
Abstract
Purpose
Telemedicine services have been recognized as a safe and affordable method for providing continuous healthcare services, especially to patients with chronic diseases. Despite all advantages, the use of this technology has faced several challenges particularly during COVID-19. The aim of this study was to investigate physicians’ and patients’ with diabetes perspectives about challenges of using telemedicine during the COVID-19 pandemic.
Methods
This survey study was conducted in 2023. The participants were endocrinologists, internal medicine specialists, general practitioners (GPs), and patients with diabetes in five teaching hospitals located in one of the underprivileged areas in Iran. Data were collected using a 5-point Likert-scale questionnaire and analyzed using descriptive statistics and the Kruskal–Wallis test.
Results
In this study, 95 questionnaires were completed by 60 patients with diabetes (30%), 21 GPs (70%), 10 internal medicine specialists (66.6%), and 4 endocrinologists (80%). The results showed that technical (4.42 ± 0.57), clinical (4.25 ± 0.52), organizational (4.23 ± 0.56), and individual (4.02 ± 0.42) challenges were the most important challenges, respectively. However, there was a statistically significant difference between the perspectives of the specialists, GPs, and patients with diabetes in terms of individual, clinical, technical, and organizational challenges.
Conclusions
Since the use of telemedicine for patients with diabetes faced several challenges during the COVID-19 pandemic, it is necessary to consider practical solutions to overcome these challenges in order to improve quality of services and increase the use of this technology, particularly in underprivileged areas. Moreover, the effectiveness of these services in different contexts, and for people with different economic conditions should be investigated in the future.
Keywords
Introduction
Diabetes is a metabolic disorder resulting from genetic and environmental factors and is characterized by high blood glucose levels. 1 Three main types of diabetes are type 1 diabetes (T1D), type 2 diabetes, and gestational diabetes mellitus. 2 Diabetes has also been identified as one of the most common comorbidities in individuals with COVID-19,3,4 and a risk factor for increasing the severity of COVID-19 and its complications. 5 Apart from this, social distancing and quarantine requirements resulted in reduced frequency of in-person visits because of the fear of exposure to infection. 6 In addition, lockdown strategies restricted access to healthcare facilities for the majority of people and affected the management of noncommunicable diseases like diabetes. This was along with limited access to physicians, limited follow-up visits, inappropriate therapies, decreased medication adherence, changes in dietary patterns, reduction in physical activity levels, and decreased social interactions leading to mental health problems. 7
During the COVID-19 crisis, caring for patients with diabetes also faced some new challenges due to the concentration of financial, physical, and human resources toward the crisis management. Some of these challenges included limited access to health education, delays in conducting laboratory tests, and low adherence to medication regimens. 8 These challenges impacted the usual care of patients with diabetes, and in turn, lead to poor blood sugar control or worsened patients’ health condition.9,10 To overcome these challenges, the use of telemedicine services has been suggested to facilitate patient monitoring. 11
According to the World Health Organization, telemedicine is the provision of healthcare services where distance is a significant factor. 12 Some examples of telemedicine services are phone-based services (the use of regular phones or smartphones to consult with patients, healthcare providers, etc.), two-way audiovisual communication (like real-time videoconferencing which allows patients and healthcare providers to see and hear each other during consultations), remote patient monitoring (RPM) which includes devices specifically designed to monitor patients’ health conditions remotely, and mobile Health services which refer to the use of mobile technologies to support and improve healthcare.13–15
In general, telemedicine refers to a set of services that can be provided remotely and is designed to empower patients and physicians or healthcare providers. 16 Recently, with the increased use of telemedicine technology, the internet, and smartphones, RPM and provision of long-term care have been facilitated, 17 and during the COVID-19 pandemic, telemedicine has provided an opportunity for patients with diabetes to receive health care services easily. 18 For instance, teleconsultation services reduced the need for travel, travel-related expenses, taking leave from work, waiting time, and ultimately the risk of exposure to COVID-19. By using telemedicine, patients who are even in remote areas will be able to have regular interactive sessions with their physicians and receive proper treatment and monitoring services. 18
Bonora et al. showed that despite the limitations in physical activity and psychological stress related to quarantine during the COVID-19 pandemic, blood sugar control in patients with T1D improved via using telemedicine. 10 However, the inability of users to use technology or a lack of access to the internet and interactive media could hinder the use of telemedicine technology. In addition, challenges such as concerns over privacy of information and virtual patient–physician relationships made the use of this technology more difficult. 2 Given that self-care for patients with diabetes is essential, especially during the COVID-19 pandemic, and the use of telemedicine technology always faces several challenges, it seems that investigating physicians’ and patients’ perspectives can help to support more effective use of this technology as well as realizing its benefits.
