
Abstract
Self-care is the ability of individuals, families and communities to promote health, prevent disease, maintain health, and cope with illness and disability with or without the support of a healthcare provider. In the field of sexual and reproductive health options for self-care predominantly include ordering contraceptives online, or testing and treating genital infections outside a healthcare setting. The shift to digitally facilitated self-care consequently requires information that was previously used by clinicians to be made available to those managing their own sexual and reproductive health. This review was specifically interested in how to optimise this informational enabling environment as self-care becomes more complex. Using a realist approach to facilitate collation, analysis and synthesis of research from multiple disciplines this review sought to enable the generation of a programme theory to inform service development. The majority of research we identified studied information to support the choice to self-care and access to self-care. In contrast to established areas of self-care, for example, the management of diabetes or hypertension, studies of the self-care process in sexual and reproductive health are lacking. There is significant potential to expand digital information resources to support sexual and reproductive health self-care, however, there are currently significant unmet informational needs. This review proposes six key recommendations for providers and key stakeholders involved with sexual and reproductive healthcare for the improvement of digital self-care services.
Background
The World Health Organisation (WHO) describes self-care as the ability of individuals, families and communities to promote health, prevent disease, maintain health, and cope with illness and disability with or without the support of a healthcare provider. 1 Self-care has always been essential for health management, but the recent expansion of access to medical technologies at home has increased self-care options. 1 Self-care options are now often provided by digital services so that self-care and online services have become linked.2–4 Sexual and reproductive health (SRH) care has been an important area for innovation in the self-care field. Specific innovations in SRH self-care include contraception provision, 4 fertility regulation (e.g. pregnancy testing), 5 self-managed abortion, 6 sexual health testing,3,7 and the alleviation of menopause symptoms. 8 The shift to self-care within the SRH field has been attributed to the need for greater privacy and stigma reduction. 9 Self-care in SRH can be categorised as self-management (e.g. self-medication), or self-testing (e.g. self-sampling, self-screening) and self-awareness. 9
Digital services increase both access and convenience,3,4 but also transfer work from clinicians to service users, with users taking on new self-care roles. 2 The transfer of roles has been described as a new ‘burden of treatment’, 10 which necessitates additional health information to be provided, 11 for example, ordering a contraceptive pill online may involve choosing a type of pill or uploading a blood pressure reading. 12 The shift to digitally facilitated self-care consequently requires information that was previously used by clinicians to be made available to those managing their own SRH. The provision of this information in accessible formats is part of an ‘enabling environment’ required to support self-care. 1 Our review focused on studies of online clinical services that sought to facilitate self-care through: the provision of contraceptives, the testing of sexually transmitted infections, the provision of information regarding pregnancy and the provision of information regarding the menopause. We were specifically interested in how to optimise this informational enabling environment as self-care becomes more complex. We deliberately excluded studies on abortion because we are currently considering this literature in a separate review examining home medical abortion 1 (see footnotes: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=225307).
Online medical information is commonly used for self-management,13–15 with people obtaining information about chronic conditions through online health information searches, user forums or social media. 16 Our review acknowledges the pre-existing evidence base regarding online access to medical information, however, our specific aim was to explore the information which enables individuals to take on new self-care roles by using technologies made available through digital services. Information required in this context has specific characteristics; the amount of technical and clinical content is high and it aims to support specific practical tasks. Given these factors we anticipated specific challenges may arise in the provision of information to support SRH self-care. Figure 1 shows an example of the type of SRH self-care information that we believe is required for online sexual health testing.

Example of the information required for online sexual health testing.
In order to inform the development of information resources to support SRH self-care, we reviewed the literature to understand best practice in this field.
Review methodology
We used a realist approach to facilitate collation, analysis and synthesis of research from multiple disciplines that were relevant to our enquiry, and to enable the generation of a programme theory to inform service development. Realist methodologies facilitate an interpretive, theory-driven approach to data analysis from multiple literature sources. The realist approach seeks to provide causal explanations for how and why contexts can influence outcomes.17,18 Our specific realist objective was to understand how information supports SRH self-care for whom, under what circumstances and why, therefore enabling us to provide a number of key recommendations for improved practice. Our aim was to surface research that might help to understand the needs of different users of information to support self-care. The realist methodology facilitates an understanding of the needs of different populations, for example, the needs of women and girls, men and boys, children, LGBTI + people, older men and women or people living with disabilities. To provide accountability and avoid duplication we registered our review on Prospero (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=226814).
