
Abstract
Objective
The goal of this research was to demonstrate the efficacy of telemedicine via design, implementation and evaluation of a web-based remote patient monitoring system (WB-RPMS) across the tertiary/university teaching hospitals in a developing country Nigeria, as a tool to continue to expand access to an affordable and resilient tertiary healthcare system through the challenging times of the COVID-19 pandemic or any future disruptions.
Methods
This research employed an agile and human-centred design thinking philosophy, which saw the researchers iteratively collaborate with clinicians across the system development value chain. It also employed qualitative and quantitative research methods for new system evaluations. After the system's development, a 20-patient sample was randomly selected from members of the National Youth Service Corp to evaluate the WB-RPMS Patient Portal for usability and user experience through a survey based on the system usability scale. Again, the COREQ standards for reporting research result were adopted for this study.
Results
The evaluation of the WB-RPMS Patient Portal by a select patient sample showed that 95.0% of the respondents believed that they would like to use the system frequently. It was also discovered that 90.0% of all respondents also indicated that they found the Patient Portal to be simple; 85.0% of the respondents believed and indicated that the WB-RPMS Patient Portal was easy to use.
Conclusions
The result of the usability evaluation of the developed WB-RPMS Patient Portal showed that it was well received by the select patient sample and by the clinicians who participated in the development process. In fact, the performance of the system shows that it has the potential to remotely support and sustain improved access to affordable healthcare for outpatients in developing countries even during times of uncertainties and disruptions as recently occasioned by COVID-19 pandemic.
Keywords
Background
There was a global disruption of healthcare delivery protocols due to the outbreak of COVID-19 pandemic. 1 The impact which had remained devastating also halted several economic value chains and resulted in deaths. In Nigeria, the experience was not different. The COVID-19 pandemic exposed the significant deficiencies in the Nigerian health system and how fragile its essential healthcare services (EHS) are when faced with sudden disruptions. 2 This starkly revealed the need for a more resilient approach to ensuring that EHS continues to be provided even in times of major health crises. It is imperative that the Nigerian health system be strengthened, with the necessary resources and infrastructure in place, to be able to withstand any future health shocks. 2 This would ensure that the basic healthcare needs of the patient population are met without interruption, even in times of emergency. 2 Additionally, it could be suggested that the government consider the implementation of alternative strategies to guarantee the provision of EHS, such as utilising mobile health centres and telemedicine services.3,4 Such initiatives would help to bridge the gap between EHS provision in urban and rural areas and guarantee that the most vulnerable communities have access to the same quality of healthcare services. Ultimately, it was clear that the COVID-19 pandemic had highlighted the urgent need for sustainable EHS provision in Nigeria to ensure better protection of the population in times of health crises. 2
On the impact of the COVID-19 pandemic on the outpatient clinics of some Nigerian tertiary/university teaching hospitals, the News Agency of Nigeria (NAN) released a report indicating that the COVID-19 pandemic had severely impacted outpatient clinics at Nigerian tertiary hospitals, including the University College Hospital, Ibadan. 5 The closure of Medicine, Surgery and Children's Outpatient Departments has left patients without access to medical care, potentially leading to delays in diagnosis, treatment and follow-up care. 5 This closure could potentially worsen medical conditions and even cause death. 5
Meanwhile, before COVID-19, these healthcare systems had hitherto been under the burden of cost-related challenges, including the high cost of access to healthcare by patients 6 and the high cost of healthcare service delivery by healthcare providers. 7 These cost-related challenges often implied that healthcare providers were unable to afford the necessary infrastructure and facilities that could support improved access and accommodate a large population of patients seeking care. 7 Again, this lack of resources to provide better working conditions can often be found prohibitive when trying to retain or employ sufficient highly skilled clinical personnel to support healthcare service delivery across these economies, including Nigeria. This had resulted in significant brain drain from the available healthcare workforce.8–10 This challenge can limit the amount of care available to those in need, and some may even be forced to go without treatment.
Now, given that the outbreak of COVID-19 had drastically changed the way healthcare was hitherto delivered, an alternative to physical attendance in the hospitals became necessary. In response, there was an unprecedented surge of interest in telemedicine as a panacea to sustain rapid expansion and sustained healthcare delivery, particularly for the outpatient population during and after the pandemic. 11 Telemedicine is rapidly evolving across the globe, but its adoption in developing and resource-constrained economies like Nigeria has been quite slow.12–14 The COVID-19 pandemic has further pushed for its wider adoption, as it has become a much safer alternative with the social distancing measures enforced by the government and restrictions on hospital visits. This is especially so in countries where there is a limited number of doctors or where healthcare infrastructure is inadequate. 12
Now, telemedicine is a part of telehealth, which uses digital tools to provide healthcare services over a distance. This type of technology can help reduce the need for physical visits to the hospital while still providing excellent medical care. It can make it easier for people to access quality healthcare without the need for in-person appointments. 14
Now, as earlier stated in the research objective, this research project sought to design, implement and evaluate a web-based remote patient monitoring system (WB-RPMS) Patient Portal as a digital healthcare intervention project to enable outpatients of tertiary/university hospitals in developing and resource-constrained economies to remain connected to necessary medical care in the event of any pandemics or future disruptions. This project was believed to have potentials for significant positive impact on the healthcare system in Nigeria, to make it more resilient and capable of responding to unexpected shocks or disturbances as recently occasioned by COVID-19. The researchers believed that by providing outpatients with remote access to necessary medical services, this approach would help mitigate some of the risks associated with pandemics or any other future disruptions and ultimately improve the quality of healthcare available in Nigeria. This project could also help reduce the financial burden on outpatients by providing them with more affordable access to medical care, saving them time that could have been used for other ventures and saving them the cost of transportation for regular health checks. In addition, it could also help reduce the strain on healthcare workers, as they can use the system to remotely monitor and manage patients without needing to physically be present.