Methods
This survey study was conducted in 2023. Prior to the study, ethics approval was obtained from the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.REC.1400.727). The participants were divided into two groups: physicians and patients. Physicians included endocrinologists (n = 5), internal medicine specialists (n = 15), and general practitioners (GPs; n = 30) who worked in five teaching hospitals affiliated with two medical universities located in an underprivileged area in the southeast region of Iran. As the number of physicians was limited, no sampling methodology was used and all of the physicians were invited. The second group was patients with diabetes who visited their physicians in these five hospitals. To select the patients, convenience sampling methodology was used, but only patients who were familiar with information technology were included in this study and those who were not familiar with the technology (e.g., computers and mobile phones) or didn’t use them in their daily life were excluded from the study. Due to the large number of patients, the research team decided to collect data during a two-week period (February 12, 2023, to March 7, 2023). In this period, 200 eligible patients were invited to take part in the study; however, only 60 patients completed the questionnaire. Before collecting data, a signed, written informed consent was obtained from all participants of the study.
To collect data, a questionnaire was designed based on the results of a previous scoping study.19 The validity of the questionnaire was assessed by three experts in medical informatics, and its reliability was calculated using Cronbach's alpha (α = 0.953). The questionnaire was designed based on a 5-point Likert scale (not important (1), slightly important (2), moderately important (3), important (4), and very important (5)) in four sections: individual, clinical, technical, and organizational challenges of using telemedicine for patient with diabetes during the COVID-19 pandemic. The questionnaire consisted of 58 questions, including individual challenges (18 questions), clinical challenges (6 questions), technical challenges (13 questions), and organizational challenges (20 questions) (Supplementary file).
The researcher (FM) visited the selected teaching hospitals and provided the research participants with a paper-based questionnaire. Having data collected, they were analyzed using SPSS software version 25. Initially, descriptive statistics (frequency, mean value, and standard deviation) were calculated. Then, the Kolmogorov–Smirnov test was applied for each of the participating groups to assess normal distribution of data. As the distribution of data was not normal for the participating groups, the Kruskal–Wallis test was used to compare the opinions of different groups. The pairwise comparison test was also performed for subsequent comparisons between groups.
Results
The total number of respondents was 95. Four endocrinologists (80%), 10 internal medicine specialists (66.6%), 21 GPs (70%), and 60 patients with diabetes (30%) participated in the study. Among patients (n = 22, 36.7%) and the specialists (n = 7, 50%), the age group of 41–50 years and among GPs (n = 16, 76.2%), the age group of 21–30 years had the highest frequency. The majority of patients were women, and the majority of physicians were men. In terms of education level of patients, the highest frequency belonged to the bachelor's degree (n = 20, 33.3%).
