
Abstract
This paper endeavors to identify the causal effects between the smart city transition and the provision of healthcare services while uncovering potential pathways of influence. This study first constructs a logical analytical framework and posits five hypotheses for examination. Subsequently, leveraging the quasi-natural experiment of the China Smart City Pilot Policy (CSCPP), empirical tests are conducted utilizing a Difference-in-Differences (DD) two-way fixed effects model. The findings suggest that the CSCPP has significantly enhanced the provision of healthcare services. Even after addressing the formidable challenges of endogeneity, sample self-selection, and spatial spillovers, the conclusion remains robust. Mechanism tests indicate that the CSCPP primarily operates through two avenues: augmenting human resources and institutional services. Heterogeneity tests reveal that the efficacy of CSCPP is heightened in cities boasting administrative approval service centers, experiencing diminished financial constraints, and exhibiting elevated healthcare provision levels and situated in the eastern region. The theoretical and empirical analysis of this paper demonstrates that smart city transitions can facilitate the enhancement of healthcare services. The potential contribution of this paper is to enrich the conceptualization of governance frameworks for smart city transition while providing empirical evidence from China.
Introduction
As urban populations continue to grow and aging becomes increasingly severe, cities urgently need to strengthen the provision of healthcare services to meet the growing medical and healthcare needs of residents. Improving urban healthcare services can help improve residents’ quality of life, enhance social welfare, alleviate social conflicts, promote social harmony and stability, and provide support for urban economic development, promoting sustainable urban development. However, the current level of urban medical care is still relatively low, leading to a series of social problems such as increasing doctor–patient conflicts, difficulty seeing a doctor, high medical costs, and a shortage of medical resources. These problems not only affect residents’ health and lives but also impact the social harmony and stability of cities. Therefore, it is urgent to improve the provision of urban healthcare services to better protect the development of cities and the well-being of residents.
Today, the world is in a booming era of digitalization. Haverinen et al. 1 believe that digitalization can have a significant impact on the healthcare sector, and the primary phase is the construction of health information technology infrastructure. Jedamzik 2 and Han et al. 3 assert that the meticulous establishment of health information technology infrastructure has significantly propelled the profound integration of digitization and healthcare services, thereby fundamentally transforming medical practice. Similar viewpoints have been expressed by Zayas-Cabán et al. 4 and Sheikh et al., 5 who contend that harnessing the potential of medical information infrastructure enables swifter and enhanced communication with patients, ultimately enhancing the quality, safety, and effectiveness of healthcare provision. China is presently embarking on a gradual strengthening of its digital infrastructure, propelling the advancement of a smart city transition. According to Mora et al., 6 smart city transition refers to the process of introducing smart city technologies into urban infrastructures to enhance the ability of urban services to meet societal needs in a sustainable manner, thereby improving the quality of urban life. Based on the aforementioned analysis, we have reason to believe that the Chinese smart city transition will impact the provision of urban healthcare services through the reinforcement of digital infrastructure construction.
Therefore, this paper explores the impact of the smart city transition on the provision of healthcare services. There are still three theoretical and practical reasons for choosing this perspective of smart city transition: First, according to the technology acceptance model, the perceived usefulness and ease of use of technology are critical factors that affect users’ acceptance and adoption of technology. The use of digital technologies such as telemedicine, smart wearable devices, and electronic health records can improve the perceived usefulness and ease of use of medical services, thereby improving the provision of urban healthcare services. Second, according to the social determinants of health theory, the impact of social environmental factors on health is considered the fundamental cause of determining people's health and disease, and its core value concept is health equity. Digitalization can provide urban residents with more opportunities to access health information and services, reduce health disparities, promote health equity, and improve the provision of urban healthcare services. Third, in 2016, the Chinese government issued the “Healthy China 2030” planning outline, proposing policy measures to strengthen the construction of primary healthcare service systems, optimize the allocation of medical resources, and promote the construction of medical informationization, providing policy guidance and the basis for the digitalization perspective of this paper.
Has smart city transition enhanced the provision of healthcare services? Existing literature on smart city transition predominantly focuses on qualitative perspectives, exploring the developmental pathways of smart cities,7–9 investigating the factors influencing the level of healthcare services,10–12 and analyzing governance frameworks for smart city transition.13–16 However, there is limited empirical evidence from a quantitative perspective.
This paper aims to construct a theoretical framework for analyzing the relationship between smart city transition and the provision of healthcare services and provide rigorous empirical evidence to fill the research gap. Specifically, this paper first conducts theoretical analysis and proposes several hypotheses to be tested. Then, using the China Smart City Pilot Policy (CSCPP) as a quasi-natural experiment, and based on balanced panel data for 286 Chinese cities from 2000 to 2019, a two-way fixed effect difference-in-differences (DD) model is applied to rigorously identify the causal relationship between smart city transition and the provision of healthcare services.
Using the Chinese context for verification has three advantages. First, China has a large number of smart city pilot projects, with the Ministry of Housing and Urban-Rural Development announcing 290 such projects to date. China's smart city pilot projects exceed the sum of those in Europe, India, and the United States. Therefore, this paper's exploration of the impact of smart city construction has important reference value for other countries. Second, China currently has the largest elderly population in the world, with 264 million people aged 60 and over as of 2020, accounting for 18.7% of the total population. At the same time, China is accelerating its urbanization process, with rural populations migrating to cities, greatly exacerbating the supply–demand imbalance in urban healthcare services. Therefore, this paper's research can provide experiential references for other countries to alleviate the supply–demand imbalance of healthcare services. Third, China's regional economic development is highly uneven, with significant differences in regional cultures and policies and regulations. The promotion and effects of smart city construction vary greatly across different regions, providing rich variation information for identifying the causal relationship between CSCPP and the provision of healthcare services.
To prevent potential biases from different measurement methods, this paper uses two weighting methods—principal component analysis (PCA) and entropy weighting method (EWM)—to measure the provision of urban healthcare services. The basic regression results show that CSCPP, respectively, promotes PCA and EWM by 3.21 and 6.39 percentage points, indicating that smart city transition significantly improves the provision of healthcare services. This result has undergone a series of robustness tests, parallel trend hypotheses, and placebo tests. Mechanism tests suggest that the promotion effect of CSCPP on medical and health service supply is mainly achieved through two channels: increasing human resources and institutional services. Heterogeneity tests show that CSCPP has a better effect in cities with administrative approval service centers, less fiscal pressure, and higher level of medical service supply and in eastern regions.
The potential contributions of this paper lie in enriching the connotations of the governance framework for smart city transition and providing causal identification evidence from China. Specifically, first, while current scholars have focused on investigating case studies of smart city transformation governance in Europe, 16 this paper offers empirical evidence from China in Asia, demonstrating that smart city transformation can promote the provision of medical resources. Second, the current academic discourse has overlooked small-scale city contexts 17 and location-based characteristics. 18 In contrast, this paper incorporates data from smart city transformation pilot policies widely implemented across China on a national scale, encompassing cities of various sizes for empirical testing. Furthermore, the city samples are further divided into two sub-samples: developed cities in the eastern region and less developed cities in the central and western regions, subjecting them to in-depth examination. Third, there is a lack of relevant empirical studies on the experiences of public sector establishment during the smart city transformation process. 19 This paper examines the differences in impact across sub-samples of administrative approval service centers, shedding light on the coordination and cooperation of China's administrative departments during the governance process of smart city transformation, thereby providing partial evidence for this research. Fourth, existing research has overlooked the influence of financial support on smart city transformation. In contrast, this paper examines the differences in impact across sub-samples facing varying fiscal pressures, highlighting the crucial significance of financial funding in the process of smart city transformation. The aforementioned heterogeneity test results in this paper also offer evidence from China in support of the viewpoints put forth by Esposito et al. 20 They advocate for policymakers to adopt a place-based approach in formulating smart city development strategies to ensure these strategies align with the local socio-economic context.
The sections of this paper are as followa: the second section comprises the literature review, while the third section provides a background introduction to the pilot policy of smart cities. The fourth section puts forth theoretical analysis and hypotheses to be tested. Moving on, the fifth section presents the empirical design, encompassing data sources, econometric equations, and variable definitions. The sixth section presents the basic regression analysis and robustness tests. Subsequently, the seventh section demonstrates the parallel trend test. In the eighth section, potential concerns for causal identification are discussed and addressed systematically. The ninth section presents the heterogeneity test. Lastly, the conclusion, policy recommendations, and shortcomings are presented.
