
Abstract
Objective
Eliminating HIV transmission worldwide could become a reality with the advent of HIV pre-exposure prophylaxis (PrEP) where people take HIV medication to prevent HIV acquisition. Incorporating digital health into PrEP provision could help services scale up and meet increasing demand. We aimed to explore the prospective acceptability of a novel online PrEP care pathway (the ePrEP clinic) among PrEP users and healthcare professionals. The ePrEP clinic is composed of online postal self-sampling for HIV and other sexually transmitted infections, an online consultation, and remote medication provision.
Methods
We conducted semi-structured interviews with 15 PrEP users recruited from a large sexual health service and online cohort, and focus groups with nine healthcare professionals from the same sexual health service (May to December 2021). We analysed data using framework analysis.
Results
Participants found the ePrEP clinic highly acceptable, anticipating that it would provide convenience, empower PrEP users, and increase capacity within sexual health services. The need for blood self-sampling was a considerable barrier for some. Participants anticipated that the ePrEP clinic would be appropriate for established PrEP users with adequate digital health literacy and no medically significant conditions requiring in-clinic monitoring. Participants highlighted the need for support, including access to in-clinic care, and the integration of the ePrEP clinic within existing services.
Conclusions
Our findings provide clear justification for the development of the ePrEP clinic as an addition to in-clinic PrEP care pathways and provide useful insights for those developing digital services for other conditions incorporating testing, consultations, and prescribing.
Introduction
HIV continues to be an important global health concern despite major improvements in HIV prevention with the advent of new prevention technologies. 1 Oral HIV pre-exposure prophylaxis (PrEP) is one such tool in which people take antiretroviral medication to prevent HIV acquisition. 2 PrEP reduces HIV transmissions by up to 86%.3–5 Elimination of HIV transmissions is now realistic, and PrEP will play a major role in achieving this goal. 1 While PrEP provision has steadily increased globally in recent years, coverage is far from universal and currently falls short of the numbers needed to achieve zero new transmissions. 6 The World Health Organization (WHO) has called for methods of providing PrEP efficiently at scale to everyone who could benefit and suggests that digital health could help increase coverage. 7
In 2017, Scotland became one of the first countries worldwide to introduce PrEP within a national programme, free at the point of care, through state-funded sexual health services, guided by eligibility criteria. 8 To date, uptake has almost exclusively been among gay, bisexual and other men who have sex with men (GBMSM). 9 While most new HIV transmissions in Scotland continue to be among GBMSM, the incidence of new HIV infections within this group has fallen since the introduction of PrEP, 10 demonstrating the real-world effectiveness of PrEP in reducing transmissions for those who access it and, to a lesser extent, the wider GBMSM population.
In many countries, national guidance recommends that care for people taking or seeking PrEP includes regular screening for HIV and other sexually transmitted infections (STIs), renal function monitoring, and opportunities to discuss any PrEP-related issues such as side effects.2,11 In many settings, PrEP users access care through face-to-face, clinic-based services. However, HIV and STI self-sampling is increasingly available, with the user collecting their own samples using specially designed kits and posting them to a laboratory for testing. 12 The potential for remote testing creates opportunities for self-managed, digital PrEP care pathways. This aligns with WHO recommendations for the demedicalisation and simplification of PrEP care through various delivery models, including digital health, with the aim of increasing uptake and effective use of PrEP. 7
In Scotland, sexual health services initially provided PrEP care through three-monthly in-clinic appointments that shifted to telephone assessments and brief clinic visits for sample collection during the COVID-19 pandemic. 13 In line with HIV transmission elimination goals, Scotland now needs to scale up PrEP provision by creating new and/or expanding existing care pathways. The Scottish government has recently committed to developing a national ‘Scottish ePrEP clinic’, based on a novel online PrEP care pathway. 14 The ePrEP clinic will consist of three stages (see Figure 1): (1) online postal self-sampling for HIV and STIs, (2) an online PrEP consultation (online medical questionnaire) that determines if any clinical input is required before further PrEP is provided (e.g. additional tests or further discussion), and (3) provision of the PrEP medication, if medically appropriate. In the future, the ePrEP clinic could implement automated prescribing, in which a PrEP prescription is automatically issued if the online postal self-sampling and online clinical consultation outcomes satisfy an algorithm's criteria for safe prescribing. However, we will only implement this once the ePrEP clinic is well established and after careful development and consideration.

The three stages of the ePrEP clinic.
