
Abstract
Objective
A rise in non-communicable diseases, driven by poor lifestyle behaviors, demands a shift from conventional, reactive, and episodic care to next-gen, proactive, and real-time lifestyle management. Digital health technologies (DHTs) and digital health interventions (DHIs) are poised to shepherd this transformation. Given the proliferation of digital health applications, a scoping review was conducted to map the DHTs and DHIs targeting lifestyle behavior change in Singapore.
Methods
A systematic search of PubMed, Scopus, and clinical trial registries and a manual search of gray literature and mobile app stores were conducted to identify patient-facing IoT (internet of things) technologies (wearables, apps, bots, websites) that target physical activity, diet, tobacco/alcohol use, sleep quality, and/or mindfulness in Singapore from 2013 to 2023.
Results
Forty-six DHTs and thirty-five DHIs were identified. Apps were the most common while websites and bots were the least common. Most DHTs and DHIs played monitoring or preventative behavior change functions. Most applications targeted multiple behaviors, with physical activity being the most common and tobacco/alcohol use being the least common. Behavioral change strategies included feedback and monitoring (80%), goals and planning (70%), associations (62%), personalization (59%), gamification (54%), rewards (33%), human coaching (30%), and just-in-time adaptations (4%).
Conclusion
This review identified gaps in digital health applications that address addictive behaviors and the elderly. Future efforts should prioritize adaptive, personalized technologies based on user-centric designs and robust behavioral frameworks to enhance long-term behavioral change. Insights from Singapore's experience can guide the global development of more effective health-improving digital applications.
Introduction
A rise in chronic illnesses and non-communicable diseases (NCDs), such as heart disease, diabetes, and obesity, place considerable strain on healthcare systems worldwide. Globally, these conditions account for 74% of fatalities. 1 Poor lifestyle factors, ranging from sedentary behavior to unhealthy dietary choice, are major contributors to the onset and progression of NCDs.2–4 While the traditional healthcare model has excelled in acute and episodic care, it often falls short in addressing the complexities of lifestyle modifications necessary for tackling NCDs. 5 The inherent challenges lie in transitioning from reactive care to a proactive approach that centers around empowering individuals to adopt healthier lifestyles. This paradigm shift requires continuous monitoring and personalized guidance, which is precisely where digital health applications, such as wearable devices and mobile health apps, can come into play.
Digital health aims to empower individuals and populations to take an active role in managing their health through connectivity and collaboration within adaptable, integrated, and digitally-driven care settings. 6 There is a burgeoning interest in digital health and wellness, as exemplified by the staggering popularity of leading mobile applications such as FitPro, which boasts 4.6 million downloads per month. 7 Evidence suggests that digital health technologies (DHTs) and digital health interventions (DHIs) can effectively support through components like personalized feedback and social support.8–10 Particularly, a systematic review by Müller et al. demonstrated the effectiveness of mobile applications, wearable devices, and web-based platforms in promoting healthy lifestyle changes. 11 Similarly, a meta-analysis by Gomez Quiñonez et al. found that tailored interventions delivered via mobile phones and the internet significantly improved physical activity levels. 12 Other reviews have also focused on using digital health to target specific NCDs, such as diabetes, obesity, and hypertension.13–16 Despite the growing body of evidence, the bibliometric and scoping review conducted by Taj and colleagues 17 highlighted that the rapid proliferation of digital health applications necessitates regular and up-to-date landscape assessments. While prior studies have explored the general effectiveness of digital health tools, there remains a lack of comparative analysis of different modalities (e.g. mobile apps, wearable devices, bots, websites) and the behavioral change strategies they employ to enhance health outcomes. Moreover, there has been no prior review focusing on Singapore to our knowledge.
Singapore is a prime setting for examining the intersection of digital health applications and lifestyle behavior change. As a highly urbanized and technologically advanced nation, it has prioritized digital health innovations to improve population health outcomes. The nationwide government-led initiatives such as Smart Nation, 18 National Step Challenges,19–23 and Healthier SG 24 reflect a strong commitment to leveraging technology in healthcare. Furthermore, Singapore's unique healthcare ecosystem, renowned for its blend of public and private healthcare providers, strong focus on preventive health, cutting-edge research and innovation, strategic public health policies, and high digital penetration rate stand out as both robust and exemplary.25–29 Additionally, Singapore prioritizes having a progressive regulatory environment30–33 to foster safe and effective adoption of digital health solutions34,35 in the nation. NCDs account for approximately 80% of Singapore's disease burden. 21 Coupled with an aging population and increasing healthcare costs, the need to leverage digital health solutions to promote healthier lifestyle behaviors has never been more pressing.36–40 These attributes collectively position Singapore as a quintessential case study to explore the convergence of digital health applications and lifestyle behavior change that can be optimized for diverse populations, offering valuable insights for research and practice.
This review has three primary objectives: first, to catalog the range of DHTs and DHIs targeting lifestyle behavior change within the Singaporean context; second, to elucidate the behavioral change strategies underpinning these interventions; and third, to critically appraise the landscape to identify gaps and implications for future practice. By thoroughly examining this landscape, we aspire to inform researchers and technology developers about current digital health tools and guide the development of future digital health applications that enable healthy lifestyle behavior changes and combat NCDs.