Literature review
The inaugural strand of literature resonates most profoundly with the essence of this manuscript. Lyu et al. 21 analyze the relationship between China's digitization construction and the efficiency of public health service supply and ultimately found that China's digitization construction has a significant positive effect on the efficiency of public health service supply. Their main problem is the lack of sufficient attention to potential endogeneity issues, which may lead to serious biases in the results. Building on their research, this paper mainly makes four extensions: (a) constructs a theoretical framework and proposes several theoretical hypotheses for testing, enhancing the theoretical depth of the paper; (b) employs the CSCPP as a quasi-natural experiment for strict causal identification, which can better overcome potential endogeneity issues; and (c) uses propensity score matching (PSM)-DD and spatial DD models to better overcome self-selection and spatial spillover effects; and (d) using city-level data instead of provincial-level data can provide richer sample variation information and provide more micro-level empirical evidence.
The second scholarly work bears relevance to the trajectory of smart city development. Existing research on smart cities, influenced by dimensions of time, space, and other factors, has emphasized various focal points in the construction of smart cities. Komninos et al. 9 put forth the notion that smart cities represent a novel urban paradigm, an overarching phenomenon in contemporary urban development. By automating and innovating urban activities and public utilities, smart cities enhance efficiency, thereby introducing the concept of creating “connected intelligence spaces.” In contrast, Kumar et al. 8 propose the smart city transformation framework, which strives to transform cities into intelligent ones through key areas encompassing planning stages, physical infrastructure, information and communication technology (ICT) infrastructure, and the deployment of intelligent solutions. Mora et al. 7 summarize and reveal five major paths to smart city development: the experimental path, ubiquitous path, corporate path, European path, and holistic path. Additionally, they suggest four distinct choices within the context of smart city construction. Angelidou, 22 considering different strategic choices in smart city spatial planning, categorizes smart city construction strategies into four types: national versus local, new versus existing cities, hard versus soft infrastructure, and economic versus geographical perspectives. In summary, existing relevant studies primarily adopt a holistic and macro perspective, lacking an in-depth examination of specific components. This article addresses the healthcare service dimension within smart city construction, expanding the research on smart city development.
The third cited literature pertains to the factors influencing the level of healthcare services. According to McCullough et al., 11 increasing government expenditure on healthcare and social services, as well as strengthening collaboration between local governments and hospitals, significantly enhances the quality of healthcare services. Moreover, the introduction of private healthcare institutions contributes to the optimal utilization of healthcare resources. Zhou et al. 12 propose that constructing a policy framework based on regional differentiation and spatial clustering, known as “regional governance-classification management,” can further improve the level of healthcare services. Fu et al. 23 argue from the perspective of healthcare facility development that the level of healthcare services is not only associated with the equipment and medical capabilities of hospitals but is also influenced by the geographical location of these institutions. Wang et al. 24 suggest that sharing healthcare services and human resources among healthcare institutions at all levels can generate a significant ripple effect, benefiting high-level healthcare service areas and their surrounding regions. Bombard et al. 10 assert through a literature review that involving patients in service planning, design, and evaluation contributes to the improvement of healthcare service levels, with the degree of patient involvement impacting the effectiveness of enhancement efforts. Existing research primarily focuses on aspects such as economics, policies, and resources, while some researchers have begun recognizing the impact of digitalization on healthcare service levels. However, such studies often explore the digitalization of healthcare services solely from the perspective of the services themselves. This article enriches the existing research by examining the implications of smart city transition in this context.
The fourth referenced literature relates to the governance of smart cities. Lee et al. 25 propose that the governance of smart cities aims to address various urban issues through infrastructure and communication technologies. The ultimate goal is to rectify structural imbalances within cities by effectively redirecting information, creating a better and sustainable urban environment. Ruhlandt 14 defines smart city governance as a process of interactive engagement among different stakeholders with distinct roles and responsibilities. Through the driving and facilitation of technology and data, this governance approach involves a series of policy arrangements and exchanges, ultimately leading to substantial outcomes or procedural transformations for the city. Specifically regarding healthcare, Kamel and Al-Shorbaji 13 believe that the Internet of Things (IoT) can propel smart cities to become healthier urban environments, leveraging IoT technologies to improve the health and well-being of local residents. Sharifi et al. 26 propose that smart cities can provide intelligent infrastructure, fostering collaboration and integrated planning and management. By utilizing smart technologies, these cities can prevent or minimize the impact of sudden public health emergencies. Shi et al. 15 present a governance model for smart cities that combines a top–down and bottom–up approach, using China’s implementation of the health code system and the development of health regulations during the COVID-19 pandemic as an example. This article primarily analyzes the impact of smart cities on the level of healthcare services from both theoretical and empirical perspectives, introducing a fresh angle to the governance of smart cities. In their enlightening work, Mora et al. 16 delve into the governance practices and theoretical framework surrounding the transformation of smart cities. Through a meticulous review of literature and thoughtful case analyses, they present a sophisticated governance framework. This framework serves as a valuable resource, aiding urban managers and policymakers in gaining a deeper grasp of the challenges entailed in the transformation of smart cities and empowering them to respond effectively. Furthermore, the study delves into the theoretical underpinnings of smart city transformation, skillfully intertwining innovative management theories with urban research to enhance our comprehension of smart city governance.
Policy background
The concept of “smart cities” was first born in the United States. In November 2008, IBM released a speech on “Smart Earth: Next Generation Leaders’ Issues” at the Foreign Relations Council, first proposing the concept of “Smart Earth.” In January 2009, President Obama of the United States publicly affirmed IBM's “Smart Earth” concept. In 2009, IBM introduced the concept of smart cities to China and proposed five major themes for the development of smart earth in China: sustainable economic development, competitive enterprises, efficient energy use, environmental protection, and harmonious society.
The concept of smart cities has been a subject of extensive debate within academia, but a unanimous consensus has not been reached. Mora et al. 27 provided a comprehensive review on this matter. In essence, the notion of smart cities is multifaceted, encompassing both future visions and urban development strategies. Its definition has shifted from a purely technology-centric perspective to a more holistic understanding, emphasizing the social, cultural, and environmental dimensions of cities. Furthermore, the definition of smart cities highlights how people drive urban transformation and pursue their aspirations through the use of technology.
Here, we briefly introduce several recent representative definitions: According to Mora et al., 16 smart city transformation is not a static state or product, but rather an urban innovation process that involves a combination of management and policy efforts with technological advancements. It is a sustainable journey aimed at enhancing urban efficiency, sustainability, and the quality of life through digital technologies and data analytics. Smart city transformation requires interdepartmental collaboration and public participation to ensure that the application of digital technologies aligns with the needs and expectations of urban residents. Consequently, it becomes a complex process necessitating close cooperation and coordination among policymakers, city administrators, technology experts, and the public. Komninos et al. 9 define smart cities as places where digital technologies, innovation, and the urban environment intersect—a burgeoning urban paradigm designed to more effectively address complex challenges such as urban growth, sustainability, and governance by leveraging intelligent systems for decision-making and innovation. Realizing smart cities necessitates an organic fusion of digital technologies, innovation, and the urban environment to enhance the efficiency, reliability, and quality of urban governance and public services, while also promoting urban economic development and reducing resource consumption and environmental pollution. Esposito et al. 20 describe the definition of smart cities as the utilization of ICT to create resource-efficient, secure, inclusive, and accessible urban environments, fostering economic growth based on environmental sustainability and inclusive prosperity and ensuring equal access to public goods and high-quality services for all.
According to the “Global Review of Smart City Governance Practices” 28 by United Nations Habitat, healthcare constitutes an integral component of the manifold services provided by cities to meet residents’ needs and is increasingly reliant on digital technologies. Meanwhile, local governments worldwide are propelling the transition toward smart cities, presenting novel opportunities for enhancing healthcare services. The smart city agenda encompass more than mere technological advancement; successful navigation toward smart cities necessitates the convergence of technology with internal policy, regulation, organizational, and institutional changes within local governments. The report highlights the latest trends and best practices in global smart city governance, namely, (a) comprehensive, sustainable, inclusive, and innovative planning of smart cities, taking into account the overall development of urban areas; (b) digitization as the keystone of smart cities; (c) public engagement as a vital constituent of smart city governance; (d) sustainability as a core principle in smart city governance; (e) ethical considerations governing the development of smart city technologies; and (f) the pivotal role played by local governments in smart city governance.