Regarding the individual challenges of using telemedicine for patients with diabetes during the COVID-19 pandemic, patients’ preference to receive face-to-face services was the most important individual challenge from the specialists’ (4.93 ± 0.26), GPs’ (4.81 ± 0.40), and patients’ (4.70 ± 0.64) perspectives. The specialists also believed that the low level of user acceptance, the low level of patients’ and their families literacy, and a lack of access, or limited access to technology were other important individual challenges (4.93 ± 0.26), and the lack of access to multilingual resources for users (patient, patient's family, and service provider) (2.93 ± 0.73) was the least important one. From the GPs’ perspectives, the lack of access to multilingual resources (3.10 ± 0.94), and from the patients’ perspectives, the limited use of telemedicine by non-native speakers (3.10 ± 0.81) were the least important individual challenges.
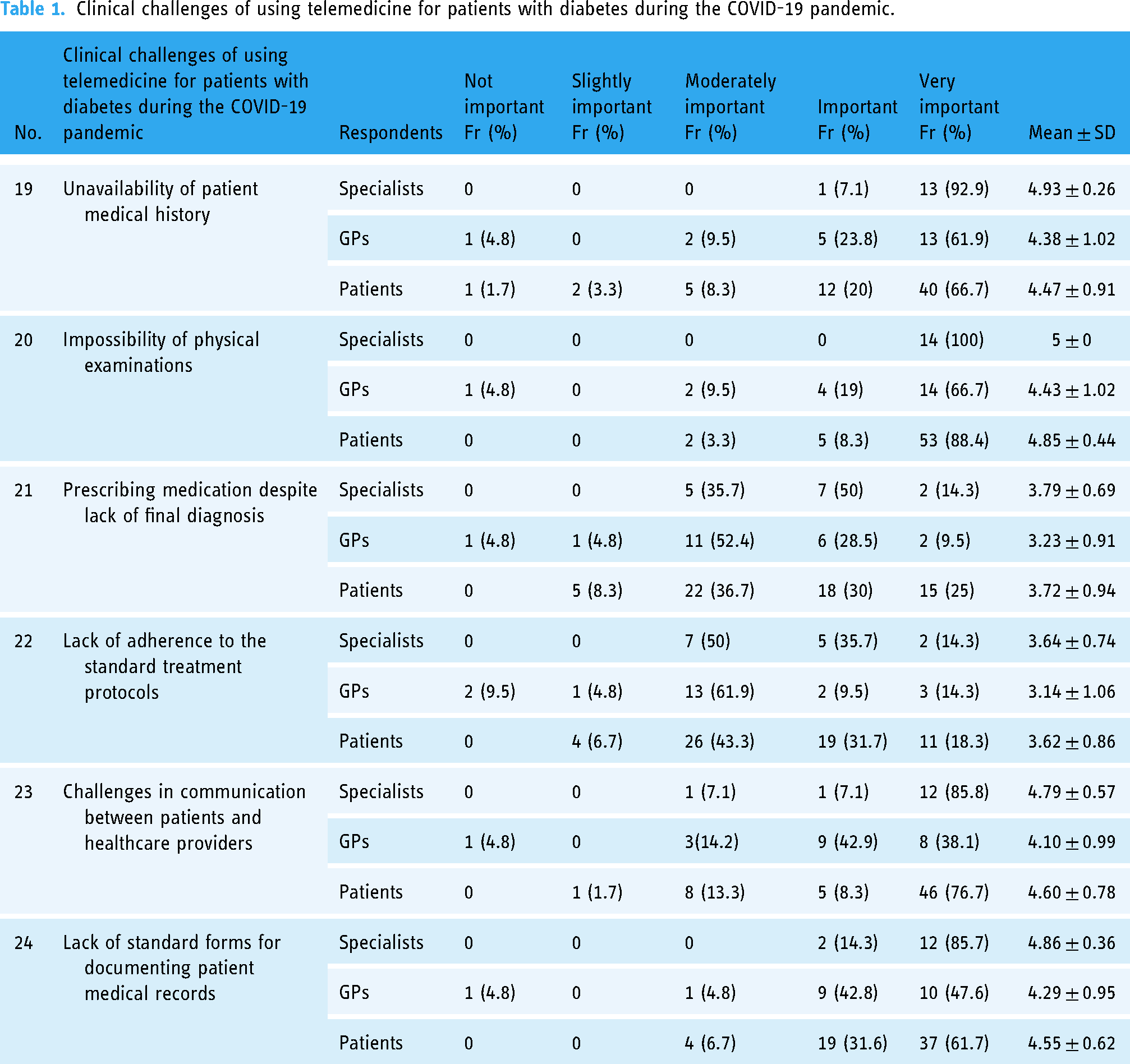
All of the participants (specialists (5 ± 0), GPs (4.43 ± 1.02), and patients (4.85 ± 0.44)) believed that the impossibility of physical examinations was the most important clinical challenge of using telemedicine for patients with diabetes. The least important challenge was the lack of adherence to the standard treatment protocols which was mentioned by all of the respondents (specialist (3.64 ± 0.74), GPs (3.14 ± 1.06), and patients (3.62 ± 0.86)). Table 1 shows the participants’ responses regarding the clinical challenges of using telemedicine for patients with diabetes during the COVID-19 pandemic.