Methodology
Definitions and eligibility criteria
This study was designed as a scoping review following the Preferred Items for Systematic Reviews and Meta-Analysis guidelines extension for Scoping Reviews (PRISMA-ScR) 41 (see PRISMA checklist in Supplemental materials). A scoping review of DHTs and DHIs that target lifestyle behavior change in Singapore was conducted. A scoping review was chosen over a systematic review for two reasons. First, the goal was to conduct a scan of the current climate, which is inherently broad, making a systematic approach impractical due to the vast number of studies. A systematic review requires a narrower scope and a more focused research question, which would limit comprehensive insights and make it difficult to capture the full landscape. Second, given the rapid evolution of technological advancements, a full systematic review would take too long, risking outdated findings by the time it is completed. We scoped our study to focus on patient facing IoT (internet of things) technologies only. This includes wearables, mobile apps, bots, and websites that are internet and/or Bluetooth enabled. Wearables can include smart trackers, smart watches, smart rings, or smart bracelets. Mobile health apps are defined as software programs on mobile devices that process health-related data on or for their users. A bot is any software program that performs health-related automated tasks and/or repetitive functions without human intervention over a network. A website is a set of webpages on the internet published by a single entity about a particular topic, in this case, regarding health and/or lifestyle. For this study, we scoped lifestyle behaviors to include physical activity, diet, tobacco/alcohol use, sleep quality (which relates to sleep efficiency, sleep latency, sleep disturbances, sleep time, and/or wake after sleep onset), and mindfulness (refers to self-focused attention and awareness of one's current internal states and surroundings). According to the World Health Organization (WHO), 42 DHIs are interventions delivered via digital technologies to improve health. According to the U.S. Food and Drug Administration (2022), DHTs are systems that use computing platforms, connectivity, software, and/or sensors for healthcare and related uses. 43 In the literature, the terms DHT and DHI are often used interchangeably. For the purpose of this study, we refer to DHIs when referencing published research studies and clinical trials while we use DHTs to refer to gray literature. The geographical focus of this study was on Singapore, with an emphasis to capture the current landscape. Published studies and clinical trials were included if they were conducted in Singapore and focused on DHIs that were currently on the market in Singapore. Studies were included if they focused on the link between DHIs and the resultant lifestyle behavior change. DHTs identified from gray literature were included if they were widely cited or used in Singapore. The search was limited to the last 10 years (2013–2023) due to the recency of using digital health innovations for lifestyle behavior change and the constantly evolving nature of this field. The eligibility criteria are summarized in Table 1. This scoping review is not registered.
Inclusion/exclusion criteria.

IoT: internet of things; DHI: digital health intervention; DHT: digital health technology.
Information sources
Two separate search strategies were used. First, a systematic search of clinical trial registries and peer-reviewed published literature in Google Scholar and PubMed was conducted to identify studies and information sources reporting on DHIs and programs targeting lifestyle behavior modification in Singapore. Other systematic and scoping reviews were excluded but their included studies were individually scanned and included in our study if eligible. In cases where a published study and a clinical trial record were identified for the same DHI, only the published study was included to prevent duplication and because the published study would have the most updated information about the DHI.
Second, as substantial information about technologies used locally in Singapore was expected to be available in gray literature and other information sources, an open-ended search was performed. Google web search was used to identify technical reports, guidance from local government health and digital agencies, government press releases, reports from industry players and online news media describing any aspect of DHTs for lifestyle behavior modification in Singapore. In addition, app stores were screened for relevant mobile health apps. Due to the large number of mobile health apps used in Singapore, only those listed in the top 100 apps in the health, fitness, and/or medical categories on the Apple App Store and Google Play Store were screened for eligibility. The “Top Apps” lists for the “Health & Fitness” category and the “Medical” category are displayed on both app stores. These apps are automatically chosen by the app stores based on various factors like high user engagement, positive user feedback, and consistent app download numbers. We limited our search to the top 100 apps in each category—similar to the methodology employed by other studies44,45—which was deemed sufficient since users often limit their search to the first 10–20 apps. The app store search was conducted in Singapore. The most recent gray literature search was conducted on January 30, 2024.
Search
The final search strategy for PubMed and Google Scholar is presented below (see Table 2). Similar keywords, search terms, and filters were used for the search in clinical trial registries. Google Scholar only allowed basic Boolean operators in search strings and limited the search to 256 characters. As recommended by Haddaway et al., 46 only the first 300 searches were included from Google Scholar in our scoping review due to the limitless number of hits that the search retrieved.
Search strings developed for the scoping review.

Selection of sources of evidence
All studies from the database search of PubMed, Google Scholar, and clinical trial registries were pooled into EndNote and duplicates were removed. This pool of studies was imported into Rayyan for a final round of duplication removal and title and abstract screening. Two reviewers screened the titles and abstracts of all studies and any conflicts were resolved by consensus and discussion with the whole team (four reviewers in total). The shortlisted pool of studies was imported into Covidence for full text screening. Two reviewers screened the full texts of all studies and any conflicts were resolved by consensus and discussion with the whole team. Articles were screened based on the inclusion and exclusion criteria; whenever there were uncertainties or disagreement regarding the criteria, the whole team would come to a consensus through discussion and update the eligibility criteria accordingly.
Three reviewers conducted the open-ended gray literature search using Google web search, Apple App Store, and Google Play Store and imported records that fit the eligibility criteria into Google Sheets. The fourth reviewer conducted an in-depth analysis of all the records and screened them based on the eligibility criteria. Any disagreements or ambiguities were resolved through discussion and consensus with the whole team.
Data charting process
Two data charting forms were developed for (i) literature from databases and clinical trial registries (DHIs) and (ii) gray literature (DHTs) since the variables to extract would differ. This was designed by one reviewer, in discussion with the other three reviewers, based on our research questions. An initial calibration exercise was conducted to pilot the data charts. Each of the four reviewers was assigned one DHI and one DHT to extract data on. The extracted data was reviewed by a second reviewer for quality control. Disagreements, ambiguities, and suggestions were discussed, and the data charts were modified accordingly. For the full data charting process, data from each eligible study was charted by one reviewer and then reviewed by a second reviewer for quality control. Google Sheets was used for data charting. Any conflicts or uncertainties were discussed with the whole team to come to a consensus. Throughout the data charting process, the data charts were continuously updated in an iterative manner. For instance, certain fields were condensed, expanded, or re-categorized. A major change to the data charts occurred in the behavior change strategies section. A Behavior Change Taxonomy (v1) was used to categorize the behavior change strategies. 47 Initial data charts included one free-text section to extract any behavior change strategies employed in the DHIs and DHTs but this was modified to a check-box format to indicate if a certain strategy was employed (gamification, rewards, personalization, goals and planning, human coaching, associations, feedback and monitoring, just-in-time adaptive interventions (JITAIs)) along with a free-text section to elaborate on the strategies if needed.