In November 2012, the Ministry of Housing and Urban–Rural Development of China issued a notice to launch the national smart city pilot program, marking the first step toward promoting smart cities. In January 2013, the Ministry of Housing and Urban–Rural Development of China announced the first batch of 90 national smart city pilot cities, including 37 cities, 50 districts/counties, and 3 towns. In May, 103 more cities (districts/counties/towns) were added to the pilot program after approval. In August, the State Council of China explicitly called for the acceleration of smart city construction and encouraged all types of market entities to participate in smart city development in cities with favorable conditions. In October, the Ministry of Science and Technology and the National Standardization Management Office of China clarified the technical definition of “smart city” and announced 20 pilot cities. In March 2014, the Central Committee of the Communist Party of China and the State Council issued the “National New Urbanization Plan (2014–2020),” which listed smart cities as one of the three major goals of urban development in China and proposed the construction of a number of distinctive smart cities by 2020. In April 2015, 84 cities (districts/counties/towns), including Mentougou District in Beijing, were designated as new national smart city pilot cities, while 13 cities (districts/counties), including Zhengding County in Shijiazhuang City, Hebei Province, were designated as expanded pilot cities. In December 2016, the State Administration for Market Regulation and the National Standardization Management Office issued GB/T33356-2016 “Evaluation Index System for New Smart Cities,” providing necessary criteria and standards for smart city construction. The State Council pointed out in the “Thirteenth Five-Year National Informatization Plan” that by 2018, 100 new model smart cities would be constructed in a graded and classified manner, and significant achievements would be made in the construction of new smart cities by 2020. In October 2017, GB/T34678-2017 “Technical Reference Model for Smart Cities” was promulgated, providing an overall plan for smart city ICT and the technical principles and requirements for smart city construction. In June 2018, GB/T36333-2018 “Guidelines for Top-level Design of Smart Cities” was promulgated, specifying the specific requirements for the top-level design of smart cities and providing the overall principles, basic processes, and specific recommendations for the top-level design of smart cities. In April 2021, the National Development and Reform Commission issued the “Key Tasks for New Urbanization and Urban–Rural Integration Development in 2021,” which included the construction of new smart cities as a key task for the year. Table 1 delineates the smart city pilot policies relevant to this paper.
China Ministry of Housing and construction of smart city pilot list.
Note. Compiled by the author.
The following geographical distribution map (Figure 1) showcases the implementation of smart city pilot policies at different time points in various cities. It is evident that the smart city pilot policies are mainly concentrated in the eastern and central provinces of China, with fewer in the western region. Additionally, there is a relatively dispersed distribution in the central and eastern regions, indicating that the smart city pilot policies are universal and not targeted at individual cities.

National smart city pilot area distribution.
Theoretical hypotheses
Basic hypothesis
The CSCPP aims to strengthen urban development, optimize urban governance, promote sustainable economic and social development, and enhance the quality of life of citizens through the use of advanced technology. Specifically, the CSCPP can impact the provision of urban healthcare services in four ways: first, by encouraging the sharing of medical and health big data. The promotion of smart city construction can strengthen the application of medical information technology and support information exchange and sharing among public health management institutions and medical institutions. This will help improve collaborative work efficiency, enhance the efficient allocation of medical resources, and improve epidemic prevention and control and emergency medical rescue capabilities. Second is by building a smart healthcare platform. Smart city construction can promote remote medical platforms, online diagnosis and treatment systems, and online consultations based on 5G networks, supplemented by wearable devices and home medical equipment,
29
to realize medical services such as disease monitoring, health support, and intelligent medical treatment.
30
Third is by establishing a mechanism for balancing medical service supply and demand. Smart cities can optimize the allocation of medical resources through electronic diagnosis and treatment, remote consultations, image transmission, etc., to avoid duplicate construction. At the same time, using big data, artificial intelligence, and other technologies in various fields related to production and life can provide more convenient and effective medical services for patients.
31
Fourth is by promoting medical and health technological innovation. Relevant studies have shown that in the field of medical and health technological innovation, smart city construction can promote the deep integration of “digitalization, intelligence, and interconnection” technologies with medical resources,
32
thereby improving the quality and efficiency of medical service supply. Based on this, the following theoretical hypothesis is proposed.
Heterogeneity hypothesis
In the construction of smart cities in China, there is a need for collaborative coordination and administrative approval from multiple sectors and departments, including urban planning, industry and information technology, transportation, environmental protection, and public security institutions. Each department has specific responsibilities and approval authority, providing support to ensure the smooth progress and implementation of the project. Therefore, in the process of building smart cities, close collaboration and efficient cooperation among multiple departments are crucial to ensure the seamless implementation of the entire project plan. The establishment of administrative approval service centers can shorten the approval time, increase approval concentration, redesign the approval process, significantly reduce institutional transaction costs,33,34 and improve economic efficiency.
35
Based on this, the following theoretical hypothesis is proposed.
The construction of smart cities requires a large investment in digital technology and infrastructure. When local fiscal pressure is too high, on the one hand, insufficient fiscal revenue to support the funding required for large-scale infrastructure construction may lead to a reduction in investment to balance the budget. At the same time, high fiscal pressure often accompanies a high debt burden, which may also lead to a reduction in infrastructure investment to reduce debt pressure. On the other hand, excessive local fiscal pressure may crowd out public service investment such as medical care,
36
leading to an increase in public fiscal expenditure and waste
37
and inhibiting urban scale and coordinated development level.
38
Based on this, the following theoretical hypothesis is proposed.
The construction of smart cities requires multidimensional and diverse advanced technologies, and cities with a higher level of medical service already have advanced technologies that can provide better urban management decision-making and improve disease control efficiency,39,40 thereby effectively promoting the pilot construction of smart cities. Conversely, Zhu et al.
41
believe that when the medical level of a city cannot meet the needs of its development, it is easy to lead to a shortage of medical resources, which in turn affects the construction of smart cities. Based on the above analysis, the following theoretical hypothesis is proposed.
The construction of smart cities generally varies regionally and internationally.
42
Specifically in China, there are huge differences in geographical location, development level, and planning direction among cities. Eastern regions place more emphasis on social governance, such as improving public service capabilities such as medical care, while central and western cities focus more on urban innovation and economic vitality.
43
Generally speaking, the higher the economic development level, the higher the level of smart construction.
44
Based on the above analysis, the following theoretical hypothesis is proposed.
Empirical design
Data source
The data for this paper mainly comes from three batches of “National Smart City List” announced by the Ministry of Housing and Urban–Rural Development of the People's Republic of China, which includes a total of 290 cities (districts), as well as the National Bureau of Statistics, China Statistical Yearbook, and various provincial and municipal statistical yearbooks. Missing values are filled in using the average interpolation method, and the data is trimmed at the upper and lower 1% tails. Finally, a balanced panel data set is obtained, consisting of 286 cities (districts) with a total of 5720 observations from 2000 to 2019.
Econometric equation
There is a typical two-way endogeneity between smart city transition and the provision of healthcare services: the higher the level of smart city transition, the more digital technologies can be applied in the healthcare field, which can affect the provision of healthcare services, and the higher the provision of healthcare services driven by digital technology, the more it can influence smart city transition in return. In 2013, the Chinese government launched the smart city pilot policy, which encourages pilot cities to use digital technologies such as the IoT, big data analysis, and artificial intelligence to improve urban operations and citizens’ quality of life by providing funding, policy guidance, and technical assistance. After the pilot, the level of smart city transition is bound to be enhanced, so we can fully utilize the CSCPP as a quasi-natural experiment to identify the causal relationship between smart city transition and the provision of healthcare services.
To test the theoretical hypothesis, this paper constructs a double-fixed effects DD model
45
as follows:
Variable definition
Explanatory variables (PCA and EWM). The explanatory variable in this paper is the level of medical services. Following the approach of Bai,
46
Xin,
47
and Tian et al.,
48
and considering the availability of city-level data, this paper selects three indicators—the number of medical institutions (hospitals/clinics), human resources (number of doctors), and institutional services (number of hospital/clinic beds)—to measure the provision of medical and health services in cities. To facilitate empirical analysis, we use PCA and the EWM to weight the three indicators. Before weighting, we first normalize the three indicators using the formula below:
Principal component analysis.
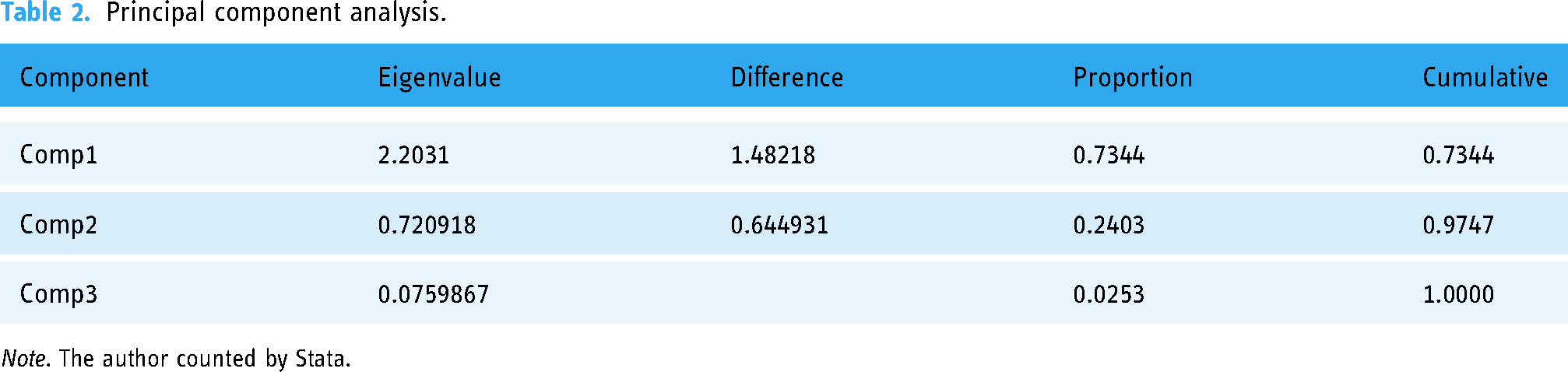
Note. The author counted by Stata.
