
Abstract
Objective
The aim of the current study was to explore the relationship between online and offline health information-seeking behaviors, as antecedents and consequences, and health anxiety and related belief factors in rural residents.
Methods
Based on the ABC theory of emotions (ABC model), this study developed two theoretical models of the association between health anxiety and health information-seeking behavior: Placing health information-seeking behavior (both online and offline) as an outcome and antecedent, respectively, and setting three belief factors of the perceived health threat, intolerance of uncertainty, and catastrophic misinterpretations. We collected 730 self-reported data points from 20 June to 5 July 2022 for rural residents in China and empirically tested the research model and hypotheses using partial least squares-based structural equation modeling.
Results
The perceived health threat and intolerance of uncertainty are significant motivators of health anxiety, and health anxiety has a direct beneficial effect on both online and offline health information-seeking behaviors. Health anxiety is influenced either directly or indirectly by catastrophic misinterpretations resulting from online health information-seeking, while offline health information-seeking behavior does not contribute as strongly to health anxiety directly but mainly reinforces it through the mediating influence of catastrophic misinterpretations.
Conclusions
Rural residents’ health anxiety promotes their online and offline health information behaviors. And both their online and offline health information-seeking behaviors may promote health anxiety directly and through catastrophic misinterpretations. Comparing the two, online health information-seeking behaviors primarily exacerbate health anxiety through direct effects, whereas offline health information-seeking behaviors primarily affect health anxiety through catastrophic misinterpretations. We provide suggested guidelines for alleviating health anxiety and regulating health information behaviors among rural residents.
Introduction
According to the 2022 China National Health Insight Report, anxiety regarding one's current health state is on the rise. Up to 70% of people are worried that they will die suddenly, and 91% of respondents were worried that they had a mental health problem, when in fact only 30% were actually diagnosed. 1 With the unexpected outbreak of coronavirus disease 2019 (COVID-19), it appears that health anxiety (HA), which refers to worry or fear about health issues, is progressively becoming a symptom that is spreading over the world. 2 HA not only causes distress in individuals and families but also ultimately puts a drain on societal resources by tying up healthcare resources and reducing medical service take-up. 3 Proactively seeking health information has the potential to alleviate this situation by empowering individuals to become health literate and to make prudent health decisions. However, incorrect health information seeking, such as excessive or ambiguous information searching, mistrusting or over-interpreting such information, can be counterproductive and increase anxiety. 4 Researchers from many different fields, like information science, medicine, and psychology, are interested in this complicated way that HA and health information-seeking behavior (HISB) work together.
One is to consider excessive online health information-seeking behavior (OHISB) as a prerequisite for exploring the development of cyberchondria, which is characterized as a recurrent or overly frequent search for health information meant to reduce HA but instead raises anxiety levels.5,6 Empirical evidence indicates that OHISB can induce cyberchondria. For example, emerging adults frequently seek answers to the origins and implications of their pain perceptions online, nevertheless, a catastrophic interpretation of the results may result in cyberchondria. 7 Also, in the context of COVID-19, excessive OHISB may result in information overload, which exacerbates HA and sets off cyberchondria. 8 However, these studies positioned HA and OHISB as excessive and pathological, which have been questioned for often exploring them in general samples rather than clinical disease samples. 9 In other words, the impact of general OHISB (as distinguished from excessive OHISB, referred to later as OHISB) on HA in non-clinical samples has been ignored.
The other mostly discussed is OHISB as a safety action outcome of HA. 10 That is, HA can stimulate health-related internet behaviors. Singh and Brown 11 confirmed that college students’ HA tends to cause them to be more frequent and spend more time on OHISB. HA was found to encourage online information seeking through neuroticism when Lagoe and Atkin looked at characteristics that might affect HISB among individuals in the United States. 12 A qualitative study found that undergraduate and postgraduate students’ reasons for conducting online searches were to obtain health information to reduce anxiety about an undiagnosed condition. 13 Evidently, studies have emphasized the general public that may employ internet technology effectively, such as college students 14 or adult internet users, 5 while disadvantaged groups with inadequate health literacy and information literacy are overlooked. 15 Rural residents in China, who are economically disadvantaged, under-resourced, and digitally illiterate, are among this vulnerable group. 16 Despite the fact that getting health information and services online is a growing trend, traditional offline HISB (FHISB), such as reading newspapers, watching television, or consulting relatives, friends, sick friends, or doctors, remain key health access channels for this group, even though the fact that internet-based availability to health information and services has become a prevalent trend; and FHISB is as important, if not more important, than OHISB; and HA is not a uniquely Internet-era innovation; the overemphasis on online health information activities has led to the neglect of the relationship between HA and HISB (both online and offline) among these vulnerable populations. 17
Overall, the relationship between OHISB and HA in a single direction was fully explored, i.e., OHISB as a dependent variable for HA and excessive OHISB as an antecedent variable of cyberchondria, respectively. An exploration of the relationship between HA and OHISB, FHISB, and the simultaneous introduction of HISB as a consequence and cause was neglected. To fill the gap, this study attempts to investigate the connection in both HA and HISB (including OHISB and FHISB) in an integral way among the rural population. Specifically, exploring how HA predicts OHISB and FHISB, how OHISB and FHISB predict HA in turn, and the associated belief factors of HA.
