
Abstract
Background
Tackling physical inactivity represents a key global public health challenge. Strategies to increase physical activity (PA) are therefore warranted. Despite the rising availability of digital interventions (DIs), which offer tremendous potential for PA promotion, there has been inadequate attention to the special needs of older adults.
Objective
The aim was to investigate community-dwelling older adults’ needs, requirements, and preferences toward DIs to promote PA.
Methods
The target population of this cross-sectional study was community-dwelling older adults (≥60 years old) within German-speaking Switzerland. Potential respondents were informed about the study and sent a link to a self-developed and self-administered online survey by our cooperating institutions.
Results
Overall, 922 respondents who completed the online survey were included in the final analysis. The mean age of the sample was 72 years (SD 6.4, range 60–98). The preferred delivery mode of DIs to promote PA was a website (428/922, 46.4%) and 80.3% (740/922) preferred video-based structures. Most respondents expressed the need for personal access, personal goals, personal messages, and a personal contact in case of problems or questions (585/817, 71.6%; 546/811, 67.3%; 536/822, 65.2%; 536/822, 65.2%). Memory training, psychological wellbeing, and nutrition were mainly rated as relevant additional content of DIs to promote PA (690/849, 81.2%; 661/845, 78.2%, 619/849, 72.9%).
Conclusion
Community-dwelling older adults may be willing to use DIs to promote PA in the long term, but this study identified particular needs and requirements in terms of design, technological realization, delivery mode, support, and individualization/personalization among the sample. Our results can inform future developments of DIs to promote PA specifically tailored to older adults. However, caution is warranted in interpreting the findings due to the sample's high PA and education levels.
Introduction
Background
Worldwide, about 28% of adults fail to meet physical activity (PA) guidelines of the World Health Organization (WHO) with even higher levels among older age groups.1,2 Physical inactivity is a known risk factor for numerous noncommunicable diseases, such as cardiovascular disease, and augmented all-cause mortality.1,3 A study in 2021 reported a prevalence of mortality related to physical inactivity of 9.3% in high-income countries. 4 Additionally, the global target of a 10% relative reduction of physical inactivity by 2025, set by WHO member states, is not on track. 1 In Switzerland, 1 out of 5 older adults aged 65 to 74 years is not sufficiently physically active, whereas the proportion increases to one-third from the age of 75 years. 5 Thus, physical inactivity needs urgent action, and effective as well as engaging interventions for PA promotion and participation in older adults are needed. 6
The WHO defines PA “as any bodily movement produced by skeletal muscles that requires energy expenditure.” 7 In consequence, PA is not limited to sports but can involve traveling, work, domestic tasks around the home, or active forms of recreation. 8 According to the WHO, adults (including those 65 years and older) should complete at least 150 minutes of moderate-intensity aerobic PA per week, or at least 75 minutes of vigorous-intensity aerobic PA per week, or an equivalent combination of the two intensities throughout the week. Supplemental muscle-strengthening activities on 2 or more days of the week should be performed for additional health benefits. 8 The health-enhancing effects of PA are well documented. PA can positively affect cognitive and physical decline, symptoms of depression and anxiety, functional mobility, and wellbeing.1,9 Embracing clinical, psychological, and social benefits, PA represents a major contributor to successful healthy aging. 10
Digital interventions (DIs) employ digital technologies (e.g. websites, applications, and wearable devices) that can be used to promote health and support behavior change. 11 Different digital devices can be used for DIs with each having its specific characteristics, for example, in terms of screen size, screen resolution, and portability. As regards support and interaction levels, different categories of DIs are used in research—from providing educational material only to coaching and monitoring. DIs offer a feasible and easily accessible alternative to counteract some of the obstacles to on-site interventions since they may be able to mitigate location constraints as well as financial and time limitations.12–14 Computer-tailoring techniques even enable personalization at low cost 15 and simultaneously entail sustainable and scalable properties allowing widespread dissemination.16,17 When looking at the effectiveness, there is growing evidence that blended PA interventions—a new delivery mode of linking face-to-face with digital components—show more promising results in older adults than the separated components.18–20 A meta-analysis showed that, in the short term, digital behavior change interventions to promote PA and/or reduce sedentary behavior in older adults aged ≥ 50 years may lead to increases in PA levels and physical functioning as well as reductions in sedentary behavior. 21 Additionally, evidence suggests that web-based PA programs are suitable,22,23 economical,12,24 and effective at increasing PA levels in older adults.25–29
A lack of user engagement, that is, nonuse or insufficient use, can hinder the optimal exploitation of potential within DIs. Different reviews of DIs targeting lifestyle behaviors concluded that better engagement was associated with larger effectiveness.30,31 However, there seems to be a discrepancy between newly developed digital technologies and older adults’ needs, requirements, and preferences.32,33
The myriads of available websites and apps tend to focus on younger adults with higher levels of digital literacy. 17 Digital technologies aiming at older adults are required to be designed appropriately in order to be suitable for them.22,34 Shaping DIs to promote PA to an older audience requires a prudent approach because barriers to uptake and use remain in older adults.29,35 Barriers can include, for instance, physical impairments or lack of instructions and guidance. 36 In addition, older adults are often the last group to adopt internet use making them particularly vulnerable to digital inequality. 37 Hence, the investigation of how older adults use and perceive DIs is a salient point to assist with introducing technology to this population. 36 A focus group study explored older adults’ perceptions and preferences regarding web-based PA interventions and gave first insights into characteristics of these interventions that should be addressed to satisfy the needs of older adults. 38 The study's findings indicated that web-based PA interventions should prioritize simplicity and clarity, and include features such as reminder check-ins, goal review options after illness or injury, clear and visually appealing PA graphs, self-monitoring capabilities and personalized advice based on the user's health status. Nevertheless, these results are limited to web-based PA interventions. Research on a more generic level that covers all types of DIs to promote PA without being limited to specific devices or mediums is required. 32 Moreover, cross-sectional data from larger samples and samples living in different regions are warranted.