The EWM aims to assign weights to each evaluation index according to its degree of difference.
49
If the information entropy of the index is smaller, the more information the index provides, the greater the role it plays in the synthesis, and the higher the weight. After the EWM, a comprehensive index is derived, which is shown in the following equation:
Core explanatory variable (City*Post). The core explanatory variable in this paper is the smart city pilot policy. Considering that the implementation of smart city pilots is gradual, this paper adopts a generalized DD model based on two-way fixed effects in the model setting. Following common practice, if a city implements the policy in the second half of year t, then year t + 1 is set as its pilot year; if the policy is implemented in the first half of year t, then year t is set as the pilot year.
Control variables. Referring to the methods used by Tian et al., 48 Xin, 47 An and Jia, 50 and Jiang and Liu, 51 the control variables mainly include the economic development level (economic), as higher economic development levels in a region correspond to higher demand for medical services, and the region also has greater ability to improve the supply of medical services; industrial structural changes (Struc2 and Struc3), changes in the industrial structure, which will increase population mobility, leading to corresponding changes in the supply and demand of local medical resources, and will also directly affect the government's resource input into the medical industry, affecting the supply and demand of local medical resources; population density (density), as higher population density in a region corresponds to higher demand for medical services, which will affect the supply of medical services in the region; government intervention (revenue), as government intervention in the economy will affect the future development of different industries, thereby changing the industrial structure, which will obviously affect the medical service industry; and medical security (security), as higher levels of medical security in a region imply that the government has invested more funds into the medical service industry and also mean that the cost of seeking medical treatment is lower for individuals, which will improve the supply of medical and health services in the region.
The main variables and definitions in this paper are shown in Table 3.
Variable definitions.
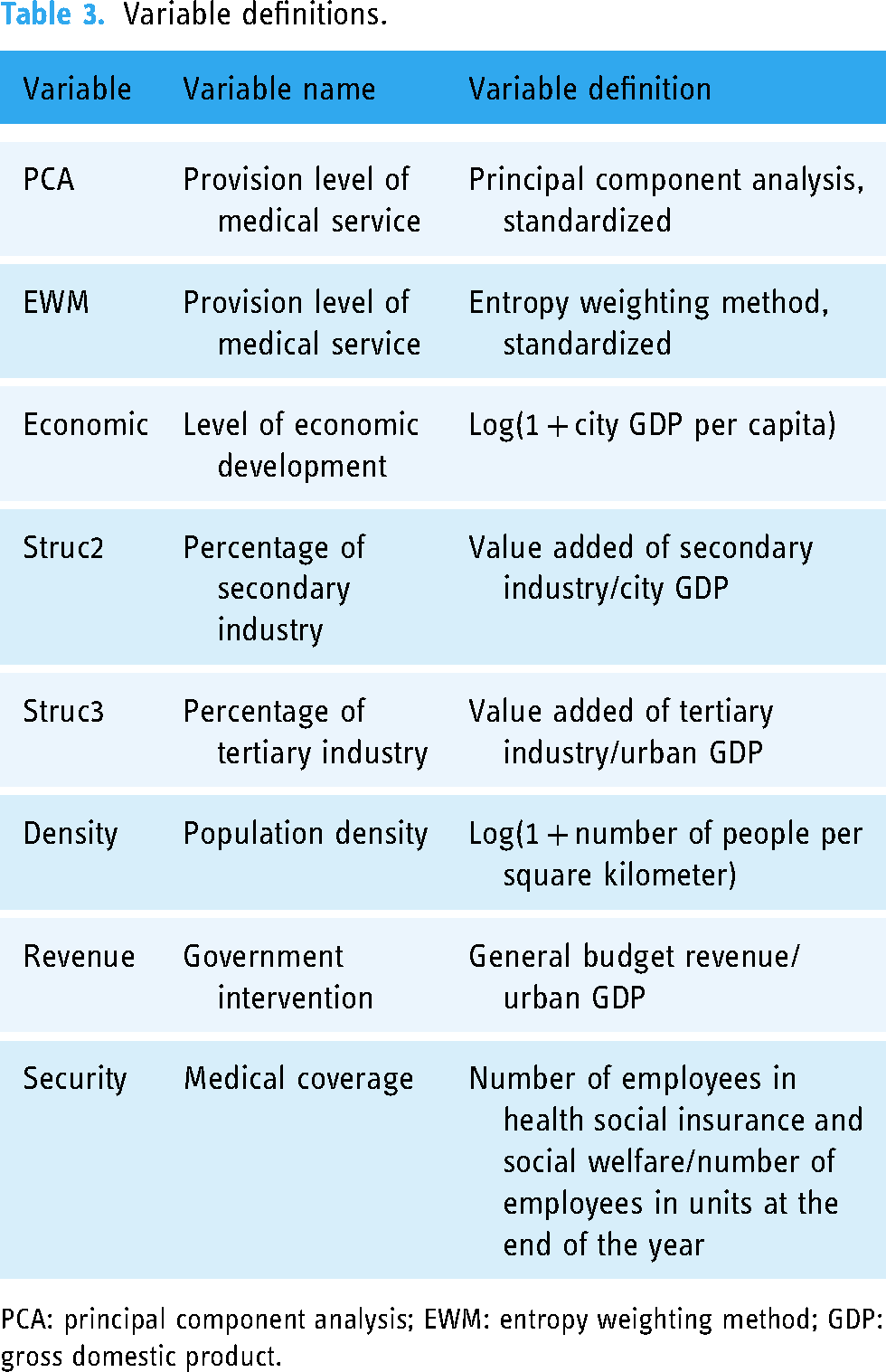
PCA: principal component analysis; EWM: entropy weighting method; GDP: gross domestic product.
Descriptive statistics
Table 4 presents the descriptive statistics of the main variables in this paper. The mean of PCA is 0.193, while the mean of EWM is 0.401, indicating a certain difference between the two measurement methods of the dependent variable. This also highlights the necessity of using both methods for empirical analysis in this paper. Other variables are not further elaborated upon.
Descriptive statistics.

Note. Compiled by the author.
PCA: principal component analysis; EWM: entropy weighting method.
Regression analysis
Basic regression
To show the impact of introducing different control variables on the basic regression, a stepwise regression approach was used. The specific results are shown in Table 5. Columns (1)–(3) present the regression results for PCA as the dependent variable. As control variables and fixed effects are gradually added, the coefficients show a trend of first decreasing and then increasing. Based on the results in column (3), the coefficient of Post*City is 0.0321 and significant at the 1% level, indicating that after CSCPP, the level of medical and health service supply in pilot areas has increased by 3.21 percentage points compared to non-pilot areas. Columns (4)–(6) present the regression results for EWM as the dependent variable. As control variables and fixed effects are gradually added, the coefficients show a continuous decreasing trend. Based on the results in column (6), the coefficient of Post*City is 0.0639 and significant at the 1% level, indicating that after CSCPP, the level of medical and health service supply in pilot areas has increased by 6.39 percentage points compared to non-pilot areas. It is clear that both measurement methods regarding the level of medical and health service supply consistently indicate that CSCPP can improve the level of medical and health services, which is in line with the expected Hypothesis 1.
Basic regression.

Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
PCA: principal component analysis; EWM: entropy weighting method.
*p < .1. **p < .05. ***p < .01.
Robustness checks
Driscoll-Kraay(DK) standard errors. In consideration of the potential impacts of heteroscedasticity, autocorrelation, and cross-sectional correlation on the basic regression results, this paper re-estimated the regression to obtain DK standard errors that simultaneously control for these three issues. 52 The results are presented in columns (1)–(2) of Table 6. Compared with the basic regression results, the standard errors of Post*City have significantly increased, but CSCPP still has a significant promoting effect on both PCA and EWM, indicating the robustness of the results.
Robust regression.
