
Abstract
Background
Digital health technology (DHT) has become an essential part of an effective and efficient healthcare information system. Although DHT promises great potential it does not always meet the expectation of users. Often, in low- and middle-income countries (LMICs), the implemented DHT does not function as intended and impacts negatively on health professionals and their work. Therefore, this study explored the views of participants about the impact of DHTs on the work of health professionals after it has been introduced in Ghana.
Methodology
The study used a qualitative research approach where in-depth interviews (IDIs) were conducted with study participants across three health facilities in Ghana. A purposive sampling technique was used to select participants. All interviews were audio recorded, transcribed, and coded into themes using QSR Nvivo 12 software before thematic content analysis.
Results
Our findings revealed that DHT reduced the workload on the healthcare providers and also ensures continuity of care. Participants perceived that DHT was fast, and ensures quality and accurate information, which could be easily accessed by health professionals for better decision making. However, poor internet connectivity and erratic power supplies were reported as the main impediments causing delays and frustrations to the staff at the study health facilities.
Conclusion
The study found that DHT has a positive effect on the work of health professionals. However, poor internet connectivity and unstable power supply caused delays in the provision of care and disruptions in the work process affecting the smooth operation of the DHT and threatening to erode the potential benefits to the health system and users.
Introduction
Digital health technology (DHT) has the potential to improve healthcare delivery and enhance patient safety.1,2 Its adoption and use for the provision of healthcare services is fast gaining pace.2–5 DHT has been recognised as an essential part of an effective and efficient healthcare information system that ensures positive health outcomes.6–8 The utilisation of this technology in healthcare offers a wide variety of benefits. These include the elimination of time-consuming procedures in recording patient data, which has been associated with paper-based systems, provision of easy access to patient information, increased use of practice guidelines, enhanced communication between healthcare providers and patients, better decision making and reduced medical errors.4,9
DHTs are of high priority in developed countries and have been used to achieve many feats in these settings.3,10 However, the health systems in many low- and middle-income countries (LMICs) are faced with challenges such as inadequate funding, limited resources and poor infrastructure, making the outcome of DHT implementations unpredictable in these settings, and its impact and utilisation uncertain.10–14
Poor implementation of DHTs have been associated with unintended consequences that sometimes leads to negative effects such as decreased time efficiency, poor quality of care and increase threat to patient safety. Though, a lot of benefits resulting from the use of DHTs have been reported in current literature,9,15–17 the technology could distract clinical workflow and cause workaround. 18 Further, DHT has been perceived by clinicians to cause burnouts, increase workload and time spent on documentation. 18 Concerns have also been raised about security breaches threatening patient privacy and confidentiality of patient information. 19 Health workers are responsible for keeping patient information secure because they can be held liable for breach of patient confidentiality.20,21
In settings with acute infrastructure challenges, especially in LMICs, DHTs have been reported to be unreliable.9,12 The perceived impact of DHT on health workers has been varying and often misrepresented, raising concerns about the effectiveness and reliability of the electronic systems. 17
The Ghana Government initiated an eHealth strategy policy in July 2010. This policy plan aim was to improve healthcare delivery by streamlining and integrating Information and Communication Technology into the health sector. Additionally, the technology is expected to enhance healthcare operations and management as well as to promote evidence-based decision making.22,23 This will help the country to accomplish the objective of a paperless records and reporting system.
However, it is uncertain what effect the installed systems would have on health professionals and their work. Therefore, the study aims to explore the perception of health professionals about DHT and its impact on their work and to recommend steps to mitigate it. The specific objectives are to (a) explore the perception of healthcare professionals about using the DHTs to provide healthcare; (b) investigate the perceptions of health professionals about the impact of DHTs on their work; and (c) suggest means to mitigate the impact.
Methods
Study design
This was a cross-sectional exploratory study using a qualitative research approach where 40 in-depth interviews (IDIs) were conducted with healthcare professionals in three selected facilities between February and May 2022. Qualitative research technique enables study participants to share their views and rich experiences on a particular issue under investigation. 24 Therefore, this method was deemed appropriate because the study sought to investigate health professionals’ perceptions about the impact of DHT on their work.