And because the developed WB-RPMS Patient Portal can support remote clinician–patient engagement, it has the potential to help healthcare providers optimise the cost of healthcare administration. This is important for healthcare providers in developing economies and Nigeria, as they do not always have to spend huge and scarce resources trying to expand their healthcare facilities to accommodate the increasing patient population. With the deployment of WB-RPMS Patient Portal, some of their services can now be moved online/remotely for outpatients on regular health checks, while those in critical condition who really need to see the doctor for physical examinations can now go to the physical clinic in the respective health facility. This approach would help optimise space use. It can also help optimise clinical staff engagements, as the same clinician who saw patients physically in the hospital could still remotely review and monitor outpatient's health status from the comfort of their convenient locations and times, thereby saving resources that could have been expended on new hires.
Ultimately, this project could help bring greater stability, security and access to medical care for all individuals in Nigeria.
Enabling environment and government policy initiatives that could support WB-RPMS Patient Portal
When considering whether Nigeria has the necessary enabling policy environment to support a WB-RPMS via a patient portal, it is important to note that relevant policies are already in place. Moreover, conversations about digital health in developing countries, particularly Nigeria, are becoming increasingly popular due to the rapid spread of mobile phones and other devices among various sections of the population. 15 It is strongly believed that these mobile technologies would be leveraged by authorities towards the attainment of the Universal Health Coverage (UHC) and eventually be able to reach the ultimate sustainable development goals (SDGs) on health. 15
At this juncture, it is essential to note that, despite the potential that digital health intervention programmes and projects had in Nigeria's healthcare system, the country had yet to take full advantage of the huge inherent opportunities owing to various factors, which could include inadequate resources, challenges due to healthcare governance structures, poor infrastructure and a lack of highly trained tech personnel to run such implementations. Again, there were challenges due to the high cost of implementation of such programmes vis-à-vis the limited funding available to countries in sub-Saharan Africa and Nigeria in particular. 15
Be that as it may, it is important to state that the Nigerian government has made significant efforts towards creating an enabling environment to support digital health intervention programmes and projects across Nigerian healthcare institutions. For instance, WB-RPMS projects would significantly benefit from government policies on cloud technologies, national data regulations and the nation's health ICT strategic framework, as discussed below.
National Cloud Policy
The National Cloud Policy was created to encourage the use of cloud technology among government entities and among small to medium businesses in order to enhance their services and internal operations. 16 The implementation of this cloud policy is meant to help different parts of the government achieve proficiency in the implementation of cloud-based services. It was intended that all sectors of the economy would benefit from this, including healthcare. 16 The National Cloud Policy was again intended to provide make-up for government agencies struggling with infrastructure deficits, which had hampered their full implementation of their digital initiatives. The cloud policy was also intended to provide an enabling environment for potential indigenous cloud service providers in Nigeria. 16 All of these benefits of the cloud policy could significantly provide the needed support to healthcare digital transformation initiatives based on cloud computing solutions, including the WB-RPMS via the patient portal.
Nigeria Data Protection Regulation 2019
The Nigeria Data Protection Regulation 2019 was formulated by an approved agency of the Federal Government of Nigeria, the Nigeria Information Technology Agency (NITDA). The goals of the regulation were to uphold citizens’ rights to privacy of personal data, guarantee secure transactions that involve the exchanging of such information, protect personal data and information from any unauthorised manipulation or alteration and ensure secure e-commerce operations in Nigeria as well as with other countries while following global standards. 17
National Health ICT Strategic Framework
The National Health ICT Strategic Framework, created by the government, is an essential document that aims to unify stakeholders in the healthcare industry to make the most of Information and Communication Technologies (ICTs) that are utilised in healthcare. The Framework provides a clear roadmap that outlines the key objectives and priorities of using ICTs in healthcare, with an overarching goal of achieving UHC. 18 Again, the Framework is an essential tool that guides policymakers, healthcare providers and other stakeholders in the industry to identify and prioritise areas where ICTs can be effectively utilised. 18 It serves as a blueprint that outlines the steps required to implement new technologies, as well as to enhance existing systems and infrastructure. The Framework also helps to identify the potential benefits of using ICTs, such as improved patient outcomes, increased efficiency and reduced costs [ibid]. It also focuses on capacity building and training for healthcare providers and administrators to ensure that they can effectively leverage the benefits of ICTs. 18
Overall, the trio of Nigeria National Cloud Policy, Nigeria Data Protection Regulation 2019 and National Health ICT Strategic Framework can effectively support the implementation of telemedicine in Nigeria. The National Cloud Policy, for instance, would provide a framework for the adoption of cloud computing in Nigeria. 16 This policy can aid the implementation of telemedicine by providing a secure and reliable platform for healthcare providers to store and access patient data. The Nigeria Data Protection Regulation 2019, on the other hand, ensures that patient data are protected and secure, preventing unauthorised access and misuse. 17 This regulation can help build trust between healthcare providers and patients, encouraging more people to adopt telemedicine. Furthermore, the National Health ICT Strategic Framework provides a roadmap for the adoption of ICT in the healthcare industry in Nigeria. 18 This framework can aid the implementation of Telemedicine by providing guidelines for the development and deployment of telemedicine programmes and projects, including the WB-RPMS, which could allow patients to access healthcare services remotely, reducing the need for physical consultations improving access to healthcare services.