Methods
We followed established realist protocols to conduct our research.19,20 We undertook the following steps:
Step 1: location of existing theories
We began the research process with an initial programme theory that identified specific points within the SRH self-management pathway where information might be required (Figure 2). We built our programme theory based upon the informational needs of users accessing online services identified from our prior work surrounding digital SRH service provision.2,4,12,21,22 We built upon our initial observations and developed questions that were relevant to a broad range of self-care technologies in SRH care (see Figure 2).

Initial programme theory: improving access to information at each stage of a user's digital self-care journey may improve satisfaction and clinical outcomes.
Step 2: searching for evidence and document selection
We defined our search terms (see Appendix 1) and completed searches within Scopus, PubMed and Web of Science. Our searches focused on five subject areas to ensure the identification of relevant literature within the SRH self-care field. We searched the following broad topics: sexual health, sexually transmitted infections and diseases (STIs/STDs), contraception, menopause and pregnancy.
Step 3: data extraction
Our analysis sought to surface mechanisms through which people access and utilise clinical information to support self-care and to identify contexts that may alter these mechanisms leading to different outcomes. We expressed this analysis in the form of context-mechanism-outcome configurations (CMOc). Analysis was completed using Nvivo 12. Analysis focused on how an intervention is supposed to work, its success and its limitations with the aim of refining our initial programme theory.
Step 4: data synthesis and step 5: refining programme theory
As our CMOc configurations evolved we iteratively developed our programme theory in response. This enabled us to make recommendations on the provision of online information to support SRH self-care (Figure 3).

Overview of approach (in accordance with established protocols) (20, p.3).
Results
The initial search identified 11,986 potentially relevant results. Using automation tools available within each database, we removed papers published before the year 2000, those not written in English, those that were not within our subject area or from a relevant journal (i.e. agricultural or veterinary studies), and those which were incomplete leaving. 2,150 potentially relevant documents. These studies were amalgamated into a single Excel database for manageability and duplicate papers were removed. We screened these articles for relevance to our review question based on their titles and abstracts, and as a result a further 2,008 additional studies were excluded. Working together iteratively, we assessed 142 full text articles. During this process we determined the relevance, reliability and applicability of each paper as follows:
Relevance: Was the data within the document relevant for theory development? Reliability: Was the data sufficient and trustworthy enough to support particular claims regarding the research questions? Applicability: Could the data be interpreted within the realist formula?