Study site
The study was carried out in three selected public hospitals, each located in the Volta, Eastern and Central Regions of Ghana. Ghana is divided into 16 administrative regions. Each region is further divided in to metropolitans, municipalities and districts. For the purposes of anonymity, the selected hospitals have been labelled A, B and C. Hospital A is a district hospital located in the Volta region with a bed capacity of 96. It has critical staff strength of more than 100. It has five wards, each with bed capacity of about 20. Hospital B is a municipal hospital located in the Eastern region. It is one of three main hospitals serving the municipality and has a bed capacity of about 85 in its five wards, with critical staff strength of about 160. Hospital C is a referral hospital located in the Central region. It is one of three main hospitals that serve the metropolis. It has a bed capacity of about 250 and critical staff strength of about 300. These facilities were chosen because they had implemented an EHR system to provide healthcare services about the same time and were easily accessible to the researchers.
Targeted population
The targeted population in this study was healthcare professionals working in the three selected health facilities who use the DHT to provide health services.
Sampling techniques
Purposive sampling is a non-probabilistic sampling method which allows the researcher to choose study participants who they think are appropriate and can provide accurate information for the study. 25 This method is widely used in qualitative research to identify information-rich study respondents. 24 Therefore, this study used purposive sampling technique to select study regions, the three public hospitals and participants for the IDIs.
Letters were written to the administrative heads of the study hospitals explaining the rationale of the study to them and also asking for permission to interview selected health professionals who were involved in the use of DHT system. After obtaining permission from the heads, the study team led by the lead Author visited the study hospitals and with support from facility heads, a list of departments, health professionals using the DHT system were provided. Using the list, these health professionals were contacted and those who were available and consented to participate in the study were included.
Participant recruitment
Forty-five (45) respondents were purposively targeted from the selected health facilities, and forty (40) interviewed. When no new comments were emerging, we determined that saturation of data was reached.
Data collection procedures
The first author and an undergraduate student conducted the interviews. The student was already acquainted with the purpose of the study and therefore received 2 days training which focused on qualitative interviewing techniques. A pre-test was conducted at the end of the training. This helped to finalise the interview guide before the actual data collection. Appointments were booked with potential study participants prior to conducting interviews after obtaining written informed consent. The interviews were conducted with participants at the health facility level. Forty interviews were conducted in English. The interviews were recorded using an audio tape recorder with consent of study participants. Participants shared their experiences and views about the impact of DHT on their work and suggested strategies to mitigate challenges encountered using the DHT system. Table 1 shows detailed information on the category and number of health professionals interviewed in each selected hospital.
Category and number of health professionals interviewed in each hospital.
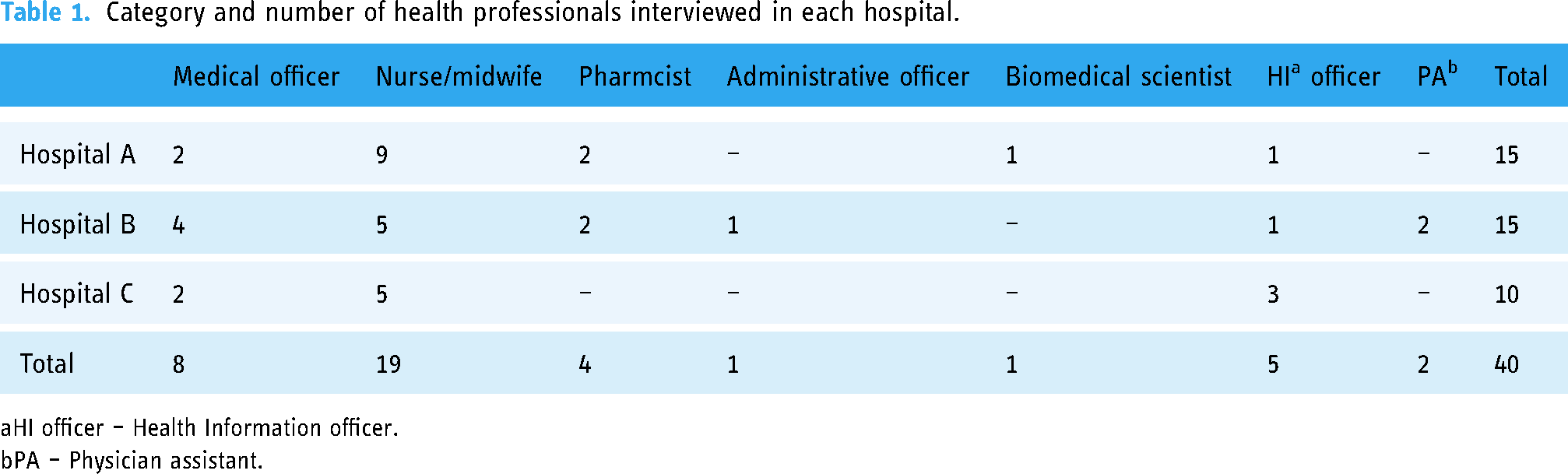
HI officer – Health Information officer.