Research model and hypotheses
The ABC theory of emotion-based research models
Quite a few models related to HISB have positioned it differently as a dependent variable and as an outcome. Such models include the risk information seeking and processing (RISP) model, 18 which considers HISB as a behavioral consequence of perceived risks, and the information motivation behavioral skills model, 19 claims that health-related information and motivation lead to health behaviors. These models provide a solid foundation for understanding how HISB has been activated. However, the consequences resulting from HISB as a prerequisite have not been well considered. The ABC theory of emotion (ABC model) offers the possibility of using HISB as both a consequence and a precursor. The ABC model describes the cyclical process of how cognition, emotion, and behavior interact, 20 i.e., when people experience an activated event (A), how they relate it to their goals, resulting in explicit beliefs about the event (B), and the emotional and behavioral consequences (C) arising from that belief, which, once formed, may become activated events (A) that further alter belief (B), emotional or behavioral outcomes (C). 21 It has been used successfully in studies looking at the links between anxiety and cyberchondria, 22 as well as HA and HISB. 23
In the current study, we thus developed a process model for HISB as a consequence of and an antecedent of HA based on the ABC model, respectively. More specifically, physical suffering or concern for illness prevention are considered activating events (A1) that trigger related beliefs about perceived health threat (PHT, B1). And these beliefs then lead to an emotional consequence, i.e., HA (C1-emotion), which in turn triggers behavioral consequences, i.e., health information behavior (HISB, C1-behavior). That is, in this process, HISB is seen as a behavioral consequence, while PHT, HA, and intolerance of uncertainty (IU) are antecedents, on which Model 1 in Figure 1 is based.
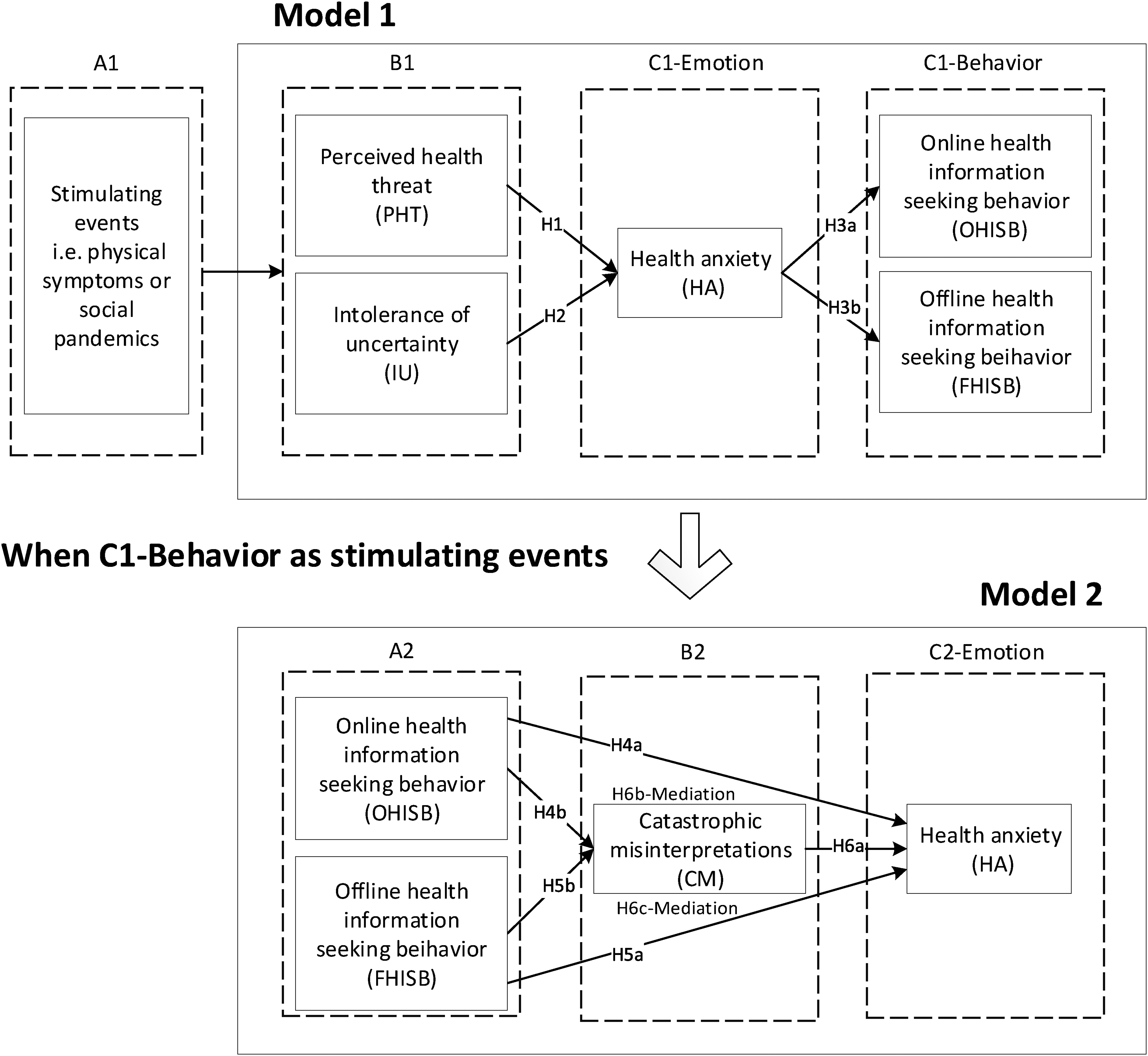
The research model.