Data items
In the DHI data chart, we extracted data on article characteristics (e.g. title, author, year), study overview (e.g. design, population, description, outcomes), targeted lifestyle behavior, behavioral change (e.g. strategies, frameworks), technology used (e.g. modality, functionality), and other relevant discussion points (e.g. patient experience, effectiveness of behavioral change).
In the DHT data chart, we extracted data on DHT overview (e.g. name, description, cost), targeted lifestyle behavior, behavioral change (e.g. strategies, frameworks), and technology used (e.g. modality, functionality, and iOS and Android integration).
Targeted lifestyle behavior could refer to physical activity, diet, sleep, mindfulness, smoking, and/or alcohol use. The section on behavioral change explored strategies and frameworks employed by the DHIs/DHTs to elicit healthy lifestyle behaviors. The behavioral change strategies that were explored were restricted to gamification, rewards, personalization, goals and planning, human coaching, associations, feedback and monitoring, and JITAIs based on established taxonomies and since the literature indicated they are the most common and comprehensive behavioral change strategies. 47 JITAIs are defined to have three key features: (1) the intervention aims to provide real-time behavioral support and direct correspondence when the user is at risk of engaging in a negative health behavior or has an opportunity to engage in a positive behavior that is in line with their health goals, (2) the content or timing of the support is adapted to input collected by the system, and (3) behavioral support is triggered by the system. 48 Behavioral change frameworks referred to the underlying theories and/or models about human behavior that the DHIs were developed, designed, and based on. Information about the modality and functionality of the technologies in the DHIs and DHTs were extracted. Technology modality included wearables, apps, websites, and bots. As a caveat, DHIs and DHTs were categorized as bots only if explicitly mentioned as bots in the literature. Technology functionality was assessed based on a functional classification framework. We adopted the 2022 National Institute for Health and Care Excellence Evidence Standards Framework for Digital Health Technologies 49 due to its relevance and applicability to the Singapore context. We adapted the framework to suit our research questions and study scope. The modified framework stratifies DHIs and DHTs into two tiers: (1) simple functionality and (2) complex functionality. Tier 1 includes three categories: inform, monitor, and communicate. Tier 2 includes one category: preventative behavior change. Table 3 presents the description and examples of each category.
Adapted functional classification framework.

DHI: digital health intervention; DHT: digital health technology.
Synthesis of results
Data on targeted lifestyle behavior, behavioral change strategies and frameworks, and technology used in the DHIs and DHTs were analyzed via descriptive analysis and cross tabulation. These data are presented below in a narrative format and through tables and graphs.
Results
Our comprehensive literature search identified a total of 1233 records across multiple sources: PubMed (n = 553), Google Scholar (n = 300), ClinicalTrials.gov (n = 379), Health Sciences Authority of Singapore registry (n = 0), and through manual hand search (n = 1). Post the removal of 54 duplicates using Endnote and Rayyan, 1179 records remained for the abstract and title screening phase. The screening process led to the exclusion of 1061 records by human reviewers due to irrelevance, leaving 118 reports for full-text retrieval and eligibility assessment. Of these, 82 reports were excluded for various reasons: duplicates (n = 14), incorrect technology used in DHTs/DHIs (n = 18), irrelevant outcomes (i.e. not related to lifestyle behavior) (n = 22), wrong geography (i.e. not applicable to Singapore) (n = 15), and emerging/upcoming technologies not yet available on the Singapore market (n = 13). In parallel, an additional search of gray literature and other information sources identified 105 records, including website searches (n = 100) and hand searches (n = 5). All records were retrieved and assessed for eligibility. Of these, 59 reports were excluded due to the following reasons: duplicates (n = 9), irrelevant outcomes (n = 47), wrong geography (n = 2), and wrong technology used in DHTs/DHIs (n = 1). Figure 1 presents the PRISMA flow diagram for the final selection of 36 studies and 46 gray literature sources used for data extraction.

PRISMA flow diagram of the selection process.
Characteristics of individual sources of evidence
The characteristics of the 36 included studies19–23,50–80 and 46 gray literature sources are detailed in Tables 5 and 6 (see Supplemental materials). It is important to note that both Finkelstein et al.79,80 studies draw from the same study and sample, with the 2015 study focusing on baseline characteristics and the 2016 study focusing on intervention effectiveness. To avoid duplication in result analysis, we considered there to be 35 DHIs instead of 36 DHIs. Among the 35 studies from Table 5 (Supplemental materials), the majority were designed as randomized controlled trials (RCTs) (n = 17), while others employed quasi-experimental (n = 5), qualitative (n = 3), feasibility (n = 3), mixed methods (n = 2), pre-post (n = 1), exploratory (n = 1), longitudinal (n = 1), cohort (n = 1), and unspecified (n = 1) study designs. Target populations were diverse, encompassing the general population (n = 18), patients diagnosed with diabetes (n = 9), individuals with overweight or obesity (n = 2), those with comorbidities (n = 3), patients with non-alcoholic fatty liver disease (n = 1), populations at risk for NCDs (n = 1), and children (n = 1). Out of the 35 DHIs, only three studies captured elderly populations (defined as 65 years or older).
Technological landscape
Technology modality
Among the 46 DHTs, 34 were app-based (74%), eight were wearable-based (17%), one was a website (2%), and three used a combination of technology modalities (7%). All three of the combination DHTs used a dual approach, with two of them including app and bot components while one included app and website components. The most common DHT modality was app-based. Among the DHTs with app components, 30 were compatible with iOS and Android while seven were only compatible with iOS (Figure 2).