Methods
Research aim
The aim of this research was to design, implement, test and demonstrate the efficacy of a WB-RPM (via patient portals) across the tertiary/university teaching hospitals in a developing country, Nigeria, as a verifiable tool to continue to expand access to affordable, resilient tertiary healthcare systems.
The research design
This project involved different research paradigms, like qualitative, quantitative and design research paradigms. Specifically, the researchers employed interviews and observations of existing healthcare protocols and workflow, and they also integrated the iterative agile and human-centred design thinking methods in order to avail them a hybrid system development life cycle that could guarantee a user-centred healthcare support system that satisfies end-user expectations. The three senior orthopaedic surgeons provided the specifications for the remote patient monitoring and engagement module or portal. They also iteratively evaluated the improved prototypes until the final module was ready. Issues about the safety of patient information were considered. Issues about online consultation payment by the patient were also considered. The clinicians provided all the requirements to support their full expectations from a web-based patient portal that can guarantee comprehensive remote patient monitoring and viable orthopaedic outpatient–clinician engagements. These senior orthopaedic chief consultant surgeons either headed or are heading the orthopaedic departments of either of the tertiary/university teaching hospitals studied: a federal university teaching hospital, a state university teaching hospital and a national orthopaedic hospital.
After the system's testing and implementation, it was evaluated for usability by a 20-patient sample representative. This evaluation was achieved through a validated questionnaire that was based on the system usability scale (SUS).19–21 The choice of patient representatives was because it was not always easy to get the attention and consent of real patients to review and evaluate new digital healthcare systems given their (sometimes) very challenging health conditions, and the researchers wouldn’t want to appear insensitive to these realities. Again they were particularly interested in patients who are computer literate or whose caregivers are computer literate and are willing to take responsibility for the system use. Then, the researchers reached a consensus that only being ill met the criteria for being considered a patient and anyone can be. So, they randomly selected a 20-patient sample (as patient representatives) from young university graduates who are also members of the National Youth Service Corps and who are also computer literates, thereby satisfying the eligibility criteria. The result was quantitatively evaluated using SPSS and Microsoft Excel for the dashboard.
At this point, it is important to note that the COREQ standards were adopted while reporting this research.
The research setting
The implementation of the WB-RMPS Patient Portal was intended to support outpatient care management across the tertiary/university teaching hospitals in Nigeria. The researchers therefore selected the University of Nigeria Teaching Hospital (UNTH), the ESUT Teaching Hospital and a National Orthopaedic Hospital as the case study environments.
Meanwhile, the UNTH is one of the foremost and oldest university teaching hospitals in Nigeria. The UNTH was established over 60 years ago and serves as the Teaching Hospital for the University of Nigeria College Of Medicine. The hospital was designated the World Health Organisation Centre for Innovation in Medical Education between 1991 and 2000. The UNTH was also designated a centre of excellence in cardiothoracic surgery by the Federal Government in 1986. The teaching hospital currently hosts about nine training programmes and schools. It currently has 41 departments (with 3 outposts). The UNTH is currently over 500-bed-capacity. 22
On the other hand, the ESUT Teaching Hospital has a capacity of about 350–400 beds. Its history dates back to the 1930s, but it was made a state university teaching hospital in 2006 by then Governor Chimaroke Nnamani. The ESUT Teaching Hospital, a tertiary care provider, was designed to provide specialists Medicare to the general public and also provide a training facility for the ESUT College of Medicine. The ESUT Teaching Hospital also runs other ancillary programmes like the School of Nursing and the School of Midwifery. As a tertiary care provider, ESUTH provides care services in general medicine, obstetrics, paediatrics and various branches of surgery, as well as other affiliate/support services such as radiological services, physiotherapeutic services, pharmacy and laboratory investigations. The ESUTH is also a referral centre for healthcare services. 23
The National Orthopaedic Hospital in Enugu, which was one of the research environments studied, was established in 1979 through an Act of the National Assembly. It was established to provide specialist tertiary care services in the areas of orthopaedic surgery, nursing services, residency training, radiological services, dietetics and catering services, trauma surgery, burns and plastic surgery, pharmaceutical services, physiotherapy, anaesthesia, etc. The National Orthopaedic Hospital was established to serve one third (1/3) of Nigeria's population residing in the Eastern and Southern parts of Nigeria. There are two others of this kind in other parts of Nigeria. 24
System interaction modelling using UML
The patient would be able to accomplish the following functional operations, as illustrated in Figure 1 UML diagram.

Patient's use case diagram of the WB-RPMS Patient Portal.