HISB as an outcome in Model 1 may be a stimulus event (A2), leading to the user's belief in the event, i.e., catastrophic misinterpretation (CM) (B2), and thus to HA as an emotional consequence (C2-Emotion), a process in which HISB acts as an antecedent and which is illustrated in Model 2, Figure 1. The detailed hypotheses for every model will be described in the next section.
Hypotheses for model 1
Belief-related antecedents and HA. PHT refers to people's beliefs about health-related threats, specifically the perceived vulnerability to the threat and the perceived severity of the expected consequences of the threat.
24
Perceived severity is a subjective belief about the probability of suffering a health problem, and perceived severity characterizes opinions regarding the severity of the outcome of health problems.
25
As the RISP model points out, perceived risk triggers related emotional reactions like worry.
18
PHT has been regarded as a key factor in driving individuals’ HA. There is evidence that Chinese consumers’ anxiety levels are rising as a result of the feared COVID-19 pandemic danger.
26
Zhao and Cai
27
confirmed that smokers’ perception of the risk of developing lung disease was strongly correlated with their concern when seeking health information. Therefore, the proposed hypothesis is as follows:
H1: PHT has a positive impact on HA.
The IU is broadly defined as the tendency to fear the unknown.
28
IU is considered to be a biased cognitive belief that activates an individual's emotional responses to uncertain events, such as physical health problems.
29
Existing research has supported the idea that uncertainty about health issues motivates individuals’ HA.
30
People with lower IU brought about by somatic symptoms or health conditions tend to be HA.
31
Therefore, the proposed hypothesis is as follows:
H2: IU has a positive impact on HA.
HA and HISB. HA refers to a person's worry or fear about their health, which is a constant emotional state ranging from indifference to excessive anxiety about health.
32
Emotional states are often a strong motivator for health-related behaviors.
33
Prior research has confirmed that HA is the key motivating factor for OHISB.
34
But the effect of HA on FHISB, which is a way of accessing information based on offline sources rather than the internet, e.g., through consulting family, friends, patients, doctors, books, TVs, etc., is neglected. Despite the internet age, FHISB is equally important for rural residents who are deficient in health and information literacy. Therefore, our study implies that HA motivates both online and offline safety-seeking activities. On this basis, the hypotheses listed below are presented:
H3a: OHISB is positively impacted by HA. H3b: FHISB is positively impacted by HA.
Hypotheses for model 2
HISB and HA. The existing literature has yielded two claims about the effect of OHISB on HA in different contexts: One claims that access to health information may be beneficial in reducing HA through gaining knowledge about health-related issues; the other suggests that OHISB reinforces HA if the information accessed is overwhelming, negative, or confusing.
35
The current study focuses on rural people who are more likely to be hindered in their HISB; for example, they may not be able to retrieve or filter relevant information accurately, and they may not be aware of the channels and departments of health services. As a result, health information seekers in this group are more likely to suffer negative outcomes, thus deepening their HA. Thus, the hypotheses listed below are presented:
H4a: OHISB has a positive impact on HA. H5a: FHISB has a positive impact on HA.
The role of catastrophic misinterpretations. Though negative reinforcement of one's HA by OHISB is well documented,
36
little is mentioned about the mediation factor of this relationship.
37
CMs refers to individuals’ exaggerated beliefs about harmless somatic symptoms,
38
such as mistaking a regular headache for a brain tumor.
32
CM may become an HISB-induced cognitive belief,
39
i.e., when people access and understand relevant health information, they match incorrectly or excessively what the information describes to their own symptoms, resulting in catastrophic beliefs about current health conditions. Such dysfunctional beliefs have been shown to lead to further HA.
40
And it may be more noticeable among the disadvantage group like rural residents, who have limited health awareness and find it difficult to sift through the wealth of health information. Based on this, this study suggests that CM may be a potential mediator between HISB and HA. On this basis, suggested hypotheses include the following:
H4b: OHISB has a positive impact on CM. H5b: FHISB has a positive effect on CM. H6a: CM has a positive effect on HA. H6b: CM mediates the relationship between OHISB and HA. H6c: CM mediates the relationship between FHISB and HA.
Method
Measures
The constructs employed in this research were derived from well-established scales in the existing literature. Each item was measured using a seven-point Likert scale, ranging from “strongly disagree” to “strongly agree”, as detailed in Table 1. The measures of PHT were developed with five items based on Dodel and Mesch. 24 IU measurements with seven items were adapted from Baerg and Bruchmann. 14 HA measurements were adapted from Lucock and Morley 41 with seven items. OHISB measurements with three items were modified from Griffin et al., 42 as were FHISB measurements based on this. The three-item CM measurements were modified from Yang et al. 43
Constructs and measurements

PHT: perceived health threat; IU: intolerance of uncertainty; HA: health anxiety; OHISB: online health information-seeking behavior; FHISB: offline health information-seeking behavior; CM: catastrophic misinterpretations.
Ethical approval and patient consent
The study protocols were approved by the Ethics Committee of the School of Information Management, Nanjing University. Rural residents willing to complete the survey indicated their informed consent. Subjects’ confidentiality and privacy were upheld. Participants were free to skip any questions they chose or refrain from responding at all.