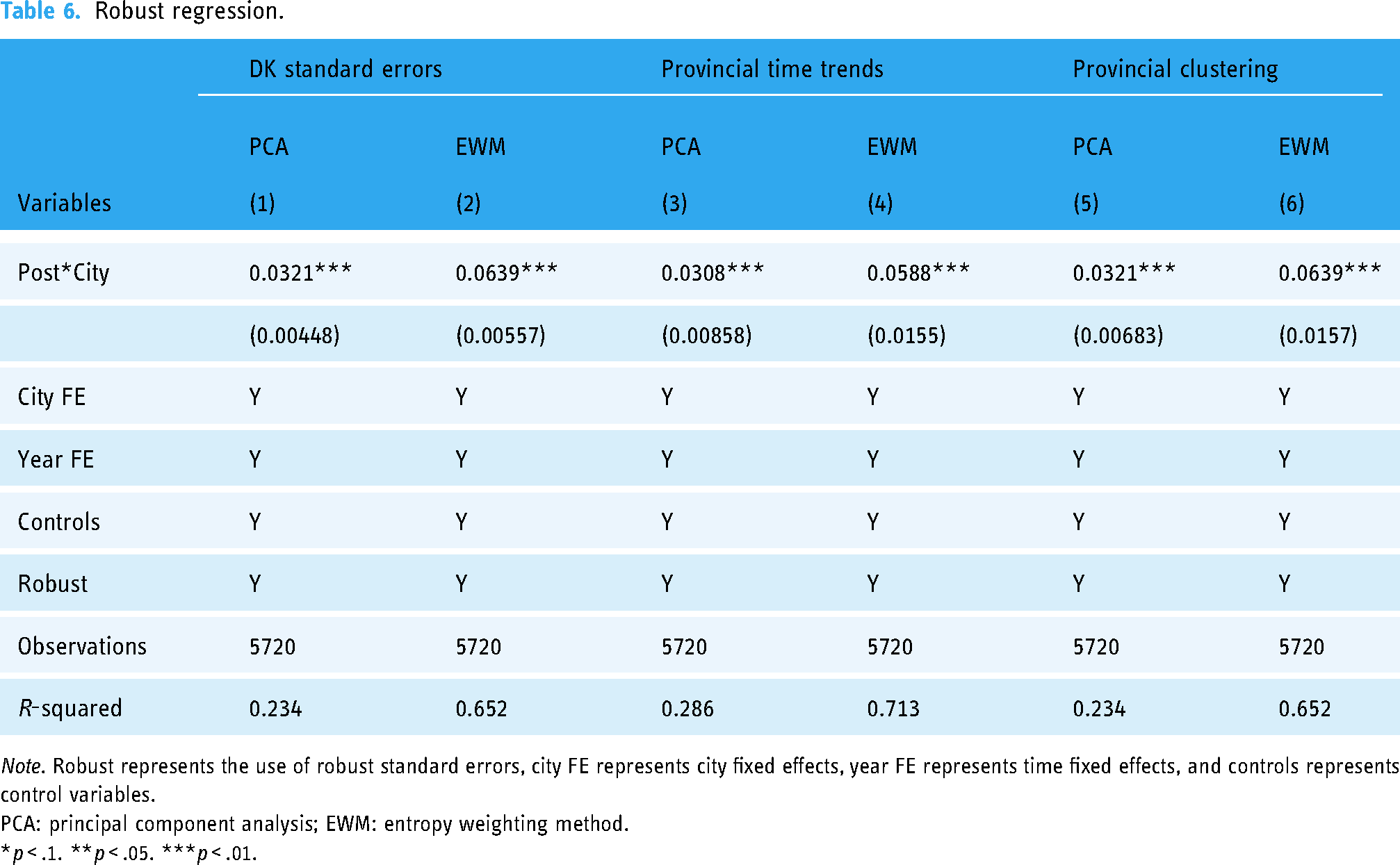
Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
PCA: principal component analysis; EWM: entropy weighting method.
*p < .1. **p < .05. ***p < .01.
Provincial time trends. To address the concern that the regression results may be driven by city time trends, 45 which means that the level of medical and health services in cities may continue to increase over time even without CSCPP, this paper introduced city time trend variables into the regression. The results are presented in columns (3)–(4) of Table 6. We can see that the impact coefficients of Post*City on both PCA and EWM have slightly weakened compared with the basic regression results, but they are still statistically significant at the 1% level, indicating the robustness of the results.
Provincial clustering
Parallel trend test
Dynamic test
In this paper, we use the DD causal identification framework for empirical analysis, which requires the fulfillment of the parallel trend assumption, i.e. there are no significant differences between the treatment group and the control group before the policy intervention. Drawing on the event study method in finance, we construct the following dynamic regression equation
54
for testing:
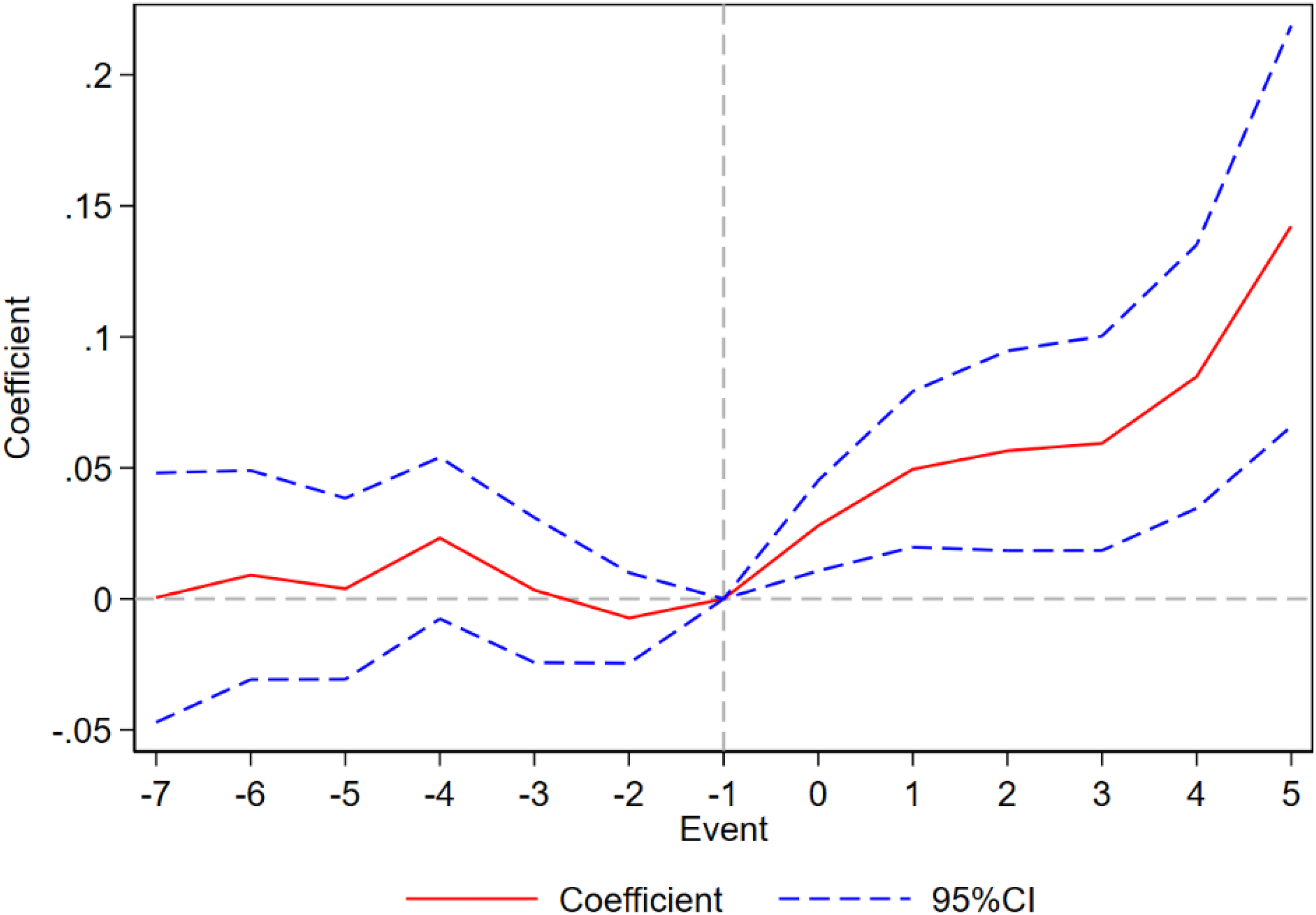
The specific regression results are shown in Figures 2 and 3: It is not difficult to find that the regression coefficients in each period before CSCPP occurrence are not significant, indicating that there is no significant difference between the treatment group and the control group before the policy intervention, fulfilling the parallel trend assumption. After the policy intervention, we can also see that the coefficients show an increasing trend, indicating that CSCPP's promotion effect on the level of urban medical and health service supply is becoming more significant.

Principal component analysis dynamic diagram.
Entropy weighting method dynamic diagram.