Objective
This cross-sectional survey study aimed to examine the needs, requirements, and preferences of community-dwelling older adults aged 60 years and above toward DIs to promote PA. In addition, determinants for the design, technological realization, and delivery mode of DIs to promote PA targeting older adults should be pinpointed.
Methods
Design
The present study was conducted as a cross-sectional study using an online self-administered survey. The STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology) 39 for cross-sectional studies were followed (Supplemental file 1).
Setting and recruitment
The target population was community-dwelling older adults. There are different classifications of age groups, and the concept of “old age” is multidimensional. Thus, thresholds of old age can differ across countries and organizations. This study adopted the definition of the United Nations that uses 60 years or above to refer to older people. 40
The inclusion criteria for survey participation were a minimum age of 60 years and an understanding of German. An internet connection was required since the survey was solely provided in a web-based format. The sampling technique used for recruitment was chain-referral sampling. The survey invitation and the eligibility criteria were announced via email, social media, or on the corresponding website by Bern University of Applied Sciences, the Senior Citizens’ University of Zurich, senior platforms and websites, senior associations, and service providers for older people within German-speaking Switzerland. The survey link was embedded in this invitation. Participation in the study was voluntary and the respondents were assured irreversible anonymity. Nonparticipation did not entail any disadvantages. The survey was accessible online from October 4, 2021. Data collection remained open until February 15, 2022. Study data were collected and managed using REDCap (Research Electronic Data Capture)41,42 tools hosted at the University of Zurich (Epidemiology, Biostatistics and Prevention Institute).
Online survey
We constructed the survey based on literature and the experience of relevant professionals because there were no suitable published survey instruments assessing the needs of older adults toward DIs to promote PA. The original version of the survey in German and an English translation are provided in Supplemental files 2 and 3. A pretest was performed with two community-dwelling older adults (target group) and five research associates. One of these professionals had expertise in physical therapy and sports science, another one in gerontology, one in nutrition, one in medical informatics, and the last one in health psychology and public health. The main evaluation criteria were relevance, comprehensibility, and structure. After the revision, all participants of the pretest agreed that each item was relevant and the wording of the items was appropriate.
The following definition of DIs derived from Alkhaldi et al. 30 (translated into German) was given to the respondents at the beginning of the survey to enhance consistent understanding: “Digital interventions to promote physical activity are programs that provide information and/or support about physical activity via a digital platform (e.g. websites, television, or applications).”
The survey consisted of the following sections:
Sociodemographics, use of technology, and PA levels: Comprising items related to respondents’ gender, age, weight, height, living status, highest education level, use of digital technologies, and PA levels in line with the WHO guidelines. Use and motivation: Comprising items related to the use and the reasons for (not) having used/using DIs to promote PA. Technological realization and design: Comprising items related to the preferred technological realization (e.g. video- or text-based), delivery mode, and design (e.g. clarity and font) of DIs to promote PA. Support and individualization/personalization: Comprising items related to the required level of support and individualization/personalization within DIs to promote PA. Modalities and other content: Comprising items related to PA modalities and interest in additional content within DIs to promote PA.
Ideas and remarks
Neither personally identifying information nor IP addresses were collected. The survey comprised closed-ended questions (numerical, single-, and multiple-choice) as well as two open-ended questions for comments. Besides, each item included the optional answer “other” where additional input could be entered in a free-text field. Two authors (MW and AMR) reviewed and categorized all answers within free-text fields separately. In case of discrepancies, a third author (KUS) was consulted to reach a final consensus. The fully de-identified dataset is kept on password-protected computers of the involved investigators. Further details can be found in the Checklist for Reporting Results of Internet E-Surveys (CHERRIES)
43
listed in Supplemental file 4.
