
Abstract
Objectives
As the digital wave reshapes the future of cities, smart city construction (SCC) is emerging as a key driver for improving public health and bridging social gaps through its inclusive potential. This research aims to investigate the impact of SCC on the health of middle-aged and older disabilities individuals, focusing on its dynamic trends, underlying mechanisms, unequal selection effects, and overall welfare.
Methods
Based on data from the China Health and Retirement Longitudinal Study, this paper estimates the impact of SCC on the health of middle-aged and older disabilities using the double machine learning method with the random forest algorithm, and examines the dynamic trend of the health effects using event study method.
Results
The results indicate that SCC significantly enhances the health of middle-aged and older disabilities, without resulting in a concomitant increase in healthcare expenditure. In the long term, the positive health effect increases year by year. Mechanism analysis reveals that SCC promotes health improvements through two key channels: enhanced accessibility of living infrastructure, including access to running water and internet, and increased household annual income. Heterogeneity analysis reveals that there are unequal selection effects in impact, the health-enhancing effects of SCC on middle-aged and older disabilities are more pronounced among non-retired individuals and those with a more extensive household composition. Finally, welfare analysis shows that SCC reduced their healthcare expenditures and improved labor market performance, with a conservatively estimated welfare benefit of US$3448.65.
Conclusion
By unraveling the underlying mechanisms and inequality selection effects, this study provides a comprehensive analysis of the potential for digital inclusion to inform scientific understanding and guide policy aimed at promoting health equity and improving the well-being of disadvantaged populations.
Keywords
Introduction
Ensuring equitable access to healthcare and enhancing the well-being of vulnerable populations are central to the United Nations’ Sustainable Development Goals for 2030.1,2 However, significant health disparities continue to be faced by middle-aged and older disabilities, due to structural barriers in urban infrastructure, limited access to healthcare services, and socioeconomic constraints.3–5 As global populations age and urbanization accelerates, the role of digitalization in promoting inclusive urban development has become increasingly prominent. 6 Smart City Construction (SCC), through the integration of digital technologies (such as Internet of Things systems, telemedicine platforms, electronic health records, and AI-powered public service applications) into urban infrastructure, has the potential to bridge existing accessibility gaps, improve healthcare delivery, and enhance the quality of life for people with disabilities. 7 Yet, despite rapid advancements in digital infrastructure, disparities in health outcomes persist, raising critical questions about the effectiveness and inclusivity of SCC in addressing the health needs of vulnerable populations. 8 It is therefore essential to understand the mechanisms through which SCC influences health outcomes for middle-aged and older disabilities so that more inclusive and effective urban policies can be designed.
However, while SCC is widely expected to optimize urban living conditions and reduce health inequalities, its potential positive impact on the health and well-being of middle-aged and older disabilities has not yet been fully realized.9,10 In response to the growing demand for inclusive urban development, many countries have launched SCC projects aimed at enhancing the efficiency of public services, improving accessibility, and promoting social inclusion through the integration of digital technologies. These projects focus on providing digital solutions in healthcare, transportation, and social services to improve the health of vulnerable groups, including middle-aged and older disabilities. 11 However, the impact of SCC on the health of this group remains unclear. Specifically, it is uncertain whether SCC significantly improves the health of middle-aged and older disabilities, and whether these effects are influenced by individual characteristics such as household composition and retirement status. Therefore, an in-depth exploration of the underlying mechanisms through which digitalization contributes to health improvements in the context of SCC projects is crucial for a comprehensive understanding of the inclusive potential of digitalization and its long-term impact on health equity and social justice.
As one of the largest developing countries, China faces significant challenges in addressing the health and well-being of its middle-aged and older disabilities.12,13 Despite considerable strides in healthcare infrastructure and social security expansion, there remain persistent disparities in access to healthcare services, exacerbated by uneven distribution of resources and demographic shifts. 14 The elderly and disabled populations are especially vulnerable, given the compounded barriers they face in urban environments, including limited access to healthcare, transportation, and social support. 15 SCC aimed at improving urban accessibility and social inclusion through digitalization, which is particularly focused on enhancing the healthcare system, social services, and mobility for middle-aged and older people with disabilities. SCC has contributed to notable economic and social advancements, making it increasingly important to investigate its effects on health and well-being. In light of the country's demographic trends and the ongoing health challenges it faces, China provides a valuable research context for examining the role of SCC in improving the health and social participation of middle-aged and older disabilities.
Based on the quasi-natural experiment of SCC pilot policy in China, this paper employs a double machine learning method to estimate the impact of SCC on the health of middle-aged and older disabilities. The conclusion remains robust after conducting various robustness tests, including event study, sample selection bias, short-term effect, eliminate concurrent policy interference, reset the double machine learning model, and instrumental variable method. In the mechanism analysis, SCC enhances their health through three primary channels: improving the accessibility of living infrastructure, increasing household income, and facilitating greater financial support through intergenerational transfers. Heterogeneity analysis reveals that there are unequal selection effects in impact, the health-enhancing effects of SCC on middle-aged and older disabilities are more pronounced among non-retired individuals and those with a more extensive household composition. Finally, welfare analysis shows that SCC reduced their health-care expenditures and improved labor market performance. Research framework is shown in Figure 1.

Research framework.
