of the IPS the evaluation criteria ((i) accuracy to (ix) scalability)28,29 were used to gather expected and unexpected limitations. As those limitations are numerous and (mostly) heterogeneous, they are presented in the Appendix, from A-3 to A-11. Considering the study design (S) of the PICOS approach, 31 most studies are experimental (as controlled experiments) or observational (as case studies) according to the definition of Hevner et al. 61
Discussion
With regard to the analysis of participants, one hospital is especially relevant. The results regarding participating hospitals show that the National Taiwan University Hospital Yun-Lin Branch has been involved in a multitude of IPS studies. Thereby, the hospital is most relevant for those stakeholder groups seeking interchange and helpful insights of IPS implementation and/or development in hospitals. Concerning the evaluation criteria that are used to compare and limit the existing IPS, this study led to several propositions showing the need for further IPS studies.
First, concerning the evaluation framework used and by considering (i) accuracy, Wi-Fi-based IPS are less accurate than other technologies used for IPS in hospitals. However, together with the BLE-based IPS, provide a higher (ii) availability than the other approaches, which supports existing insights concerning IPS.28,29 The evaluation of (iii) cost is disputed, as some of the IPS used additional devices other than smartphones without a technical need to do so. The reasons therefore are various, for example, to adapt the IPS to meet certain demands of specific stakeholder groups 44 or to meet the overall aim of the IPS.4,55 Unfortunately, reports about (iv) energy efficiency are disputed as well, as they are often not available, despite the fact that (iv) energy efficiency is important for IPS, since some studies addressed this aspect accurately (e.g. Refs.38,47,52) The same holds true for (v) latency/delay, as details are often not available or a high (v) latency/delay is considered less important for the aim of the IPS, as for example, a live determination of a position within milliseconds is not necessary for the overall aim of the IPS (e.g. Refs.4,14,38). Regarding (vi) precision, most of the IPS obtained high values concerning the fulfillment of their IPS tasks. Therefore, the values of (vi) precision should be handled cautiously, as every study developed their own evaluation criteria to assess the IPS performance, leading to mere (vi) precision values without demonstrating the estimation of them (e.g. Refs.34,44,55). Surprisingly, some IPS failed to achieve a sufficient (vii) reception range compared to ascertained reception ranges for specific IPS technologies (such as Wi-Fi and BLE28,29) and (i) accuracy of other IPS. As some of them chose to keep the distance between the measurement points lower than 10 m (e.g. Refs.1,51) using more measurement points than technically necessary,28,29 probably to increase (i) accuracy, 29 other IPS that achieved sufficient (vii) reception range also reached a higher (i) accuracy (e.g. Refs.15,35). Concerning the (viii) robustness, it is likely that more than those IPS evaluated as “poor” determined problems/concerns that limit their IPS while implementing/testing their system, as statements about (viii) robustness were often not available. Nonetheless, some studies reported their problems/concerns concerning (viii) robustness adequately (e.g. Refs.7,47), whereas (ix) scalability in Zafari and Leung 29 was defined as: “we require the system to support multiple device for scalability”, this study requires that the respective IPS has been tested with more than one device to be able to verify (ix) scalability. Given that, a surprising amount of IPS (10) have not been verified with more than one device. Again, several studies did not report their experiences concerning the (ix) scalability of their IPS.
Based on the results of the evaluation framework, there are research gaps regarding IPS in hospitals that should be addressed in the future. First, the algorithms of IPS should be addressed in further studies, which is supported by van Haute et al. 53 stating that: “the complexity of the algorithm is more important than the raw technology choice”. The results show that IPS that used the same technology performed differently, with for example, BLE-IPS that were tested in a hospital in a larger space achieving (i) accuracy from 1.48 m 42 as the mean error compared to similar IPS in a larger space that achieved (ii) accuracy of 3 to 5 m, 51 despite the fact that the study of Chu et al. 51 is more recent. One possible explanation is the prediction improving method used, as an important factor in determining the (i) accuracy of the IPS according to Liu et al. 28 and Zafari and Leung 29 whereas Ho et al. 42 used fingerprinting as a prediction improving method, Chu et al. 51 incorporated the strongest signal for position determination, indicating that fingerprinting is better suited for BLE-IPS in hospitals than the strongest signal for position determination in larger spaces. Future research should thus investigate the prediction improving methods presented in this study to the respective IPS technologies to verify which prediction improving method is best suited for the respective IPS technology by addressing multiple prediction improving methods for IPS in different hospitals in large spaces.