Statistical analysis
We included all responses in the analysis regardless of missing data; thus, the number of total responses for each survey item varied. Data were collected anonymously and descriptively analyzed. The results of the descriptive statistics were presented as frequencies and percentages for categorical data and additionally medians and interquartile ranges for ordinal data. Means and standard deviations as well as medians and interquartile ranges were indicated for numerical data. Owing to rounding error (one decimal place) total percentage can deviate slightly from 100%. Due to the descriptive nature of the study, outliers were retained in the analysis. An exploratory graphical approach to subgroup analyses through density plots without hypothesis testing was conducted. The following subgroups were investigated: (i) having already used DIs to promote PA versus never having used DIs to promote PA and (ii) willing to use DIs to promote PA in the long term versus not willing to use DIs to promote PA in the long term. The dependent variables were total PA per week, body mass index (BMI), and daily use of digital devices.
Analyses were conducted using R software 44 (version 4.1.3 for Windows) and figures were produced using the R packages ggplot2 45 and likert. 46
Results
The flow chart of study enrollment is depicted in Figure 1. A total of 953 survey returns were registered, whereby 24 duplicate datasets, which displayed the same timestamp and entries, were excluded. Moreover, seven respondents had to be excluded due to their age (<60 years). Hence, 922 respondents were included in the final analysis. Overall, 93% (857/922) had no difficulties in filling out the survey, whereas 3.1% (29/922) did not answer this question. The main problems raised by the other respondents (36/922, 3.9%) were the length of the survey and difficulties in responding to the items concerning their PA levels. All optional free-text answers are summarized in Table S1 in Supplemental file 5.
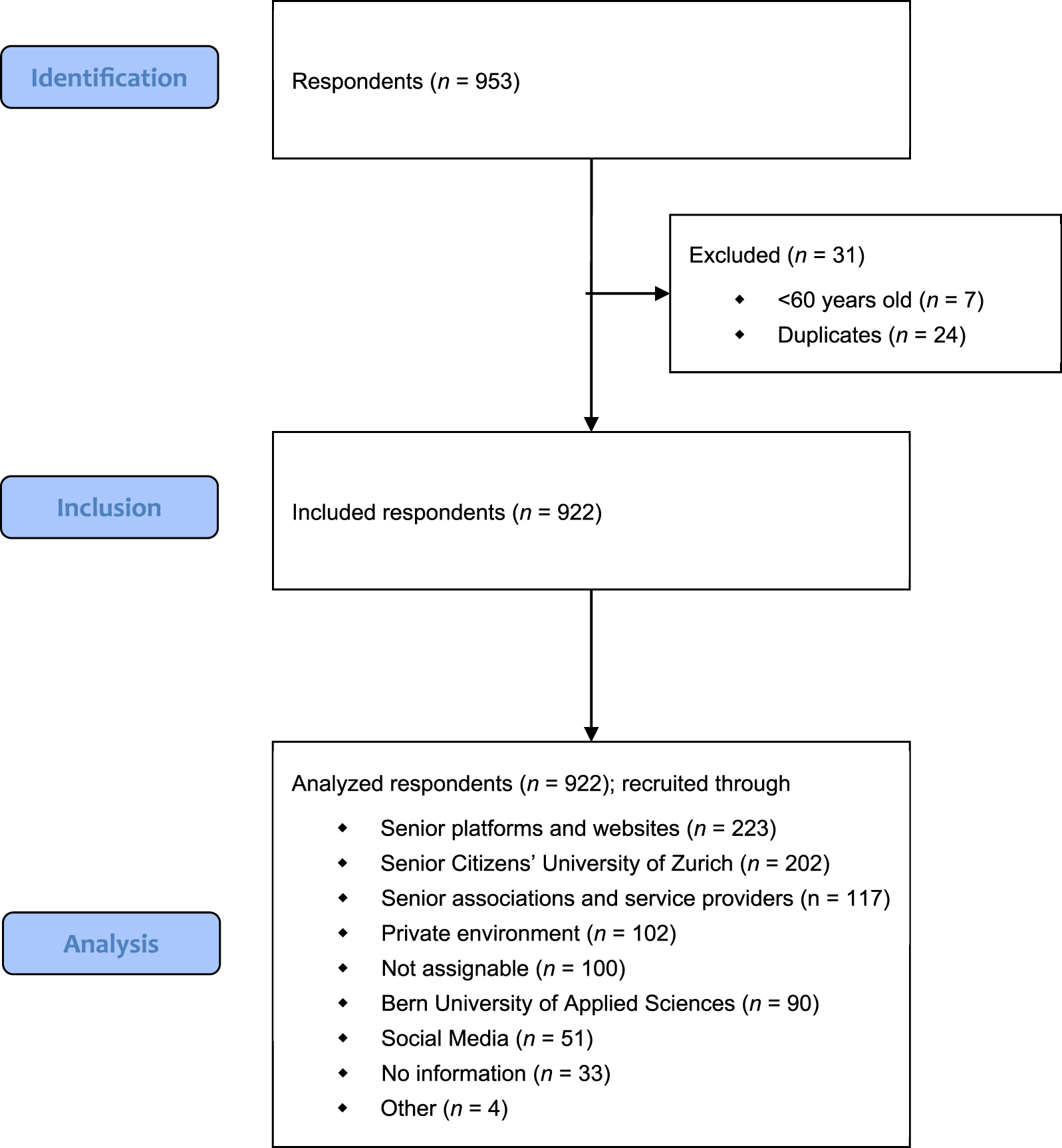
Flow chart of study enrollment.