This paper makes several key contributions to literatures. First, while existing researches have extensively examined the economic and social benefits of SCC, limited attention has been paid to its health effects, particularly among vulnerable populations such as middle-aged and older disabilities.16–20 By focusing on the specific population group, this study expands the scope of SCC research to public health and social equity, addressing an important but underexplored dimension of digital urban transformation. Second, this paper employs an advanced causal inference approach using a double machine learning model, which mitigates potential biases caused by model misspecification and alleviates issues such as the “curse of dimensionality.” 21 This allows for a more precise estimation of the marginal impact of SCC on their health. Third, this paper empirically verifies how SCC influences health outcomes by improving living infrastructure accessibility, boosting household income, and enhancing financial support through intergenerational transfers. It also provides insights into how SCC affects health disparities and highlights unequal selection effects, emphasizing the need for targeted policy interventions to promote inclusive development. Finally, by leveraging empirical evidence from China's SCC pilot program, this paper provides valuable policy insights for other developing countries seeking to harness digitalization for social welfare enhancement.
Policy background
The concept of smart cities emerged from IBM's 2008 Smart Planet vision, reflecting the digital transformation of urban areas. 22 Leveraging digital technologies such as big data, broadband networks, and cloud computing, SCC aims to enhance interconnectivity, efficiency, and intelligence in urban operational systems, manifesting as urban innovation. In China, the development of smart cities is crucial for driving digital transformation and modernizing urban governance systems. The Ministry of Housing and Urban-Rural Development initiated smart city pilot projects in 2012, with subsequent promotions in 2013 and 2014. Spatial distribution of SCC is shown in Figure 2. These pilot cities were required to formulate implementation plans based on national indicator systems and local conditions, focusing on network infrastructure, urban public platforms, government services, basic public services, smart applications, and smart industries. The National Development and Reform Commission later emphasized the importance of new-type smart cities, promoting sustainable urban development through innovation and the integration of new information technologies with urbanization strategies. As SCC evolves, its scope has expanded to include innovative development, citizen-oriented services, precise governance, ecological livability, smart facilities, information security, and information resources.

Spatial distribution of SCC.
Relevant government documents outline the national smart city pilot policy, focusing on two primary objectives: enhancing urban governance for healthy and harmonious city development, particularly through illness prevention, reduction, and prompt treatment; and improving residents’ lifestyles by ensuring they genuinely benefit from smart city conveniences and affordability. 23 According to the 14th Five-Year Plan for National Informatization, Chinese digital economy has grown rapidly, with significant advancements in intelligent infrastructure, new business formats, and digital government construction. The market size of smart cities in China reached 25 trillion yuan in 2022, indicating a profound impact on the country's economy and society. However, as demonstrated in Figure 3, the number of persons with disabilities in different age groups in China., the majority of whom are middle-aged or older, is increasing annually, which has a substantial impact on economic growth and social stability. This poses a salient question regarding the impact of SCC on the health of middle-aged and older disabilities.

Number of persons with disabilities in different age groups in China.
Methodology
Samples and data
The data utilized in this cohort study stems from the esteemed China Health and Retirement Longitudinal Study (CHARLS) database, which boasts five waves of survey data from 2011 to 2020 (2011, 2013, 2015, 2018, and 2020). Jointly initiated by Wuhan University and Peking University in China in 2011, it is a rare long-panel tracking survey in China. Widely acknowledged as one of the most authoritative and exhaustive household-centric research resources in China, the database is openly accessible to support various research objectives. A total of 150 counties in China were selected to conduct in-depth household surveys, utilizing a rigorous multi-stage, random cluster sampling approach. The survey generates a robust dataset spanning three levels: individual, household, and community, encompassing approximately 450 families and over 10,000 individuals. All participants confirmed their informed consent prior to completing the questionnaire.
This paper constructs sample data through the following steps: (1) Utilizing individual ID, we create an unbalanced panel dataset, incorporating data from five survey years. (2) Samples of individuals with disability characteristics are retained. (3) Variables at household and community levels are associated with the individual sample pool using household ID and community ID. (4) Samples with missing key variables, such as dependent and independent variables, are excluded. The final dataset comprises an unbalanced panel containing 19,239 samples.
CHARLS is a longitudinal survey conducted across five waves over a span of ten years. Due to the extended time frame and the inherent challenges of tracking middle-aged and older disabilities, constructing a fully balanced panel would result in the exclusion of a substantial portion of the target population—particularly those with more severe health conditions, higher mortality rates, or unstable living circumstances. Such exclusion would likely introduce more serious selection bias and significantly reduce the representativeness of the sample. Consistent with practices in the econometric literature, we opted to use an unbalanced panel to retain greater sample variation and preserve statistical power. 52 We acknowledge that attrition may not be entirely random. To address this concern, we employed a double machine learning framework for the empirical analysis, which is robust to high-dimensional control variables and model misspecification, thereby helping to mitigate potential biases from unobserved confounding and non-random sample selection.
Definitions and variables
Dependent variable
The dependent variable is the health of the middle-aged and older disabilities, which is assessed through the activities of daily living (ADL). This is primarily due to the fact that the majority of disabled individuals in China are physically disabled, as illustrated in Figure 4, which presents the time trends in the number of people with different types of disability. ADL consists of six key activities: can or can’t dress (Dress), bath (Bath), eat (Dine), getting in and out of bed (Get-up), go to the toilet (WC), and pee and poo (Relieve), independently.24,25 To assess ADL, each activity is assigned a value of 1 if the individual is able to perform it independently without assistance. Scores for all six activities are then added together. The total score ranges from a maximum of 6, indicating complete independence in all activities, to a minimum of 0, indicating that assistance is required for each activity. Furthermore, annual medical expenditures (AME) are employed as an ancillary proxy variable for HED, in order to ascertain whether enhancements in health are not accompanied by elevated medical expenditures.

Time trends in the number of people with different types of disability in China.
Key independent variable
SCC was taken as the key explanatory variable, represented by the dummy variable SCC. Given that the Ministry of Housing and Urban-Rural Development selected three batches of SCC pilot lists between 2012 and 2014, we adopted a double machine learning model. We treat the three batches of SCC pilots as a quasi-natural experiment, with these three years serving as the respective time points for the policy shock affecting each batch of pilot cities. If a city implements the pilot policy after its designated policy processing time point, the SCC takes the value of 1; otherwise, it is 0.