Figure 1 represents the patient and who is also at the centre of the WB-RPMS Patient Portal design. The use cases captured several potential functionalities that would enable the patient to fully engage with the doctor remotely. These were the products of the several interactions the researchers had with the orthopaedic doctors, who were also part of the research team. Important to note is also that one of the members of the research team was once an orthopaedic outpatient who suffered distal femoral fractures due to a car crash. He was presented at one of the hospitals under study, and the researchers found his experience helpful during this study. So, when the researchers interacted with the orthopaedic doctors on what they really want from the orthopaedic outpatients who were placed on regular health checks, they were detailed on their treatment protocols, and it was so good to know that this can be managed remotely if a robust remote patient monitoring support system is in place. To be specific, after a patient is discharged, they become an outpatient and are placed on regular health checks. They would be expected to come to the clinic from home to see the doctor on a regular basis. The doctors with whom the researchers interacted indicated that any orthopaedic outpatient could often be expected to return to the hospital with new clinical images based on X-rays, computed tomography (CT) scans, magnetic resonance imagings (MRIs) and other images and reports on a new clinic appointment date of, say, 2 months. The doctor reviews these images and the accompanying medical reports to ascertain the patient's health progress. Afterwards, the patient could be asked to continue with current medication or new prescriptions could be made. A new lab or radiological request could be issued by the doctor pending future visits. Then, the doctor issues a new appointment date. It is important to note that before seeing the doctor at the hospital, the outpatient must have paid the day's consultation fee. Now, based on these clinician expectations, the WB-RPMS Patient Portal has functionalities to enable patients to upload these images and reports remotely, pay for online consultations and access the doctor's feedback. He could also request a new appointment on the WB-RPMS Patient Portal, view old and new lab and radiological uploads and view and even print his own clinical data documented by the physician according to dates of encounter.
Figure 2 shows the order of the patient's activities on the patient dashboard. The patient remains at the centre of the remote care delivery model. At the start of interaction with the Patient Portal, the patient enters his username and password. This is usually the hospital number and their private email, respectively. If these entries are correct, then the patient moves on to the next stage of user authentication, which generates an one-time password (OTP) and sends it to the patient's mobile phone or email. This is intended to ensure that patients do not inadvertently expose their health information to unauthorised persons due to poor login credential management. If OTP is correct, patients would now have access to a wide range of options or menus to execute, like upload lab/radiological results and reports/images, view past vital signs, view the doctor's clinical documentation by their dates, request an appointment to see the doctor, view the doctor's feedback and even pay for an online consultation. Once he is done, these activities could be terminated through a logout operation.

Patient's activity diagram with WB-RPMS Patient Portal.
Now it is important to note that some of the goals of this research were to provide a platform that guarantees successful remote patient–doctor engagement, particularly during trying times as recently occasioned by the COVID-19 pandemic, and also serve as a cost-saving measure for the care delivery providers and the patients alike by transferring their outpatient clinics for the digitally literate population online/remotely, thereby freeing up the usually overcrowded health facility for outpatients who are in critical shape and who really needed to see the doctor physically and those who are not computer literate. It was also expected that successful implementation of these features would also protect as many outpatients as possible from the risk of the COVID-19 pandemic, other health challenges or any other future disruptions and further free up the health facility to ensure social distancing protocols are adequately observed.
Now, when the above features on the activity diagram of Figure 2 were iteratively tested (on the functional WB-RPMS Patient Portal) by three orthopaedic doctors who were also part of the research team, they found the outcome of the evaluation to fulfil the above goals of the system design. These three doctors also participated at various stages of the system's development. Again, these features were further tested by a select sample of 20 patient representatives, and the results were discussed in the appropriate section below.
Overall, it is important to state that outpatients on the WB-RPMS Patient Portal must have visited the hospital at least once when their biodata and other preliminary clinical documentation would have been performed by the clinicians. After this stage, they would become eligible for remote patient care, but this choice is voluntary for the outpatient, particularly based on the level of their digital literacy.
System architecture
When a patient uses their browser from the Client Tier to request clinical documentation from the Application Tier web server, the server will process this request and send it to the database server (Figure 3). After retrieving this information, it would then be visible on any device connected to the client web browser, such as laptops, desktops, tablets and smartphones. These movements of data ensure that patients are able to read doctor messages and view patient medical records, including clinical encounters with doctors. The patient is also able to upload medical updates, lab and radiological investigation reports, images, etc., for the orthopaedics. Now, it should be noted that the digital remote doctor–patient engagement support system is practically non-existent across any of the tertiary/university teaching hospitals under study. The standard mode of healthcare delivery across these hospitals had been through physical attendance. Therefore, the adoption of this implementation (WB-RPMS Patient Portal), it is believed, would innovate outpatient healthcare delivery at each of the hospitals under study (provided all key factors like training and supporting infrastructure are in place).

Three-tier software architecture around which WB-RPMS Patient Portal module was built.
WB-RPMS Patient Portal interface and interaction design
Figure 4 shows a wireframe of the Patient Portal on the remote patient monitoring system, where patients, upon login, could have access to a wide range of menu options and functionalities to execute patient-centred operations. The interface in Figure 4 shows that patients, upon system implementation, could remotely upload up to three orthopaedic clinical images and accompanying reports, with which the doctor could monitor progress and send feedback as appropriate.