Sample characteristics
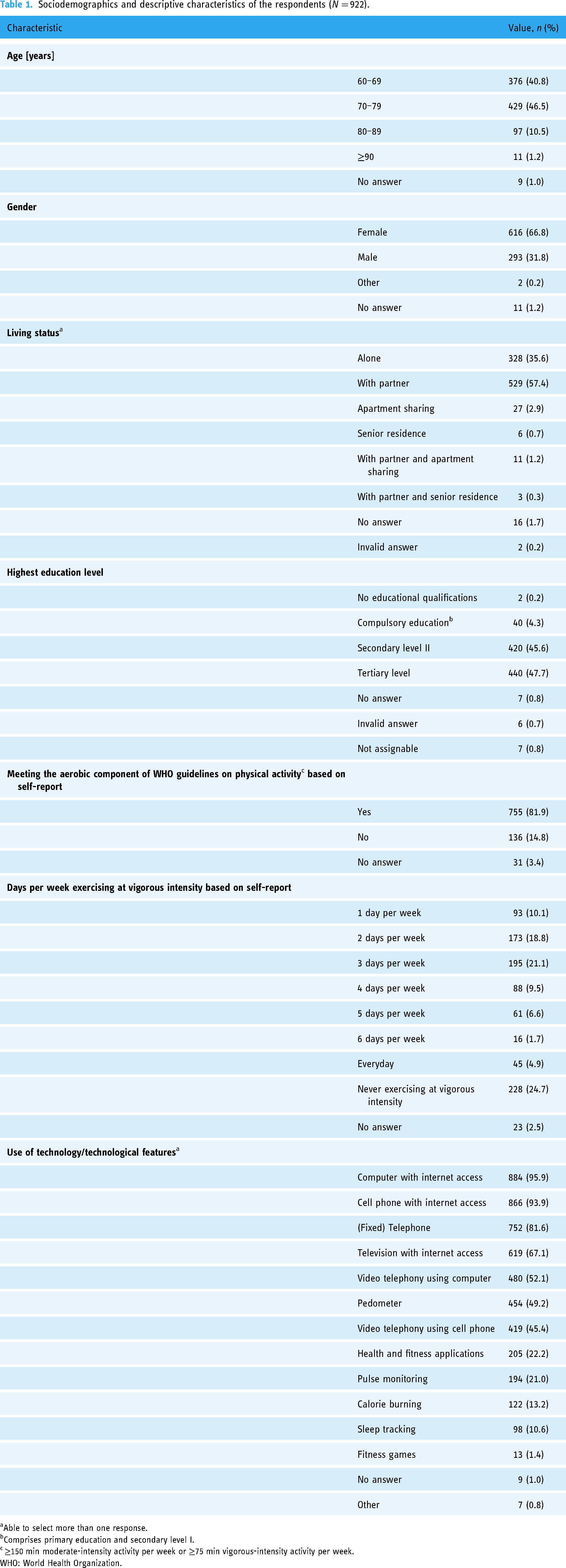
The majority of the sample identified themselves as women (616/922, 66.8%) (Table 1). Most older adults were between 70 and 79 years old (429/922, 46.5%) and lived together with a partner (543/922, 58.9%). The respondents’ highest education level was most frequently secondary level II or higher (860/922, 93.3%). Overall, 81.9% (755/922) of the sample met the aerobic component of the official guidelines of the WHO on PA based on their self-reported PA. Few respondents (16/922, 1.7%) indicated that they would never be physically active at moderate intensity, whereas 24.7% (228/922) stated that they would never exercise at vigorous intensity. The most used technologies and technological features in everyday life were computers and cell phones with internet access (884/922, 95.9%; 866/922, 93.9%). The self-reported daily use of digital devices ranged from 20 minutes to 12 hours (mean 3.3, SD 1.9) (Table 2). A differentiation of the descriptive characteristics by gender can be found in Table S2 in Supplemental file 5.
Sociodemographics and descriptive characteristics of the respondents (N = 922).
Able to select more than one response.
Comprises primary education and secondary level I.
≥150 min moderate-intensity activity per week or ≥75 min vigorous-intensity activity per week.
WHO: World Health Organization.
Descriptive characteristics of the respondents with and without extreme outliers.

All characteristics are based on self-report.
Never using digital devices (n = 2).
Intensity level according to the World Health Organization; moderate-intensity activity: 3–6 metabolic equivalents; examples include brisk walking, hiking, dancing, gardening, and vacuuming.
Never physically active at moderate intensity (n = 16).
Intensity level according to the World Health Organization; vigorous-intensity activity: >6 metabolic equivalents; examples include running, fast cycling, and fast swimming.
Never exercising at vigorous intensity (n = 228).
BMI: body mass index; EO: extreme outliers (defined as 3 × IQR); IQR: interquartile range; SD: standard deviation.