Clinical challenges of using telemedicine for patients with diabetes during the COVID-19 pandemic.
Most of the respondents believed that technical challenges played a significant role in the use of telemedicine for patients with diabetes during the COVID-19 pandemic. According to the specialists, lack of an integrated tool for documenting data (including self-assessment data, screening questionnaires, and sharing the results of blood tests) (4.93 ± 0.26) was the most important technical challenge. From GPs’ and patients’ perspectives, patients’ lack of access to electronic devices (4.67 ± 0.48) and lack of access to high-speed internet services (4.70 ± 0.78) were the most important technical challenges, respectively. Difficulty in retrieving information from different databases (specialists (4.21 ± 0.57) and patients (3.88 ± 0.95)) and the complexity and nonuniformity of digital platforms (GPs (3.95 ± 0.86)) were the least important technical challenges.
In terms of the organizational challenges, the specialists believed that inadequacy of providing patient-centered healthcare services (5 ± 0) and inadequacy of users’ training (patient, patient's family, and service providers) (4.93 ± 0.26) were the most important challenges. However, the GPs were more concerned about a lack of an electronic health records system in hospitals to integrate patient data (4.38 ± 0.92) and a lack of a long-term strategic plan (4.38 ± 1.11). The specialists (4.07 ± 0.61) and the GPs (3.57 ± 0.97) thought that the inadequacy of rules for financial support via insurance companies was the least important organizational challenge.