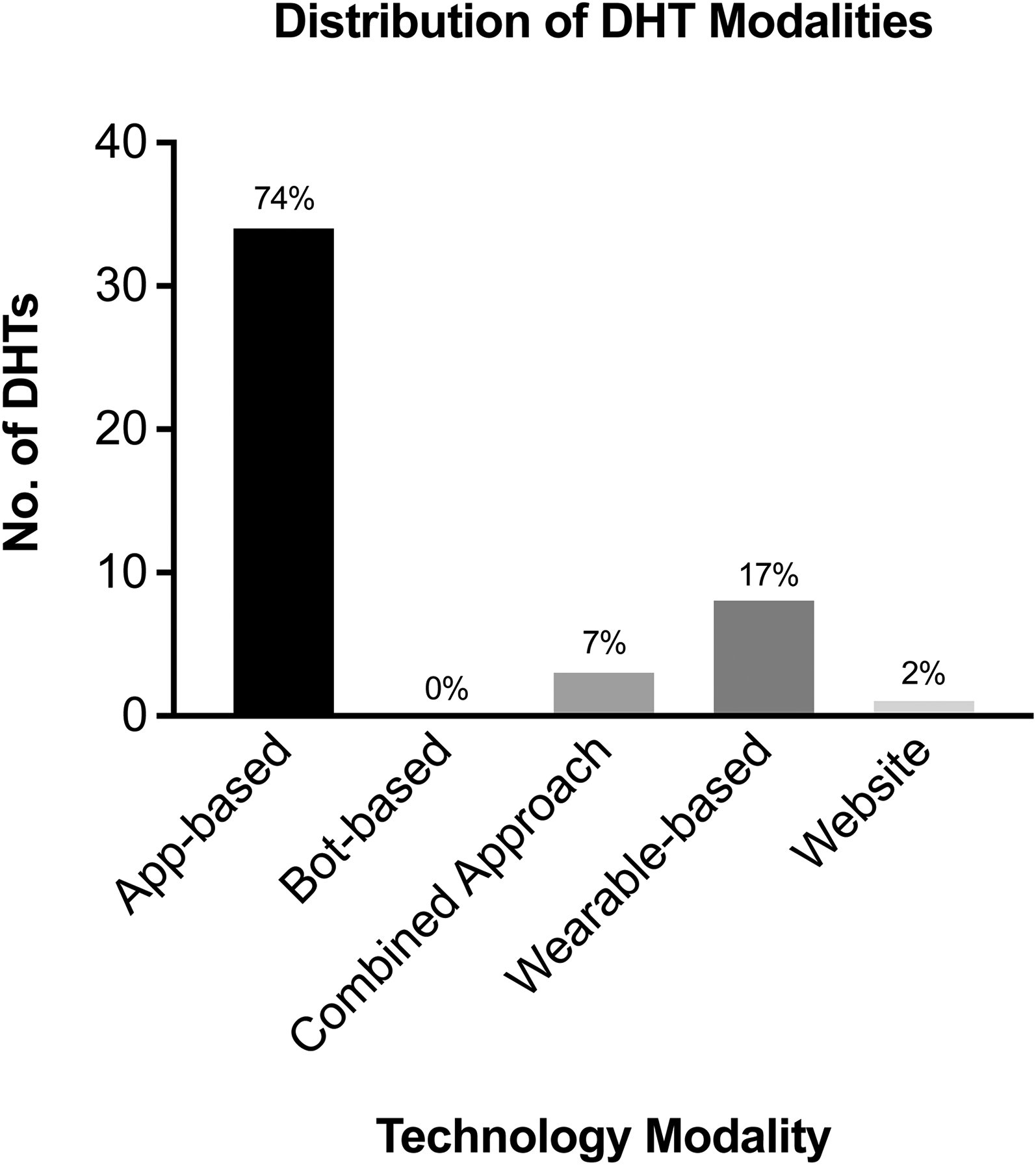
Distribution of digital health technology modalities.
Among the 35 DHIs, 16 were app-based (46%), three were wearable-based (9%), two were bot-based (6%), one was a website (3%), and 13 used a combination of technology modalities (37%). Among the combination interventions, the most common modality included app and wearable components, with 12 of them using an app and a wearable and one of them using an app, wearable, and website. The most common DHI modality was also app-based. Websites and bots were the least common across DHTs and DHIs (Figure 3).

Distribution of digital health intervention modalities.
Technology functionality
With regard to DHT functionality, four DHTs played an “inform” role (9%), 28 played a “monitor” role (61%), 0 played a “communicate” role (0%), and 14 played a “preventative behavior change” role (30%). An example of DHTs in the “inform” category is Mindline.sg which is a mental health website that provides resources, articles, and information on mental health support services. Examples of the “monitor” category include smart watches such as the Fitbit Watch. The “preventative behavior change” group included DHTs such as Healthy365. Healthy 365 is a mobile app by Singapore's Health Promotion Board that tracks physical activity, diet, and health metrics while offering rewards and wellness programs. It integrates with fitness trackers and provides personalized health tips and reminders to promote overall well-being (Figure 4).

Distribution of digital health technology functionality roles.
Among the DHIs, 2 played an “inform” role (6%), 2 played a “monitor” role (6%), 1 played a “communicate” role (3%), and 30 played a “preventative behavior change” role (86%). An example of a DHI in the “inform” category was Precilla—a Facebook Messenger bot that provides educational resources on healthy living. 76 An example of a DHI in the “monitor” category was Goh et al.—an exploratory study on the short-term trajectories of a caloric-monitoring mobile health app. 64 The “communicate” category included an RCT on the effectiveness of Acceset—a digital mental health peer support website that facilitates exchange of letters to allow users to share experiences and advice. 53 A unique use case of a “preventative behavior change” DHI is Castro et al. which covers the development of LvL UP—a smartphone-based and conversational agent-delivered holistic lifestyle intervention built around three pillars: Move More (physical activity), Eat Well (nutrition), and Stress Less (emotional well-being). 67 Coaching sessions between users and the conversational agent are text-based, motivational interview-inspired dialogues. The app features the LvL Up Shield to visualize progress, with tasks including psychoeducational coaching sessions, life hacks, and tools like breathing exercises and journaling. Additionally, LvL Up uses storytelling through animated videos for health education (Figure 5).

