
Abstract
Objective
As worldwide population aging is accelerating, innovative technologies are being developed to support independent living among community-dwelling older adults with mild cognitive decline. However, the successful implementation of these interventions is often challenging. Until now, literature on implementation issues related to the specific context of older adults with mild cognitive decline is lacking and the few studies available do not focus specifically on the perspective of professional caregivers. Yet the perspective of these caregivers is important as they can be considered a key facilitator for technology implementation among this population. Therefore, this study was the first to examine technology implementation among community-dwelling older adults with mild cognitive decline from the broader perspective of professional caregivers.
Methods
In this qualitative study, two focus groups consisting of a heterogeneous pool of professional caregivers were conducted: one in Quebec (Canada, n = 6) and one in Brussels (Belgium, n = 8). Braun and Clarke’ method for thematic analysis, guided by a qualitative descriptive approach was applied to inductively identify themes from the data.
Results
We identified factors influencing technology implementation in older adults with mild cognitive decline on three levels: an individual level (e.g., characteristics of older adults with mild cognitive decline and professional caregivers’ attitude), an organizational level (e.g., lack of training among professional caregivers) and a level referring to the broader context (e.g., ethical considerations).
Conclusions
This study contributes to the research gap in knowledge on the needs of professional caregivers to facilitate technology implementation among the population of older adults with cognitive decline. Future directions for research, practice, and policy are given, more specifically to improve knowledge among caregivers and on the development of decision support to retrieve safe and effective technologies that suit patient-centered care.
Keywords
Introduction
As worldwide population ageing is accelerating, 1 increases in the prevalence of neurocognitive disorders such as mild cognitive impairment (or mild neurocognitive disorder) and dementia (or major neurocognitive disorder), from here on referred to as ‘mild cognitive decline’, are arising.2–4 In addition to memory and cognitive disorders, older adults with cognitive decline often face limitations in activities of daily living (ADL), 5 safety issues, and neuropsychiatric symptoms such as depression and irritability. 6 Hence, this increases the burden on informal caregivers involved in the care of these older adults. 7
This demographic transition is associated with high strain on residential healthcare, mainly related to residential staff shortages and high work-load 8 and high cost of admission. 9 Moreover, most older adults wish to age at home and in the community. 10 Therefore, it is important to develop innovative strategies to support these community-dwelling older adults with mild cognitive decline to support functional autonomy and independent living in the community. 11
According to the World Health Organization (WHO), 12 the development and deployment of age-inclusive innovations and interventions, including new technologies, make up an important strategy to improve the lives of older adults with mild cognitive decline and their informal caregivers and to decrease the impact of cognitive decline on communities. These technologies can be applied to relevant care processes, such as diagnosis and disease monitoring among older adults with cognitive decline, but can also improve the lives of these older adults by implementing these technologies in their daily lives. 12 The latter involves the deployment of technologies to support memory and ADL, amongst others, and to ultimately improve cognitive and social functioning and overall quality of life amongst this older adult group. 13 These technologies consist of a broad range of promising applications, such as computer and mobile applications to support memory functioning and training, web-based platforms for support and education of informal caregivers, assistive technologies and wearables for ADL assistance, virtual reality and exergames for cognitive training, monitoring technologies for ADL and location tracking, etc.14–17
Acceptance and uptake of technology among the older adult population is often challenging and unsuccessful.18,19 Findings of a previous study by our research team 20 involving older adults with mild cognitive decline and informal caregivers revealed that these challenges consist mainly of end-users factors. These involve a lack of knowledge or skills, personal relevancy to the older adults’ individual needs, attitudes, and interests, etc. In addition, other research has shown that factors related to the wider organizational context, including care practices and policies, are also important for technology implementation in this specific population group and among older adults in general.18,19,21 Examples of these include financial and time constraints within organizations, often reflected by a lack of professional caregivers or training, as well as issues concerning privacy of data sharing, reflected by concerns of older adults over who gets access to their personal or health-related data.18,21
To understand why and how these factors play a role in the integration and successful implementation of technology among older adults with mild cognitive decline, the application of qualitative research methods can be a valuable approach. Previous qualitative research on technology acceptance in the older adult population, in general, has already been performed.19,20,22,23 However, few have included the perspective of professional caregivers on this topic and within this specific older adult population22,23 and, to the best of our knowledge, no study ever focused exclusively on the perspectives of professional caregivers in relation to this research topic and population. Nevertheless, their perspectives are of great value, as they serve an important role as potential facilitator of technology implementation, introducing technologies to the older adults with mild cognitive decline as part of the delivered clinical care. Therefore, it is worthwhile and important to explore the perspective of professional caregivers on this topic.
This study is part of a larger bilateral (Belgian–Canadian) research project on technology acceptance among community-dwelling older adults with mild cognitive decline and the main research findings from the perspective of these older adults and informal caregivers were already extensively described elsewhere. 20 The present study's aim is to examine the implementation of technology among older adults with mild cognitive decline from the professional caregiver perspective.