Although individual elements of PrEP-related care have already been delivered digitally (e.g. ordering HIV and STI self-sample kits and accessing HIV results) and some PrEP services incorporate digital components, 15 there is a lack of evidence on comprehensive, fully digital PrEP services such as the proposed ePrEP clinic.
Given the novelty and ambition of the ePrEP clinic, we aimed to understand the prospective acceptability of the ePrEP clinic from the perspective of PrEP users and healthcare professionals (HCPs), including factors that may affect the appropriateness of ePrEP and how to support ePrEP clinic users to engage with the service effectively.
Methods
Design
We conducted semi-structured interviews with PrEP users and focus groups with HCPs involved in PrEP provision because we wanted to understand acceptability from both perspectives. We anticipated that a one-to-one setting would be best for the PrEP users to ensure they felt comfortable sharing their individual experiences, thoughts and feelings.16,17 We gave the PrEP users the choice between a telephone or Microsoft Teams interview. We used a focus group design for the HCPs to facilitate rich discussions between participants, capturing interactions revealing normative and contradictory views among participants. 18 We conducted the focus groups on Microsoft Teams.
Participants and recruitment
PrEP users
We recruited people who identified as GBMSM, aged 18 years or older, who had used PrEP in the past 24 months, who had a means of participating in a telephone/Microsoft Teams interview, and who spoke English proficiently enough to complete the interview in English. We focused on GBMSM because the vast majority of PrEP users in Scotland are GBMSM. 19 We aimed to recruit purposively based on age and ethnicity given the documented digital and health inequalities experienced by older adults and ethnically minoritised people.20,21 Our target sample size was approximately 12–15.
We recruited two groups of participants: (1) PrEP clinic attendees from a large urban sexual health service and (2) members of an online Scottish cohort of GBMSM established as part of the Social Media, Men who have sex with men, Sexual and Holistic Health-Pandemic Study (SMMASH-Pan). 22 We used this approach to increase the diversity of the sample and transferability of the findings.
For PrEP clinic attendees, a clinician (LH) introduced the study within PrEP appointments. If the attendee was interested in the study, LH sent them the participant information sheet via SMS and arranged a telephone call to discuss the study further. At that stage, if the PrEP clinic attendee wanted to participate, LH arranged a time for the interview and passed the participant's contact information securely on to the lead researcher (RK) who then confirmed the interview arrangements with the participant. For the online cohort, RK identified and emailed participants who had consented to receiving emails about further research. The email introduced the study and had the participant information sheet attached with a link to an online expression of interest form. Participants provided electronic consent within the expression of interest form for the data provided, which we used to assess eligibility and to facilitate the purposive sampling. RK then contacted people who completed the expression of interest form and scheduled interviews as appropriate.
Healthcare professionals
We recruited HCPs who delivered PrEP care within a large, urban sexual health clinic that provides PrEP care to half of all PrEP users in Scotland. We aimed to recruit purposively based on years of experience in PrEP care/sexual health and job role. Our target sample size was approximately 10. The clinical lead for PrEP emailed all staff involved in providing PrEP care, introducing the study and linking them to the participant information sheet and online expression of interest form. Participants provided electronic consent within the expression of interest form for the data provided, which we used to assess eligibility and to facilitate the purposive sampling. The lead researcher (RK) followed up each of the completed forms and allocated participants to focus groups based on their availability.
Researchers
This study formed part of RK's doctoral research (PhD). Participants were aware of this prior to providing consent. Participants were also aware that this study formed part of a larger programme of research developing the ePrEP clinic. RK had an MSc in Health Psychology, which included training in qualitative research. RK had no previous relationship with any of the participants. LH is a speciality registrar doctor in genitourinary medicine and had existing relationships with the healthcare professionals who participated in the focus groups as they worked at the same sexual health service. RK and LH were supervised closely by CE, JF, JG and JD throughout the study.
Data collection
PrEP users
We created a topic guide based on the structure of the ePrEP clinic and key considerations. We piloted the topic guide with a small number of lay GBMSM. The lead researcher (RK) interviewed participants between 19 May 2021 and 16 December 2021. For participants recruited online, we collected demographic and contact information via the online expression of interest form. For participants recruited through the sexual health service, RK collected demographic information at the beginning of the interview. The demographic questions addressed age, ethnicity, gender identity and sexual orientation.