Placebo test
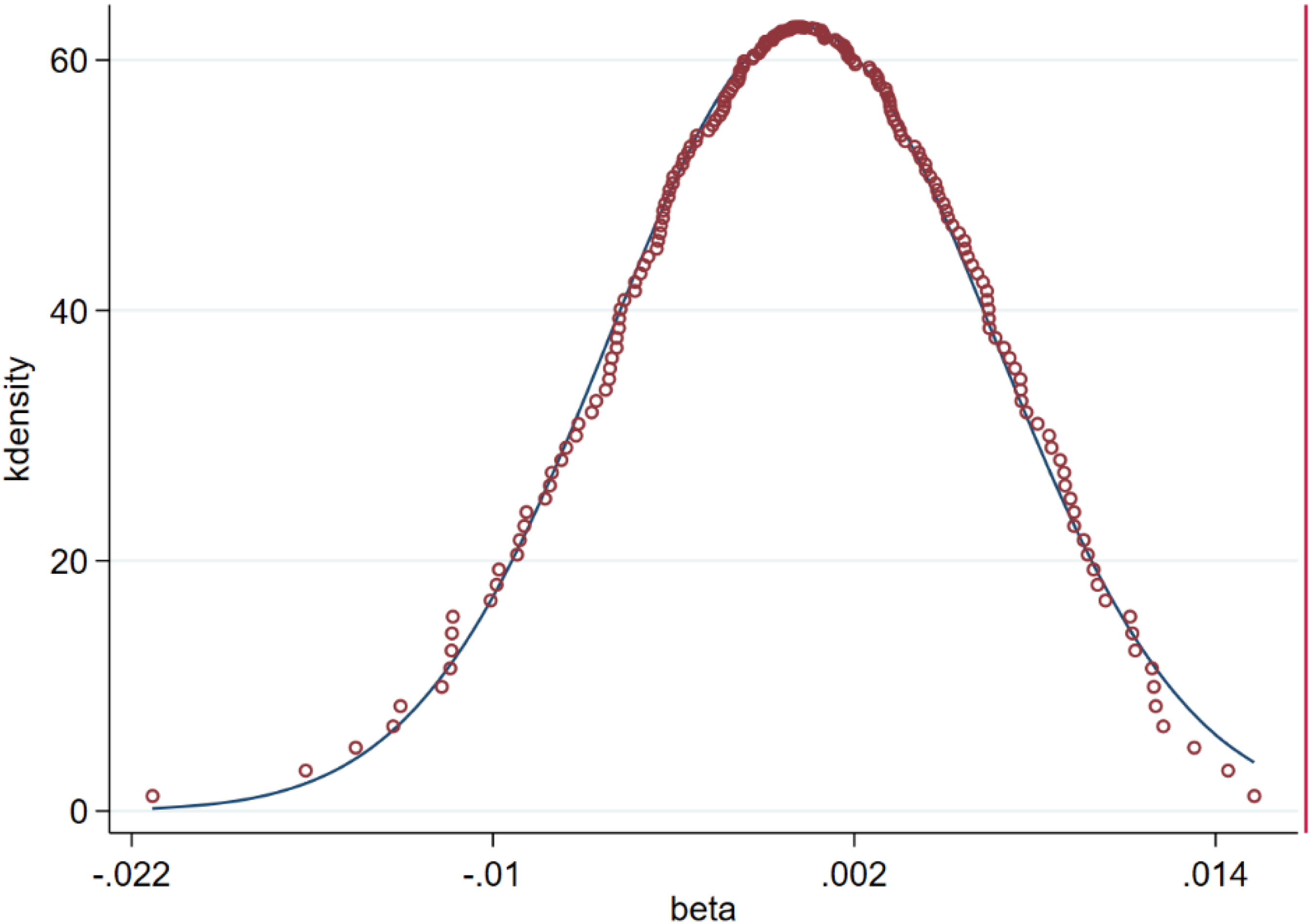
There is a potential concern in this paper that the basic regression results may have been driven by chance assignment rather than by CSCPP. To eliminate this potential confounding factor, we arbitrarily designated false treatment and control groups and conducted 200 random samplings for placebo testing. 55 The density distributions of the coefficients are shown in Figures 4 and 5. It is evident that the true regression coefficients are significantly different from the false regression coefficients, indicating that the basic regression results are indeed driven by CSCPP rather than chance factors.

Principal component analysis consolation chart.
Entropy weighting method consolation chart.
Discussion
Symbiotic event
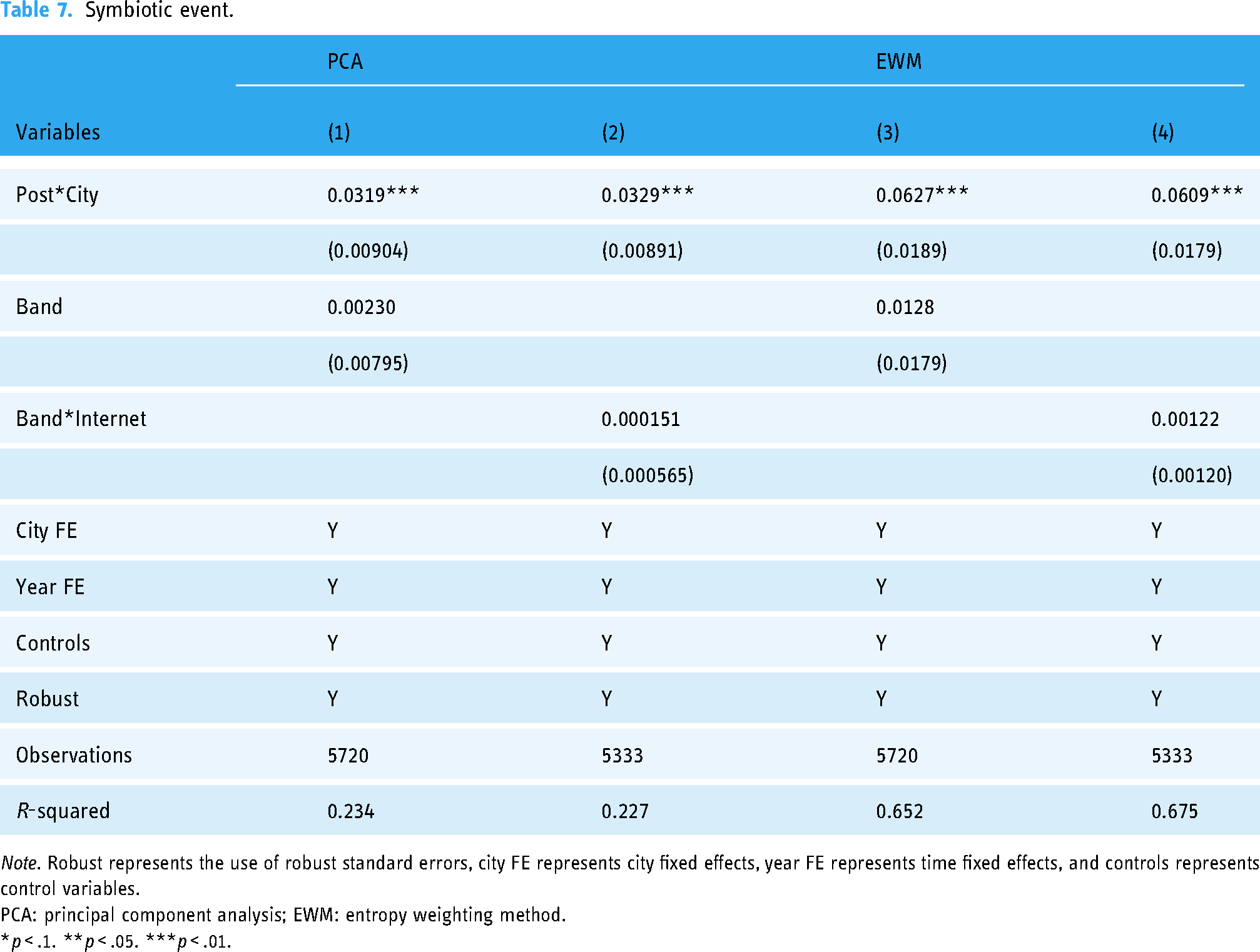
On 17 August 2013, the Chinese State Council released the “Broadband China” strategic implementation plan, which set the goals and paths for broadband development in the next 8 years. This marked the elevation of the “Broadband Strategy” from a departmental action to a national strategy, with broadband becoming a strategic public infrastructure for the first time. The Broadband China strategy and the implementation of CSCPP coincide in time, and their objectives are both to enhance the public infrastructure of information technology. Wirtz and Müller 56 contend that the broadband network infrastructure serves as the technological foundation for the provision of public services. Therefore, the results of this paper's basic regression are likely to be severely affected by the Broadband China strategy policy. To eliminate this concern, this paper adopts two strategies: First, a virtual variable of the Broadband China strategy (Band) is introduced in the basic regression, and the results are shown in columns (1) and (3) of Table 7. It is observed that the influence of Band on PCA and EWM is not significant, while the impact coefficient of CSCPP on PCA and EWM slightly decreases compared to the baseline regression results, indicating that the Broadband China strategy policy does not exert a substantial interference on the findings of this study. Second, a virtual variable of the Broadband China policy and the product of the number of Internet users before the policy is introduced (Band*Internet) are introduced to control the intensity of the implementation of the Broadband China strategy. The results are presented in columns (2) and (4) of Table 7. It is evident that the impact of Band*Internet remains insignificant, and the coefficient of CSCPP on PCA and EWM is similar to the baseline regression results, once again indicating that the Broadband China strategy policy has minimal interference with the findings of this study.