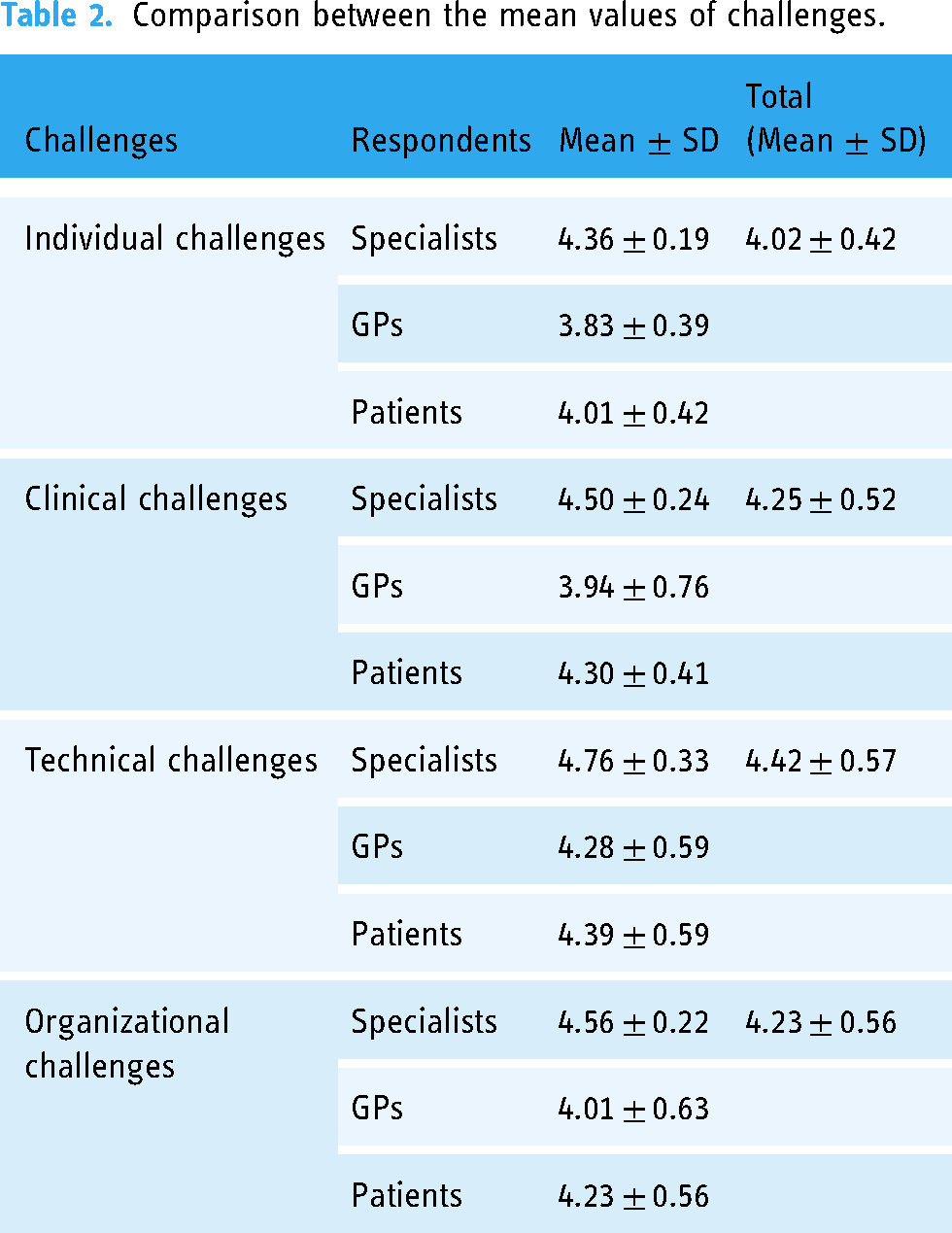
For patients, limited knowledge of healthcare providers about the ethical aspects of telemedicine (4.63 ± 0.68) was the most important, and intensive work processes in the healthcare centers (3.88 ± 0.84) was the least important organizational challenge. Overall, the results showed that technical (4.42 ± 0.57), clinical (4.25 ± 0.52), organizational (4.23 ± 0.56), and individual (4.02 ± 0.42) challenges were the most important challenges, respectively. Table 2 shows the mean values for each group of challenges based on the respondents’ perspectives.
Comparison between the mean values of challenges.
As Table 3 shows, the Kolmogorov–Smirnov test demonstrated that the score distribution for the individual challenges in the patient’s group, clinical challenges in the GPs and patients groups, technical challenges in the specialists and patients groups, and organizational challenges in the specialists and patients groups were not normal (p > 0.05). Therefore, the Kruskal–Wallis test was used to compare the opinions of different groups.
The results of the Kolmogorov–Smirnov test.

*Significant difference at the level of 0.05.
The results of the Kruskal–Wallis test showed that there was a significant difference between the individual (p = 0.000), clinical (p = 0.003), technical (p = 0.004), and organizational challenges (p = 0.009). To understand the differences among the respondents, a pairwise comparison test was conducted. The results of this test are shown in Table 4.
Results of the pairwise comparison test.

*Significant difference at the level of 0.05.