Immediately prior to the interview, RK sought informed consent from the participant. Due to the government-imposed restrictions on social mixing resulting from the COVID-19 pandemic and our decision to conduct the interviews online, written consent was not feasible. Therefore, we opted for an auditable, verbal consent process wherein RK read each consent form statement to the participant, who verbally agreed in place of initialling and signing. This process was audio-recorded and stored separately from the interview and all other personal information. RK also completed a paper consent form on the participant's behalf. Although we did not have written consent penned by the participant, we had two methods of verifying informed consent was provided by each participant ahead of data collection. The interview then commenced and was audio-recorded. RK started by exploring the participants’ experiences of the existing PrEP care pathway before explaining how the ePrEP clinic would work using a diagram and followed a script so that each participant had the same understanding of the proposed ePrEP clinic. RK then invited the participant to share their views on the ePrEP clinic via open-ended questions based on the topic guide. After the interview was completed, RK thanked the participant and provided them with a document signposting them to sources of support including sexual and mental health services. Although we did not anticipate that the interviews would trigger any negative feelings, we wanted to ensure participants had clear routes to support. RK also offered participants a £30 shopping voucher as reimbursement for their time and contribution. The interviews lasted between 35 minutes and an hour and 15 minute. No one was present in any of the interviews besides the participant and researcher. We stored all the data collected in this study in line with the approved study protocol and General Data Protection Regulation (GDPR). 23
Healthcare professionals
We conducted the focus groups between 17 August 2021 and 26 November 2021. We collected demographic and contact information via the expression of interest form. The demographic questions covered job role, years working in healthcare, sexual health and PrEP care, respectively, gender identity, sexual orientation and ethnicity. Two researchers (RK and LH) facilitated each online focus group. After entering the Microsoft Teams call, RK took each participant into a ‘breakout room’ to complete the informed consent process individually. Consent was verbal and recorded in the same ways as in the PrEP user study. Once each participant had provided consent, the focus group began and followed a topic guide. We had piloted the topic guide with a small number of HCPs. First, the researchers asked the participants to discuss their experiences of providing PrEP care during the COVID-19 pandemic. The researchers then delivered a two to three minute presentation explaining the ePrEP clinic before exploring participants’ thoughts and feelings towards the ePrEP clinic. The focus groups each lasted for two hours. No one was present in any of the focus groups besides the participants and researchers. We stored the data collected in this study in line with the approved study protocol and GDPR. 23
Data analysis
We used the framework approach because it provides a clear and flexible method of organising and analysing qualitative data, allowing for deductive and inductive coding. 24 The lead researcher (RK) created a priori coding frameworks ahead of data collection (one for the PrEP users and one for the HCPs). RK based these frameworks on the stages of the proposed online PrEP pathway. The wider team reviewed these frameworks before coding commenced. An external company transcribed the interview and focus group audio files verbatim. RK checked the accuracy of all transcripts, removed any identifiable information and uploaded them to NVivo version 12 to facilitate coding. RK performed the initial coding, sections of which were reviewed by the wider study team. RK adapted the frameworks during the coding process to add iterative, data-driven codes. RK synthesised the coded data thematically to form the themes and subthemes presented in the results section. The wider team then reviewed these themes and subthemes. Initially, we considered the PrEP user and HCP data separately and then brought them together once we had decided on the final themes and subthemes. While the researchers guided the PrEP users and HCPs towards similar areas, the extent to which they explored different topics varied. When the views of the two groups conflicted, we considered both perspectives.
Results
Participant characteristics
PrEP users
Fifteen PrEP users participated in interviews (11 from the sexual health service and four from the online cohort). One PrEP user who expressed interest withdrew from the study. While we were not aiming for saturation, 25 we did reach the point at which we did not identify any entirely new concepts or opinions within the transcripts. We present the participant characteristics in Table 1. The median age (IQR) of the sample was 35 (24,42) years. Thirteen participants identified as cis-men, and two participants identified as trans. Most participants identified as gay, and all but one reported White ethnicity. This is fairly representative of PrEP users in Scotland and the wider Scottish population.9,26
Summary of PrEP users’ demographic information.

Healthcare professionals
Nine HCPs participated in three focus groups (three participants per group): six doctors and three advanced nurse practitioners (these were specialist sexual health nurses who delivered PrEP care). Three healthcare professionals who expressed interest withdrew from the study. We do not present the reasons for withdrawal to prevent potentially identifying individuals. Similarly, we have not specified job role further to avoid inadvertently identifying participants. We summarise participant demographics in Table 2. The median time participants reported working in healthcare, sexual health care and PrEP care was 10 years, 7 years and 3 years, respectively. All but one participant identified as female, all identified as cis-gender, most identified as heterosexual and all reported White ethnicity.