Distribution of digital health intervention functionality roles.
One interesting thing to note is the functionality of a single DHT or DHI can be significantly enhanced when integrated with other behavioral change strategies. This integration can transform a DHT or DHI from merely informing, monitoring, or communicating to actively facilitating preventive behavior change. This “tier jump” was exemplified by Finkelstein et al., 80 which demonstrates that Fitbits in combination with cash incentives or charitable donations lead to increases in physical activity (example of Tier 2: Preventative Behavior Change DHI) compared to Fitbits alone (example of Tier 1: Monitor DHT) (Figure 6).

Illustration of adapted functional classification framework.
Technology modality and functionality
Cross tabulating technology modality with functionality brought up several noteworthy results (see Table 4). Among all DHTs and DHIs categorized as wearables, 9 out of 11 fell in the “monitor” category, possibly indicating that a wearable is an apt modality to choose when the intended function of a DHT/DHI is to monitor and track lifestyle metrics. Apps seemed to be the most multi-functional as they spanned across functionality tiers (inform, monitor, preventative behavior change) unlike other modalities (e.g. bots and websites which are more restrictive in terms of functionalities). Lastly, all DHTs and DHIs that employed a combination of technology modalities (e.g. app and wearable) were used for eliciting “preventative behavior change,” potentially delineating that DHT/DHI developers should deploy a mix of modalities to achieve multiple higher-order functions.
Cross tabulation of technology functionality and modality.

Lifestyle behaviors
Targeted lifestyle behavior
Out of the 46 DHTs, six targeted physical activity only (13%), two targeted diet only (4%), three targeted sleep only (7%), two targeted mindfulness only (4%), 1 targeted smoking only (2%), and 32 targeted multiple lifestyle behaviors (70%) with a combination of physical activity, diet, sleep, and/or mindfulness being the most common. There were no commonly used DHTs that targeted alcohol use in Singapore (Figure 7).

Distribution of digital health technology by targeted lifestyle behaviors.
Out of the 35 DHIs, 10 targeted physical activity only (29%), one targeted diet only (3%), one targeted sleep only (3%), three targeted mindfulness only (9%), and 20 targeted multiple lifestyle behaviors (57%) with the combination of physical activity and diet being the most common. There were no DHIs that met our inclusion criteria that targeted smoking or alcohol use in Singapore (Figure 8).

Distribution of digital health intervention by targeted lifestyle behaviors.
Across DHTs and DHIs, the only included application that targeted smoking was QuitNow!—a smoking cessation app that focuses on tracking progress post-quitting, offering positive reinforcement through achievements, reminders, and visual stats on number of cigarettes avoided, number of days since last cigarette, health benefits regained, and money saved (see Table 6 in the Supplemental materials). Unique features include a community-based chat for social support, a QuitNow! bot for answering FAQs, and guidance from WHO archives, making it a comprehensive tool that provides tangible insights on progress.
Behavioral change
Behavioral change strategies
Out of the 81 DHTs and DHIs, 80% used feedback and monitoring, 70% had some form of goals and planning, 62% used associations (i.e. nudges), 59% employed a multi-component strategy to achieve personalization (feedback and monitoring, goals and planning, and associations), 54% used gamification, 33% used rewards, 30% incorporated human coaching, and 4% were JITAIs. Feedback and monitoring generally took the shape of graphs, dashboards, progress rings, and/or healthy living scores. Included studies showed that users preferred visual representations of progress and linking the progress to the end-goals (e.g. displaying the current steps achieved and the ultimate step goal). For instance, the Ōura ring is a DHT that can measure over 20 biometrics from a user's finger and it visually displays them on a dashboard with real-time insights into sleep patterns, stress triggers, and heart rate variability. The types of gamification strategies included team-based challenges, quests, community and/or corporate activities, leaderboards, quizzes for friends to compete on, and the sharing of statistics on social media. For example, Pokémon Go employs gamification by blending physical activity with virtual gameplay, encouraging players to walk and explore real-world locations to capture Pokémon. Another unique use case in Singapore is Habbie: Step Tracker & Pet—an app that combines step tracking with virtual pet care, motivating users to stay active by caring for their virtual pets. Rewards took the form of monetary rewards, such as financial payments and vouchers, or non-monetary rewards, such as the achievement of badges, points, and medals. Finkelstein et al.50,57,80 demonstrated that many design features, including type, frequency, and duration of rewards (e.g. group-based incentives, charitable incentives, etc.), are likely to influence the effectiveness of behavioral change. Sweatcoin is an app that awards users with bitcoins when they achieve certain step counts. Human coaching seemed to be an emerging behavioral change strategy, usually delivered via in-person face to face sessions or remotely with digital health coaches. Novify is an app built by NOVI Health—a startup in Singapore—which enables one-on-one digital health coaching to set goals and devise personalized plans on diet and physical activity. JITAIs were very rare potentially due to their recency, with only one DHI employing just-in-time (JIT) features. EMPOWER is an adaptive platform that has artificial intelligence (AI)-powered personalized associations, Bingo games, health diaries, motivational interviewing, and health coaching in order to tackle chronic diseases. The use of AI associations instead of rule-based associations allows the platform to be predictive, customized, and real-time instead of reactive (Figure 9).

Distribution of deployed behavioral change strategies.