Methods
Design
We performed a qualitative descriptive research study 24 comprising of two multidisciplinary focus groups: one in Quebec (Canada, n = 6) and one in Brussels (Belgium, n = 8), to reveal the perspectives of professional caregivers on technology implementation among the population of community-dwelling older adults with mild cognitive decline. These focus groups were held as part of a broader bilateral research collaboration on technology acceptance in older adults with mild cognitive decline. Description of the study methodology was based on the consolidated criteria for reporting qualitative studies (COREQ) checklist. 25
Participants and recruitment
Qualified professional caregivers experienced in the care for community-dwelling older adults with mild cognitive decline and professionals involved in care management services for these older adults were purposively sampled on type of health profession to obtain two multidisciplinary focus groups. To be eligible for participation, caregivers had to be (a) involved in the support and care of community-dwelling older adults with a formal diagnosis of cognitive decline such as in mild cognitive impairment or dementia and (b) be fluent in Dutch (in Brussels) or French (in Quebec). In Quebec, caregivers were recruited by email using a list of eligible staff provided by the manager of the Support for the Autonomy of the Elderly service, organized by the Integrated Health and Social Services University Centre of Capitale-Nationale (CIUSSS-CN). Most caregivers were both involved in outpatient care (day clinic) and home care for older adults with mild cognitive decline living in the territory of the Capitale-Nationale in Quebec (Canada), comprising urban as well as rural areas. In Brussels, caregivers were recruited face-to-face from the pool of staff members of the memory clinic of the Universitair Ziekenhuis Brussel (UZ Brussel), and their professional network contacts and contacts from the networks of researchers involved in this study (SD [PhD], EG [PhD], MF [PhD]) were approached by email. All caregivers were involved in either outpatient care (day clinic, primary care practice) or home care for older adults with mild cognitive decline living in urban and rural areas of Belgium. The focus group held in Quebec took place in the St-Sacrament Hospital in Quebec City and consisted of six participants (six women) between the ages of 30 and 60 years old, among which were: two occupational therapists, one physiotherapist, one social worker, one clinical nurse in geriatrics and one special education technician. In Brussels, the focus group took place at the UZ Brussel and consisted of eight caregivers (six women and two men, age range: 23–54 years), including one neurologist, one geriatrician, one general practitioner, two occupational therapists, one social worker, one home care service manager, and one home care nurse.
Although these countries differ on some aspects (e.g., federal organization of healthcare in Belgium vs. provincial organization of healthcare in Quebec; older citizens living predominantly in and around urban areas and often in close proximity to a hospital in Belgium vs. a higher number of older citizens living in rural and sparsely populated areas in Canada), these countries are still sufficiently similar (similar proportion of those aged 65 + years among the population; similar life expectancy, rate of physicians/nurses per citizen, etc.) to allow for combined discussion of focus group findings.11,26
Data collection
Main sociodemographic data, such as age, gender, profession, and institution were collected through a short written survey. Semi-structured topic guides consisting of open questions were developed based on discussion between all team members within each research institution. These topic guides included icebreaker questions to establish rapport, e.g., ‘What are your experiences with the use of technologies among older adults with cognitive decline?’ and several questions on implementation processes and opportunities, such as ‘What would facilitate or hinder the promotion of technology use among older adults with mild cognitive decline?’ and ‘What will be needed in the future to implement these technologies among a wider group of older adults with mild cognitive decline?’ Photo-elicitation was added to the topic guides as a technique to broaden the discussion on technologies when professional caregivers lacked knowledge or experience with technologies. 27 The photo-elicitation consisted of five vignettes depicting five categories of technological applications: communication (e.g., tele-conferencing with family or clinicians), medication management (e.g., traditional pill dispenser with reminder feature, mobile devices with reminder features, robot-assisted pill dispenser with reminder features), orientation/navigation (e.g., smart key chain with geo-tracking and retrieving feature, watch with geo-tracking features, mobile applications for navigational assistance), fall detection and assistance (e.g., watch and necklace with fall detection feature, wearable airbag belt, ambient monitoring system for fall detection and signaling) and leisure (e.g., mobile applications for media usage, mobile memory training applications, and exergames). The topic guide of the focus group in Brussels also comprised a combination of brain storms (i.e., by using scribble paper) and conceptual mapping (i.e., sorting the scribbles into categories ‘facilitators’ and ‘barriers’) as a technique to generate and facilitate the discussion (see Figure 1), but did not guide the data analysis. Before each focus group, the moderators introduced themselves and briefly summarized the research goal. The Brussels’ focus group was moderated by a gerontopsychologist (SD) and assisted by a postdoctoral researcher experienced in qualitative research (MF) who took notes and supported adequate time management. The Quebec focus group was moderated by an experienced research assistant (MAN [MSc]). During the focus groups, the interviewer intensively used facilitating communication techniques such as paraphrasing and summarizing to organize the data received and to if interpretation of the data was correct. The Brussels’ focus group lasted 1 h and 51 min and the Quebec focus group lasted 1 h.

Conceptual mapping result.
Ethics
Ethical approval of this study was obtained by the local Ethics Committees of both research institutions: the Vrije Universiteit Brussel and UZ Brussel (B.UN 143201835242) and CIUSSS-CN (# MP-13-2019-1522). At the start of both focus groups, participants were asked to read and sign an informed consent form to consent to participation and audio-recording of the data.