Sample
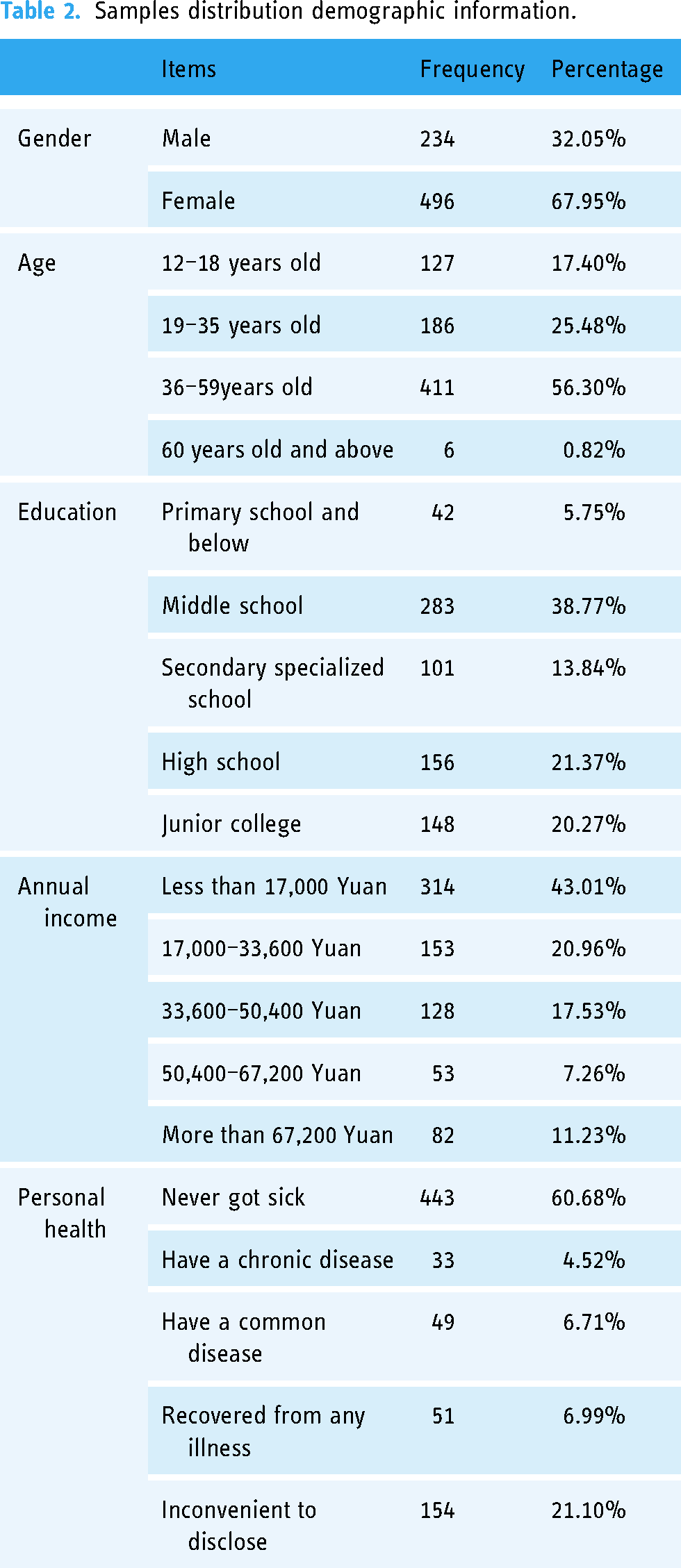
We designed the online survey and posted it on Wenjuanxing (https://www.wjx.cn/), a survey platform in China. Using snowball sampling, the participants were recruited from June 20 to July 5, 2022. To be more precise, we first recruited a group of students at a large comprehensive university from rural areas of different Chinese provinces (including Hubei, Jiangxi, Sichuan, Guangdong, Chongqing, Fujian, Zhejiang, and Guizhou). These students were invited to send a link to the questionnaire via WeChat to local residents they were familiar with. They also got in touch with the local residents’ committee and asked for help in sharing the questionnaire with the local villagers. We provided the official research survey statement released by the organization where the research team was based and instructed the students in order to successfully connect with the residents’ committee. After completing the survey, each participant will be given a $1 prize. 977 questionnaires in total were collected, and data were screened in two ways: (a) Data with less than 120 s of response time; (ii) data with the same options selected for all items; and finally, there were 730 valid responses recorded, for a recall rate of 75%. Table 2 provides information about the sample. Among the 730 participants, 57.12% were aged 36 and over. 79.93% have a high school education or below, and 82.5% have an annual income of 50,400 yuan or less. The demographic profile is in line with the documented attributes of the rural population in China, suggesting that our study has a relatively good sample representation. 44
Samples distribution demographic information.
Data analysis and results
Considering that all constructs in our model were measured using a seven-point Likert scale based on respondents’ subjective perceptions, it is difficult to easily determine normality. Therefore, partial least squares-based structural equation modeling, which does not require consideration of data normality, was used for analysis in our study.
Measurement model. We first employed Harman's single-factor test to examine common method variance. 45 The results from SPSS 25.0 showed that the overall cumulative variance was larger than 60% and the explained variance of the first component was less than 40%, thus dictating that there was no common method bias in this study.
Then the reliability and validity of the measurement model were checked using SmartPLS 3.2.8. All indicators in our study are modeled to reflect their respective structures. As shown in Table 3, the factor loadings for all measurement items on their respective constructs were higher than the suggested threshold of 0.60, 46 indicating sufficient indicator reliability and convergence validity. And values of Cronbach's alpha (α) and composite reliability for each construct in the scale are respectively greater than 0.70 and 0.80, meeting the established criterion for construct reliability values, 47 hence suggesting internal consistency.