Summary of healthcare professionals’ demographic information.

Themes and subthemes
We identified six themes, which we summarise in Figure 2, and explore below in detail alongside illustrative quotes from participants.
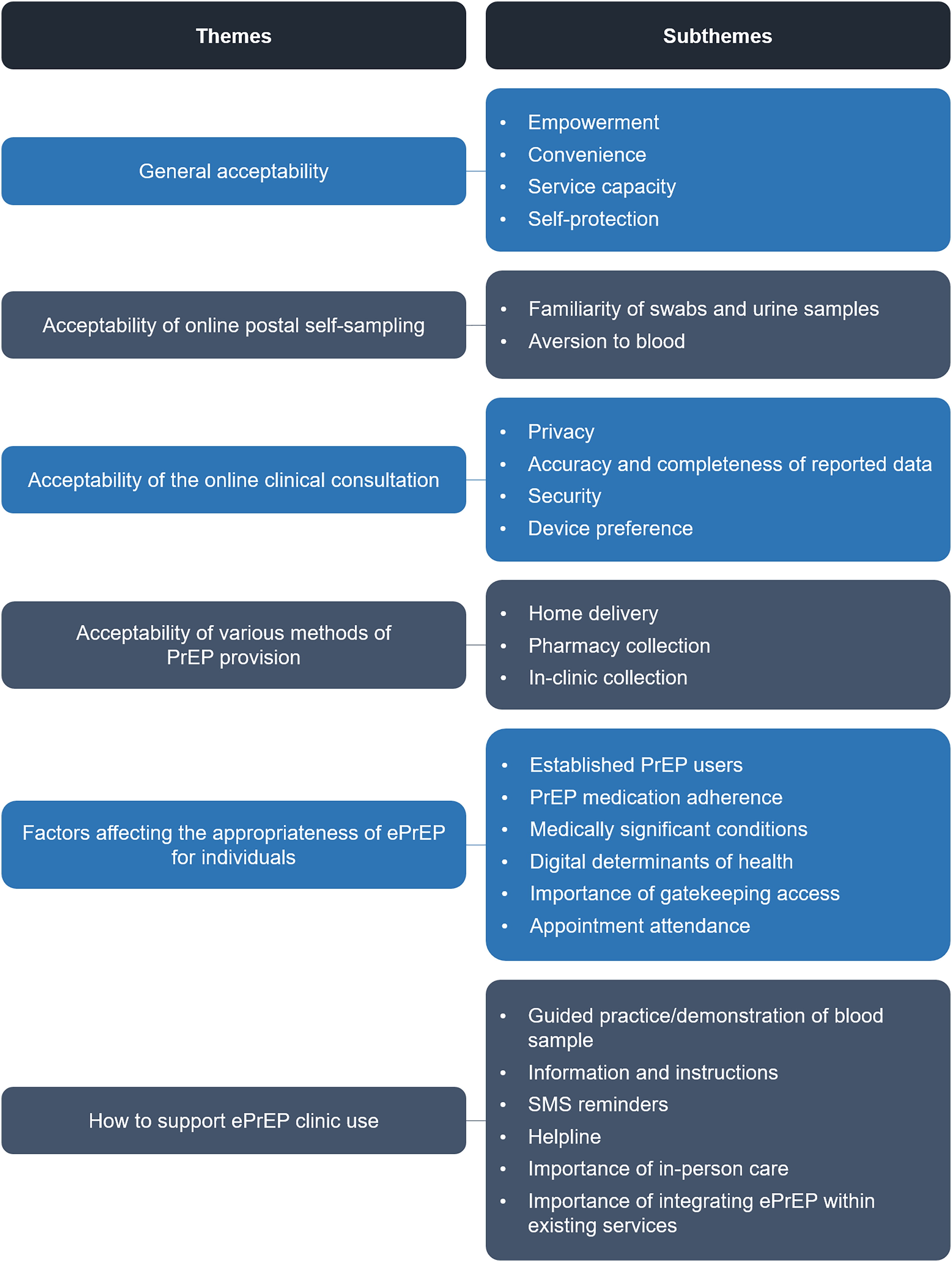
Themes and subthemes relating to ePrEP acceptability, appropriateness and necessary support.