Data analysis
We applied an inductive thematic analysis to the data to inductively identify and select themes from the data. Throughout this process, we used the qualitative analysis software package NVivo 12. 28 The thematic analysis followed the steps described by Braun and Clarke 29 and was independently performed by two researchers: SD and IS [PhD]. As a gerontopsychologist, SD has experience with working with older adults, as with multidisciplinary caregivers, but has no experience with focus groups. IS has a background in computer sciences and criminology, has experience with mobile application development, and performed qualitative studies in the past, but has no experience with older adults. First, the auditory data were transcribed ad verbatim by two researchers (SD and MB) and actively read by the analyzing researchers (SD and IS) before being chunked into meaningful text segments (codes) and collated into coherent and distinctive themes. We applied a semantic approach to the coding and theme-generating process. The researchers discussed their results until consensus about the themes was reached. Thematic maps were drawn to gain insight into the data in the process of theme construction. The thematic analysis was validated by three additional researchers (MF, EG, MPG). Quotes were translated from French (Quebec data) and Dutch (Brussels data) to English for the manuscript.
Results
The major themes identified in the data comprised determinants for technology implementation among community-dwelling older adults with cognitive decline on three different levels: the individual level, the organizational level, and the broader contextual level. Figure 2 shows the thematic map that was drawn while constructing the themes.
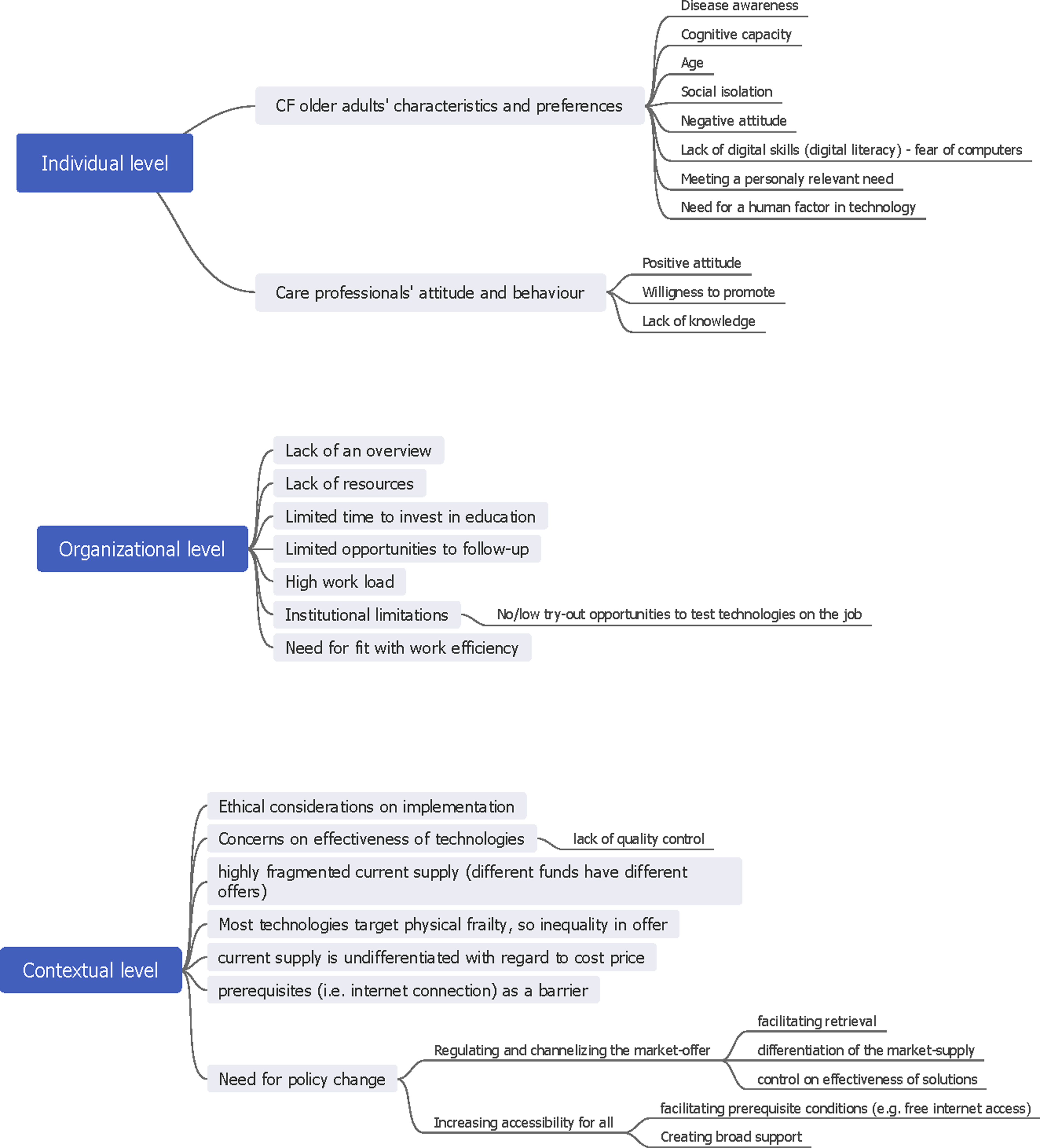
Thematic map.