Symbiotic event.
Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
PCA: principal component analysis; EWM: entropy weighting method.
*p < .1. **p < .05. ***p < .01.
Sample self-selection bias
Another important potential challenge faced by the basic regression results in this paper is sample self-selection bias, which occurs when different cities actively choose to join or not join the smart city pilot program by utilizing their available resources. This can seriously overestimate the basic regression results in this paper. To eliminate sample self-selection bias, this paper applies the PSM-DD causal identification framework 57 for re-regression, with the covariates being the control variables mentioned earlier.
Regression results. Table 8 shows the PSM-DD regression results: columns (1) and (2) are the results of 1:1 nearest neighbor matching; columns (3) and (4) are the results of 1:3 nearest neighbor matching, and columns (5) and (6) are the results of kernel matching. Overall, taking into account the self-selection effect, CSCPP still exhibits a significant positive effect on PCA and EWM, without significantly interfering with the fundamental conclusions of this study. In comparison to the baseline regression results, the notable change lies in the impact of CSCPP on EWM, which decreases by approximately half. However, it remains statistically significant at the 1% level, and this change may be attributed to the specific method of calculation.
Propensity score matching–difference-in-differences regression.

Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
PCA: principal component analysis; EWM: entropy weighting method.
*p < .1. **p < .05. ***p < .01.
Balance test. The prerequisite for using the PSM-DD method is that covariates must pass the balance test; otherwise, the regression results are likely to be driven by covariate differences. Table 9 shows the balance test results for covariates, and after matching, covariate differences (%bias) generally decreased to below 10%, satisfying the balance test.
Balance test.

Note. Compiled by the author.
Spatial spillover effects
The level of healthcare service supply in one region can have an impact on another region, either a positive impact, where an increase in the level of healthcare service in one region may lead to the spread of technology and experience, thereby having a positive impact on other regions, or a negative impact, where an increase in the level of healthcare service in one region may attract more healthcare resources and talent, which may lead to a reduction in resources in other regions, thereby affecting their healthcare service level. It is evident that the level of healthcare service supply has a significant spatial spillover effect, which means that the basic regression results may be driven by spatial spillover effects. To eliminate this concern, we apply a spatial DD causal identification framework for analysis.
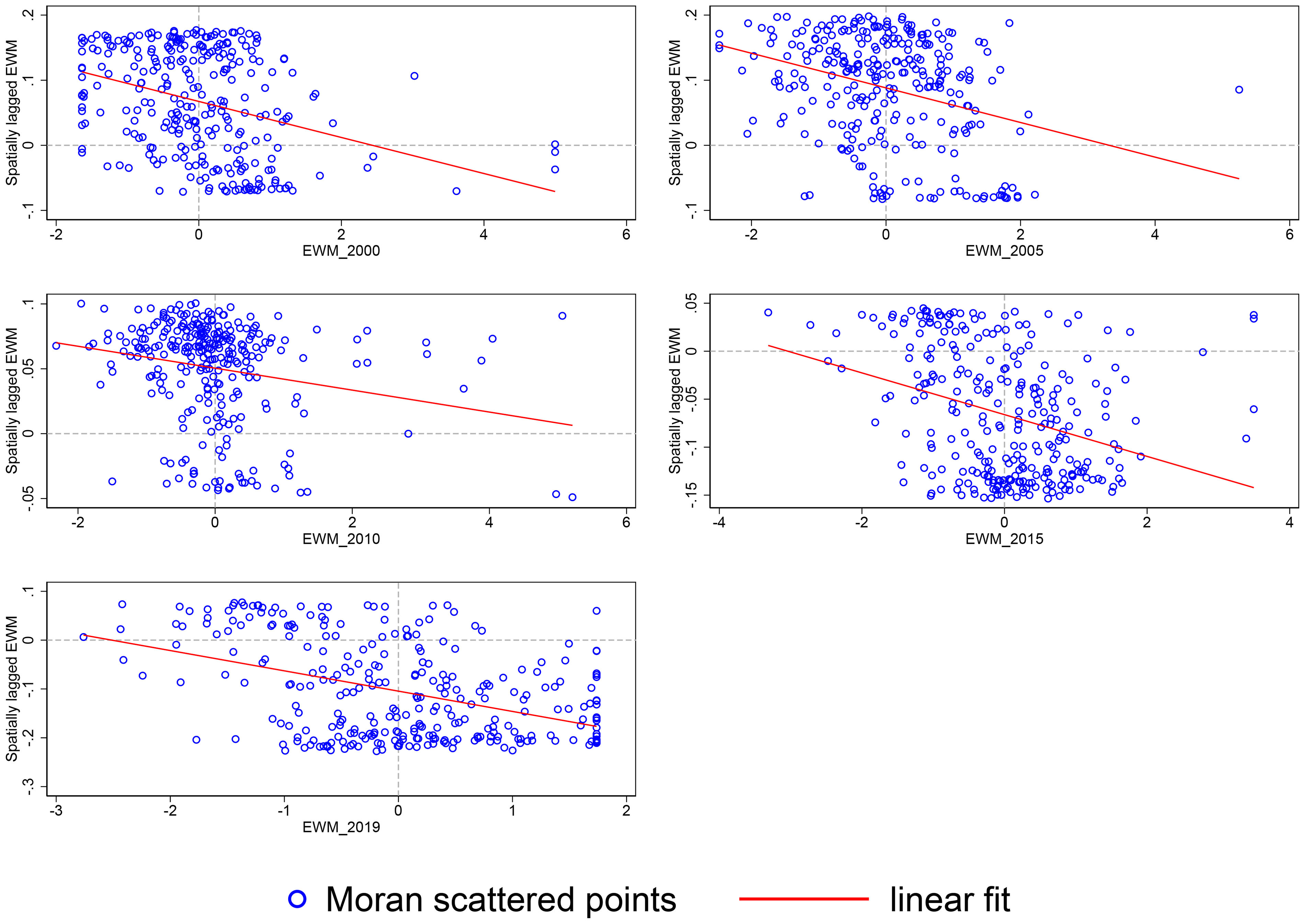
Moran scatter plot. We use city-level Moran scatter plots to determine the existence and directionality of spatial spillover effects. The Moran scatter plots in Figures 6 and 7 over the years indicate two points: first, there is a significant spatial spillover effect in the level of healthcare service supply; second, this spatial spillover effect is negative, meaning that the higher the level of healthcare service supply in the surrounding areas, the lower the level in the local area, and vice versa.

Moran scatter plot (principal component analysis).
Moran scatter plot (entropy weighting method).
Spatial econometric model. The Moran scatter plot presented earlier was merely an intuitive representation. To rigorously test the hypothesis, we will construct a spatial Durbin model (SDM) at the city level, following the approach of Jia et al.
58

Different spatial models.

Notes. The sources are derived from Chen Qiang. 59
Spatial regression. Table 11 displays the regression results of different spatial econometric models: columns (1) and (2) show the results of applying the spatial lag model (SLM) spatial econometric model, it is evident that ρ has a significant negative impact on PCA and EWM, indicating a crowding-out effect of healthcare resource supply from neighboring cities on the focal city. This finding is consistent with the conclusion drawn from the Moran scatter plot. In contrast, CSCPP exhibits a significant positive effect on PCA and EWM, which is similar to the baseline regression results. This suggests that the conclusions of this study are not significantly influenced by the spatial geographic effects of healthcare resources in surrounding cities. Columns (3) and (4) show the results of applying the SDM spatial econometric model, it is evident that τ has a positive impact on PCA and EWM, indicating that the CSCPP policy in neighboring cities can facilitate the smart city transition in the focal city. Even after controlling for this positive spillover effect, CSCPP still exhibits a significant positive impact on PCA and EWM, which is similar to the baseline regression results. This suggests that the conclusions of this study are not significantly influenced by the spatial geographic effects of CSCPP in the surrounding areas. Columns (5) and (6) show the results of applying the spatial errors model (SEM) spatial econometric model; it is apparent that γ does not have a significant impact on PCA and EWM, indicating that the unobservable factors in neighboring cities do not affect the provision of urban healthcare services. In this scenario, CSCPP still exhibits a significant positive impact on PCA and EWM, which is similar to the baseline regression results.