PA – Physician assistant.
Data processing and analysis
The recorded interviews were transcribed verbatim after repeatedly listening to them. To ensure that qualitative principles for transcribing interviews were applied, two independent people with experience in qualitative research transcribed the recorded interviews. This was done to avoid bias in the transcription process. The transcripts were edited by the lead and second authors, without changing the original meaning of statements. Guided by the objectives of the study and the themes contained in the interview guide, a codebook was developed using a combination of established categories based on the original research questions (examples of broad themes included ‘Positive impact of DHT on health professionals’ work’, ‘Negative impact of DHT on health professionals’ work’, ‘Strategies to improve use of DHT’, etc.) and the sub-themes that emerged from the data such as ‘DHT guides in making good clinical decision’ and ‘Improve power supply and internet connectivity to support the use of DHT’. The transcripts were then prepared and imported into QSR Nvivo 12 software to facilitate data coding and analysis. To ensure a fair interpretation of the data, the coding was done by the first and second authors and validated by the co-authors. The coding process involved a critical review of each transcript and coding of the data into themes. Thematic content analysis was used to analyse the data. The results were presented as narrative and supported by relevant quotes from the data.
Ethical consideration
Ethical approval to conduct this study was sought and obtained from the Cape Coast Teaching Hospital Ethical Review Committee with approval number (CCTHERC/EC/2022/115). Administrative permission was also obtained from the heads of the health facilities. Written informed consent was obtained from all participants. All aspects of the study including the rationale, objectives and participants’ responsibilities in the study were all explained to them prior to their participation. Participants were not compensated for their time but were offered a bottle of water as refreshments. Also, participants’ rights were observed and they were told they could discontinue the interview any time without any consequences. To ensure confidentiality of information, personal designation and other related information which could be used to identify participants were not collected. Study participants were identified by codes assigned to them during the interviews.
Results
Demographic characteristics of participants
Table 1 describes the role and the number of health professionals interviewed in each hospital. All the participants had tertiary level education except two persons with diploma certificates. Seventeen (17) participants had between 1–5 years of working experience, nineteen (19) participants had 6–10 years of working experience, and four (4) participants had more than 11 years of working experience. The average number of working years of the participants was 8 years, with range (1–22) years. The majority of the participants (19) were nurses/midwives, eight were medical officers, and four were pharmacists. The remaining comprise five health information officers, two physician assistants, an administrative officer and a biomedical scientist.
Themes
Several themes emerged from this study which has been summarised in Table 2 and discussed in the results.
Main and sub-themes on the impact of DHT on health professionals’ work and suggested strategies for improvement.

Positive impact of DHT on work of health professionals
Fast and easy access to patients’ information
According to participants, the DHT had made work easier as compared to the paper-based system. They explained that since moving from paper-based to the electronic system, patient health information could easily be accessed anytime. Almost all the participants held that the DHT was fast and could help retrieve patients’ information with ease as exemplified in the quotes below: … since moving from paper-based record to electronic-based record patient health information can be easily accessed. (C. IDI 1, medical officer). …it easy to access client information; anytime you need it, just a click [and] you get all the medical records of the client which makes work easy and more efficient. (C. IDI 8, nurse Officer). It has massively and positively affected our work! I mean it has improved our work, as I was saying before, it has made retrieving of information very easy and information is not lost. (B. IDI 15, medical officer).