Individual level
This theme comprises determinants of technology implementation that are associated with characteristics of older adults with mild cognitive decline and characteristics of professional caregivers.
Characteristics of older adults with mild cognitive decline
First, the characteristics of the older adults with mild cognitive decline included disease awareness, in the sense that caregivers believe the older adults are willing to adopt and hold on to technologies if they are aware of their cognitive decline and were at least worried by its implications for daily life functioning. Moreover, caregivers identified the level of cognitive functioning of the older adults as an important determinant for technology implementation. On the one hand, cognitive decline can introduce new or increased care needs in this population, for which technology can be adopted. On the other hand, according to caregivers, decreasing cognitive ability can also function as a barrier to the adoption and continued use of technologies, for instance when it is too hard to learn them or when forgetting to use them or how to use them. Therefore, caregivers believe in the importance of a fit between the ease of use and user-friendliness of a technological solution on the one hand and the older adults’ capacities on the other hand. Hence, technological appliances that are highly customizable and that flexibly adapt to the need and cognitive capacity level of the older adult are therefore more likely to be adopted and continuously used, according to professional caregivers.
Other individual characteristics were also believed to influence the uptake and use of new technologies by older adults with mild cognitive decline, according to caregivers. Negative attitude, social isolation, belonging to the oldest generation and being low digitally literate were mentioned as barriers to the use of technologies. “They also need to know it exists. (…) I think most people know that personal alarm systems exist, but for instance for calendar clocks: not everyone knows that. (…) For the current generation of older adults, that is indeed a barrier. I think that the generation that is coming of age now is more familiar with that [technology] than the current 80-plus… (…)” (caregiver of the Brussels’ focus group)
Furthermore, older adults with mild cognitive decline who lack digital skills, or even ‘fear computers’ as one Canadian caregiver formulated it, are obstructed to use new technologies. In these cases, the tools might be an asset for the older adults, but they lack the skills to use them. Therefore, a lot of tools, including digital tools to book tele-consultations with medical professionals are believed to be accessible only to older adults who are already digitally literate to some extent.
Overall, caregivers believe that implementing new technologies for older adults with mild cognitive decline can only be successful if they meet a relevant present or future need. Technologies should therefore offer an added value or clear benefits for the older adults with mild cognitive decline. Professional caregivers mentioned several need domains that could benefit from technological solutions: memory support (e.g., with calendar clock for temporal orientation), support of medication management (e.g., with pill dispensers and digital reminders) and maintaining social contacts and the need for meaningful activities (e.g., playing games or looking at photos for leisure). Moreover, caregivers considered technology as creating opportunity for empowering older adults with mild cognitive decline. “I work together with a home care assistant who takes her smartphone with her when she goes grocery shopping for a person with dementia. This person with dementia found it so impractical that he had to make a list in advance and that he can't even chose between products. So what does she [the home care assistant] do? She calls him with FaceTime and asks him real-time what product he wants. And that's great. (…) She brings him the groceries of his choice, this way. (…) and so he can decide for himself.” (caregiver of the Brussels’ focus group)
The need for reassurance on personal safety and therapy adherence of the older adults with mild cognitive decline among caregivers was also described. In Quebec, e.g., a platform with movies, photos, and information on specific physiotherapeutic exercises can be prescribed by the therapist. The application allows the therapist to send exercises by mail, and serves as a visual aid during exercises at home. It benefits the patient by accurately visualizing how an exercise needs to be performed and minimizes the risk of injuries due to imprecise moves.
Older adults with mild cognitive decline also need to be able to connect with technological applications, and therefore prefer humanlike experiences when interacting with technology. Applications that use a robotic voice instead of a human-like voice, or robots that miss a certain cuddle factor are not in favor of being advised to these older adults, according to the caregivers.
Characteristics of professional caregivers
In addition to characteristics of older adults with mild cognitive decline, we identified determinants of technology implementation that were related to professional caregivers’ characteristics. First, caregivers agreed that technology can offer opportunities to older adults by increasing the capability to live longer independently at home. Moreover, they believe technology can support themselves in the process of caring for these older adults, by taking over routine tasks (e.g., in the case of evaluating medication adherence) and, thus, saving time for other care tasks. Thus, caregivers mainly reflected positive about the usefulness and relevancy of technology implementation among these older adults and, equally as important, were willing to participate in the facilitation of this implementation process by applying technology in clinical practice and recommending technologies to older adults with mild cognitive decline and informal caregivers. At the same time, however, caregivers felt a strong lack of knowledge on existing and available supportive technologies. Therefore, caregivers considered this to be an important barrier for them to actively taking up a role as promotor and advisor in this matter. “I think that the essence is that all healthcare professionals should have a basic knowledge on that [technological applications], because if not, technologies are not going to be used. For instance, if one is asking me a question, I’m going to have to say, “I can't help you,” and then the person's going to put it [the technological application] aside and it’ll be done.” (caregiver of the Brussels’ focus group)
Organizational level
Care professionals mentioned a few implementation challenges that were related to the organizational context in which care practices take place.