Spatial regression results.

Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
SLM: spatial lag model; SDM: spatial Durbin model; SEM: spatial errors model; PCA: principal component analysis; EWM: entropy weighting method.
*p < .1. **p < .05. ***p < .01.
Mechanism testing
The level of healthcare service provision is determined by three sub-indicators: the number of healthcare institutions (hospitals/clinics), human resources (number of doctors/practitioners), and institutional services (number of hospital/clinic beds). Considering the potential error in the composite indicator, does CSCPP truly affect the original three sub-indicators? To test this, we replaced the dependent variable and re-conducted the regression analysis. The results are shown in Table 12. Column (1) shows the regression results with the number of healthcare institutions (Hospital) as the dependent variable; column (2) shows the regression results with human resources (Doctor) as the dependent variable; column (3) shows the regression results with institutional services (Bed) as the dependent variable. These regression results indicate that the promotion of healthcare service provision by CSCPP is mainly achieved through the two channels of increasing human resources and institutional services. This is also in line with institutions, as the number of healthcare institutions requires strict approval processes and significant capital investment, making it difficult to achieve significant growth in the short term.
Mechanism testing.

Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
*p < .1. **p < .05. ***p < .01.
Heterogeneity tests
This section will conduct a series of heterogeneity tests aimed at both verifying the theoretical hypotheses presented earlier and enriching our understanding of the impact of CSCPP on the provision level of urban healthcare service. The specific regression results are presented in Table 13.
Heterogeneity regression.

Note. Robust represents the use of robust standard errors, city FE represents city fixed effects, year FE represents time fixed effects, and controls represents control variables.
*p < .1. **p < .05. ***p < .01
Administrative approval service centers
The theoretical Hypothesis 2 presented earlier suggests that the effectiveness of CSCPP is greater in cities with administrative approval service centers. To test this hypothesis, we divided the sample into two sub-samples, one with administrative approval centers and one without, and conducted separate regressions. Data on administrative approval centers were obtained from three sources: the main source was the official websites of local administrative approval centers, followed by formal documents on the establishment of administrative approval centers published on government websites, and news reports released by local media and city-level government websites. To ensure data quality, we cross-validated the information obtained from the three sources, and in cases of conflict, we selected the information based on the priority of administrative approval center official websites, government documents, and news reports. Panel A shows the results of the grouped regression: Columns (1) and (2) show that the impact coefficient of City*Post in the sub-sample with administrative approval centers is 0.0251 and significant at the 1% level, while there is no significant impact in the sub-sample without administrative approval centers; columns (3) and (4) show that the impact coefficient of City*Post in the sub-sample with administrative approval centers is 0.0492 and significant at the 1% level, while there is no significant impact in the sub-sample without administrative approval centers. Hypothesis 2 is confirmed.
Fiscal pressure
The theoretical Hypothesis 3 presented earlier suggests that CSCPP is more effective in cities with lower fiscal pressures. To test this hypothesis, we divided the sample into two sub-samples, one with high fiscal pressure and one with low fiscal pressure, and conducted separate regressions. Fiscal pressure was measured by “general public budget expenditure/general public budget revenue” of the cities, and sub-samples were defined as those above the 66th percentile and those below the 33rd percentile. The specific results of the grouped regression are shown in panel B: columns (1) and (2) show that the impact coefficient of City*Post in the sub-sample with low fiscal pressure is 0.0359 and significant at the 1% level, while there is no significant impact in the sub-sample with high fiscal pressure; columns (3) and (4) show that the impact coefficient of City*Post in the sub-sample with low fiscal pressure is 0.0500 and significant at the 5% level, while there is no significant impact in the sub-sample with high fiscal pressure. Hypothesis 3 is confirmed.
Provision level of healthcare services
The theoretical Hypothesis 4 presented earlier suggests that CSCPP is more effective in cities with a higher level of healthcare service provision. To test this hypothesis, we conducted quantile regressions on the provision level of healthcare services at the 66th and 33rd percentiles, respectively. The results are shown in panel C: columns (1) and (2) show that the impact coefficient of City*Post in the sub-sample with a high provision level of healthcare service is 0.0722 and significant at the 1% level, while the impact coefficient in the sub-sample with a low provision level of healthcare service is only 0.0229 and significant at the 1% level; columns (3) and (4) show that the impact coefficient of City*Post in the sub-sample with a high provision level of healthcare service is 0.0509 and significant at the 1% level, while the impact coefficient in the sub-sample with a low provision level of healthcare service is only 0.0403 and significant at the 1% level. Hypothesis 4 is confirmed.
Regional heterogeneity
The theoretical Hypothesis 5 presented earlier suggests that CSCPP is more effective in eastern regions. To test this hypothesis, we divided all cities into sub-samples of eastern regions and central and western regions and then conducted grouped regressions. The eastern region includes 12 provinces: Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, Guangxi Zhuang Autonomous Region, and Hainan Province, while the remaining provinces belong to the central and western regions. The results are shown in panel D: columns (1) and (2) show that the impact coefficient of City*Post in the sub-sample of the eastern region is 0.0396 and significant at the 1% level, while the impact coefficient in the sub-sample of the central and western regions is only 0.0285 and significant at the 5% level; columns (3) and (4) show that the impact coefficient of City*Post in the sub-sample of the eastern region is 0.0820 and significant at the 1% level, while the impact coefficient in the sub-sample of the central and western regions is only 0.0322 and not significant. Hypothesis 5 is confirmed.
Conclusion and policy recommendations
Theoretical scrutiny and empirical investigation revealed compelling evidence that the advent of smart city transition holds the potential to profoundly enhance the provision of healthcare services. This inference has been subjected to meticulous scrutiny, successfully navigating the intricate labyrinth of potential causal identification. The crux of this discourse predominantly emanates from the augmentation of healthcare human resources and institutional services, which serve as intrinsic channels for its attainment. The impact of the smart city transition exhibits greater potency within cities harboring administrative approval centers, experiencing minimal fiscal constraints, and thriving with an abundance of healthcare service supply, particularly prominent in the eastern region.
Based on these findings, three policy recommendations emerge. Firstly, it is imperative for the government to expedite the advancement of the smart city transition, a notion corroborated by the theoretical and empirical foundations of this discourse. Presently, smart city transition in China remains predominantly focused on the construction of digital infrastructure, necessitating a shift toward a citizen-centric approach, whereby technology serves as a means to address the needs and aspirations of urban residents. 27 This transition demands interdepartmental collaboration and public engagement to ensure the application of digital technologies aligns with the expectations and demands of the urban populace, 16 as well as to achieve sustainable urban development. Secondly, a cautious and tailored approach is essential when initiating the smart city transition, given the considerable fiscal investments required. This assertion finds support in the heterogeneous examination of fiscal pressures conducted in this study. To best attain desired outcomes, governments should pioneer pilot projects in cities facing greater fiscal burdens, thus yielding more favorable results. Furthermore, commencing pilot initiatives in economically prosperous regions, most logically, would render superior outcomes, as such areas often experience lower fiscal pressures. 60 Lastly, bolstering collaborative support among pertinent public sectors is paramount. This study uncovers that regions with greater administrative approval for service centers exhibit superior outcomes in smart city transition. This stems from the understanding that smart city transition encompasses a comprehensive urban governance process, necessitating support and cooperation from multiple public sectors. Failure to foster such collaboration would amplify institutional transaction costs, 34 impeding the progress of the transformation process.
This paper primarily focuses on examining the impact of smart city transition on the provision of healthcare services. However, an important unanswered question arises: if a certain city already has an excessive supply of healthcare services, is it reasonable to further augment the provision of healthcare? To address this inquiry, a potential avenue for future research would involve investigating the effects of smart city transition on the allocation of medical resources. Mora et al. 16 proposed a governance framework for smart city transition, consisting of four dimensions and 12 governance practices. These dimensions and practices collectively form the governance framework for smart city transition. Another question worth exploring in the future is how to provide empirical evidence to evaluate the effectiveness of this framework in enhancing smart city transition, as well as the strength of the interaction between the dimensions.
Footnotes
Acknowledgments
The authors would like to sincerely thank the editor and reviewers for their kind comments.
Contributorship
Conceptualization, LG and YC; resources, LZ and CY; writing—original draft preparation, LG and YC; writing—review and editing, YC and HG; data processing, LG and HY. All authors have read and agreed to be the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Doctoral Research Innovation Program of Weifang Medical University (grant number: 041174).
Guarantor
LG.
Informed consent
Not applicable, because this article does not involve any studies with human subjects.
Note
To provide a visual representation of the logical flow of this paper, a roadmap has been included in Appendix A.
Appendix A