Reduced workload and medical errors
Most of the health professionals perceived that the introduction of the DHT had reduced their workload and also made their work easier compared to the paper-based system. “…actually it [DHT] has really decreased some of the things we use to do […] it has actually reduced some of the workload” (A.IDI 9, nursing officer). “It has made my work easier and more efficient, …, it has improved our work a lot, because one, it prevents delays, … so you (the staff) can focus on the client too to deal with every client at a time” (A. IDI 5, midwifery staff). …it reduces the workload and makes it easy to access client information; anytime you need it, just a click, [and] you get all the medical records of the client which makes work easy and more efficient. (C. IDI 8, nurse officer).
Some participants also reported that the DHT had reduced medical errors, which had helped to improve quality of healthcare delivery. Health professionals maintained that they were no longer struggling with illegible hand writing, which was a source of medical errors when they were using the paper system. …it has reduced medical errors, which has improved patient healthcare delivery. (C. IDI 2, medical officer). … it has affected my work in the sense that there is no more struggling to read illegible handwriting from other health professionals, which has reduced medical errors if comparing with paper record. (C. IDI 2, medical officer).
Reduced consultation processes and patient's waiting time
Views expressed by most participants suggested that the introduction of the DHT had shortened the consultation processes, making it possible for a lot of patients to be seen within a short period of time. Some participants also said that it facilitates doctors’ work on ward rounds, by eliminating difficulties posed by illegible handwritings when searching for patient information. …it [DHT] makes the time that you take to do your consultation very shorter, meaning you can see a lot of patients in a short period of time. So, it makes the work very efficient. (A. IDI 15, medical officer). …when it comes to diagnosis; when doctors come for Ward rounds, finding the diagnosis is easier unlike the written [paper system], where you will have difficulty checking the handwriting to see the actual diagnosis that the doctor has written. (A. IDI 8, nursing officer). …doctors are changed every now and then, so in case a new doctor wants a patient's record, he can access the information he needs on DHT; which ensures continuity of care, which has improved patient healthcare delivery. (C. IDI 2, medical officer).
According to participants, the DHT had reduced patients’ waiting time at the study health facilities. They explained that patients could receive health services and leave the facility early because of the use of the DHT system. They added that the technology had helped minimise loss of patient information at the study health facilities. Participants expressed their views this way in the following excerpts on the issue: … it has also reduced patient waiting time at the facility and it has also reduced loss of patient health information since it is not paper record which can get wet or get lost in storage. (C. IDI 1, medical officer). …our patients are able to leave the facility on time; so, as you can see, it has reduced the patients waiting time; at first, they used to stay here for a long time, someone can even spend the whole day here, but with the electronic system they are able to leave the facility very early, so I think has been helpful. (B.IDI 2, pharmacist).
DHT facilitates communication
The results also showed that the DHT provides them with the opportunity to capture relevant patient information into the system, thereby facilitating communication between other healthcare providers within the health facility. They said they could see what their colleagues have done. This is how some respondents expressed their views: .…the DHT gives you the opportunity to input relevant information into the system, so that all health workers, wherever they are in the facility can assess it and be able to continue care of clients who have previously been seen in the facility. (B. IDI 7, midwifery officer). …It has helped to easily exchange information within the facility or with other healthcare facilities. (C. IDI 5, health information officer).
…information is not lost and it promotes the continuity of care, you can even see what your other colleagues have done. (B. IDI 15, medical officer)
Ensures quality documentation and continuum of care
Study participants were thrilled by the DHT documentation capabilities. They mentioned that the DHT ensures accurate and quality data. Health professionals were of the view that they could easily access vital information from the system, which had helped to ensure continuity of care for their clients. Some of the participants expressed their views this way on the issue in the following quotes: “…it's good when it comes to data quality, if you open the system, you get everything you want to get; unlike the paper where some pages can be torn, some lost, but with the DHT everything you want, you will get it” (C. IDI 9, nurse officer). “When it comes to doing our documentation, because of the DHT it took us shorter time; it has two sides; one, record keeping has been okay and then continuum of care has been improved because I can at least review patient previous information,” (B. IDI 9, Senior medical officer). “…doctors are changed every now and then, so in case a new doctor wants a patient's record, he can access the information he needs on DHT; which ensures continuity of care.” (C. IDI 2, medical officer).