Lack of an overview of trusted technologies
In addition to knowledge of technologies, caregivers lack trustable sources to retrieve these technologies.
Caregivers reported lacking an overview of the proven effectiveness of the existing technological applications. This results in insecurities to advise technologies amongst caregivers, and in the purchase of potential malfunctioning or non-adapted (e.g., calendar clock operating in another language than the older adults’ native language), and therefore, relatively useless technologies by the older adults. This was considered an important limitation by the caregivers, as this might result in discontinuance of use or even adverse effects of use. Caregivers considered this argument to be an important barrier for them to take up an active role in the implementation of technology. “If I say to a patient: “order that calendar clock,” and then at the next consultation the daughter says: “yes, but I’ve been looking on Google and I bought another one”, which then doesn't contain the required functions. Or if the displaying of the day is very important, for example, that it [the calendar clock] says MONDAY [“Maandag” in Dutch] in a very large size, but that it is displayed as an abbreviation of the English word “Monday”, none of that is taken into account.” (caregiver of the Brussels’ focus group)
Lack of resources to increase knowledge on technologies
Another important aspect of the organizational context of technology implementation is the lack of resources among professional caregivers to learn about technologies that could support older adults with mild cognitive decline. Caregivers mentioned this is often the result of time restraints due to high work-load, preventing them from keeping up with the state-of-the-art in the technology market supply. Moreover, the follow-up of the use of implemented technologies (i.e., with home visits) is considered limited by time restraints, potentially leading to discontinuance of technologies among the older adults.
As a result of the former two problems, in the context of professional care, the introduction to and implementation of technologies by older adults with mild cognitive decline merely depends on the knowledge scope of the caregiver they are confronted with and the training opportunities the caregiver has had. In practice, caregivers mostly execute broad internet searches for relevant technologies on own initiative and in their spare time (e.g., lunch breaks or after working hours). Often, technologies that were implemented on initiative of the older adult or an informal caregiver were added to the knowledge base of the professional caregiver. “We inform ourselves. We ask them [the older adults or informal caregivers] where they found this solution and how much they paid for it.” (caregiver of the Quebec focus group)
However, this ‘reverse’ technology introduction process often also leads to issues, as older adults with mild cognitive decline turn to caregivers for information and support on technological applications when caregivers feel insufficiently skilled to provide these or when the application itself does not work properly.
“This leads to issues at times. Families often come up with things they bought on the internet. Afterwards they try to get it to work and need to get it operational. A month ago, I had someone whose tool didn't work. Then they come to us and ask to fix it and help them. However, when things don't work, we can't help them either.” (caregiver of the Quebec focus group)
Sometimes, caregivers disseminate knowledge on potential valuable technologies among each other. In Belgium, this knowledge sharing could take place at a multidisciplinary care meeting organized to streamline and coordinate the multidisciplinary care of an individual older adult with mild cognitive decline. Although these meetings provide great potential for caregivers to learn from each other and broaden each other's knowledge on valuable technologies to support these older adults, in practice, they are only very rarely organized and little attended due to time limitations and low financial incentives. Efforts to digitize these meetings have been unsuccessful in the past, as the outdated technological infrastructure of some caregivers does not allow for it. Hence, in practice, most of the knowledge on technology is informally exchanged between caregivers. Nevertheless, this exchange practice is also believed to contribute to quality of care. “It is important that that interdisciplinary exchange will always exist. There will always be people like you [pointing at an occupational therapist], for example, you have a lot of experience and a lot of knowledge about what exists, while as a general practitioner, I see a very diverse range of pathologies. I am less specifically specialized in that part [on technologies] or know less about it. This exchange will remain important in order to achieve well-developed, personalized care.” (caregiver of the Brussels’ focus group)
Institutional limitations
More explicit institutional limitations were also identified to hinder the process of knowledge acquisition of technological applications to support older adults with mild cognitive decline. First, training opportunities to gain experience and test technology on the job were almost completely lacking. In Quebec, a remarkable discrepancy in this regard was observed: more resources were made available by the organization for training on intra muros technological applications (i.e., smart hospital beds), as opposed to extra muros applications (i.e., those targeted to be used in the older adults’ living environment) for which no time or financial resources for training and trying out were provided. “Testing is really necessary to be able to assess an eHealth solution and to make sure it is effective and helpful or not, before starting to recommend it to patients. But we don't really have access to these tools.” (caregiver of the Quebec focus group)
Furthermore, limiting organizational regulations were also specifically described in Quebec, hindering the introduction of technologies (i.e., small pill dispensers) that were not approved by the organization. “In the sense that the pharmacy doesn't allow us to introduce no matter what, since this is all [technology that can be advised] managed by the hospital.” (caregiver of the Quebec focus group)
Need for efficiency supporting technologies
Lastly, caregivers reported the reliability of technological applications as important. This reflected on the belief that, in addition to facilitating positive care outcomes, applications should also facilitate efficiency of care processes, and never hinder them. This was illustrated with an anecdote of smart hospital beds that were too sensitive and consequently generated an overload of false positive alarms of getting out of bed, thus hindering the efficiency of delivered care.