Behavioral change frameworks
In total, 43% of DHIs employed a behavioral change theory, framework, or model to guide the design and development of the intervention. The most commonly used theoretical underpinnings were the Behavior Change Wheel—which identifies policy enablers (e.g. guidelines, legislation, etc.) and intervention functions (e.g. education, persuasion, etc.) that can affect sources of behavior (capability, opportunity, motivation)—and the self-determination theory—which posits that autonomy, competence, and relatedness (all intrinsic factors) are required for sustainable behavior change. Other reported frameworks included the social cognitive theory, health belief model, and social sharing of emotions framework.
Discussion
Current landscape
Singapore has a plethora of DHTs and DHIs that target lifestyle behavior. This scoping review identified 46 DHTs and 35 DHIs that utilize patient-facing IoT technologies and target physical activity, diet, tobacco/alcohol use, sleep quality, and/or mindfulness. The most utilized technology modality was app-based whereas websites and bots were the least utilized modalities. These differences may be attributed to several key advantages offered by apps. Their customizable nature enables the integration of diverse behavioral change strategies—such as real-time tracking, push notifications, associations, and gamification. Moreover, apps are highly accessible, requiring only a smartphone for download while retaining user history, and their multi-functionality allows them to address a broad range of lifestyle behaviors. In contrast, websites and chatbots are less customizable, often fail to retain user history consistently, and may struggle to target complex behaviors such as sleep effectively. Moreover, websites typically facilitate one-way information flow—from the DHT/DHI to the user—while chatbots have faced skepticism over AI accuracy. Similarly, wearables generally incur higher costs than apps and require ongoing commitment from users to wear and maintain the devices.17,81 In terms of functionality, the majority of DHTs played monitoring roles while the majority of DHIs played preventative behavior change roles. DHIs may be more geared toward preventative behavior change because they are generally more complex programs with stronger theoretical behavioral foundations and involve multiple DHTs, such as an app and a wearable, thereby unlocking multiple functionalities. The least common functionality was “communicate,” demonstrating that DHTs and DHIs with a sole focus on social and peer support channels are rare. Since our inclusion criteria focused solely on patient-facing technologies, provider-facing technologies such as teleconsultations which are more common “communicate” tools were not captured in this review. With regard to targeted lifestyle behavior, most DHTs and DHIs targeted multiple behaviors, with physical activity being the most common and tobacco/alcohol use being the least common. A variety of behavioral change strategies were used in DHTs and DHIs and behavioral change frameworks were employed in 43% of DHIs.
Gaps in the landscape
Several gaps exist in the DHT and DHI landscape in Singapore. First, only a few of the included DHIs focused on the elderly—who are defined as 65 years or older. This gap is mirrored in other countries as well; for example, a global scoping review on digital health promotion and prevention found that only 9% of studies targeted older adults. 8 The elderly population has been reported to be systematically excluded from health-risk behavioral clinical trials. 82 However, this is a critical gap that developers need to address. Since the elderly have the highest burden of chronic conditions, DHTs and DHIs can play a big role in facilitating healthier lifestyles for this age group. More research should be conducted on how to tailor DHTs and DHIs to be purpose-fit for the elderly and effort should be put into providing continuous technical and social support to increase technology use among the elderly. 83 Some attempts have been made in Singapore; for example, Wu et al. 84 conducted a pilot study of a community-based e-health program to promote self-management of chronic conditions for older adults but to our knowledge, this has not been translated from a controlled experiment into real-world implementation yet.
Second, our review indicated that very few DHTs and DHIs in Singapore target tobacco and/or alcohol use with the current digital health landscape predominantly emphasizing physical activity and nutrition. Stark et al. 8 corroborate these findings, with 40.5% of their studies addressing physical activity while 22.5% concentrated on nutrition. Another review conducted in Europe, Canada, and the UK similarly highlighted physical activity as a key behavioral outcome measure. 85 The prevalent focus on physical activity as the target behavior in DHTs and DHIs may be attributed to the fact that it is easily quantifiable and is measurable by many existing devices—such as mobile phones or pedometers—that oftentimes do not require additional input from users. DHTs and DHIs targeting smoking and alcohol consumption are relatively less common, possibly because they are not effective at combating these behaviors as O’Logbon et al. 86 indicate. Unlike promoting healthy behaviors like physical activity and healthy diet, reducing smoking and alcohol consumption require reducing addictive behaviors. This involves more habitual, psychological, and physiological dependencies, making behavioral change more complex. Overcoming addiction often requires long-term, intense behavioral reinforcement and may necessitate human intervention (e.g. counseling or pharmacological intervention), making standalone DHTs/DHIs ineffective.
Some evidence suggests that highly personalized interventions and online peer-based support channels (the lack of these “communicate” channels is another gap identified in the Singapore landscape based on our review) could be beneficial for dissuading addictions. In terms of highly personalized interventions, JITAIs can deliver interventions when and where they are needed. However, JITAIs are rare, and our review identified only one JITAI—the EMPOWER DHI.54,55 Future research and development efforts can be considered to make JITAIs more commonplace in Singapore and abroad. This can be significantly enhanced by leveraging machine learning and AI which can facilitate personalized and dynamic health interventions by analyzing real-time data to provide timely and contextually relevant support to users. For instance, Prasetyo et al. 87 created Foodbot—a goal-oriented JIT healthy eating intervention chatbot that integrates sophisticated algorithms and contextual information to enhance user experience and tailored recommendations.