In addition, because we identified few studies through our initial searches, we also hand searched journals that might contain information about SRH self-care (e.g. BMJ Sexual and Reproductive Health Care, Contraception, Current Opinion in Obstetrics and Gynaecology). This process identified eight additional documents that were not identified in our database searches. Throughout the research process references identified from within the literature were further examined and included for analysis where applicable. Overall, 25 articles fulfilled all of our criteria for inclusion (Figure 4).
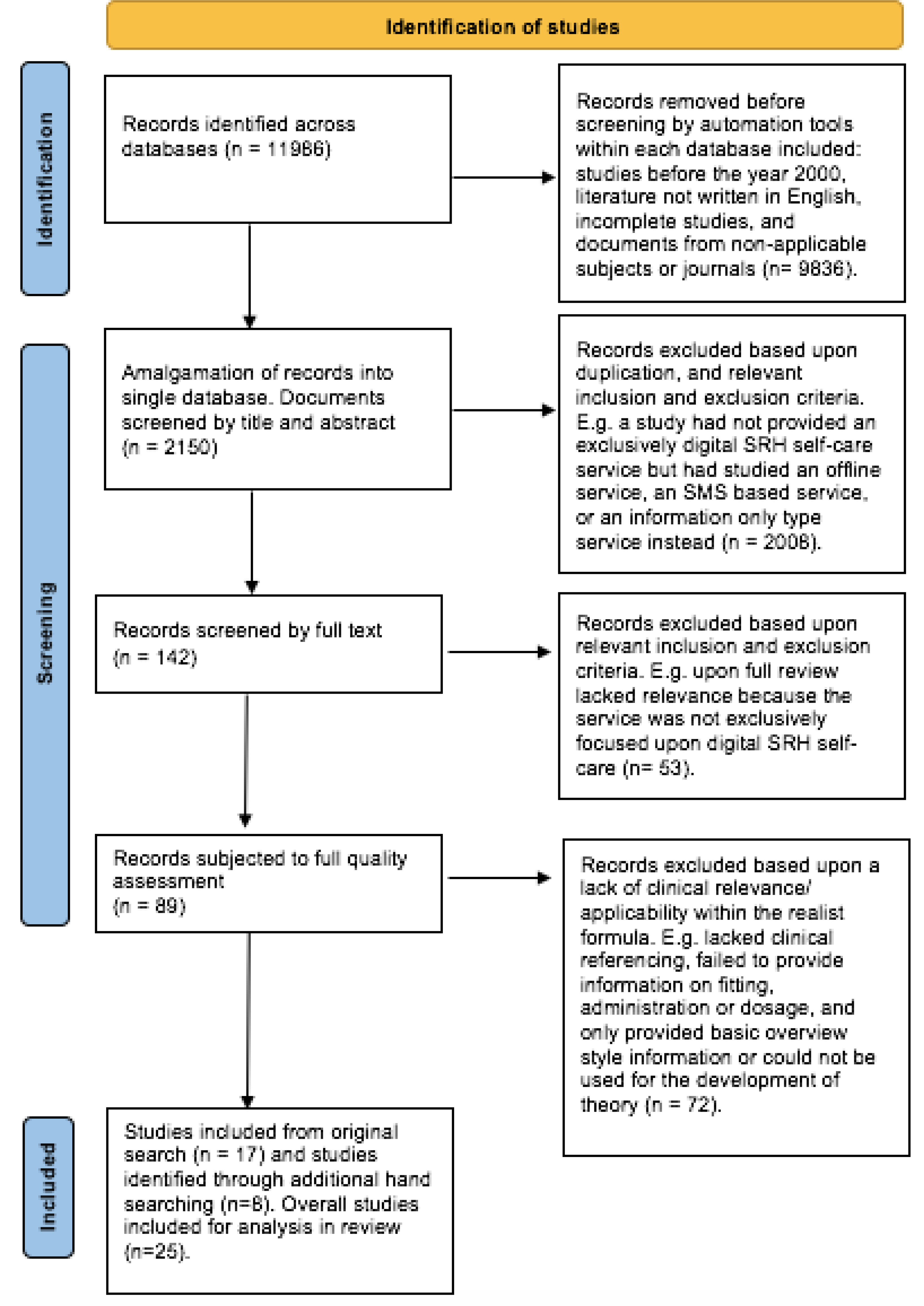
Prisma diagram of the search process.
Our analysis identified eight relevant CMOc configurations. Our CMOc configurations were linked to four main themes: information searching, finding services, presenting information and improving self-care practice. Table 1 summarises the CMOc configurations which together form the basis for the revised programme theory, with examples from the citations that provide the evidence for each element of the improved programme theory.
CMOc summary.

Overall CMOc based themes for improved practice
Theme 1: information searching
Theme one draws on CMO configurations 1,2,6,7. Young people who seek clinical self-management information online are presented with information filtered through search engine algorithms or organisational content management systems, but typically rely on top search results and struggle to assess whether sites are trustworthy. 23 Search engine optimisation by commercial organisations may be designed to promote transactional sites above public information sites, and mobile apps may contain inaccurate information. 23 Recommendations by clinicians are desired but clinicians lack confidence and training to safely recommend online information sites to enable a user's self-management. 37 Where access to self-care information is not facilitated by service providers, users are left to navigate overabundant content with very little support. 28 The separation of digital SRH information and trusted online/offline services is a missed opportunity to create an enabling environment for self-care.
Theme 2: finding services
Theme two draws on CMO configurations 3,5,2. Users value signposting to services that facilitate self-care (either online services or offline clinics). The information services referenced in CMO configuration 3 were highly valued by MSM, because they provided a combination of general information about PrEP and practical advice about accessing local testing, prevention and advice services.29–31 CMO configurations 5 and 2 highlight how young people value the linkage between online information and trusted health care organisations; particularly the opportunity for anonymous interaction with clinicians before visiting a service. 36 Those using clinic-based services want information on self-care provided anonymously by a health care professional that supplements their face-to-face care.29,36 Overall, the literature suggests that the relationship between online information and offline services is important in terms of maintaining credibility, ensuring trustworthiness and increasing audience access. Services which accommodate these trust-generating factors are highly valued and are supportive to a user's self-care journey.