DHT guides in making good clinical decision
Some of the participants perceived that the introduction of the DHT provides needed information to make good and fast clinical decision for effective management, thereby avoiding wrong medical diagnosis and prescribing errors. Some of the respondents’ views are shared as follows: “…it will help you to take decisions as to what time you need to procure new stock. Yea, it makes you to be able to take decisions fast. You are able to get all the information to take decisions for effective management.” (A. IDI 11, pharmacist). “…it prompts you on some of the things, especially what to do and not to do when consulting…” (B. IDI 10, physician assistant). “…it helps me to take decisions that I need to […] you will see the medication the patient is supposed to take. So, if the patient just brings the number to the dispensary, I know what to dispense” (A.IDI, 11, pharmacist).
DHT enforces privacy, confidentiality and security
Some of the respondents mentioned that the DHT keeps patient information safe, secured and confidential. They mentioned that the DHT provides privacy of information, and it gets people to be accountable for everything they do, since the system tracks all activities. The views of some of the respondents are as follows: “… patient medical record is safe when you use the DHT to provide service than the paper-based record, because the patient folder can get wet or be misfiled which can stop continuity of care and also can bring legal charges to the facility” (C. IDI 2, medical officer). “…it also gets people to be accountable for everything written, because everything you write has your name and your ID attached to it; so, it helps to some extent in protecting the patient's confidentiality” (B. IDI 1, nursing officer). “Every individual or client has privacy of information because we use our passwords. Patient confidentiality is assured because access is controlled. I have a different interface; my staff have a different interface; you don’t have to leave it [password] for somebody to also use. Everybody uses his or her password” (A. IDI 5, medical officer)
Negative impact of DHT on health professionals’ work
Delayed in provision of care due to poor internet connectivity
Despite the benefits of using DHT, participants reported various factors affecting smooth operations of the technology. According to some participants, poor internet connectivity caused delays in the smooth operations of DHT. They held that each time the network connectivity went off, they were unable to work, and this delays the process of provision of care. For instance, patients are unable to get their medication on time, because the order has not been received at the pharmacy. Below is how some respondents expressed their frustration with the DHT: “There are instances whereby you will be working and the network will just go [off], it means you have to wait for a while, for the network to be restored before you can continue your work” (A. IDI 4, nursing officer). “…sometimes we do get intermittent network challenges. More so, supposing there is light outage; we would have to sit and wait for the light to come back; which delays our work” (B. IDI 13, health information officer). “When the network is not that good, the patients go to the pharmacy to collect their drugs and they tell them it has not appeared so they have to come back for it to be retyped and go again. That's is the only sad aspect” (C. IDI 1, medical officer).
Disruption in work process due to unstable power supply
According to the participants, unstable power supply is another pain to contend with when using the DHT. The participants mentioned that the erratic power supply caused unplanned system shut down. When the system goes down, work comes to a halt and patients’ information is temporary lost and has to be re-entered again when power is restored. Entering the patient information again is viewed by the health professionals as double work. The views of some respondents are expressed as below: “…my main challenge is when the light goes out or you are working and it [system] happens to go off; you are not able to continue from where you ended up with; you will have to enter everything all over again; that's the main challenge” (B. IDI 6, medical officer). “…but the issue I have with DHT is that whenever the light goes off, work comes to a halt. (C. IDI 1, medical officer).
Strategies and suggestions for improving the DHT
Various strategies were recommended by participants to improve the use of DHT.
Improve power supply and internet connectivity
Almost all participants mentioned that improved network system, internet connectivity and power supply could facilitate smooth operations of the DHT system at the study health facilities as illustrated in the following quotes: Sometimes we have problem with the network. The network is poor and then sometimes the ‘on and off light off’. Our plants (generator system), sometimes does not work. So, if they can work on that, we will be very glad. (A. IDI 2, nursing officer). For me, most of this electronic stuff thrives on internet access and our system isn’t strong in that, so if there is anything to do, internet access should be worked on and made stable all the time, so we do not have to restart each time the system is down. (B. IDI 9, medical officer). There are a lot of things to be done but the major one is the internet service because whenever there is light out, it affects the work where clients complain of time wasting. (C. IDI 10, nursing officer).