General acceptability
Participants considered the acceptability of the ePrEP clinic as a whole and each of the three stages (Figure 1). In general, participants found the ePrEP clinic to be highly acceptable and reflected on some anticipated benefits detailed below: Like I said, it [ePrEP clinic] 100% should happen – it's a good option, and that's the key thing, it's the option, it's the choice and it's the ability for myself to have the autonomy over my healthcare to be able to pick and choose the channel that I would want to use when I would want to use it. PrEP user (aged 25–34) I think you’re giving the patients control, and giving them the opportunity to take things into their own hands. I think, sometimes, with the way that we’re doing things just now, we maybe ‘mollycoddle’ [treat in an overprotective way] our patients a wee [little] bit. Doctor I think it's good having it online; especially if you’re really busy. [If] you know your PrEP review is coming up and you’re literally struggling to get some time, then at least, you know ‘right, I can just go online.’ That takes away that added stress. PrEP user (aged 16–24) It means that there will be more appointments available. If people are only going once or twice a year [in person] rather than every three months, then it will be so much easier to get an appointment rather than having to wait two weeks to get in. PrEP user (aged 16–24)
One PrEP user linked this to the idea of ‘NHS [national, state funded health service] guilt’ – feeling guilty for using clinic resources, accessing what they considered ‘non-essential’ care, at a time when there are well-documented pressures on the NHS.27,28 They anticipated that the ePrEP clinic would help them overcome these feelings by reducing the amount of clinic time they were using.
I would expect that for [some people], they might not want to make it public [that they are taking PrEP], so they might feel a bit anxious about going into [the sexual health clinic], in case somebody might see them. […] I think it would be a lot easier for a lot of people to have it [their PrEP review] at home. PrEP user (aged 35–44)
Acceptability of online postal self-sampling
The acceptability of online postal self-sampling varied between participants. This was largely due to the need for self-collected blood samples as detailed below.
I’ve been getting tested a good few years now so I’m quite comfortable with doing the swabs [myself]. PrEP user (aged 35–44) I just hate the sight of blood. […] Sometimes in the clinic, I’m fine getting bloods taken and other times you’re walking out feeling woozy. That's my biggest hurdle. PrEP user (aged 35–44)
Acceptability of the online clinical consultation
PrEP users found the prospect of reporting medical and sexual information (i.e. the questions asked in the online clinical consultation) through an online questionnaire acceptable.
[The ePrEP clinic] would probably be easier because it is like talking to a blank screen, which is easier than talking to some stranger… the blank screen… it won’t judge you. PrEP user (aged 16–24) I think you might miss some things […] Sometimes, prompting some of the questions, and [asking] them in different ways, can get answers that you maybe wouldn’t get online. Advanced Nurse Practitioner
I can see maybe some people would potentially be worried about privacy online, but it doesn’t bother me… I enter information on other sites and I don’t think about it too much. PrEP user (aged 16–24) I think a phone is more convenient, you can do it on the go. I have it with me nearly all the time, so it's one of those things like: ‘oh, I need to [order] my [self-sampling] kit!’ So, I can just do it there and then. Being able to [access the ePrEP clinic] on a phone would be really important. PrEP user (aged 16–24)
Acceptability of various methods of PrEP provision
The researcher (RK) asked PrEP users how they would like to receive their PrEP medication within the proposed ePrEP pathway. They discussed three options: home delivery/posted to an address of choice, collection at a local community pharmacy and collection at the sexual health clinic. Participants suggested these options in the first few interviews. Accordingly, in subsequent interviews, the researcher gave participants time to suggest their own ideas and then offered these as potential options as prompts.
I was a wee [little] bit concerned, because I don’t really know my neighbours that well, that the PrEP was going to end up with my next-door neighbour, and I was going to have to go and try and retrieve it, or ask my neighbour for my parcel. I don't really want my neighbours knowing my personal activities and making assumptions. PrEP user (aged 35–44) Pharmacies could be good because you can select the pharmacy that is open at the times that suit you and that is close by. It's not like going to the clinic [which involves] driving. PrEP user (aged 25–34)
Factors affecting the appropriateness of ePrEP for individuals
PrEP users and HCPs identified many of the same factors that would make the ePrEP clinic more or less appropriate for individual PrEP users. However, HCPs focused on this area in more depth and identified additional factors relating to initiation, adherence and service engagement, while PrEP users focused on factors such as the individual's digital literacy and health.