Contextual level
In addition to the individual and organizational level, we identified determinants of technology implementation that are related to the broader environment in which the care takes place.
Ethical considerations for technology implementation
First, our data show that caregivers highly value ethical principles regarding implementation of technology among older adults with mild cognitive decline. According to caregivers, technology implementation should always meet certain relevant needs of older adults and serve a purpose. Moreover, it should never be forced upon them but needs to be experienced as a voluntary choice or enforced by consent. This was especially relevant for privacy invasive technologies, such as location tracking and video surveillance technologies, as one occupational therapist reported to frequently object the thoughtless implementation of video surveillance technology by informal caregivers in the home of these older adults without their knowing about it. Caregivers believe that implementation of those technologies, especially without consent of the older adults, could result in adverse effects on overall well-being of the older adult, for instance when an intercom technology placed in the home scared the older adult and led to increased anxiety and caused hallucinations. A similar example was given by a Quebec caregiver, reporting on older adults with mild cognitive decline who felt spied on. Involving and empowering the older adult in the process of privacy-invasive technologies was described as very important: “With those GPS trackers, only when you push the emergency button you can see a location. It is very important for these people that you have that option. (…) And I really take that into account myself: I only recommend GPS systems where this choice is given. That you can ask the patient: “Look either we set it up so that your family can track you at all times or we set it up so that they can only track you from the moment you push that button; or if you have fallen, someone in the environment pushes that button.” Then they often say “I like it, but I wouldn't want my son to see me going everywhere all the time.” (caregiver of the Brussels’ focus group)
Furthermore, the implementation of technological applications is considered solely an additional supporting strategy that must never replace real human contact, as older adults with cognitive decline need closeness and connectedness of caregivers.
Need for policy action
Caregivers formulated issues concerning the market offer of technologies for older adults with mild cognitive decline and the opportunities for policy making. A first concern involves the effectiveness of technologies and the associated lack of quality control of these technologies. Moreover, caregivers felt that the current market-supply (i.e., regulated by the insurance funds) was too fragmented (i.e., different insurance funds have different offers) and mostly consisting of technologies to support physical decline rather than cognitive decline. For this, caregivers proposed regulating and channelizing the market offer, thus allowing caregivers to retrieve applications that are proven effective at one designated place. According to the caregivers, an ‘effectiveness’ label could be obtained through consensus of a special commission evaluating these applications, as is already existing for evaluating pharmaceutical drugs. This commission could eventually evaluate (a) the purposefulness and relevancy of a certain technological application, (b) aspects related to its development, and (c) its safety. Caregivers also identified the current supply as being too undifferentiated regarding cost, resulting in a lot of the supportive technologies being too expensive for a lot of older adults. They proposed future policy plans to include a range of alternatives of different purchasing prices, so that there would be basic and more advanced variants of technological applications, suitable to every older adults’ budget. “I think there should be an initiative coming from the government to bundle things [technologies] and also to recommend retrieval sources and companies and found some kind of consumer organization or something you can turn to and where you know: “That is reliable”. Because of course, we deal with the free market: Everyone offers something and 9 times out of 10 it's just worthless, it's just about money.” (caregiver of the Brussels’ focus group)
Third, in addition to the governmental action proposed to organize the market offer of technologies, a few measures are proposed to facilitate access to technology by older adults with mild cognitive decline. One of them consist of facilitating prerequisite conditions. This was illustrated by a caregiver proposing full governmental funding of home access to internet. Also, creating broad support is considered a very important step forward. This refers to increasing engagement among caregivers to take up an active role in the recommendation of technologies to older adults with cognitive decline. Therefore, more resources should be made available for training and education of caregivers. To increase awareness it is believed that enforcing the initial education of caregivers (i.e., basic medical or nursing training) with knowledge on technological applications to support older adults with cognitive decline. Additionally, the use of technological applications should be increasingly integrated in clinical internships and, also, continuing educational activities on this topic, such as conferences, providing exchange and learning opportunities, should be accessible to all caregivers.
Discussion
In this study, we identified factors influencing the implementation of technologies among community-dwelling older adults with cognitive decline in Brussels and Quebec, through the perspective of professional caregivers.
Multilevel identification of challenges and opportunities
We were able to identify implementation factors interacting on three different levels: individual, organizational, and broader contextual factors. The individual-level consisting of characteristics of older adults with mild cognitive decline is similar to those identified in former research.20,22,23 However, our in-depth findings related to the organizational and policy context can be considered important additions to the limited body of evidence in this field.22,23
The identified levels are similar to those occurring in the WHO's Innovative Care for Chronic Conditions framework (ICCC) 30 consisting of a micro, meso, and macro level, and to those occurring in the social-ecological model 31 consisting of an intra- and interpersonal level, an organizational level, a community level and a policy level. This illustrates that care and the organization of care are invested with different stakeholders, perspectives, and contexts. Therefore, implementation of technology in care for older adults with cognitive decline needs also to be approached in a multilevel way. Hence, interventions to optimize technology implementation among this population should always be developed for and deployed on these different levels. Thereby, interventions at the intra- and interpersonal level should overall focus on changes of attitude, behavior and competences, and those at the middle and highest levels should focus on creating opportunities for the latter by providing experience, education, and tools (organizational level) and developing overall values, principles and strategies of care, including decisions concerning resource allocation (broader policy contextual level). 32 Hence, interventions aimed at improving technology implementation in this specific population and care context often need to have multilevel targets.