Control variables
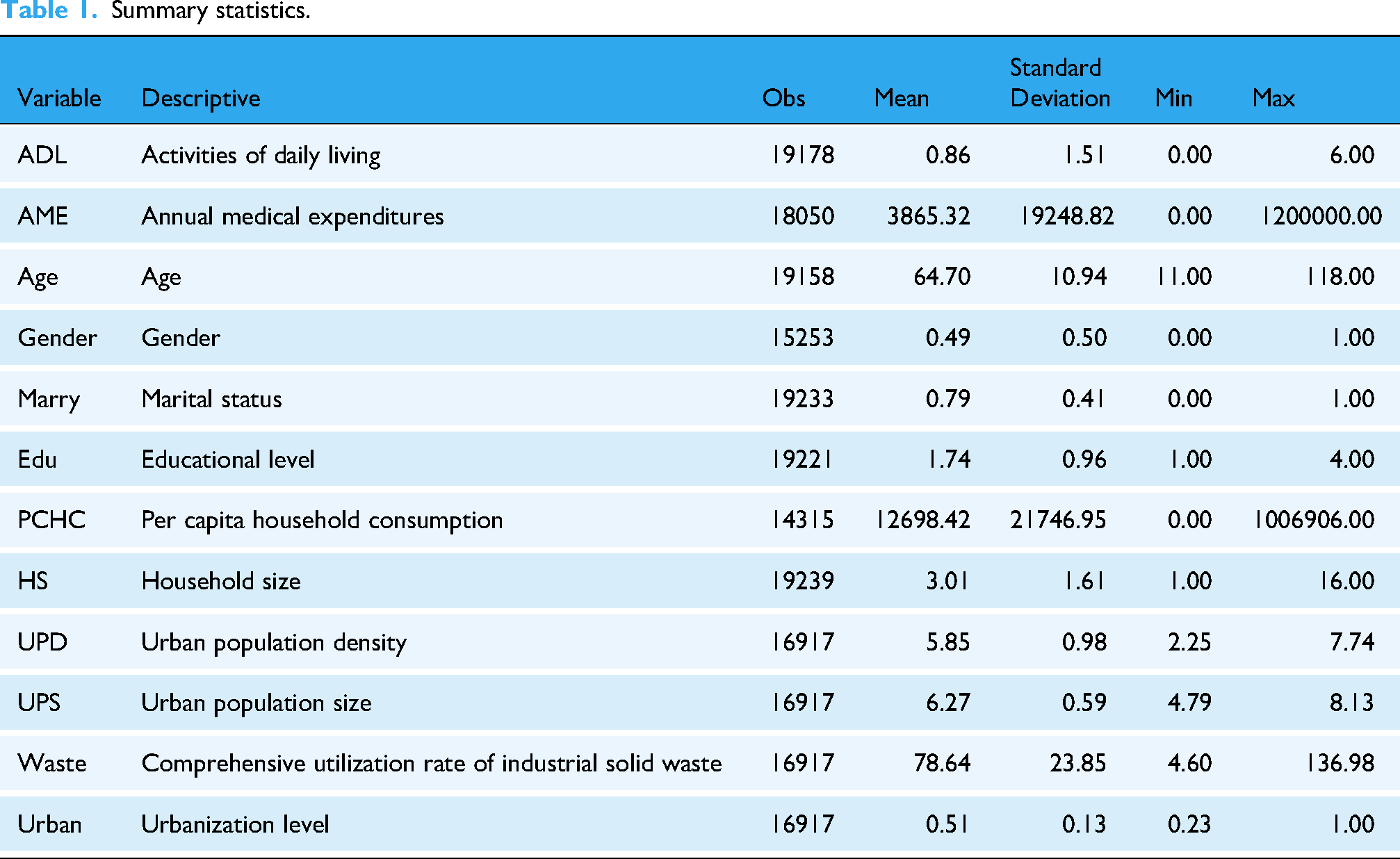
Double machine learning, equipped with its regularization algorithm, can effectively tackle the issue of high-dimensional control variables. Consequently, to ensure the accuracy of policy effect estimation, this paper, while consulting relevant materials and considering the availability of household data, also accounts for other factors that may influence health.26–28 At the individual level, the control variables are primarily selected based on the characteristics of the household head, encompassing gender (Gender), age (Age), marital status (Marry), and education (Edu). At the household level, the following control variables were selected: per capita household consumption (PCHC), household size (HS). At the city level, the following variables are controlled: urban population density (UPD), urban population size (UPS), comprehensive utilization rate of industrial solid waste (Waste), and urbanization level (Urban). The individual and household data used above are all sourced from CHARLS database, and the city data above are all sourced from Chinese Urban Statistical Yearbook. In addition, this paper includes the quadratic terms of continuous variables in regression analysis to enhance the precision of fitted model. Furthermore, to mitigate information loss across cities and time periods, individual-specific and year-specific fixed effects are introduced through the use of dummy variables. Descriptive statistics of selected key variables are reported in Table 1.
Summary statistics.