I’d say, somebody that's been on PrEP at least, kind of a year, or something, so they’re kind of fairly well established and, I’m assuming, someone without other risk factors. Advanced Nurse Practitioner
Obviously, it's a new system, it's for people that probably don’t have underlying health conditions, obviously not taking [many other] medications, not seeing much change in their medication. PrEP user (aged 35–44) Obviously, there are some people who are simply not going to be able to engage with any level of technology. […] There is a presumption that you’re going to have an iPhone or equivalent, and that surely can't be the case for everyone. PrEP User (aged 55–64)
You would need to filter out the [PrEP users] that you think aren’t going to engage with it [the ePrEP clinic]. Anyone that's not really engaging that well with the current PrEP system is probably not going to engage with that system either. Advanced Nurse Practitioner
This contrasted with PrEP users who felt that the ePrEP clinic would overcome some of the barriers that may affect attendance such as difficulty scheduling appointments at a time where there was sufficient privacy.
I wonder if it could be something that a clinician would have to opt you in for. So, somebody would have to have their usual telephone appointment, […] making sure there aren’t any big risks, then being able to say ‘we feel that you’re somebody who would be able to self-manage your PrEP some of the time’ […] as opposed to, it's this big button on the website that anyone can click. Doctor
How to support ePrEP clinic use
Participants suggested a number of ways to support ePrEP users. This theme relates to specific support features as well as the importance of clear, integrated care pathways.
Maybe run through it [the self-collected blood sample procedure] and give [the PrEP user] a show of how you do it. […] I think it would actually completely make it [my anxiety about doing the procedure] go away because if you have seen it being done, then you’re just like ‘oh I know it is possible’. PrEP user (aged 16–24)
I think it would be important to have the [SMS] reminders, like before, and maybe give [a reminder] within like a week […] to make sure you’re going to complete it and you just don’t leave it. PrEP user (aged 25–34) Maybe just have a helpline number that they can call just to give them a bit more advice if they get a bit lost […] Sometimes I think it is helpful to talk to someone to try to explain what is going on rather than trying to fill out a box […] you get instant answers as well. PrEP user (aged 16–24) The option to come into the clinic, have [your PrEP review] done in the clinic because you wanted to have a chat with the doctor or nurse would also need to be there when you were notified that your three-monthly was coming up. You could say ‘could I please have a face-to-face in the clinic this time’? PrEP user (aged 65–74) I think it would be really, really difficult if you had to look at what they’d put online separately to their clinical notes […] I think that would be a bit of a nightmare, and there would be a lot of room for error or confusion about what was going on. Plus, some patients appear sort of in-between [the three-monthly PrEP appointments]. So, a lot of people, you’ll find, they got seen the week before by a separate clinician but they’ve still got a PrEP review but you don’t need to do any tests, because somebody did them the week before in the clinic. Doctor
Discussion
Main findings
Overall, PrEP users and HCPs viewed the ePrEP clinic as a welcome addition to existing care pathways and anticipated that it would directly address existing challenges such as difficulty scheduling appointments around other commitments and limited clinic capacity. PrEP users and HCPs both acknowledged that the ePrEP clinic would not be appropriate for, or preferred by, every PrEP user. Instead, it would be the right choice for some people some of the time. The need to maintain access to in-clinic care was clear, as was the ability for users to be able to choose between online and in-clinic care, as required. Both participant groups called for integration between ePrEP and in-clinic services to ensure HCPs have all the information necessary to provide appropriate care and to support PrEP users to make informed decisions, irrespective of whether users access services online or in clinic. PrEP users recommended various ways to support them when using the ePrEP clinic, such as SMS reminders to prompt them to schedule a PrEP review appointment. HCPs felt that the ePrEP clinic would be best suited to PrEP users who had already started PrEP following an in-clinic or telephone consultation, demonstrated good PrEP adherence, diligently attended their in-person appointments, have no medically significant comorbidities and have an adequate level of digital health literacy.
PrEP users and HCPs felt that the self-collect blood samples would be an important barrier. However, the right support could mitigate this issue to an extent. HCPs were concerned about the accuracy of the information users would provide in the online consultation, as this would inform prescribing decisions. However, PrEP users anticipated that the information they would provide in the online consultation might be more accurate, partly because they would feel less embarrassed inputting sexual and medical information into an online questionnaire compared to telling a HCP directly.