Reliability and convergent validity of measurement model.
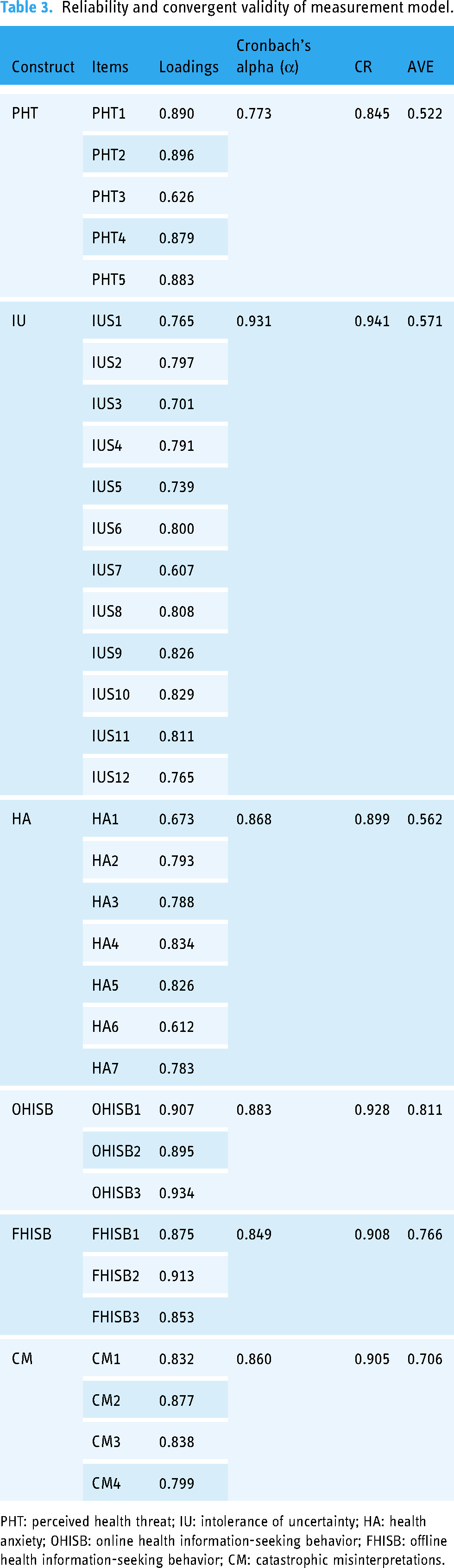
PHT: perceived health threat; IU: intolerance of uncertainty; HA: health anxiety; OHISB: online health information-seeking behavior; FHISB: offline health information-seeking behavior; CM: catastrophic misinterpretations.
And the AVE values shown in Table 3 were higher than 0.5, demonstrating convergent validity. In a latent variable correlation matrix, the square root of AVE for each construct was higher than the intra-construct correlations, indicating discriminant validity; 46 see Table 4.
Discriminant validity for Models 1 and 2.
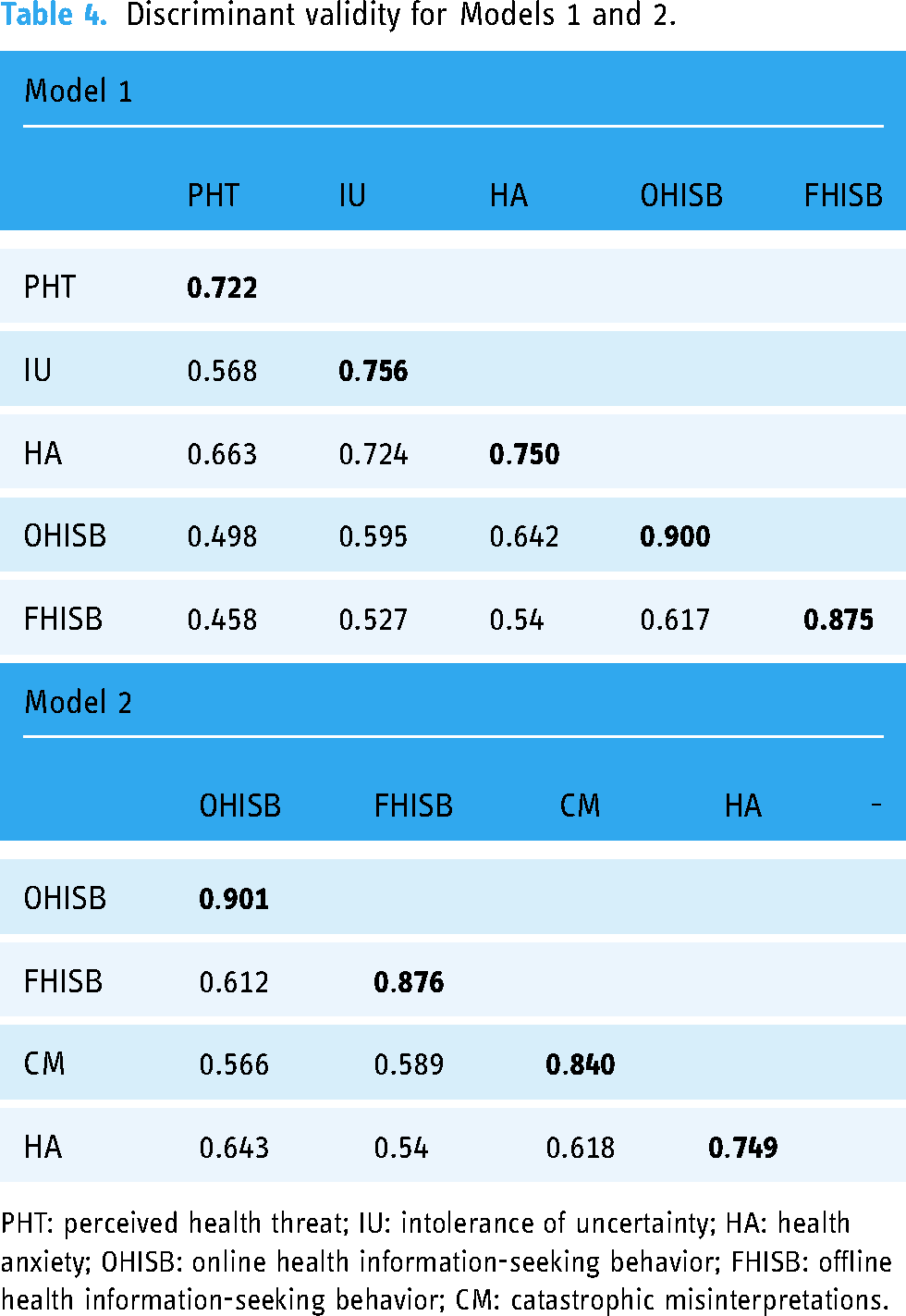
PHT: perceived health threat; IU: intolerance of uncertainty; HA: health anxiety; OHISB: online health information-seeking behavior; FHISB: offline health information-seeking behavior; CM: catastrophic misinterpretations.
Structural model. In this stage, we first assessed the degree of multi-collinearity with the variance inflation factor (VIF) for each independent variable. Regression analyses were conducted, respectively, by modeling OHISB and FHISB as dependent variables and the other three variables as independent variables in Model 1, or the other three variables as dependent variables with HA as the predictor variables in Model 2. The results show that the value of VIF varies from 1.00 to 1.47 in Model 1 and from 1.60 to 1.85 in Model 2, all of which are much less than 3, thus it can be regarded that there is no significant multi-collinearity in our data. 48
Then the path coefficient, the correlation coefficient R2 of the endogenous variables, and the effect size f2 were tested using the bootstrapping (N = 5000) technique. The value of f2 is independent of sample size and can be used to compare values measured at various sizes, indicating practical significance. 49 As shown in Table 5, the values of R2 range from 0.292 to 0.618 in Model 1 and 0.414 and 0.514, respectively, in Model 2, indicating that both models have favorable explanatory power. 