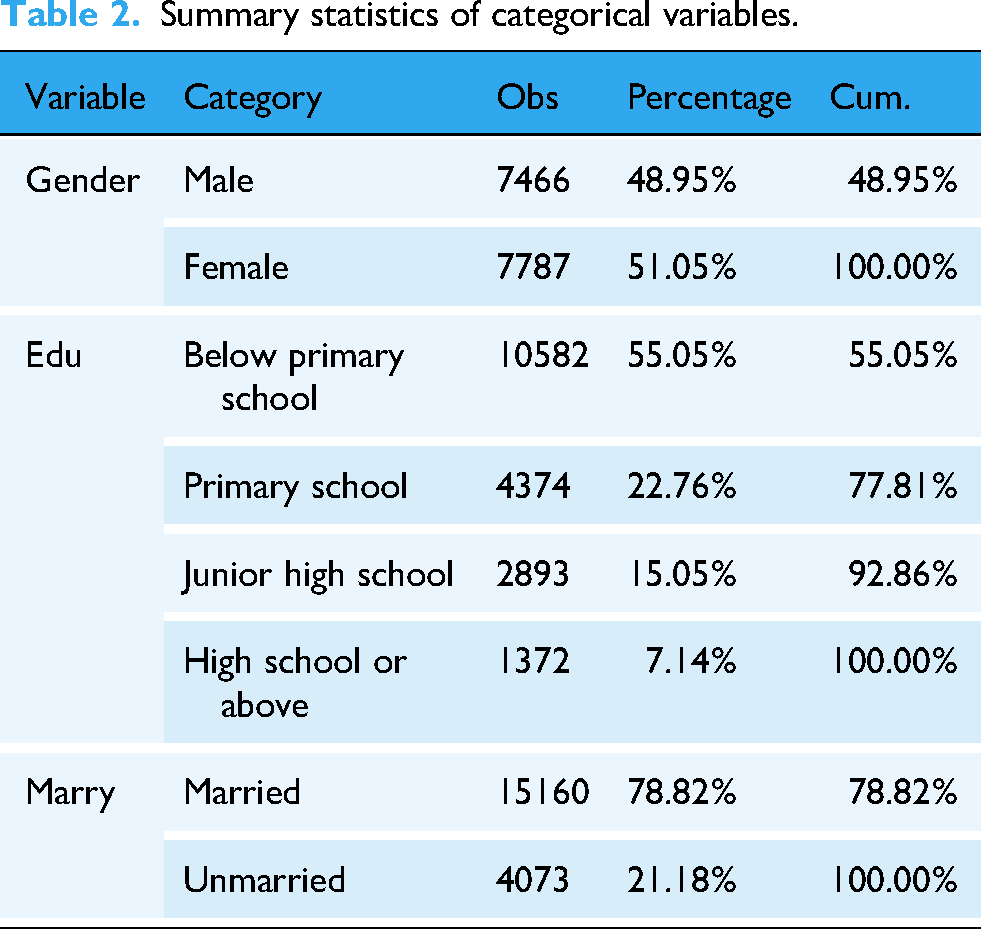
To ensure proper handling of categorical variables in the double machine learning framework, we applied dummy encoding before model fitting. Gender was encoded as a binary variable (Male = 0, Female = 1); Marry as a dummy indicating marital status (Married = 1, Other = 0); and Edu was recoded into a multivariate indicator based on original values: Below primary school = 1, Primary school = 2, Junior high school = 3, High school or above = 4. 53 This approach avoids imposing artificial order and aligns with best practices in causal machine learning. The summary statistics of categorical variables is shown in Table 2.
Summary statistics of categorical variables.
Model setting
Double machine learning
This paper focuses on the application of double machine learning in economics, which has already been utilized in policy evaluation in existing research.29,30 It serves as a model for estimating treatment effects.
31
In contrast to traditional policy evaluation methods (such as difference in differences and synthetic control), this model relaxes the linear assumption constraints between variables, allowing for nonlinear and interactive effects among them, which aligns more closely with policies and economic environments in the real-world economy. Furthermore, this method can accurately estimate causal relationships even when confronted with numerous control variables, thereby offering unique advantages in policy causality analysis. Consequently, this paper employs it to assess the impact of SCC on HED. The specific model is outlined in equations (1) to (2).

HED represents the health of middle-aged and older disabilities; SCC is a policy dummy variable indicating the policy of SCC, with a value of 1 after the pilot program is set up and 0 otherwise. Its coefficient θ0 reflects the promotional effect of SCC on HED; X represents control variables; U and V are disturbance terms; i represents respondent; t represents the time. The estimation order is as follows:
First, we proceed with the first-stage estimation and equation (1) serves as the primary regression model. By directly estimating equation (1), we derive the estimator for θ0 as follows:

The estimation bias is:
Where θ0 represents the sample size, and let
To obtain unbiased processing results, an auxiliary regression formula (2) is constructed based on the main regression for a second-level estimation. Specific steps are as follows:
Firstly, perform a regression on the auxiliary formula (2), estimate
Second, we conduct regression for the main regression formula (1) with the same method and estimate 
Third, we use the residuals 
The estimation bias is:
Similarly, let 
The speed at which b tends to zero depends on the speed at which
To mitigate overfitting and ensure the empirical validity of our estimates, we adopt the cross-fitting strategy, combined with multiple robustness checks. 31 We vary the sample-splitting ratio (1:2, 1:4, 1:7), replace the base learner (random forest) with lasso and neural networks, and extend the partially linear double machine learning model to a more flexible interactive form. These steps confirm the stability of our results across model specifications, data partitions, and learning algorithms. Hyperparameters were tuned using 3-fold cross-validation within each training fold. These procedures jointly ensure that double machine learning estimator achieves orthogonality, resists overfitting, and aligns with theoretical convergence guarantees.
Event study
To alleviate concerns about parallel trends and explore the dynamic trends of SCC impacts on health, we employ event study for validation.
32
We test whether time trends in ADL remain consistent between treatment and control before policy is implemented. We also observe the dynamic effects that occur after SCC implementation.
33
The construction of event study method is described in equation (9).