Second and simultaneously, those studies should address the evaluation framework proposed in Liu et al. 28 and Zafari and Leung 29 to enhance the comparability between the different IPS in hospitals and to verify the propositions of Liu et al. 28 and Zafari and Leung 29 regarding IPS in hospital contexts. Until now, the overall evaluation of IPS in hospitals is limited, as the presentation of most of the IPS in this study is, measured against the criteria of the evaluation framework according to Liu et al. 28 and Zafari and Leung. 29 For instance, some IPS required high (iii) cost, while providing a poor (vii) reception range (which is likely, due to the use of more devices than necessary28,29) and achieving poor results in (i) accuracy (e.g. Refs.45,49,51). In contrast, other IPS required low (iii) cost, while providing a good (iii) reception range and achieving better results in (i) accuracy (e.g. Refs.15,34). As this may belong to the algorithm of the IPS that leads to good (i) accuracy, respectively,28,29 the handling of an appropriate IPS is too complex to evaluate it using mere (i) accuracy as a measure to compare IPS. 47 Therefore, the reasons for different IPS performances will be more clear and further Scoping Reviews concerning IPS in hospitals will be more precise, if the IPS are to be evaluated using the same evaluation framework. Besides, the evaluation framework itself could be further evaluated, for example, concerning a ranking of the different evaluation criteria of the framework by interviewing stakeholders (such as (i) researcher who investigate the adoption, diffusion and evaluation of IT for hospitals, (ii) IT developers for hospitals and (iii) hospital management) and by analyzing the relationships between the evaluation criteria, as some of them seem to be dependent of each other, such as (iii) cost and (vii) reception range.
Conclusion
This research investigates current and future IPS in hospitals by reviewing relevant studies obtained from the literature databases AISeL, IEEE and Scopus using the Scoping Review method. It was conducted using the PRISMA Framework and PICOS approach 31 to gather the results. To critically assess the IPS, the highly cited evaluation framework for IPS according to Liu et al. 28 and Zafari and Leung 29 was used and current and future IPS in hospitals gathered and evaluated concerning: IPS technology, technique and prediction-improving method as well as: (i) accuracy, (ii) availability, (iii) cost, (iv) energy efficiency, (v) latency/delay, (vi) precision, (vii) reception range, (viii) robustness and (ix) scalability.28,29
This study provides several theoretical implications. First, this research contributes to our knowledge about IPS in hospitals by presenting the (1) technology, (2) techniques, (3) prediction-improving methods, (4) evaluation results as well as (5) limitations during testing/implementing IPS in hospitals. The highly cited evaluation framework for IPS28,29 ensured that sufficient comparability to assess IPS was given. Unfortunately, only few studies utilized the evaluation framework to assess their IPS, leading to a limited evaluation of all IPS in hospitals and the insights of this study, respectively. Therefore, and to improve further IPS reviews, the author of this study strongly encourages researcher to use the evaluation framework to assess their IPS. Additionally, future research should focus on improving the evaluation framework. Currently, all the evaluation criteria ((i) to (ix), see section “Methods”) are considered as equally important. Given that, it is likely that stakeholders with partly opposing interests (such as hospital management and IPS developers) could consider certain evaluation criteria ((i) to (ix)) more important than others, demonstrating the need to rank those evaluation criteria and therefore to provide a weighted framework to assess IPS (in hospitals).
As practical implications, the insights of this study can be used by (i) researchers who investigate the adoption, diffusion and evaluation of IT for hospitals, (ii) IT developers for hospitals and (iii) hospital management that try to determine an appropriate IPS for their hospital, as (1) application scenarios for IPS in hospitals were determined (represented by the objectives of the studies, see Table 1) that could be relevant for other hospitals seeking to implement an IPS. (2) Hospitals seeking to implement an IPS can use the perceptions of this study (IPS technologies, techniques, prediction-improving methods, the evaluation and limitations of IPS in hospitals) to determine an IPS technology that satisfies their demands towards IPS in hospitals. Decision-makers in hospitals benefit from this study by obtaining an evaluation of existing IPS approaches in hospitals, which can help them to decide which IPS technology to adopt. This evaluation can be used in conjunction with the prediction improving methods to define the IPS technology, technique as well as prediction improving method for their IPS in question.
Ultimately, this research is limited, as every study. As the databases AISeL, IEEE and Scopus were used to gather relevant studies, other databases (such as Web of Science or Google Scholar) could lead to different results. This could also be subject of further studies. Additionally, this research does not consider IPS in hospitals that are dedicated to robot navigation. Thereby, this study is only partially relevant for researchers or hospital management seeking to implement an IPS in a hospital dedicated to robot navigation.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076221081696 - Supplemental material for Indoor positioning systems in hospitals: A scoping review
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076221081696 for Indoor positioning systems in hospitals: A scoping review by Johannes Wichmann in Digital Health
Footnotes
Acknowledgements
The author would like to thank Wieland Müller from Rostock University for peer-reviewing the search process and the data extraction form.
Conflict of interest
The authors have no conflicts of interest to declare.
Contributorship
Explanations concerning contributorship are not applicable to this study since it was conducted by one author only.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Ethical approval
The ethical approval is not applicable to this study, because this research does not contain any studies with human or animal subjects.
Guarantor
JW.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.