Features that elicit lifestyle behavior change
As demonstrated earlier by the “tier jump,” behavior change is challenging to achieve without incorporating specific behavioral change strategies into DHTs and DHIs. 52 For example, National Steps Challenge 3 (NSC3), 20 which incorporated activity feedback, gamification, and health points, resulted in larger step counts than in NSC1. 19 Similarly, Finkelstein et al. 80 observed that trackers alone had limited impact on behavioral outcomes but combining them with rewards showed promise. Although most DHIs with behavioral change strategies reported positive short-term outcomes, sustaining long-term behavioral modifications remained a challenge.21,67 While NSC3 20 showed longer user engagement than NSC1, 19 less than a third of users remained active by the end of the intervention, and the effect of cash rewards in Finkelstein et al. 80 diminished beyond 6 months after withdrawal. The process of adopting and maintaining new behaviors in the long-term requires additional strategies. Our review identified two key solutions for this issue: systemic change and fostering intrinsic motivation. Systemic change involves making healthy choices the easier choices by integrating healthy lifestyle options into society, such as enhancing social prescribing practices, increasing chances for incidental exercise, and incorporating healthy lifestyle considerations into urban planning. 21 Intrinsic motivation focuses on internal drivers rather than external rewards. Personalized goals, self-monitoring, and self-reflection can maintain behavior change by enhancing a sense of agency and personal achievement. According to the theory of self-efficacy, if participants feel a sense of achievement and control over their health outcomes, they are more likely to sustain desired habits even after rewards cease.22,63 Strategies like mental contrasting with implementation intentions, where individuals visualize a desired future and a plan to overcome obstacles, further support sustained behavior change. 51
In addition, our findings corroborate that the design and usability of DHTs and DHIs are critical determinants of adoption, sustained engagement, and ultimately, successful behavioral change. Many of the studies discussed key elements for optimizing user experience, including triangulation for developing intervention design, patient experience frameworks, technology modality, contextualization to the local context, UI (user interface)/ UX (user experience), and integration across devices and systems. Triangulation refers to involving multiple stakeholders, co-designing features, and conducting formative evaluations and pilot studies. Acceset's 53 emphasis on community engagement, EMPOWER's54,55 rapid prototyping with user input, and LumiHealth and LvL UP's 67 engagement of public health experts, physicians, and users are examples of triangulation. Several DHIs employed patient experience and usability frameworks to ensure interventions met user needs and achieved desired outcomes; for instance, Kurbo 66 used the RE-AIM framework, LvL UP utilized APEASE criteria, and NSC20,21,23 adopted the EAST framework with features like free wearable trackers that enabled easy tracking, attractive redeemable vouchers, social marketing, and timely associations. When developers design DHTs/DHIs, they should consider how various technology modalities can affect the desired outcomes, especially with regard to behavioral change. Studies, such as LvL UP, demonstrate that adding human support alongside a digital intervention (i.e. a blended approach) can increase behavioral change effectiveness. Interventions like EMPOWER, nBuddy,69–72 iDAT, 64 and Habits GDM 61 have incorporated local food databases and cultural nuances into their design, ensuring interventions resonate with the target population. User experience and interface are critical for user engagement, with features like free text boxes, easy entry methods, simplified logging processes, technical stability, and downloadable reports being essential to prevent user abandonment, as shown by EMPOWER. Visualization of data, coupled with remote monitoring and actionable insights, empowers users to make sense of their data leading to health-improving behaviors, as demonstrated by Novify. Integrating trackers and devices like glucometers with a central app can prevent manual entry and improve remote monitoring. The Healthy 365 app exemplifies successful integration, serving as a central touchpoint for multiple health programs, including the NSC and the “Eat, Drink, Shop Healthy Challenge,” thereby ensuring a streamlined user experience. Incorporating these design features into DHTs/DHIs can improve user adoption and behavior change.
Global relevance
Singapore has proactively addressed health inequalities and the social determinants of health by leveraging its strong health policies and advanced digital infrastructure. A key initiative is the NSC,19–23 which encourages healthier lifestyles through the widespread adoption of free smart trackers compatible with most smartphones. Enabled by high internet accessibility and smartphone penetration, the program is further supported by Singapore's emphasis on preventive care and community engagement. By integrating reward strategies and making health-promoting activities easily accessible, this national initiative showcases Singapore's effort to improve digital inclusion in the backdrop of the nation's robust digital and healthcare infrastructure. However, the effectiveness and scalability of such initiatives hinge on the dual pillars of well-developed infrastructure and an enabling policy environment. While Singapore's model may be adaptable to other high-income nations with advanced technological ecosystems and proactive health governance, such as Australia,88,89 where comprehensive digital health policies, widespread internet access, and government-led preventive health programs converge, its applicability to low- and middle-income countries (LMICs) is far more constrained. Many LMICs contend with systemic barriers, including unreliable electricity, inconsistent internet connectivity, limited smartphone penetration, low digital literacy, and fragmented healthcare systems, all of which undermine the scalability of DHIs. Once basic infrastructure is in place, there are more advanced technical considerations to account for in establishing an eHealth ecosystem, 90 such as optimizing interoperability between DHTs/DHIs and across electronic health record systems. 91 Yet infrastructure alone is insufficient; a nation's policy landscape is equally instrumental in shaping the success of such programs. Policies to protect data security and privacy and mechanisms to ensure these policies trickle down to the ground are required to enable adoption of DHTs and DHIs by the public. 91 In addition, digital literacy is a critical factor that can influence the initiation and sustainability of digital technology adoption. Policies that advocate for training individuals in digital skills can facilitate the efficient and effective use of DHTs/DHIs. 92 Singapore's achievements stem from a confluence of strong governmental leadership, centralized health strategies, and sustained public investment in digital health—factors that may be absent in settings with weaker policy coordination and resource constraints. Thus, for LMICs to effectively implement similar initiatives, a dual approach is imperative: significant investment in foundational infrastructure alongside the development of cohesive, forward-thinking policies that foster equitable access to digital health innovations.
These disparities directly influence the generalizability of our findings. Our findings are less generalizable to LMICs with less developed digital infrastructure, low levels of internet penetration, low digital literacy, and limited government digital services. Conversely, countries such as Australia 93 and South Korea 94 are renowned for their fast internet speeds, extensive fiber-optic networks, and government initiatives promoting internet accessibility, affordability, and digital literacy to narrow the digital divide within these nations.95–97 Insights from examining Singapore's digital health landscape may be applicable to countries like Australia and South Korea.