Theme 3: presenting information
This theme draws on CMO 4. The literature suggests that young people generally find visual and auditory information engaging in comparison to text-based information, however, visual/ audible information may compromise confidentiality and cause embarrassment for some individuals.28,32–35 Young users are concerned about viewing or being seen to view information which may be perceived as sexually explicit by their peers or family.28,32 These concerns have a broad basis in personal, religious or cultural beliefs.28,32 A discreet option such as text-only information should be available within a digital service, to reduce the risk of embarrassment or shame, therefore enabling individuals from a range of cultural backgrounds/belief systems to access SRH self-care information.
Theme 4: improving self-care practice
This theme draws on CMO 8 and shows that interactive online contraceptive information may have similar clinical outcomes to clinician delivered contraceptive counselling in offline contexts. The long-term impact upon a user's knowledge from digitally delivered SRH education is similar to information delivered in person, suggesting that this approach has value in supporting self-care and SRH knowledge.43,45–48 It is therefore necessary that misconceptions regarding digital SRH service delivery are further researched, and the positive impacts of online education highlighted. The positive impact of digital health care should be recognised and utilised by health care services and clinicians to support a broader audience of users to improve their self-care journey.
Improved programme theory
From the CMO configurations within these themes we modified our programme theory as shown in Figure 5.

Improved programme theory.
Discussion and CMOc based recommendations
This review aimed to develop our initial programme theory ‘What information supports whom to effectively access and use self-care technologies in what circumstances and why?’ Our review found limited information to develop our theory.
The majority of research that we identified studied information to support the choice to self-care and access to self-care. In contrast to established areas of self-care, for example, the management of diabetes or hypertension, studies of the self-care process in SRH are lacking. Comprehensive information regarding conditions, sophisticated digital monitoring tools, personalised educational interventions and customised coaching are widely available for the management of diabetes and hypertension; 49 but are not available for SRH. Self-care in diabetes or hypertension is often clinician initiated, is considered an essential element of treatment, and training and support is usually provided. 50 In SRH, self-care is usually initiated by users and is less integrated into clinical care, for example, the decision to take a sexual health test or switch contraceptive method is often made by the user with little training provided.
Our review suggests that despite the recent expansion of digitally facilitated self-care technologies in SRH, interactive digital information to support self-care remains limited. Online interventions are becoming more routine and there is significant potential to expand digital information resources to support SRH self-care. There are currently unmet informational needs, for example, understanding the ‘window’ period for STI testing, choosing the most appropriate form of emergency contraception, interpreting test results, understanding treatment dosing and understanding timing for PrEP. Tools to support these self-care strategies are gradually becoming available, however, there has been little evaluation of usability or the measurement of sexual health outcomes. Our review suggests that SRH providers and key stakeholders within SRH have an important role to play in improving the experience of SRH self-care by providing more appropriate information. Based upon this realist review, we suggest the following key improvements should be undertaken to improve online clinical information for user self-care:
Sexual health services should provide or link to high quality, interactive sexual health self-care information that is endorsed by trusted services. Providers should recognise that interactive digital information appears to be as effective at supporting contraceptive decision making as clinician delivered information, and has an especially important role in the provision of digital contraceptive services. Sexual health services should support young people to find information online through search engine optimisation and clear signposting within organisational websites. Sexual health services should train clinicians on how to assess the value of external sites and encourage them to recommend those assessed as high quality. Information only sites should include an option to find local services which have the capacity to enable the user to anonymously speak with a clinician without the need for registration. Self-care information should be provided in a variety of media that includes a text only format to protect confidentiality and reassure those who are concerned about inadvertently finding sexually explicit material.
Limitations of review
This area of SRH information provision to support self-care is currently under researched. The research gaps include a lack of evidence on the information needs of those from older age groups, religious/ethnic minorities, LGBTQI + communities and individuals with disabilities. In addition, whilst the realist approach offers strategies to interpret the existing evidence to inform practice and policy, and our review used these established research protocols, the limited evidence available means that our conclusions are limited.
Footnotes
Acknowledgements
There are no acknowledgements required for this study.
Conflict of interest
The authors have no conflicts of interest to declare.
Contributorship
TC and PB contributed equally to this article.
Ethical approval
Ethical approval was not required for this review.
Funding
This research was self-funded.
Guarantor
Dr Tom Courtenay.