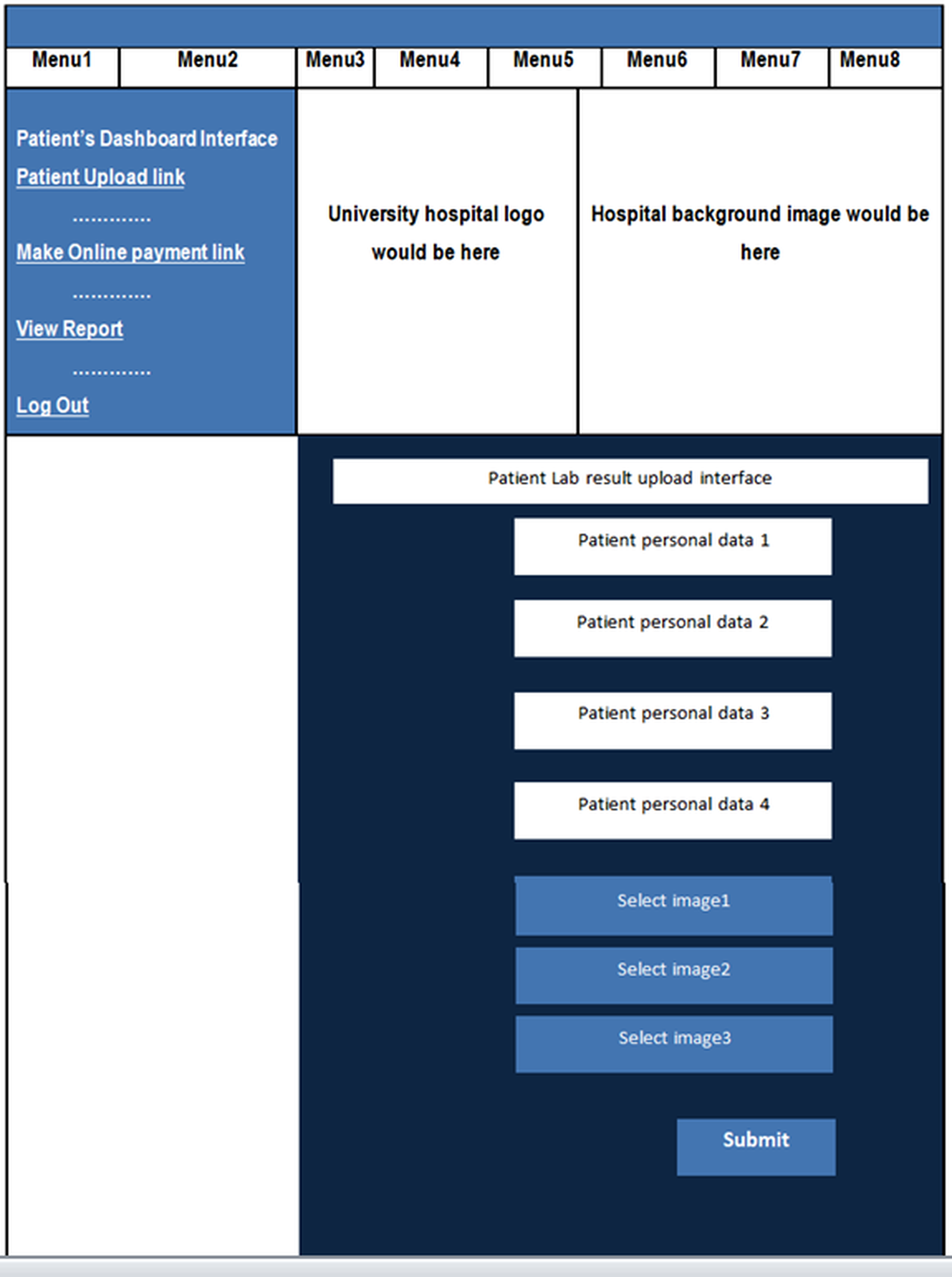
Patient lab result upload interface design.
Results
The results of the WB-RPMS Patient Portal implementation and usability evaluation
This section presents the outcomes of the WB-RPMS Patient Portal implementation and usability assessment conducted on a patient sample comprising of 20 members. This patient group was a representative of the intended user population. The survey utilised the SUS to evaluate usability. Now, it is important to note that the remote patient engagement and monitoring portal was designed for a specific patient population that possesses technical/digital skills and is capable of assuming responsibility and taking precautionary measures to safeguard the privacy of their health information remotely, to the best of their abilities. The objective was to provide remote patient engagement and monitoring services to this group, thereby reducing the burden on healthcare facilities and making them accessible only to patients who require critical care or physical examination by clinicians (Table 1).
Characteristics of the respondents.