Findings applied to the wider context and literature
To our knowledge, this is the first study to explore the acceptability of a comprehensive online care pathway consisting of online postal self-sampling for HIV and STIs, an online clinical consultation and remote PrEP medication provision. Despite some concerns, HCPs welcomed the ePrEP clinic, which is encouraging given the importance of having HCPs (and health services) who are open to change for the successful implementation of new interventions/care pathways. 30 Our findings relating to the importance of choice and offering care through multiple modalities echo calls for differentiated care for HIV prevention. 7
PrEP users reported varying levels of blood aversion and perceived ability to obtain a valid blood sample. Difficulties in obtaining valid self-collected blood samples with finger-prick sampling is a well-recognised issue within online postal self-sampling, 12 demonstrated by relatively low return rates of valid blood samples. 31 This could limit the utility of the ePrEP clinic given that regular HIV testing is essential for safe PrEP provision. However, PrEP users provided valuable recommendations on how this barrier could be mitigated, such as by providing opportunities to practise blood self-sampling under the supervision of a HCP, which would likely be feasible as part of a PrEP initiation consultation. As recommended by participants in this study, other studies have incorporated short videos of self-sampling techniques and tips, which the ePrEP clinic could incorporate.32–34 Moreover, the WHO and British Association for Sexual Health and HIV recommend the inclusion of informational videos to support self-sampling.35,36 Newer, patient-centric self-sampling technologies may increase acceptability of blood self-sampling (e.g. Tasso).37,38 It is also possible that, because further PrEP prescriptions will be contingent on a negative HIV test result, users might be more motivated to complete and return their self-sampling kits than in other instances.
Evidence suggests that SMS reminders, which PrEP users anticipate would help them keep track of PrEP reviews, are acceptable and cost-effective in other settings.39–41 PrEP users also highlighted the importance of clear instructions for all stages of the online pathway, in line with other studies and national guidance regarding online postal self-sampling for HIV and STIs.33,35
PrEP users and HCPs agreed that the ePrEP clinic would require a relatively high level of digital and health literacy to use effectively and that this would be a barrier to some PrEP users engaging with the ePrEP clinic. Certainly, having the requisite skills and knowledge is essential for users to navigate online health services effectively. 42 While some participants assumed that older PrEP users would have lower digital health literacy, and therefore find the ePrEP clinic challenging, older PrEP users in this study did not share this view, which is consistent with evidence suggesting the digital health literacy of older and younger adults is comparable. 43 Importantly, PrEP users did suggest ways that we can support them to develop the skills necessary to complete the ePrEP clinic (i.e. instructions, helpline and demonstration), which could mitigate this barrier to an extent.
PrEP users and HCPs disagreed on using previous PrEP review attendance as a measure of ePrEP suitability. Importantly, PrEP users anticipated that the ePrEP clinic would help them overcome some of the barriers to in-clinic and telephone-based care, such as difficulty scheduling appointments around work commitments, which could lead to them having insufficient PrEP for their needs (‘running out of PrEP’). The flexibility of the ePrEP clinic could help improve adherence by ensuring that users maintain a sufficient supply of PrEP. This is important because some PrEP users have acquired HIV because of insufficient adherence. 44
There were also divergent views between PrEP users and HCP regarding the anticipated accuracy of the online consultation. Our findings are consistent with research on computer-assisted self-interviewing (CASI), wherein participants report their sexual behaviour via an electronic questionnaire, as is used in the National Survey of Sexual Attitudes and Lifestyles (Natsal). 45 Within the context of the third iteration of Natsal, non-response to sexual behaviour questions via CASI was low (<5% for each question). 46 In addition, within an evaluation of CASI in routine sexual health practice in Australia, around half of the service users preferred CASI, while around a fifth preferred a clinician to ask the questions. 47 Most service users stated that they had answered all of the questions accurately using CASI. 47 Moreover, most HCPs were satisfied with CASI, but some perceived in-person consultations to be more accurate when identifying some STI risk factors. 47
Implications for practice and future research
Our findings suggest that the ePrEP clinic will be an appealing addition to existing PrEP care options, alongside in-clinic provision. However, there is a clear need for integration with in-person care to allow for streamlined transitions between in-clinic and online care pathways and collation of user data so it is all readily available to HCPs. Support for users is essential, and we have provided recommendations on what this may involve. While there are opportunities to help users develop the necessary skills, there will likely be insurmountable barriers for some PrEP users (e.g. blood aversion). Therefore, we must continue to explore different ways of providing access to PrEP, sensitive to the needs of key populations.