Use and motivation
More than half of the respondents have never used DIs to promote PA (556/922, 60.3%) (Table 3). The main reasons were because of already being physically active in everyday life and the lack of interest in DIs (276/570, 48.4%; 168/570, 29.5%). The optional free-text answers that appeared most frequently were the unawareness of available programs (n = 12), the preference for outdoor activities (n = 7), the participation in existing institutional/organizational programs (n = 6), and the lack of knowledge which programs are appropriate and suitable (n = 6) (Table S1 in Supplemental file 5). By contrast, the main reasons for having used or using DIs to promote PA at the time of questioning were the possibility to use them at home, the knowledge about the importance of PA, maintaining/increasing quality of life as well as strength (253/366, 69.1%; 213/366, 58.2%; 201/366, 54.9%; 198/366, 54.1%). The usage frequency of those older adults having used or using DIs to promote PA at the time of questioning ranged from daily to less than once per month (40/366, 10.9%; 11/366, 3.0%). A small minority stated that they will/would never use DIs to promote PA in the long term (74/922, 8.0%).
Use and reasons for (not) having used/using digital interventions to promote physical activity.

Able to select more than one response.
Technological realization and design
Most respondents indicated that they would prefer a complete program as a video (434/922, 47.1%), followed by short videos (306/922, 33.2%), and an individually adaptable program (297/922, 32.2%) (Table 4). Furthermore, the desired delivery mode was a website (428/922, 46.4%), whereas small proportions preferred DVD/CD (68/922, 7.4%) and fitness games (25/922, 2.7%). The most frequent free-text answers to this question were virtual meetings (n = 16) and organizational/institutional programs (n = 9) (Table S1).
Respondents’ preferences for digital interventions to promote physical activity in terms of technological realization, delivery mode, and session duration (N = 922).

Able to select more than one response.
Simple handling, trustworthiness, and clarity were indicated to be rather important, important, or very important attributes of DIs to promote PA by a vast majority of respondents (812/842, 96.4%; 818/851, 96.1%; 795/840, 94.6%) (Figure 2). The highest proportion of the response “very important” was given to trustworthiness (537/851, 63.1%). The color design was perceived to be less important compared to other attributes (475/813, 58.4%). Important elements that appeared repeatedly in the optional free-text answers were a comprehensible program with simple explanations (n = 9) as well as a motivating (n = 5), humorous (n = 5), and likable (n = 3) instructor (Table S1).

Perceived importance of different attributes within digital interventions to promote physical activity.
Support and individualization/personalization
The majority of respondents disagreed to an extent with the statements of receiving regular home visits or regular phone calls as well as scheduling regular virtual appointments with a professional within DIs to promote PA (741/809, 91.6%; 688/805, 85.5%; 596/810, 73.6%) (Figure S1 in Supplemental file 5). Moreover, most older adults indicated that they rather disagree, disagree, or strongly disagree with the statement of having an introductory meeting with a professional at the beginning (home visit: 688/804, 85.6%; phone call: 605/809, 74.7%; virtual appointment: 542/814, 66.6%). However, 54.1% (440/813) and 50.9% (414/814), respectively, agreed to an extent with the statement of receiving individual advice from a professional for content support and technical support, respectively. In addition, 65.2% (536/822) agreed to an extent that they would like to have a personal contact within DIs to promote PA in case of problems or questions. More respondents disagreed with the possibility of an exchange with other users about their private lives (696/802, 86.8%) than an exchange about the intervention itself (533/815, 65.4%). In terms of individualization/personalization, 47.5% (388/817) agreed or even strongly agreed with the need for personal access to DIs to promote PA. Setting personal goals was agreed or strongly agreed on by 40.3% (327/811) and receiving personal messages, such as reminders or tips, was agreed or strongly agreed on by 37.3% (307/822) of the respondents.
Physical activity modalities and other content
In sum, all proposed intervention foci to promote PA were indicated to be very important, important, or rather important by the sample to a high percentage (Figure 3). Nevertheless, mobility, balance, and coordination were perceived as being even more important than endurance and strength. The highest proportion of the answer “very important” was shown in balance (448/847, 52.9%), followed by mobility (432/849, 50.9%), and coordination (343/830, 41.3%). According to the respondents, the most important additional theme within DIs to promote PA was memory training (Figure 4). All suggested additional foci were rated to be important or very important by most respondents (memory training: 528/849, 62.2%; psychological wellbeing: 492/845, 58.2%; nutrition: 439/849, 51.7%). Fun and pleasure were entered into the optional free-text answer to this question by eight respondents (Table S1). As regards the duration of one PA session within DIs, the most frequently selected answer among those who were interested in DIs to promote PA was 25 to 30 minutes (281/777, 36.2%) (Table 4).

Perceived importance of different intervention foci within digital interventions to promote physical activity.

Perceived importance of additional content within digital interventions to promote physical activity.