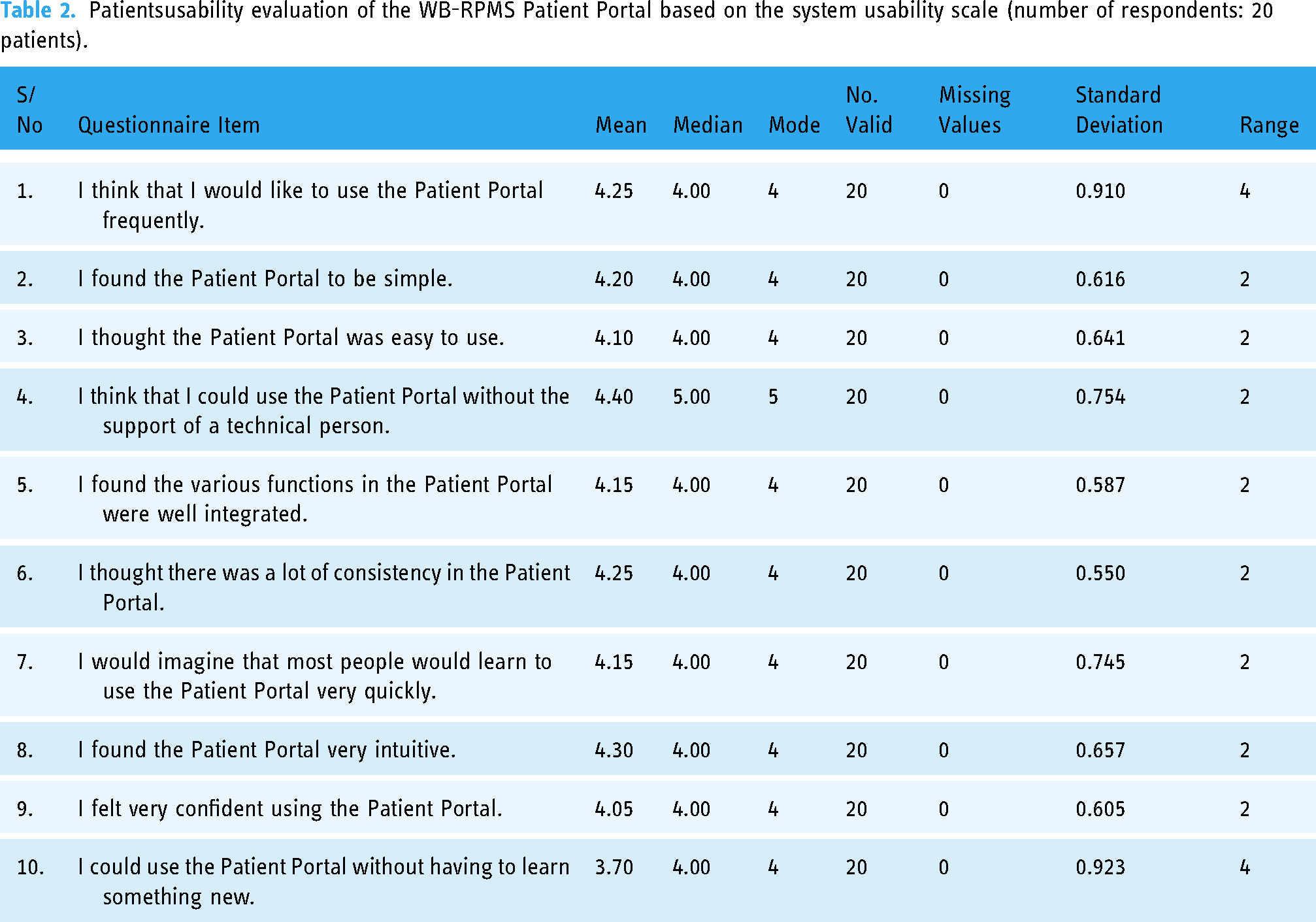
Further results (based on the practical evaluation of the Patient Portal) from the 20-patient sample evaluations can be found in Figure 5 and in Table 2, using the mean as a measure of central tendency to establish the overall position of the patients against each question of the survey based on the SUS. Now, using mean as a measure of central tendency to establish the overall position of stakeholders on each dimension of the SUS used for the Patient Portal module evaluation, Table 2 shows an overall mean value of 4.25, indicating that the patients strongly agree that they would like to use the Patient Portal frequently. Also, with a mean value of 4.20, the patients agreed that they found the new Patient Portal to be simple. More so, with a mean value of 4.10, the patients agreed that the new Patient Portal was easy to use. Further details can be found in Table 2. Meanwhile, the ranges of interpretation of the Mean Values of Table 2 can be found in Table 3.

Percentages of patients’ overall usability evaluation of the WB-RPMS Patient Portal using the system usability scale.
Patientsusability evaluation of the WB-RPMS Patient Portal based on the system usability scale (number of respondents: 20 patients).
The five-point scale interpretation (scoring range of Likert scale of the survey).

Source: Suebwongsuawan and Nomnian. 25
On the other hand, just one patient ‘strongly disagreed’ with the question, ‘I think that I would like to use the electronic health record system frequently’. It is possible that the patient could have other reasons why he thinks he would not like to use the developed EHR system frequently, and this is difficult to know, given that he agreed that the system was easy to use and that he strongly agreed to the fact that he could use the electronic health record (EHR) system without the support of a technical person. Again, a patient strongly disagreed with the question: ‘I could use the electronic health record system without having to learn anything new’. Further investigation showed that the patient indicated that she had never had any training on the use of EHR. The same patient also indicated that she had not had any personal or private experience with the use of EHR. It is obvious that such a patient needs a significant level of training and exposure to the use of the EHR system.
Result of WB-RPMS Patient Portal implementation
As shown via the screenshot of the RPMS Patient Portal dashboard implementation on Figure 6, the patient is able to accomplish a lot as listed below (Patient use case of the WB-RPMS Patient Portal/dashboard section) and as proposed through the use case diagram of Figure 1 and activity diagram of Figure 2.