Limitations
This study could not capture the entire DHT and DHI market in Singapore due to its exhaustive scope. Specifically, we did not include mobile health apps published outside the Apple App Store and Google Play Store. By limiting our search to only two databases, there may have been potential for publication bias, where certain types of studies may have been underrepresented. Instead, this study focused on capturing the most popular and widespread DHTs and DHIs in Singapore. Additionally, gray literature often lacks a standardized reporting framework, posing challenges for systematic data extraction. To address this, the study team developed and iteratively refined a structured data extraction template to ensure consistency and rigor in identifying and analyzing relevant information. Given that the DHT/DHI landscape evolves rapidly, some relevant reports may have been omitted and certain features and functionalities may be underreported. To mitigate this limitation, we extended our search until January 30, 2024 to capture the most up-to-date developments prior to the finalization of our analysis and evaluation. Finally, we did not assess DHT and DHI effectiveness based on changes in target lifestyle behaviors as our study is not focused on comparing pre- and post-intervention outcomes. Future research should focus on conducting a meta-analysis on the effectiveness of DHTs and DHIs in improving lifestyle behaviors and ultimately, clinical outcomes.
Future directions
Developers, researchers, and policymakers should prioritize scaling and optimizing DHTs and DHIs to bridge critical gaps in the current landscape, particularly for elderly populations and behaviors like tobacco and alcohol use, which remain significantly underrepresented. Given that older adults experience a disproportionate burden of chronic diseases yet face exclusion from digital health applications, it is crucial to design age-inclusive, purpose-fit solutions. This could involve user-friendly interfaces, voice-command features, and integrated social and technical support to enhance adoption and effectiveness. Similarly, the scarcity of effective digital solutions for smoking and alcohol reduction underscores the need for innovative, evidence-based approaches that extend beyond conventional behavior-tracking models. Addiction-related behaviors are deeply rooted in psychological and physiological dependencies, requiring long-term, adaptive reinforcement strategies rather than static interventions. To address this, future DHTs and DHIs should incorporate highly personalized, dynamic support mechanisms, such as JITAIs, which deliver real-time, context-sensitive guidance based on user behavior, environmental cues, and emotional states. Finally, to ensure the long-term efficacy and scalability of digital health applications, a comprehensive meta-analysis on the effectiveness of DHTs and DHIs in driving sustained behavior change and clinical outcomes is warranted.
Conclusion
This scoping review provided a comprehensive overview of DHTs and DHIs targeting lifestyle behavior change in Singapore by categorizing the landscape based on technology modality and functionality, targeted lifestyle behavior, and behavioral change strategies and frameworks. It identified a predominant focus on physical activity and nutrition while interventions targeting tobacco and alcohol use were notably less common, underscoring the need for more targeted interventions to address addictive behaviors effectively. The review also revealed a gap in DHTs and DHIs tailored for the elderly, an important demographic given their high burden of chronic conditions.
From a theoretical perspective, this study contributes to the understanding of how behavioral change strategies and theoretical frameworks are currently applied in DHTs and DHIs. The findings highlight the need for robust behavioral theories to improve engagement, adherence, and long-term lifestyle change. Researchers should focus on optimizing behavioral science integration into DHT/DHI development, with an emphasis on systemic change and intrinsic motivation as key enablers of sustained behavior adoption. Future research should further explore these aspects, particularly through a meta-analysis assessing the effectiveness of DHTs and DHIs in improving lifestyle behaviors and clinical outcomes.
On a practical level, the review provides valuable insights for technology developers and policymakers seeking to design more effective digital health solutions. Developers should keep in mind elements for optimizing user experience to elicit behavioral change, including triangulated intervention design, patient experience frameworks, technology modality selection, contextualization to local needs, UI/UX optimization, and seamless integration across devices and systems without compromising privacy. Successful examples from Singapore, such as the NSC and EMPOWER, demonstrate the potential benefits of well-designed user-centric DHTs and DHIs. Future work should focus on building technologies that provide dynamic personalization and transform static, rule-based interventions into adaptive systems capable of providing real-time responses. For policymakers, the review underscores the importance of addressing the social determinants of health to maximize the reach and effectiveness of DHTs and DHIs. While Singapore's landscape may be generalizable to high-income countries with similar digital ecosystems, such as Australia and South Korea, it also offers valuable lessons for LMICs seeking to strengthen their digital health infrastructure.
By addressing these theoretical and practical gaps and leveraging the unique insights from Singapore, policymakers, researchers, and technology developers can enhance the effectiveness of DHTs and DHIs. This will not only promote healthier lifestyles but also contribute to the global fight against NCDs.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076251337032 - Supplemental material for Scoping review of digital health technologies and interventions that target lifestyle behavior change in Singapore
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076251337032 for Scoping review of digital health technologies and interventions that target lifestyle behavior change in Singapore by Nikita Kanumoory Mandyam, Jacqueline Lau, Camille Keck, Elya Chen and Alexander Wenjun Yip in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076251337032 - Supplemental material for Scoping review of digital health technologies and interventions that target lifestyle behavior change in Singapore
Supplemental material, sj-pdf-2-dhj-10.1177_20552076251337032 for Scoping review of digital health technologies and interventions that target lifestyle behavior change in Singapore by Nikita Kanumoory Mandyam, Jacqueline Lau, Camille Keck, Elya Chen and Alexander Wenjun Yip in DIGITAL HEALTH
Supplemental Material
sj-pdf-3-dhj-10.1177_20552076251337032 - Supplemental material for Scoping review of digital health technologies and interventions that target lifestyle behavior change in Singapore
Supplemental material, sj-pdf-3-dhj-10.1177_20552076251337032 for Scoping review of digital health technologies and interventions that target lifestyle behavior change in Singapore by Nikita Kanumoory Mandyam, Jacqueline Lau, Camille Keck, Elya Chen and Alexander Wenjun Yip in DIGITAL HEALTH
Footnotes
Ethical considerations
This article does not contain any studies with human or animal participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The National Medical Research Council, Centre Grant Programme (CG21APR3001).
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.