Results
Baseline estimation
This paper estimates the policy effect of SCC on the health of middle-aged and older disabilities using double machine learning model, with a sample splitting ratio of 1:2. The Random Forest algorithm is adopted to predict and solve the main and auxiliary regressions. The regression results are presented in Table 3. Model (1) controls for the fixed effects of households and time, as well as the first-order terms of other urban variables across the full sample range. It is found that the regression coefficient of the SCC policy on ADL is 0.65 and is statistically significant at 1% level, indicating that the SCC policy has a positive impact on the middle-aged and older disabilities. Specifically, compared to the sample mean of 0.86 for ADL, the SCC policy has enabled an additional 0.65 activities to be performed independently by individuals with disabilities in the treatment group. Consequently, the mean ADL score for the sample of individuals with disabilities who received the SCC intervention is the sum of 0.86 and 0.65, amounting to 1.51. This suggests that, on average, these individuals are now able to perform 1.51 out of the six ADL activity indicators without requiring assistance. Based on Model (1), Model (2) further controls for the second-order terms of urban variables, and the regression coefficient remains significantly positive with little change in value.
The baseline estimation results.
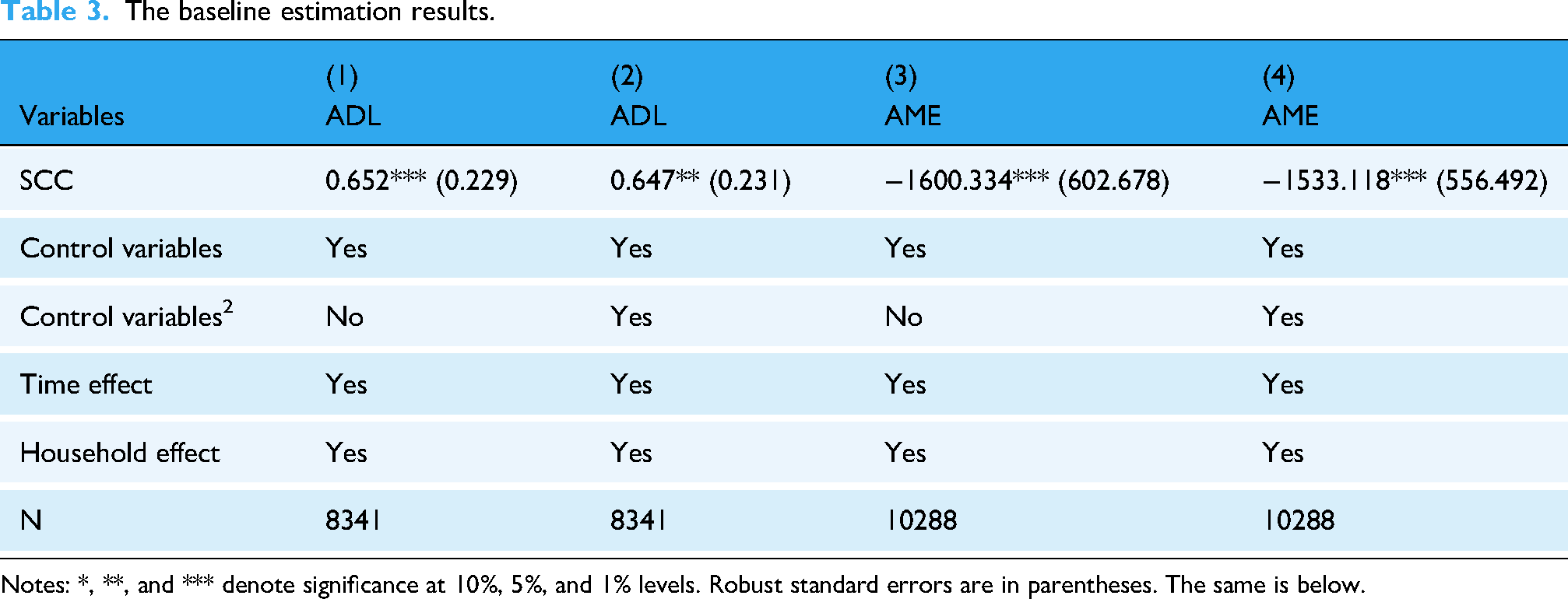
Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels. Robust standard errors are in parentheses. The same is below.
Models (3) and (4) in Table 3 show the effect of SCC on AME, with or without controlling for the secondary term, respectively. According to model (4), the implementation of SCC leads to a decrease of 1533.118 yuan in AME for middle-aged and older disabilities. This suggests that improvements in the health of the disabled do not lead to higher medicine expenditures, but rather a reduction in healthcare costs due to the better health of the disabled.
To further explore the specific impacts of SCC on various dimensions of ADL, Table 4 presents the regression coefficients of SCC on Dress, Bath, Dine, Get-up, WC, and Relieve, respectively. The SCC policy significantly improves Dress, Dine, Get-up, and WC. Conversely, the impact of SCC on Bath and Relieve is negligible, suggesting no significant effect on bathing and urinating and defecating independently. This may be due to the fact that improvements in these specific activities require more targeted interventions beyond the scope of the current SCC policy. 34
The impact of smart city construction on ADLs (classified).

Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
Dynamic trends of SCC impacts on health
Figure 5 shows the estimated coefficients βk for health effect of SCC using event study method. Vertical line indicates year prior to the implementation of SCC policy. The estimation results of the event study in Figure 5 are shown in Table 5. It can be observed that, regarding ADL, estimated coefficients are not significant (p-values for D_2 and D_1 are 0.338 and 0.615, respectively) and show no obvious trend before the implementation of SCC policy. None of estimated values exhibit a more obvious trend during this period, which suggests that parallel trend assumption is satisfied. After the implementation of SCC policy, absolute values of estimated coefficients changed significantly (p-values for D1 and D2 are 0.024 and 0.018, respectively). This indicates that individuals’ ADL changed significantly after the implementation of SCC demonstration policy, supporting results of baseline regression. The estimated coefficient of 0.216 for D2 is greater than the estimated coefficient of 0.207 for D1. In the long term, the positive impact of SCC on their health is increasing year on year, demonstrating the continued and enhanced role of digital inclusion and infrastructure optimization in improving the health and wellbeing of vulnerable groups.