Strategies to increase technology knowledge
One of our findings was that caregivers recognize the potential of technologies to support community-dwelling older adults with mild cognitive decline, but, however, lack knowledge of existing and available technologies. Caregivers described the lack of trustable resources that provide an overview of available, safe, and effective technologies, hindering their confidence to recommend technologies. This is a missed opportunity, as innovative strategies like technologies can improve patients’ managing their own health to a certain degree, making necessary lifestyle changes, developing new skills, and gain autonomy via self-management and -monitoring.32,33 The enrichment of caregiver knowledge on technologies could contribute to better patient-centered care and empowerment. These findings are aligned with those of Verloo et al. 23 who also observed a lack of technology knowledge and need for education on this matter among professional caregivers of older adults with mild cognitive decline.
Opportunities for this specific problem could stem from interventions targeted at all levels. First, in addition to informal exchange between caregivers, formal training and education of caregivers targeted at increasing knowledge of technology and its implementation strategies was identified as a need. As argued by Pruitt et al. 30 insufficient education of caregivers causes problems at the lowest distinguishable levels since it negatively affects patient care and therefore patient outcomes, in this case: cognitive and social functioning and the ability to live independently. At the same time, it is also an issue on the meso level, since organizations must ensure the expertise and tools for caregivers. 30 As training opportunities were hindered by low financial investment in staff training and time restrictions related to high workload, these are the exact leverage points for organizational change. Therefore, organizations should be encouraged to rethink their care practice priorities and enhance formal educational opportunities on this topic for their staff. Future research could also provide further insight in how caregivers would like the described challenges to be handled. This would benefit the further development of potentially successful implementation trajectories.
Second, policy decisions on educational curricula have the power to hinder or facilitate the spreading of knowledge through initial education curricula or continued education programs. 30 Moreover, as reported by the caregivers, increasing knowledge and creating broad support for caregivers to become technology implementators, practice experiences (e.g., in clinical internships) or exchange opportunities between caregivers (e.g., conferences) should also be stimulated.
A third approach to this problem might consist of developing a decision support tool (DST) that supports caregivers and older adults with mild cognitive decline in informed and shared decision making with regard to technological applications. This tool would meet the need for support of retrieval of technologies, reported by the caregivers in this study and observed among older adults in general.34,35 Such a tool might provide an overview of technologies that are available, experienced as safe, and proven effective on a range of outcomes related to sustaining independent living among older adults with mild cognitive decline. The development of a DST would meet the reported need for regulation and channelization of the market, bringing all eligible technologies together and providing choices based on individual preferences and need of this specific patient population. Moreover, as desired, this could provide opportunities to balance the offer and to integrate technologies that offer cognitive support as well as more physical support. The idea to provide quality labels to effective technologies by means of an evaluation commission is interesting and the full deployment of this quality control strategy should be investigated in further research. As this DST would be able to dynamically provide technological applications, depending on the individual characteristics of older adults, this also holds opportunities for differentiation of the market supply regarding cost price. This was valued as important by caregivers who suggested that alternatives of an application of different cost prices should be available to maximize affordability.
Other implications
Additional factors hindering accessibility, and thus implementation of technologies among older adults with cognitive decline are lack of disease awareness among older adults with cognitive decline, reflected by unawareness of its impact on ADL, and hence in increased care needs. This was believed to directly and negatively influence the older adults’ attitude toward technology adoption. As professional caregivers are frequently involved with older adults with cognitive decline as part of their clinical care trajectory, they have a potential pivotal role to play in this. It is, therefore, important to develop strategies for caregivers to broaden awareness of cognitive and ADL decline in this specific population, and thus, to open the dialogue for adoption of innovative supportive technologies.
Another accessibility issue involves affordability. As argued, cost price was reported to be important for technology adoption amongst the older adult population. This validates findings resulting from older adults with mild cognitive decline and informal caregivers themselves reporting on a lack of high financial resources (limited retirement income), high prices and opportunities for reimbursement. 20 It also confirms former research by Verloo et al. 23 in which cost price was considered a potential barrier by professional caregivers. The caregivers in this study add to this finding with the suggestion to facilitate prerequisite conditions to technology use, for instance by providing internet free-of-charge for all older adults. As affordability seems thus an important implementation factor, it should be part of future policy strategies concerning the implementation of technologies as part of health care.