48 And PHT revealed a positive effect on HA (β = 0.371, P < 0.001) with a medium effect size (f2 = 0.244), therefore supporting hypothesis H1. IU also showed a significant influence on HA (β = 0.514, p < 0.001), with large effect sizes (f2 = 0.468), supporting hypotheses H2. HA positively influenced OHISB and FHISB (β = 0.642, P < 0.001; β = 0.540, P < 0.001), both having a substantial effect (f2 = 0.701, f2 = 0.412), thus supporting hypotheses H3a and H3b. In addition, both OHISB and FHISB showed a favorable impact on HA (β = 0.389, p < 0.001; β = 0.104, p < 0.05), but only the former effect was of medium size (f2 = 0.171), thus supporting hypotheses H4a and H5a. OHISB and FHISB also have a positive impact on CM (β = 0.329, p < 0.001; β = 0.388, p < 0.05), with small and medium effect sizes (f2 = 0.115, f 2 = 0.161), supporting H4b and H5b. CM has a positive impact on HA with a small effect size (β = 0.336, p < 0.001, f2 = 0.136), supporting H6a.
R2 path coefficients, and effect sizes of the structural Models 1 and 2.

PHT: perceived health threat; IU: intolerance of uncertainty; HA: health anxiety; OHISB: online health information-seeking behavior; FHISB: offline health information-seeking behavior; CM: catastrophic misinterpretations.
***p ≤ 0.001, *p < 0.05, f² ≥ 0.02 = small effect size, f² ≥ 0.15 = medium effect size, and f² ≥ 0.35 = large effect size.
Mediation test
To describe the process of mediation tests more clearly, we use a, b, and c to denote the path effects between different variables, as shown in Figure 2. According to Nitzl et al., the test steps are as follows: (a) Determine the significance of the indirect effect ab, i.e., a1*b, a2*b. If the effect exists, the mediation effect exists; otherwise, there is no mediation effect; (b) evaluate the significance of the direct effect c’, i.e., c1′and c2′, to further determine the type of intermediation. If the indirect effect ab is significant but the direct effect c' is not, then it is full mediation; if both the indirect and direct effects are significant, then it is partial mediation. 50 Bootstrapped confidence intervals (CIs) are used to identify the significance of indirect and direct effects, 47 and all the results are analyzed from SmartPLS 3.2.8. The results shown in Table 6 indicate that CM partially mediates HISB (both OHISB and FHISB) and HA, thus supporting H6b and H6c.

Mediation model.
Bootstrapped CIs mediation test.