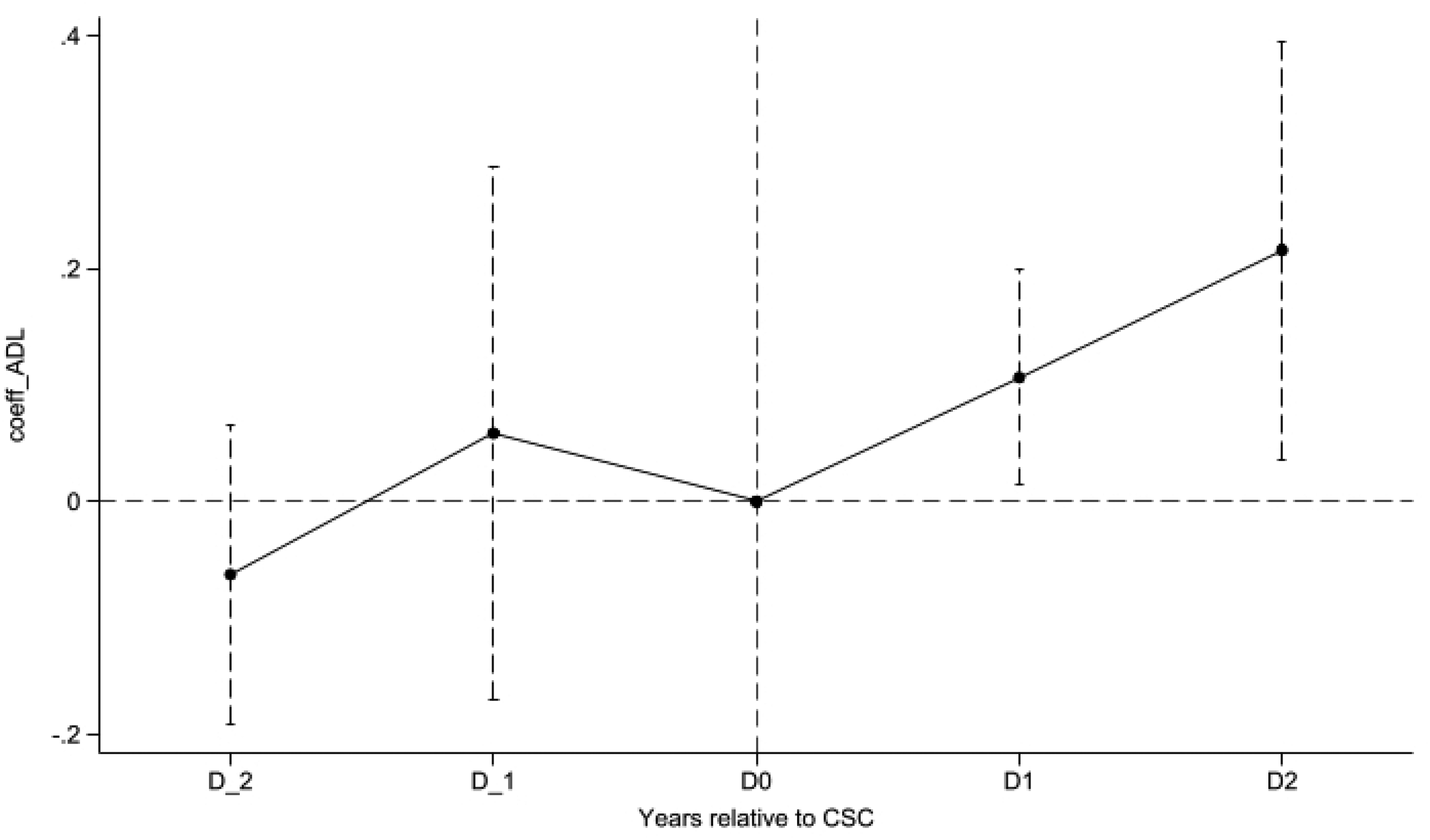
Dynamic trends of CSC impacts on ADL.
Estimated results of the event study supporting Figure 5.

Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels. D_0 is omitted. We drop dummy variables for the first year in which the SCC event occurred so that βk specifically captures the change in the treatment outcome variable, Yijct, relative to the baseline difference observed at k = 0, compared to its counterfactual counterpart.
Notes: Figure 5 displays the βk from equation (9) and it's 95% confidence intervals. Coefficients at k = 0 are normalized to zero. D_1∼TED_2 represents the first through the second wave before the operation of SCC; D0 represents current wave of the SCC's implementation; D1∼D2 indicates the first to second wave following the SCC's implementation. Detailed data results for Figure 5 are detailed in Table 5.
Robustness test
Sample selection bias
First, as one of the most economically developed regions in China, the Yangtze River Delta (YRD) region has distinct structure of the medical industry and demands compared to other regions. 35 However, as shown in Figure 6, the number of persons with disabilities in the YRD region of eastern China is in the middle to upper range of all provinces in China. These differences could either mask or exaggerate the actual impacts of SCC policy on their health. Second, the YRD region is characterized by rapid economic development, advanced digitalization and smart technologies, and a greater likelihood of implementing high-level SCC. 36 These factors could significantly influence the overall health outcomes of SCC. To avoid potential sample selection bias, we exclude the YRD region from the sample. Results in Table 6 (column 1) show that the exclusion of the Yangtze River Delta region did not substantially affect the estimation results.