Similarly, we decided to recruit GBMSM because we wanted to explore acceptability among existing PrEP users in the first instance, and PrEP uptake in Scotland was low among other key populations. It is important to note that we do not intend the ePrEP clinic to be solely for GBMSM, nor is the current pathway necessarily tailored to GBMSM exclusively; however, in the interest of creating the first iteration of the service that works for as wide a cohort of existing users as possible, we decided to take this approach. In the future, it is essential that we explore the acceptability of the ePrEP clinic among other key populations as part of wider efforts to expand PrEP access.
HCPs should not base decisions around ePrEP suitability solely on the diligence of PrEP users’ clinic attendance because, paradoxically, this could exclude the people most likely to gain from a more flexible, self-directed PrEP care pathway. Given that the ePrEP clinic could alleviate some of the barriers to attending in-clinic or completing telephone consultations, HCPs would need to have a detailed discussion with individual PrEP users to decide if online care is appropriate. Having sufficient digital health literacy will be an important factor when assessing the suitability of the ePrEP clinic for individual PrEP users; however, we need to consider how to assess this within the confines of a relatively short clinic appointment. In addition, the potential for the ePrEP clinic to overcome certain barriers to accessing PrEP could make PrEP more appealing to people who could benefit but find the current model inaccessible. However, healthcare professionals in this study felt that it was important to initiate PrEP through direct contact with a healthcare professional so that a holistic assessment of a potential PrEP user's needs can be made and wider health interventions offered, such as vaccination, before transitioning to online care. This has practical advantages as current UK national guidance recommends assessment of renal function prior to commencing PrEP, which is currently largely only available on venepuncture blood specimens. Further research is needed to understand what role the ePrEP clinic could play in widening PrEP access.
Considering similar technologies (e.g. CASI) and PrEP users’ views in this study, the online clinical consultation component of the ePrEP clinic could collect information that is more accurate in some cases, especially if the user feels embarrassed or lacks privacy when receiving a telephone consultation. Further research to assess how the information collected in the online clinical consultation compares to the information reported to HCPs is required.
Although explored in the context of oral PrEP, the ePrEP clinic could play a role in supporting the use of long-acting, injectable PrEP. 48 In particular, the ePrEP clinic could facilitate remote monitoring for sexually transmitted infections and assessing the need for any clinical input, especially in conjunction with de-centralised, community-based provision, self-administered injectable PrEP. Further research is required to understand the role the ePrEP clinic could play in long-acting PrEP provision.
If we consider other conditions that require long-term monitoring, the acceptability of the ePrEP clinic among PrEP users and HCPs suggests that similar pathways (i.e. remote self-sampling, online self-report assessment and subsequent provision of medication/clinical input as required) could be appealing in other settings and warrant further research.
Strengths and limitations
This study provides important insights into the acceptability of an ambitious, comprehensive online PrEP care pathway from the perspective of PrEP users and HCPs, laying important groundwork for the further development of the ePrEP clinic. The transferability of the findings is limited due to our relatively small sample sizes, we recruited most participants from a single site, we collected the data entirely online, and we focused exclusively on GBMSM. We were unsuccessful in recruiting purposively based on ethnicity (although our sample does reflect Scottish PrEP users in this respect); however, we did recruit across a range of ages (PrEP users) and years of professional experience (HCPs). Lastly, the focus of the study likely attracted participants who would have a favourable attitude towards digital healthcare and could underrepresent people with lower digital health literacy and/or a preference for in-person care.
Conclusions
The ePrEP clinic could play an important role in the Scottish government's HIV transmission elimination strategy 49 and aligns with WHO and Scottish strategies for self-managed and digital healthcare50–52 and WHO recommendations for more differentiated models of PrEP provision. 7 Our findings provide clear justification to develop the ePrEP clinic further and crucial insights to help optimise its development and implementation.
Footnotes
Acknowledgements
We want to thank the staff at Sandyford Sexual Health Service for their support with this study.
Contributorship
RK, CE, JG, JD and JF contributed to the design of the study. LH led the recruitment with the support from RK and CE. RK and LH collected the data. RK performed the initial coding and analysed the data with input from CE, JD, JG and JF. RK drafted the manuscript. CE, JG, JD, JF and LH reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Approval was granted by Glasgow Caledonian University (17.12.2020, HLS/NCH/20/004), the National Health Service (NHS) Review Ethics Committee (22.04.2021, 21/NS/0044) and NHS Greater Glasgow and Clyde Research and Innovation (26.05.2021, GN21PH134).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study formed part of RK's doctoral research, funded by Glasgow Caledonian University.
Guarantor
CE.