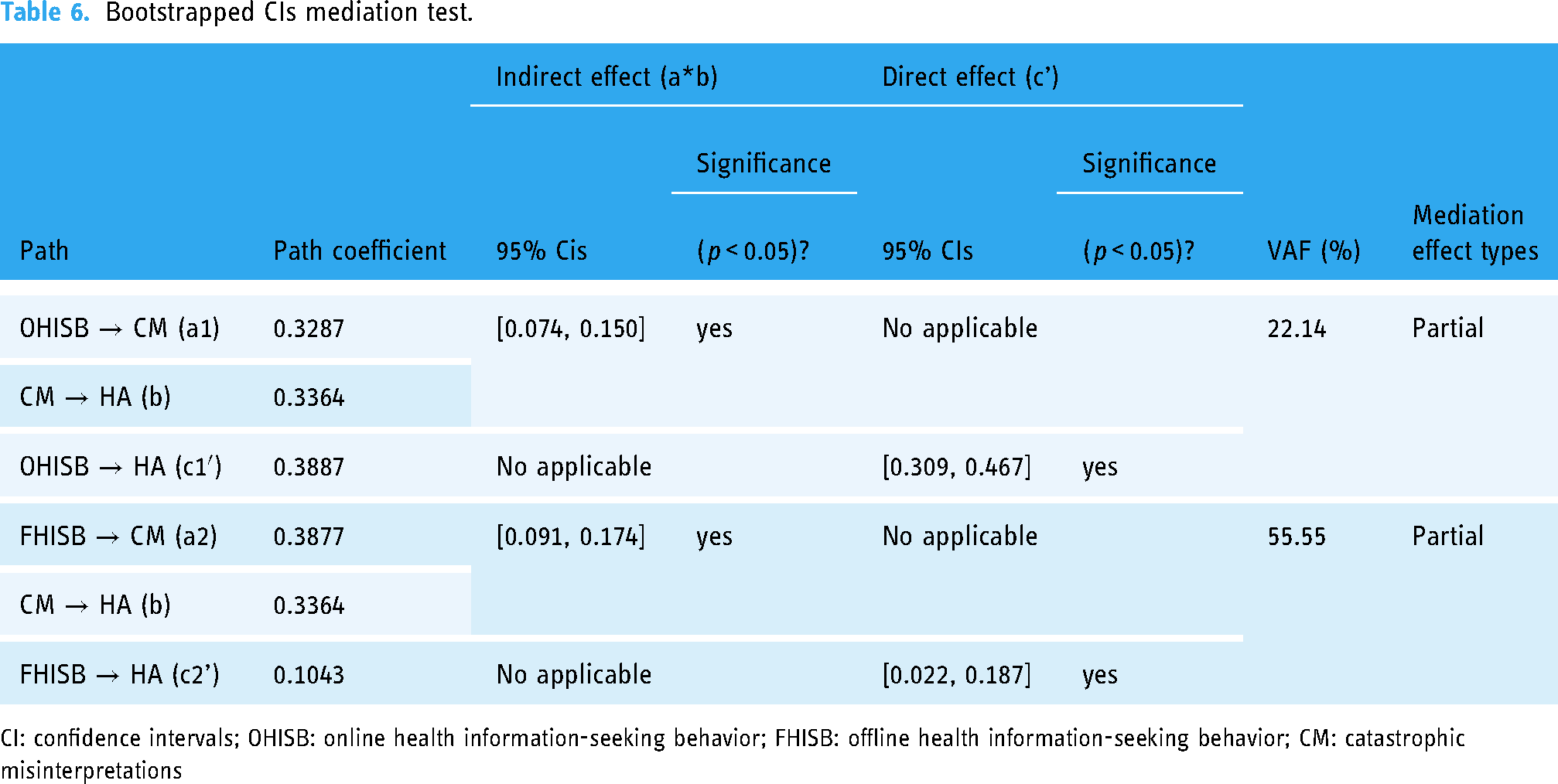
CI: confidence intervals; OHISB: online health information-seeking behavior; FHISB: offline health information-seeking behavior; CM: catastrophic misinterpretations
To find out more about the strength of the effect of CM as a mediator, we calculated the ratio of the indirect-to-total effect, i.e., (ab)/(ab + c'), which is known as the VAF value. 47 The results showed that CM mediated FHISB and HA (VAF = 22.14%) more strongly than it mediated OHISB and HA (VAF = 55.55%).
Discussion and implications
Findings
This study was conducted to investigate the relationship between HA and HISB (both FHISB and OHISB) when operating as antecedents and outcomes, respectively.
First, when considering HISB as consequences, PHT and IU are confirmed to positively contribute to HA, suggesting that when individuals feel afraid or powerless about health problems or have a low tolerance for uncertainty, it drives their negative emotions. The findings are consistent with the positive relationship between PHT, IU, and HA described in recent research. 51 And consistent findings were found in those studies conducted prior to the COVID-19 outbreak. 52 Then we identify the effect of HA on OHISB and FHISB. Consistent with recent findings in the general population, 5 the findings of this study suggest that HA motivates OHISB among rural residents in a direct and powerful manner. And the findings of studies conducted prior to the COVID-19 outbreak support this conclusion. 10 Notably, we also find that HA positively stimulates FHISB. And the size of the effect of HA on FHISB is large statistically. However, this point has received little attention in previous studies, which may be due to the fact that previous studies have focused on Internet populations.