Spatial distribution of the numbers of disability.
Robustness test I.

Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
Short-term effect
The 5-wave research samples for baseline estimation span from 2011 to 2020, yielding an average treatment effect estimate spanning 10 years through the double machine learning approach. However, an excessively long sample period may expose the estimation results to potential influences from other concurrent policies. Consequently, this paper reselects a sample period from 2011 to 2018, spanning 8 years before and after policy implementation, to verify the stability and consistency of policy effect in the short term. Result is shown in Table 6 (columns 2). Compared to benchmark estimation results, the impact of SCC on ADL has slightly decreased, yet estimated coefficient of policy dummy variable remains significantly positive. This indicates that, while shortening the sample period and disregarding the effects of concurrent policies may introduce subtle fluctuations in the estimated coefficient of the policy dummy variable, this approach does not alter the fundamental conclusion.
Eliminate concurrent policy interference
Another criticism of the baseline estimation lies in the inevitable interference from other concurrent policies when validating the policy effect of SCC on their health. To ensure a precise estimation of policy effect, this paper controls for other similar policies implemented during the same period. Broadband China strategy, initiated in 2013, represents a significant strategic adjustment to the country's informatization development, providing essential information infrastructure for digitalization and intelligent construction. Regarding improving natural environment, social environment and health services, China implemented the healthy cities pilot policy. Consequently, this paper introduces policy dummy variables for broadband China strategy (Bandwidth-China) and healthy cities pilot policy (Healthy-cities) into regression analysis. Regression results are presented in Table 6 (columns 3-4). After eliminating the influence of these two concurrent policies, the significance of SCC's policy effect remains unchanged, sufficiently demonstrating the robustness of baseline estimation.
Reset the double machine learning model
To avoid the influence of potential biases in double machine learning setup on the conclusions, this paper verifies the robustness of baseline estimation from the following aspects. Firstly, the sample splitting ratio of double machine learning is altered from previous 1:2 to 1:4 and 1:7, in order to explore the potential impact of these different sample splitting ratios on baseline estimation. Secondly, machine learning algorithm is replaced, switching from previously used random forest algorithm for prediction to lasso regression and neural network algorithm, in order to investigate potential influence of these alternative prediction algorithms on baseline estimation. Thirdly, acknowledging the subjective nature in the specification of partially linear model constructed based on double machine learning in the benchmark regression, this paper employs double machine learning to build a more general interactive model. This step aims to explore the impact of model specification on baseline estimation. Main and auxiliary regressions used for analysis have been modified as follows:

The estimated coefficient of the treatment effect obtained from interactive model is:
In the aftermath of revamping double machine learning architecture, Table 7 (columns 1-5) reveals the updated regression outcomes. It is noteworthy that baseline estimation retains its robustness, unaffected by alterations in the sample division proportions within double machine learning model, the selection of predictive machine learning methodologies, or the modifications to the model estimation schema. These modifications simply introduce subtle adjustments to the extent of policy influence, thereby further substantiating the authenticity and reliability of baseline estimation.
Robustness test II.

Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
Instrumental variable method
The econometric model developed in this paper accounts for the issue of endogeneity, which may arise from several sources. First, a bidirectional causal relationship could exist between the SCC and the health of middle-aged and older disabilities. Specifically, the health needs of disabled individuals may prompt the government to design and implement policies aimed at improving accessibility, such as expanding accessible infrastructure or enhancing telemedicine services.
37
Second, while this study controls for a range of variables affecting the health of the target population, the potential for omitted variable bias remains, especially in panel data settings. To address the endogeneity concerns and mitigate their impact on the empirical results, this paper employs the use of pilot batches as an instrumental variable. Pilot batches are closely linked to SCC, as pilot cities typically take the lead in implementing relevant policies. Thus, there exists a strong correlation between the pilot batch and policy implementation, fulfilling the necessary condition for the correlation between endogenous variable and instrumental variable.
38
Furthermore, the selection of pilot batches is primarily determined by factors such as economic development and population size, rather than their health status, thereby satisfying the exogeneity assumption. In light of these considerations, this paper constructs double machine learning partially linear instrumental variable model to test for endogeneity.

Results of instrumental variable approach are presented in Table 7 (column 6). The model builds upon the previous basic regression, utilizing the random forest algorithm to predict and resolve both the main and auxiliary regressions. Cross-validation is performed with a sample split ratio of 1:4, dividing the data into training and validation sets. The results indicate that, after incorporating the instrumental variable, the regression coefficients remain positive and statistically significant at 1% level. Furthermore, findings from baseline estimate remain robust and unchanged.
To fully illustrate how the instrumental variable satisfies the exclusion restriction, we provide a falsification test on the instrumental variable. We reassigned the SCC implementation year for pilot cities to an earlier placebo period (i.e. pre-2010, before the actual rollout of SCC policy). If the instrument is invalid or correlated with other unobserved health-related trends, we would expect to observe a spurious treatment effect in this placebo setting. The result of falsification test is shown in the column 7. It shows no statistically significant impact of the placebo SCC treatment on ADL, supporting the validity of our identification strategy. This helps reinforce the claim that SCC affects ADL primarily through the implementation of SCC rather than other confounding channels.
Discussion
Channel
Identifying the mechanism of how SCC affects the health of middle-aged and older disabilities is a challenging task. One potential channel is living infrastructure. Through the integration of advanced technologies and innovative management strategies, SCC enhanced the efficiency and accessibility of living infrastructure, thereby positively impacting their quality of life and health.39–42 The intelligent transformation and barrier-free design of this infrastructure not only improve the daily convenience for disabled but also promote their physical and mental health as well as social participation. 43 Another possible channel is income and gift. SCC directly fosters improvements in family economic conditions and can also indirectly transform gifting patterns through digitalization, allowing middle-aged and older disabilities to receive more financial support from their children.44,45 In this process, the increase in family income and the shift in children's economic contributions, as key factors, work together to enhance the quality of life and health of middle-aged and older disabilities, thereby demonstrating the positive role of SCC in improving social well-being.46,47 To this end, the two channels are empirically analyzed in this section.