Exploratory subgroup analyses
Respondents who have already used DIs to promote PA or were using them at the time of questioning were similarly physically active than those who have never used DIs to promote PA (Figure 5(a)). Similar distributions were also observed for the BMI (Figure S2A in Supplemental file 5) and the daily use of digital devices in both subgroups (Figure S3A in Supplemental file 5). When it comes to long-term use, respondents who will/would use DIs to promote PA showed comparable PA levels (Figure 5(b)), BMIs (Figure S2B in Supplemental file 5), and amounts of time using digital devices (Figure S3B in Supplemental file 5) to respondents who will/would never use DIs to promote PA in the long term.
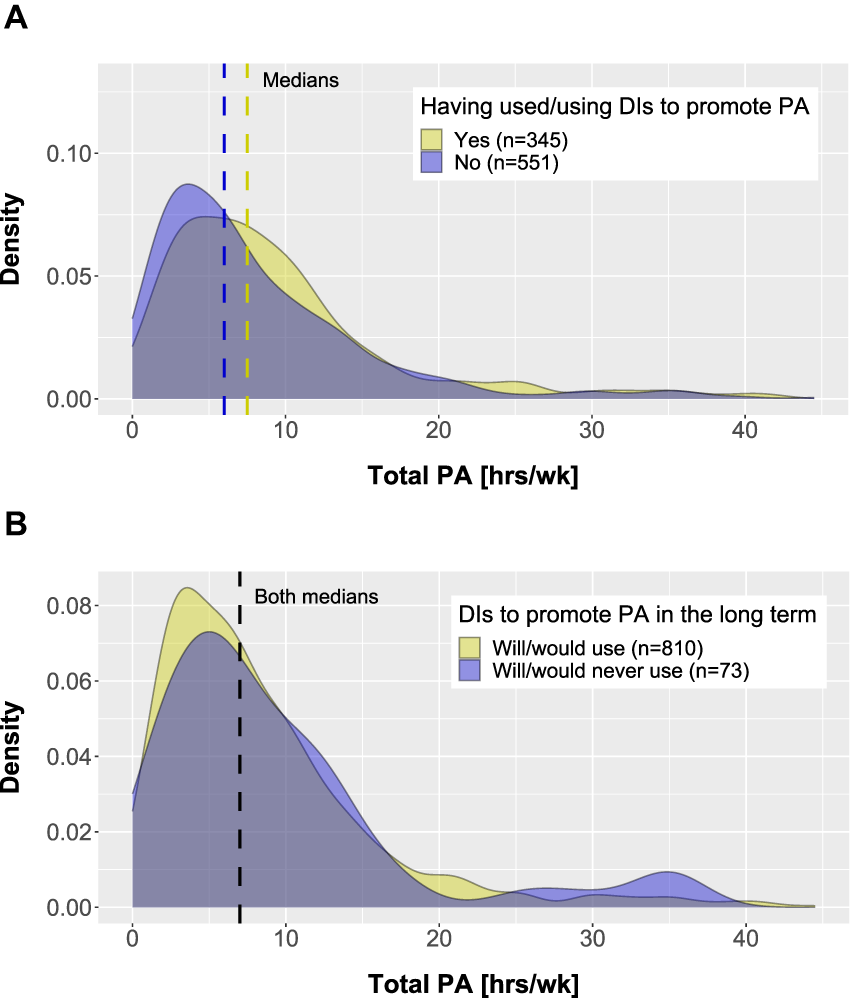
Density plots of PA by subgroups; (a) experience with DIs to promote PA and (b) long-term use of DIs to promote PA. DI: digital intervention; PA: physical activity.
Discussion
To the best of our knowledge, this study was the first cross-sectional survey study assessing the needs, requirements, and preferences of community-dwelling older adults aged 60 years and older toward DIs to promote PA. Evidence from our study suggests that a great majority of this population is willing to use DIs to promote PA in the long term, but their special needs and requirements in terms of design, technological realization, delivery mode, support, and individualization/personalization need to be considered to tailor these interventions.
Sample characteristics
This study revealed that many older adults have already used DIs to promote PA or were using them at the time of questioning. Almost 50% of respondents have already used or were using a pedometer in everyday life and one-fifth has even used or was using health and fitness applications in daily living at the time of questioning. Hence, our sample may have had high levels of digital literacy. Concomitantly, only a small percentage of the respondents indicated that they will/would never use DIs to promote PA in the long term. Interestingly, respondents who were willing to use them in the long term showed similar PA levels, BMIs, and amounts of time using digital devices per day. Likewise, PA levels, BMIs, and amounts of time using digital devices per day seemed to be comparably distributed in respondents who have already used DIs to promote PA and those who have never used DIs to promote PA. Thus, our sample included physically active older adults who have already used DIs to promote PA but also physically inactive older adults who have already used DIs to promote PA. However, our results should be interpreted with caution since our sample showed high PA and education levels, which does not apply to the entire population.