Adequate supply of equipment and maintenance
Some other participants were of the opinion that the provision of adequate equipment and regular maintenance to avoid frequent breakdowns could improve the DHT system. Okay: [one] is frequent replacement of gadget. [When] the gadget breaks down it brings everything to a halt; [two], ensure 24-hour power supply and as well as internet connectivity (A. IDI 7, nursing officer). I will suggest that they make computers available at my facility; they should improve the software system that we are using, so as to capture other aspects that are not in our system now (B. IDI 14, medical officer). “…I think the [issues with] internet service should be addressed and we need more computers, tablets to work with, because the ones here are not enough” (C. IDI 1, medical officer).
Adequate training
Training on the software was also suggested by participants to improve on the DHT usage. Some participants held that there was need for regular training to improve knowledge and usage of the technology especially people who had challenges using the system. I will suggest that there should be a lot of training on the DHT system … (C. IDI 2, medical officer). I suggest day in day out, the experts will come in and then teach those who are still finding challenges with the system (B. IDI 11, nursing officer). I think proper training of health workers on the DHT system will improve healthcare delivery (C. IDI 9, nursing officer).
Discussion
The current study assessed the perception of the impact of DHT on healthcare professionals and their work in selected hospitals in Ghana. The DHT implementation had both positive and negative impact on the healthcare professionals as has been revealed by other studies.9,26
In this study, DHT was perceived to have impacted positively on healthcare professionals’ work by reducing the workload of the clinical staff and time spent by patients to receive services as compared to the paper-based system. This notable finding can be attributed to the speed and ease with which the DHT helps in searching and retrieving of patient information as compared with the paper-based system. This outcome cuts across the three hospitals and is consistent with other studies.4,9,18,26 The study also revealed that documentation improved and medical errors reduced. This is because the DHT ensures accurate and quality data. Often the sources of medical errors when using the paper-based system are from illegible handwriting, which has been eliminated by the structured nature of the electronic systems.9,27,28 Paper-based systems have been associated with difficulties in documenting and retrieving of patient information. Studies have revealed that DHT facilitates the care processes by hastening search, retrieval and documentation of patient information. 4 The current study also reports perceived improvement in quality of data, which has helped to facilitate effective communication between staff and also improve consultation processes, thereby enhancing continuity care. 29
When care providers are able to access accurate information timeously, they are able to make quick and better-informed decisions. Improved communication between multidisciplinary team and the elimination of time-consuming procedures in recording have been reported to enhance decision making. 9
While health systems in LMICs are faced with several constraints, in our study the most notable constraints that influenced the implementation processes and negatively impacted on health professionals’ work were poor internet connectivity, unstable power supply and inadequate equipment. These negative effects were also sources of frustration to staff. 30 Delays reported in the care processes were due to unplanned system shut down or downtime caused by erratic power supply and poor internet connectivity. The use of power generators and portable uninterrupted power supply would have been a solution. However, in this study although power generators were available, they did not function because of lack of fuel. The availability of funds to purchase fuel for the generators is a difficult choice to make between many competing health needs. These findings are consistent with other studies.12,18,31 Healthcare managers should take advantage of abundance of sunlight in these settings and explore alternative power sources, such as solar energy, as a stopgap when power supplies are cut off. This may require an initial investment; however, they are far cheaper to run and maintain in the long term. In addition, low voltage consuming computers and equipment should be factored into the implementation process. This ultimately may wean the dependence of the health facilities on the national grid. The issue of poor internet connectivity could be addressed through the development of a support system so that data entry could be done offline, with auto synching of data on the main server at a later time. This approach has been explored by Ayebazibwe et al. 32 to address an issue of internet accessibility.