Patient dashboard on the Patient Portal showing the lab/radiological report and image upload.
Patient use case of the WB-RPMS Patient Portal/dashboard
Patients would be able to upload lab and radiological results and images.
Patient could view an appointment with the doctor.
They could view their personal data.
Patient could also view their past clinical encounter with the doctor.
Patient could download their past clinical encounter with the doctor as a PDF file.
Patient could view their own vital signs on the Patient Portal.
Patient could view feedback messages from the doctor, as shown in Figure 7.
Patient could view past lab and radiological results/images as shown in Figure 8.
They would be able to pay for an online consultation, as shown in Figure 9.
Patient could view appointments with the doctor, whether they have been approved or not.
Patient could view their own bill as uploaded by various departments.
Patient could log out securely.
Now shown above is an interface through which the patient could upload lab and radiological images and reports to the doctor. Given that these uploads are centred around orthopaedic care, all associated images and reports, including X-rays, MRIs, ultrasounds, CT scans and other investigative images, can be uploaded through this interface. Outpatient candidates can then come to the hospital when the doctor feels it is very necessary, saving time for the doctor to be able to see more critical patients; saving time, money and other risks for the patient; and helping the care facility to efficiently manage that existing space and expand access to health for those who are often turned back and requested to come on another date.

Patient's view of feedback messages from the doctor.
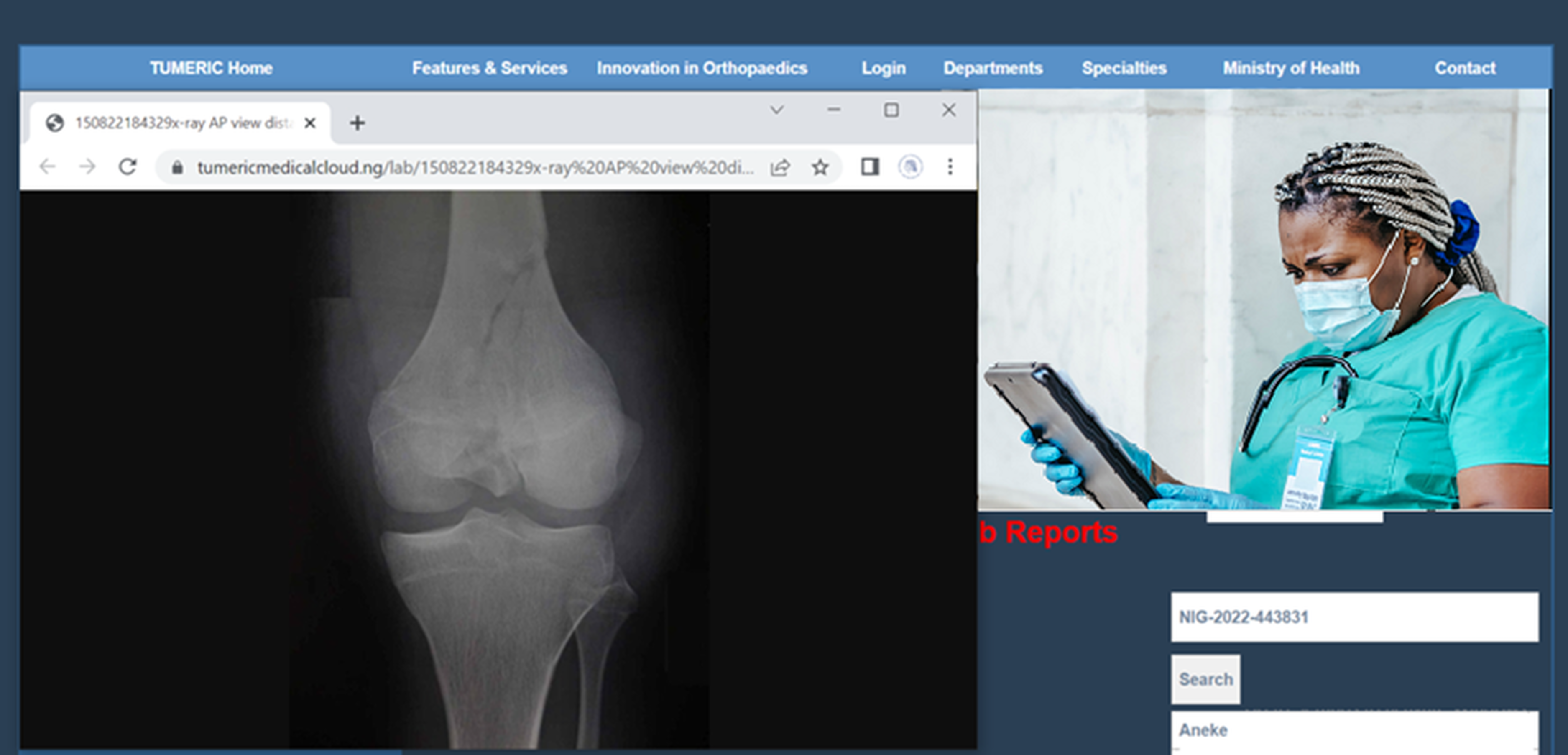
Anteroposterior X-ray view of the knee on the patient's interface on the WB-RPMS.