Also our data showed that caregivers value ethical principles concerning the process of technology implementation among older adults with mild cognitive decline. These entail the principle that technology adoption should always be a voluntary process, enforced by consent of the older adult. These findings confirm those of Verloo et al., 23 in which professional caregivers objected to the idea of technologies only serving the needs (e.g., for reassurance) of informal caregivers, and explicitly valued the voluntariness of technology adoption by older adults with mild cognitive decline. Moreover, caregivers in the current study reported that ignoring these principles in practice could lead to adverse effects of technology implementation on older adult psychological well-being and empowerment. It is, therefore, very important to take ethical considerations into account when implementing technology. Future research should examine strategies to improve engagement of older adults with mild cognitive decline in the technology adoption process and to improve shared decision-making. Also, privacy invasive technologies included in a DST should always meet these ethical considerations (i.e., provide choices regarding data and location sharing for the older end-users). Future research could focus on developing strategies to promote professional and informal caregivers to work together to ensure technology implementation is executed in an ethical way and not in undesirable outcomes (e.g., privacy violations). Lastly, according to our data, technology implementation should always serve and add to the regular care context, in which real human contact and caregiving are still assigned the central role. This finding was also obtained from the professional caregivers in the study by Verloo et al., 23 suggesting the importance of it for technology implementation in this specific care context.
Strengths and limitations
To the best of our knowledge, this is the first qualitative study to focus exclusively on the perspective of professional caregivers on technology implementation among community-dwelling older adults with mild cognitive decline, while deploying an inductive, data-driven approach to data-analysis. This exclusive focus on the professional caregiver perspective allowed for an in-depth understanding of the organizational and policy-related context in which this implementation process takes place, which adds to the limited body of evidence in this field.22,23 The identification of multiple levels of aspects of technology implementation opens a range of possibilities to address these findings in their multi-layered embedding. Furthermore, the use of a multiple-country sampling, comprising of combined data from two countries that differ on geographic distribution of older adults and on the organization of healthcare in general, but have similar technology uptake patterns across the older adult population.20,36 contributed to the richness of the description. Lastly, the current study findings allowed us to generate future directions for research, practice, and technology development. This study addressed relevant and important societal challenges, and added to the very limited body of evidence 23 in this research field.
A few limitations to the current study should be addressed. Despite the efforts to achieve common and similar procedures for recruitment and data collection, we were unable to conduct a cross-country comparative study. As formerly argued by Knodel, 37 this is often the result of tension between the need to adapt the research procedures to suit the particular circumstances of each cultural setting and the need to maximize comparability between these settings. While conducting only two focus groups might seem limited, we purposively sampled on health profession to obtain groups of heterogeneous information-rich cases.38,39 These key stakeholders have a broad perspective in the perspective in the practice field and can be considered as sources of meaningful information on technology implementation among the population of community-dwelling older adults with mild cognitive decline. This allowed for a deep case-oriented analysis 40 and a new and richly textured understanding 41 of the data resulting in conceptual depth of themes and subthemes. Conceptual depth is related to the concept of saturation in the sense that when conceptual depth is reached, themes and subthemes are sufficiently ‘rich’ and ‘thick’.42,43 The unequal gender balance in the Quebec focus group can be considered a biased sample. However, since women represent 70% of the workforce in the health sector, 44 the impact of this imbalance is estimated to be rather limited. Future research could avoid this by integrating gender stratification into the sampling method.
Conclusion
As technologies are promising to support community-dwelling older adults with mild cognitive decline to live independently, it is of utmost importance that access to these technologies is optimal. Professional caregivers are convinced of this potential and are willing to take up an active role in this by acting as an advisor and facilitator. However, they experience a significant lack of knowledge and training in this regard, as well as a lack of trustable resources for retrieval of technologies, resulting in feelings of inadequacy and insecurity, and ultimately hindering implementation. Policies are therefore encouraged to develop structural strategies to support caregivers to overcome these barriers. Investments in initial educational programs as well as continuing educational programs are important, as well as developing tools for decision support. Moreover, development of strategies to motivate older adults with cognitive decline, especially in those having low or no disease awareness, is important, as well as making efforts to improve accessibility and specifically, affordability. Moreover, ethical aspects of technology implementation, such as voluntariness and empowerment of these older adults, are important conditions to the implementation process.
Footnotes
Acknowledgements
The authors would like to thank the participants for sharing their knowledge and investing their time in this study. Moreover, we would like to thank Mylène Boucher for transcription of the Quebec data.
Conflict of interest
The authors have no conflicts of interest to declare.
Contributorship
RB, MPG and EG designed the collaborative bilateral (Belgian-Canadian) research project in which this study has taken place and were responsible for the design of this study. SD and MF designed the Belgian focus group topic guide. SD, EG and MF contributed to recruitment of professionals in Belgium. SD (assisted by MF) and MAN guided the focus groups. IS and SD analyzed the data and wrote the first draft of the manuscript. EG, MF, MPG, MS, AB and AG contributed significantly to the final version of the manuscript. All listed authors reviewed and approved the final version of the manuscript.
Ethical approval
This study was approved by the local Ethics Committees of both research institutions: the Vrije Universiteit Brussel and UZ Brussel (BUN 143201835242) and CIUSSS-CN (# MP-13-2019-1522).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds Wetenschappelijk Onderzoek (FWO) and the Fonds de Recherche du Québec (FRQ) bilateral agreement [grant number G0D8518N]
Guarantor
RB.