In our setting, provision of stable internet connectivity is intrinsically linked to funding issues.12,33 This calls for the intervention from the central government and other key players in the health industry. For example, the central government can leverage on its position through a policy framework and establish an agreement with telecom companies to provide stable internet access to the health facilities. 32 This approach has been explored in other studies.9,32 where the government as the major player in the healthcare used its influence to promote the adoption of the EHRs through the implementation of complex policy framework and controlling cost of the input. 9 A robust and stable internet infrastructure is the backbone of DHTs. The huge investment required in the provision of internet connectivity may be beyond the budget of many health facilities. It is not enough for the central governments to provide the initial DHT investments in terms of the implementation, but also to provide the necessary policy direction and to regulate the critical infrastructure in the industry. 9 For example, a policy of spreading fast and stable internet connectivity across the country would benefit health facilities in underserved communities and solve issues of accessibility to specialist care in these communities.
To realise the full benefits of DHT, the system has to function as intended. Often, DHTs implemented in many LMICs do not function as intended, because constraints, such as inadequate equipment and poor internet connectivity become obstacles to implementation and sustainable use of the system. A study that investigated health professionals’ perception on DHTs use, data quality and data reuse, revealed that most of the research participants perceived the new DHTs not to have met their expectations, because the system did not function as intended. 34
DHTs just like any technology can cause frustration to new leaners. 35 It is not surprising that staff with limited typing or computer skills would want to revert back to the paper-based system. When systems are not functioning as intended, they tend to bring negative attitudes. Some of these negative attitudes have been attributed to person with computer phobia. 29 These tendencies however can be overcome by provision of adequate training before, during and after implementation of the system.
Our current finding also shows that DHTs provides safe and secure environment for patient information. This finding is collaborated by other studies.9,36 Access to patient information is protected by different user access control levels which serves as source of security and endures confidentiality.
Limitations
Some limitations are worth mentioning. The choice of qualitative approach and purposive sampling methods for participant selection limits the generalisability of the findings to other settings. Future studies that include larger, randomised sample sizes and employing a mixed-method approach would add rigour. Also, the inclusion of patient perspectives could further enrich the understanding of the impact of DHT and probably translate into improved patient experiences and outcomes. The study design did not consider the impact of the cost of implementing the DHT would have on patient care. Future research could address this gap by incorporating cost–benefit or cost effectiveness analysis of the DHT. The full potential of DHT in improving global health can only be realised when these aspects are thoroughly addressed.
Conclusion
DHT has had a positive impact on healthcare professionals and their work. DHT was perceived to have reduced workload and drastically enhanced the documentation quality. It may have facilitated communication between staff and improved decision making, hence provision of safer and improved quality of care. However, these positive effects sometimes were eroded by poor internet connectivity, frequent system shut downs that caused delays in the provision of care, disruption of work processes, and temporary loss of information and were a source of frustration to care providers and patients.
Footnotes
Acknowledgements
The authors wish to thank all study participants for their valuable time they shared during the study. The authors are also grateful to the heads of the health facilities for their support and permission to conduct the study in their facilities. Finally, we would like to thank all those who arranged the necessary logistics for conducting the study and the research assistants for supporting us during data collection.
List of abbreviations
Authors’ contributions
NKM and GA conceptualised and designed the study, conducted data analysis, and were responsible for the interpretation of data and writing of the manuscript. NKM, GA, JK, QKA, and ROB implemented and conducted the study. NKM wrote the first draft of the article. NKM, GA, JK, QKA, ROB, HTA, and STC participated in data interpretation and manuscript writing. NKM, GA, HTA, and STC reviewed the final draft and provided substantial input. All authors read the article and substantially contributed to this paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical consideration
Ethical approval to conduct this study was sought and obtained from the Cape Coast Teaching Hospital Ethical Review Committee with approval number (CCTHERC/EC/2022/115). Administrative permission was also obtained from the heads of the health facilities. Written informed consent was obtained from all participants. All aspects of the study including the rationale, objectives and participants’ responsibilities in the study were all explained to them prior to their participation. Also, participants’ rights were observed and they were told they could discontinue the interview any time without any consequences. To ensure confidentiality of information, personal designation and other related information which could be used to identify participants were not collected. Study participants were identified by codes assigned to them during the interviews.
Funding
The authors received no financial support for the research, authorship and/or publication of this article: This study was personally funded by the authors.
Guarantor
GA.