According to Table 4, regarding the individual challenges, there was a significant difference between the opinions of specialists and GPs (p = 0.000), specialists and patients (p = 0.002), and GPs and patients (p = 0.030). In terms of the clinical challenges, a statistically significant difference was observed between the opinions of specialists and GPs (p = 0.001), and GPs and patients (p = 0.013). Regarding the technical challenges, there was also a significant difference between the opinions of specialists and GPs (p = 0.002), and specialists and patients (p = 0.004). In relation to the organizational challenges, a significant difference was observed between the opinions of specialists and GPs (p = 0.002), and specialists and patients (p = 0.019).
Discussion
In the present study, the perspectives of specialists, GPs, and patients with diabetes on the challenges of using telemedicine during the COVID-19 pandemic were investigated. The comparison of the mean values for individual, clinical, technical, and organizational challenges showed that technical, clinical, organizational, and individual challenges were the most important challenges, respectively. For the specialists and GPs, technical and organizational challenges, and for patients, technical and clinical challenges were the most important challenges of using telemedicine during the COVID-19 pandemic.
Regarding technical challenges, one of the reasons that prevented patients from using telemedicine was the weak internet connection and limited access to high-speed internet networks, especially in developing countries and underprivileged areas, which disrupts communication and interactions. The results are in line with the findings of other studies in which technical issues were the most reported challenge. 20 Bhatia et al. reported that technical difficulties were more obvious during making a video visit and patients and clinicians needed to receive more formal training. In-home technical assistance and getting access to low-cost or free broadband internet, especially for those living in geographically deprived areas can be a solution to overcome this challenge. 21 The insufficiency of technical infrastructure, 22 the lack of strong technical support and limitations in providing patients with technical support when they use the technology 23 were also highlighted by other researchers. These challenges need to be addressed properly, otherwise they force patients to ignore using telemedicine technology and choose face-to-face consultations. 24
In terms of clinical challenges, sometimes patients and clinicians believe that telemedicine does not fully meet the necessary standards for medical examinations and it is difficult to perform some diagnoses virtually. 25 They believe in-person visits provide higher quality services compared to the telemedicine visits, as care providers observe them and complete a physical examination. 21 As a result, any prescriptions and treatments are based on the final and more accurate diagnosis. 26 Although the accessibility of Internet of Medical Things (IoMT) is increasing and patients are able to provide data in a quicker manner along with using telemedicine services, this has also led to sometimes overuse of devices and increasing dependency on the collected data rather than actually assessing the clinical symptoms. The reliability of the data collected by IoMT devices can also be a challenge, as there might be false positives that emerge more frequently due to the lack of proper calibration of devices. 27 Murphy et al. showed that televisits may result in incorrect referrals and poor diagnosis, and about 18.5% of unsuccessful visits need further evaluation. 28 Therefore, more research on the clinical effectiveness of telemedicine services and devices is required, and the quality of visits, final diagnoses, and treatments need to be monitored constantly.
Regarding the organizational challenges, several recent works suggested that the neglect of changing the work processes is the main challenge to the implementation of telemedicine. In this case, the processes need to be redefined to match organizational perspectives and gain support from managers. The telemedicine implementation needs more effort to align the processes with the organizational strategy. 29 For instance, nonreimbursement or limited reimbursement of telemedicine services can cause concerns over providing high-quality services.21,30,31 In addition, several studies highlighted the importance of user training for the use of telemedicine technologies.21,32–34 As the use of telemedicine technology is a new work process, it is important to redefine all related processes to overcome any interruptions in routine activities. In particular, financial and contextual issues need to receive adequate attention to facilitate the implementing of new processes successfully.