Patient's Online Consultation Payment interface.
Discussion
This research developed a WB-RPMS via a patient portal to support remote outpatient care management at the tertiary/university teaching hospitals in Nigeria during and after the COVID-19 pandemic. The WB-RPMS Patient Portal was carefully developed to guarantee a high degree of usability amongst Nigerian clinical stakeholders, particularly at the tertiary level. Again, the performance of the system shown through the evaluation result clearly showed it was well received amongst the patient sample respondents. It is also important to note that telemedicine/telehealth are still underutilised in Nigeria at the moment. In fact, in the work of Egbewande et al., 14 which investigated the potential of telemedicine in Nigeria, their result concluded that the usage of telemedicine in Nigeria isn’t as widespread as it could be and that this was due to a range of issues, such as the lack of a policy governing virtual care, inadequate financing, high costs for running virtual health services as well as technological and infrastructure problems. All these issues are hindering the potential of telemedicine to enhance healthcare delivery, access and efficiency.
Similarly, in the report of Ezeani et al., 26 it is not yet possible to experience the thrilling story and the benefit of telemedicine in Nigeria, as healthcare providers are still finding it difficult to incorporate this technology as part of their healthcare delivery model. The overall goal of the WB-RPMS Patient Portal development approach was therefore to ensure that all care provider feature expectations are fully integrated into the system design and development; hence, clinicians were part of the research and development team.
A similar study by Olufunlayo et al. 27 still showed that the overall level of digital maturity for telemedicine implementation across government funded tertiary institutions in Nigeria was still at the beginner level.
Another key piece of research that captured the type of telemedicine that was available in Nigeria during the COVID-19 pandemic and its degree of use was reported by Olutayo et al.. 28 It showed that out of the 103 doctors who responded to the survey, 93.3% of them agreed that they used some form of telemedicine during the pandemic. Specifically, out of about 1078 patients that were attended to during the period, 358 were attended to via WhatsApp (33.2%), 278 via phone calls (25.8%), 238 via SMS (22.1%), 154 via email and 50 via video call (4.6).
These approaches show that there was hardly a structured telemedicine app currently in place to support remote patient monitoring and management across most of the hospitals studied. On the contrary, WB-RPMS Patient Portal (when compared with existing implementations) appears to be a more structured and standard approach to express telemedicine and has the potential to expand and sustain access to healthcare even in challenging times of global and regional disruptions!
Limitations of the study
There were two significant limitations to this study. Firstly, the approach used to evaluate each participant's level of computer literacy through the administered survey was subjective. The results and feedback received from the participants, though highly impressive, may not reflect exactly the very high level of digital literacy recorded as result. To address this issue, the researchers confined the evaluation of the WB-RPMS Patient Portal to a patient-representative sample with potential for high digital literacy. Additionally, the respondents were diverse, representing different cultures and tribes in Nigeria, and were participating in the National Youth Service Corps scheme. However, the researchers recognise the need to adopt a more objective approach to digital/computer literacy evaluation in future studies.
Another limitation was the inability to include real patients in the evaluation of the WB-RPMS Patient Portal. This was due to the fact that the patients who presented themselves for outpatient clinics at these teaching hospitals were often visibly dealing with precarious health challenges, and it would appear insensitive to want to subject them to evaluation of a digital healthcare system. However, the researchers were able to mitigate this limitation by considering the fact that most individuals at some point in their lives would become patients and, therefore, any individual who meets other sample selection criteria could actually evaluate the WB-RPMS Patient Portal as a patient (representative).
Conclusion
Our investigation clearly demonstrates the efficacy and prospects of telemedicine via a WB-RPMS as a veritable tool to support improved access to affordable healthcare in a developing country, Nigeria, particularly for orthopaedic outpatients during and after the pandemics. The results of the final system evaluation showed that the system was well received among stakeholders. The researchers therefore recommend that WB-RPMS Patient Portal be adopted for use across tertiary/university teaching hospitals in Nigeria to support and sustain improved affordable access to outpatient healthcare service delivery and management.
Footnotes
Acknowledgements
This research had received huge support from clinical stakeholders across the teaching hospitals studied, and for this, the researchers are grateful.
Availability of data and materials
The researchers had also made efforts to ensure the availability of the data generated during this research. Reasonable requests can be channelled through the corresponding author.
Contributorship
U.S.O. oversaw the distribution of the questionnaires to the patient representatives and conducted data analysis. U.S.O. designed the interface and interaction of the WB-RPMS Patient Portal prototypes. U.S.O. was also responsible for writing up the manuscript and conducting data analysis. The very senior clinicians W.O.O., O.O. and O.A.L. provided most clinical requirements for the design of a collaborative WB-RPMS Patient Portal and reviewed iteratively all prototypes, making all suggestions, until a final acceptable product was achieved, which they also approved. This project is part of a series of research projects in the area of health digital transformation in developing countries and is supervised by T.S., N.P. and F.B. All authors read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The researchers, respectively, applied to the ethical committees of each of the tertiary hospitals, and approval was given and granted in writing. These three approvals from the three hospitals, respectively, enabled the researchers to have a wide range of access across various departments, units and stakeholders at the three care facilities.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
OUS.