Second, when considering HISB as an antecedent, both OHISB and FHISB affect HA in two ways. The results show that OHISB is a direct predictor of HA with a medium effect size. Barriers to OHISB, such as retrieval or assessment barriers, may lead to further increases in HA in rural populations due to their lack of health information literacy, which is consistent with existing research. 10 And OHISB influences HA via the partially mediating role of CM. Inadequate health information literacy leads to individuals misjudging the vast amount of online health information, which reinforces worry. Several studies support this argument in the context of other demographics. 43 Similarly, FHISB also has a positive impact on HA, and the CM partially mediates the effect of FHISB on HA. In contrast to the effect of OHISB on HA, the direct effect of OHISB on HA, although statistically significant, was so small in effect size as to not be practically meaningful, whereas the effect on HA through the mediator of CM was sizable, suggesting consistency in the effects of the two impact pathways. It indicates that even though offline access to health information is typically the most desired method by the disadvantaged, it can still result in increased HA owing to biased perceptions of the information.
The current results provide further support for relationships between these variables in the context of late COVID-19 development. However, there is no evidence of a direct relationship between health beliefs, HA, and HISB over time to the end of the epidemic. Although data collection occurred late in the pandemic, a later date at the end of the COVID-19 pandemic may be needed to detect any temporal relationships between these variables.
Theoretical implications
There are three theoretical contributions to this study. First, this study developed two models of the relationship between HISB and HA when used as a consequence event and a stimulus event, respectively. Previous works have often focused on HISB as a consequence of HA or as an antecedent of cyber-hypochondria. We investigate the complex relationship between HA and HISB simultaneously in the same context, going beyond past studies of a single relationship between the two.
Secondly, the study focused on a subset of rural populations who were more vulnerable in terms of health perceptions and literacy, as well as information literacy and health information behaviors. Their HA and HISB performance differed from that of the general population. Together with OHISB, an association between FHISB and HA was also confirmed. This strengthens the research on HA and HISB.
Finally, we extend the literature related to the ABC model by conceptualizing stimulus events, beliefs, emotions, and behavioral consequences in the context of HA and HISB. Whereas previous literature has mostly examined theories through belief-seeking correlations, we focus on how PHT and IU influence HA, how HA in turn influences HISB, and how HISB influences HA both directly and through CM. Such conceptions are crucial because they demonstrate how stimulus events, beliefs, emotions, and behaviors interact. As a result, this study provides an original research perspective.
Practical implications
This study also offers several potential practical guidelines. Firstly, this work is important for reducing HA and promoting health management in disadvantaged groups. The health-related beliefs PHT, IU, and CM are important causes of HA. Even though more than half of the sample claimed that they had not been ill in the past year, they were still worried about their health. We suggest that individuals should focus more on increasing their health-related knowledge to develop the right health beliefs, which can help stop HA where it starts. It is also recommended that medical institutions and government organizations provide authoritative health services, including popular lectures on common diseases such as chronic diseases, frequent medical check-ups, the development of authoritative and user-friendly health information platforms, and the establishment of comprehensive personal health records that will help to understand one's health status and calibrate health beliefs for successful health management.
Secondly, this work will help guide and regulate the HISB of disadvantaged groups like rural residents. Health information-seeking activities can lead to catastrophic beliefs about the health status of individuals who blindly match their symptoms with the health information they find, thereby increasing HA. We recommend that individuals take care in their search to identify the authenticity and relevance of information and seek professional medical help whenever possible. We also recommend that medical professionals provide patients with more comprehensive and understandable explanations, as well as competent and straightforward advice. Furthermore, OHISB can directly lead to further HA. We therefore recommend that relevant information services develop specific information literacy courses or provide counseling for the rural group to guide them through the assessment and screening of health information.
Conclusions
This study investigated the interaction between HA and online and offline health information behaviors among a rural Chinese population, and the role of belief factors, which provides guidelines for the alleviation of HA and management of health behaviors in vulnerable groups. However, there are several limitations to the current study that might be considered in the future.
First, the survey in the current study was conducted at a later stage of COVID-19 development in China, but we did not investigate the role of COVID-19 and the cultural context. Although the findings are consistent with those of studies conducted before and during epidemics in different cultural contexts, there is no statistical evidence. In the future, a meta-analysis will be considered to explore in depth the differences in the strength of the relationship between health beliefs, anxiety, and behaviors before and during the COVID-19 outbreak and the reasons for this, as well as a longitudinal study that explores the relationship between these variables during and after the end of COVID-19 and the role of COVID-19 in this. Second, just three belief components were considered in this study through quantitative method. In the future, other possible factors and the complex relationships between beliefs, emotions and behaviors can be explored through a mixed research approach. Finally, our study positioned the role of HISB in two models and considered the relationship between HA and HISB through cross-sectional analyses, whereas in the future the dynamics between HA and HISB will be considered in an integrated model based on longitudinal data.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231208559 - Supplemental material for Using the ABC theory of emotion to examine the relationship between health anxiety and health information-seeking behavior among the rural population
Supplemental material, sj-docx-1-dhj-10.1177_20552076231208559 for Using the ABC theory of emotion to examine the relationship between health anxiety and health information-seeking behavior among the rural population by Hongcun Gong, Sanhong Deng, Hao Wang and Gaohui Cao in DIGITAL HEALTH
Footnotes
Contributorship
The study was conceived by GHC, the manuscript was drafted by HCG and further edited by SHD and HW. The final manuscript was approved by all four authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Fundamental Research Funds for the Central Universities, Nanjing University (No. 0108/14370317).
Guarantor
GHC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.