Barriers and facilitators
Apart from already having an active lifestyle and general disinterest in DIs, the main barriers to using DIs to promote PA were found to be a lack of self-motivation, social exchange, and supervision of movement execution, which corresponds to available literature.35,47 According to a scoping review of barriers to eHealth use among older adults, consistent barriers were problems with the user interface, for instance, screen or text issues. 35 These barriers might reflect physical conditions associated with aging, such as visual impairments or memory complaints. The framework MOLD-US synthesizes general aging barriers to digital (health) computer use classified into four categories: cognition (e.g. working memory), motivation (e.g. self-confidence using wearables), perception (e.g. color vision), and physical abilities (e.g. flexibility of joints). 34 Our study further confirms these results showing high percentages of perceived importance of color design, font and font size, simple language, simple handling, and clarity among respondents. Furthermore, two reviews suggested that digital health interventions should be trustworthy and credible in order to enhance engagement.35,48 Our findings substantiate these results because only a few respondents in our study stated that trustworthiness of DIs to promote PA was unimportant to them.
The main reasons for having already used or using DIs to promote PA in our sample at the time of questioning were the flexibility (usable at home), the knowledge about the importance of PA as well as the maintenance/increase of quality of life and strength. Therefore, most respondents were probably aware of how PA can elicit health benefits. In sum, education may represent a decisive facilitator for increasing health awareness and successful uptake of DIs to promote PA. Previous work examined the intention to use eHealth in older adults and drew comparable conclusions. 49 According to the authors, the acceptance of eHealth can be raised by informing people about the potential benefits of eHealth.
Other factors influencing the use of DIs to promote PA are their technological realization and delivery mode. Video-based and structured programs were preferred by most of our respondents. The preferred delivery mode was a website. When developing mobile applications to elevate PA levels in older adults, a web-based solution to access content should be concurrently available. Thus, interventions that are compatible and accessible across multiple technologies (e.g. smartphones and computers) ought to be offered. 35
As regards intervention foci, mobility was perceived as the most important one within DIs to promote PA among our respondents, followed by balance and coordination. These findings may be due to fear of losing independence or fear of falling, respectively, which are often highly prevalent among older populations. 50 Therefore, mobility, balance, and coordination should be integrated into future DIs to promote PA. However, strength and endurance are equally pertinent regarding the maintenance of autonomy and fall prevention. If DIs to promote PA involve strength and endurance exercises that improve mobility, balance, and/or coordination abilities as well, it should also be stated and explained to users.
Support and individualization/personalization
Surprisingly, our respondents disagreed with obtaining regular support within DIs to promote PA. Most respondents also disagreed with receiving support at the beginning of the intervention. These findings diverge from other studies suggesting that human support is vital to initial and sustained engagement of older adults in using digital platforms.51–53 A plausible explanation may be our respondents’ characteristics. Our sample showed high PA and education levels, thereby presumably being less receptive to or reliant on external support. Older adults with higher education levels master the digitalizing world better than their age peers with lower education levels do. 54 Nevertheless, half of our sample agreed with the need for individual advice from a professional for content and/or technical support. Additionally, having a personal contact in case of problems or questions was agreed on by most respondents. Overall, some sort of human support seems to be requested. Indeed, there is evidence that the effectiveness and adherence to DIs are fostered by human support.47,55 Therefore, the level and type of support should probably be modifiable and manageable by each user individually.
Compared to support, most respondents agreed with features of individualization and personalization. Future DIs to promote PA ought to enable access through a personal account. Moreover, personal messages and feedback as well as personal goals are supposed to be included. Our findings concur with existing research results showing that personalized features tailored to older adults’ needs act as motivators and facilitators.38,47,48 Likewise, previous work showed that digital behavior change interventions to promote PA or diminish sedentary time commonly feature goal setting and feedback. 21 A meta-analysis and meta-regression found that those interventions are particularly effective when feedback (e.g. text messaging) and personalization features (e.g. self-monitoring) are included. 56 By contrast, a randomized controlled trial, which evaluated personalized dietary and PA advice within a web-based intervention, revealed that different levels of personalization produced similar small changes in objectively measured PA. 57 Thus, the relationship between emerging costs when investing in highly personalized DIs to promote PA and the associated benefits remains unclear.
Limitations
The survey was self-developed since there was not yet a standardized questionnaire for assessing older adults' needs toward DIs to promote PA. Nevertheless, the survey was pretested before fielding. Further limitations of online surveys that cannot be eliminated are the presence of subjective interpretations by respondents, the self-reported nature of the data, and the exclusion of people not having access to a digital device for completing the survey. However, future older generations will supposedly become more and more familiar with digital technology leading to increasing digital literacy.
The investigated sample within the current study showed high PA and education levels such that generalizability is limited. The high percentage in our study may have resulted due to two conceivable reasons. First, we did not include older adults in assisted living or older adults in nursing and retirement homes. In a cross-sectional study, older adults in assisted living facilities showed lower PA levels than their community-dwelling counterparts. 58 Second, evidence proposes that education leads to a more physically active lifestyle. 59 Indeed, the main reason for never having used DIs to promote PA in our study sample was the answer of already being physically active in everyday life. It is therefore crucial to specifically target older adults with lower PA and education levels in future research through adequate recruitment strategies (e.g. probability sampling).