In terms of individual challenges, a number of issues related to privacy, data protection, and confidentiality of medical information should be considered. Both healthcare providers and patients must be assured that the processes of data transfer and data storage in a televisit are confidential and secure. 35 Another challenge is cultural sensitivities, and individuals might not be interested in receiving care provided by the healthcare providers in other geographical areas with cultural differences. 36 Although telemedicine may increase access to healthcare services, some ethnic groups and those experiencing economic deprivation may have less access to computers, smartphones, and the internet, which potentially creates inequality in access to telemedicine services. 37 Similarly, the results of various studies showed that patients who were older found it difficult to acquire digital literacy and did not have sufficient access to advanced technologies such as laptops and smartphones. 38 Older adults prefer face-to-face visits, as they believe this method of care is more reliable and easier for them. As a result, they have less interest in using telemedicine. 25 Apart from the mentioned individual challenges, there might be many other factors at the individual level that should be identified and addressed appropriately to improve the use of telemedicine technology.
According to the findings, there was a significant difference between the mean values of individual, clinical, technical, and organizational challenges among different groups of the respondents, and the mean values obtained for the specialists were higher than other two groups. This suggested that the specialists were more concerned about the individual, clinical, technical, and organizational challenges mainly due to their work experience, a range of patients that they visited, and their deeper understanding of patient conditions. For the specialists and GPs, technical and organizational challenges, and for patients, technical and clinical challenges were the most important challenges. This shows that users’ perspectives and priorities about different issues might be different. Therefore, to implement telemedicine technology successfully, different stakeholders should be identified, and their requirements need to be investigated and addressed properly.
Research limitations
One of the limitations of this study might be related to the limited number of participants. Although all of the physicians and more than 200 patients were invited to take part in the study, a limited number of the individuals completed the questionnaire. This might be related to their interest in the topic of the research and their workload. Therefore, conducting another study using a bigger sample size, collecting data in other areas of the country, and comparing the findings across these areas might be useful to gain a better understanding of challenges of using telemedicine for patients with diabetes during the COVID-19 pandemic. This will also help to improve the generalizability of the findings. Moreover, the data were collected from one of the underserved areas of the country, in which patients might not be computer-literate enough or may not be familiar with the importance of using telemedicine for managing their diseases. Therefore, we decided to ask people who were familiar with information technology to complete the questionnaire. In future studies, different user groups can be identified and invited to take part in the study.
Conclusion
In this study, the challenges of using telemedicine for patients with diabetes during the COVID-19 pandemic were investigated from the specialists’, GPs’, and patients’ perspectives. The results showed that technical, clinical, organizational, and individual challenges were the most important challenges, respectively. Therefore, it can be concluded that for a successful implementation of telemedicine technology, especially during pandemics, it is essential to evaluate and prioritize these challenges. This will help improving quality of care, reducing costs, ensuring continuity of healthcare services, preventing waste of time, and controlling infection. Future research can focus on other telemedicine users and their requirements to provide a deeper understanding of challenges and related solutions.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251325969 - Supplemental material for Users’ perspectives about challenges of using telemedicine for patient with diabetes during the COVID-19 pandemic
Supplemental material, sj-docx-1-dhj-10.1177_20552076251325969 for Users’ perspectives about challenges of using telemedicine for patient with diabetes during the COVID-19 pandemic by Fatemeh Mirasghari, Haleh Ayatollahi and Farnia Velayati in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251325969 - Supplemental material for Users’ perspectives about challenges of using telemedicine for patient with diabetes during the COVID-19 pandemic
Supplemental material, sj-docx-2-dhj-10.1177_20552076251325969 for Users’ perspectives about challenges of using telemedicine for patient with diabetes during the COVID-19 pandemic by Fatemeh Mirasghari, Haleh Ayatollahi and Farnia Velayati in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors gratefully acknowledge Iran University of Medical Sciences for supporting this study.
The datasets used and/or analyzed during the current study are available from the corresponding author upon a reasonable request.
Contributorship
FM conducted the research and drafted the manuscript. HA supervised the research. HA and FV participated in the review process and the critical review of the manuscript. All authors reviewed the manuscript and declared their final approval for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethics approval was obtained from the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.REC.1400.727). All respondents signed an informed written consent form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.