Furthermore, possible assistance for participants during data collection may be appropriate (e.g. completing surveys with the aid of research assistants). In addition, future research ought to utilize longitudinal data collection to gain deeper insights into how older adults use DIs to promote PA in the long term. Likewise, qualitative approaches, such as focus groups and interviews, could also be valuable to complement the understanding of older adults’ attitudes, motives, and behavior patterns.
Implications and considerations
Frequently, older adults are stereotypically framed as being frail and incompetent. Unfortunately, the development of DIs is oftentimes based on such negative clichés. 60 Our study suggests a prevalent readiness of older adults to use DIs to promote PA—above all in physically active older adults. In turn, there is a need for age-appropriate and tailored interventions to overcome usage barriers and benefit from facilitators. When the design of DIs addresses the needs of older adults, engagement increases. 35 Thus, it is crucial to understand how older adults perceive and use technology in order to meet their needs and to enhance the adoption of new technology among them. 61 The establishment of effective technologies for older adults demands their general acceptance, prioritization of their preferences and wishes, and suitable prerequisites for its adoption.61,62 Future technology creators should therefore be educated to attend to the specific needs of older adults. 62 Promising development processes are participatory approaches, such as co-creation or user involvement, in which the target population is included throughout the process and, at best, shares decision-making with professionals and researchers.63,64 Consequently, feedback from potential users (i.e. older adults) is actively incorporated into the design, engagement, and delivery strategies.
Our study revealed that older adults are interested in additional health-related fields (i.e. memory training, nutrition, psychological wellbeing) within DIs to promote PA. Therefore, future developers should consider creating more holistic DIs targeting several lifestyle behaviors. Synergetic effects may result in case of combination. 65 After having designed age-appropriate DIs, future research needs to evaluate their effectiveness and implementation in the long term, for instance, through hybrid trials. 66
Special attention must be paid to rigorous and concise reporting about the development process and content of DIs to enable reproducibility. Likewise, potentially differing needs toward technology in subgroups among older adults remain to be further determined. Evidence shows that they vary by sociodemographic and socioeconomic factors.37,54,67 Furthermore, technology usage seems to differ in older adults depending on their health status. 68 As a result, older adults with chronic conditions might require different forms of DIs to promote PA.
Conclusion
Community-dwelling older adults may be willing to use DIs to promote PA in the long term, but they have particular needs and requirements in terms of design, technological realization, delivery mode, support, and individualization/personalization that were identified in this study. Besides, our respondents showed high interest in DIs that combine PA with complementing health-related content, for instance, memory training, nutrition, and/or psychological wellbeing. Such DIs may represent a more holistic approach toward digital health and health promotion. Our findings can inform future developments of DIs to promote PA specifically tailored to older adults. However, caution is warranted when interpreting our findings as our sample exhibited high PA and education levels.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076231203785 - Supplemental material for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study
Supplemental material, sj-pdf-1-dhj-10.1177_20552076231203785 for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study by Manuel Weber, Kai-Uwe Schmitt, Anja Frei, Milo A Puhan and Anja M Raab in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076231203785 - Supplemental material for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study
Supplemental material, sj-pdf-2-dhj-10.1177_20552076231203785 for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study by Manuel Weber, Kai-Uwe Schmitt, Anja Frei, Milo A Puhan and Anja M Raab in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076231203785 - Supplemental material for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study
Supplemental material, sj-pdf-3-dhj-10.1177_20552076231203785 for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study by Manuel Weber, Kai-Uwe Schmitt, Anja Frei, Milo A Puhan and Anja M Raab in DIGITAL HEALTH
Supplemental Material
sj-pdf-4-dhj-10.1177_20552076231203785 - Supplemental material for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study
Supplemental material, sj-pdf-4-dhj-10.1177_20552076231203785 for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study by Manuel Weber, Kai-Uwe Schmitt, Anja Frei, Milo A Puhan and Anja M Raab in DIGITAL HEALTH
Supplemental Material
sj-pdf-5-dhj-10.1177_20552076231203785 - Supplemental material for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study
Supplemental material, sj-pdf-5-dhj-10.1177_20552076231203785 for Needs assessment in community-dwelling older adults toward digital interventions to promote physical activity: Cross-sectional survey study by Manuel Weber, Kai-Uwe Schmitt, Anja Frei, Milo A Puhan and Anja M Raab in DIGITAL HEALTH
Footnotes
Acknowledgements
We warmly thank all older adults and research associates who participated in the pretest of our survey, and all institutions, organizations, and associations that supported us in the recruitment of respondents.
Contributorship
MW, KUS, AF, MAP, and AMR contributed to conceptualization; MW to data curation; MW and AMR to formal analysis and investigation; MW, KUS, AF, and AMR to methodology and project administration; MW and AF to resources; AMR to supervision; MW to visualization and writing—original draft; and MW, KUS, AF, MAP, and AMR to writing—review & editing. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was submitted to the responsible ethics committee of the Canton of Bern, the study does not fall under the Swiss Human Research Act (BASEC-Nr. Req-2021-00945). Hence, the study was not identified as human subjects research. The survey was anonymous and informed consent was obtained from all those who agreed to complete the survey by clicking the corresponding button on the introductory page.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AMR.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.