Living infrastructure
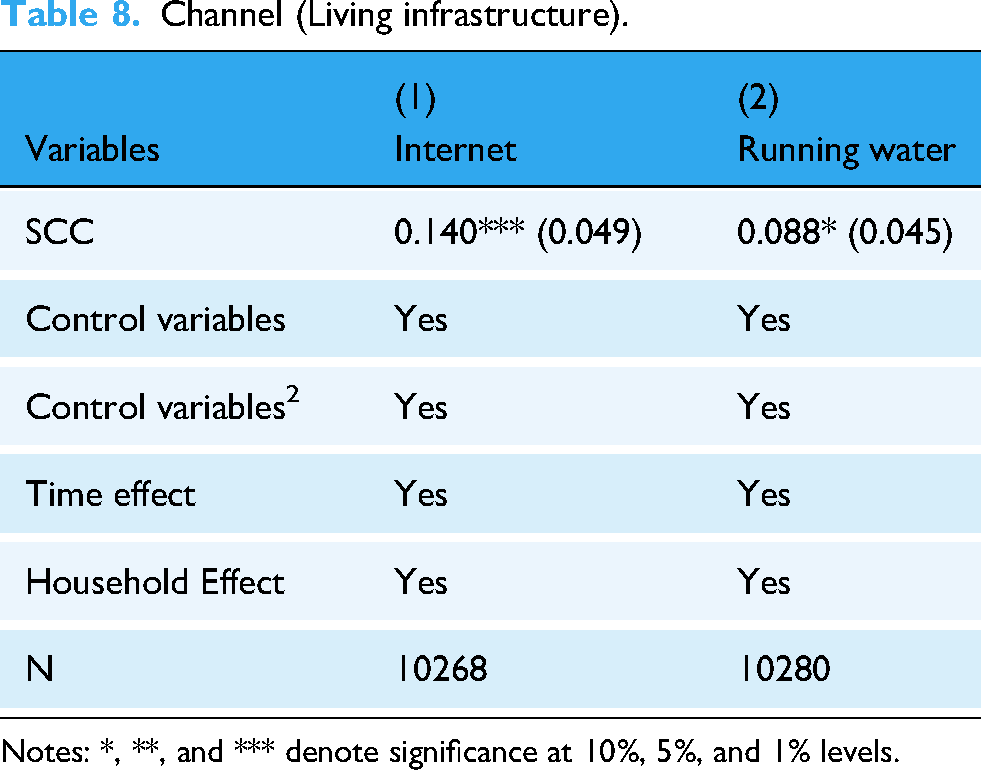
This paper examines whether SCC affects the health of middle-aged and older disable through the transmission mechanism of living infrastructure. To this end, the presence of internet access (Internet) and running water (Running water) in a household are used as proxy variables for living infrastructure, and regression analysis is conducted using the baseline model. The results in Table 8 (columns 1-2) show that coefficients of the regression terms are 0.140 and 0.088, respectively, both significant at the 5% level. These findings provide evidence that SCC has significantly improved the accessibility of the Internet and tap water in households of middle-aged and elderly individuals with disabilities, thereby enhancing living infrastructure and improving their health.
Channel (Living infrastructure).
Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
Income and financial support
To test whether SCC affects the health of middle-aged and older disabilities through the transmission mechanism of income and financial support through intergenerational transfers, this paper uses household annual income (Income) as a proxy for income and children's random gift (Random gift) and fixed financial gifts (Fixed gift) to their parents as a proxy for financial support through intergenerational transfers and conducts empirical analysis. Fixed gift is measured by the total amount of money that parents regularly receive from their children in the past year. Random gift is defined as the total amount of money that parents received irregularly from their children in the past year (excluding regular transfers). Results are presented in Table 9. Regression coefficient in the first column is 23,438.98, significant at 5% level, indicating that SCC increases the annual household income of middle-aged and older disabilities by 23,438.98 yuan. The regression coefficients in column 2-3 are positive, suggesting that SCC increases financial gifts from children to their parents. Although the channel of children's financial gifts to their parents is not statistically significant, the positive estimated coefficients suggest a potential role for such support in promoting health. These findings demonstrate that SCC can enhance their household income, thereby may be providing financial support for their health improvement.
Channel (income and gift).

Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
Unequal selection effects
To examine whether there are unequal selection effects of sample characteristics in the health effects of SCC on middle-aged and older disabilities, and to provide a more nuanced design framework for the practice of SCC and its impact on their health, this paper conducts a heterogeneity test from the perspectives of retirement (including retirement status and age) and household composition (including marital status and children).
Retirement
In theory, non-retired individuals with disabilities are more likely to benefit from SCC in terms of health improvements, given their higher levels of daily activity and greater receptiveness to new technologies. 48 Not only are they more likely to actively seek out and utilize the convenience services offered by smart cities, but they can also leverage these services to more effectively promote their physical and mental health, as well as their full integration into society. 49 Based on this reasoning, we hypothesize that the impact of SCC on their health will vary by retirement status. To test this hypothesis, the study sample is divided into two subsets—retired and non-retired—and regression analyses are conducted separately. The results are presented in Table 10 (columns 1-2). The analysis shows that SCC has a more significant positive impact on the health of non-retired individuals with disabilities compared to the retired population. However, since most rural populations in the Chinese context do not adhere to a conventional retirement model, we use age 60 as a proxy for retirement status to further validate the findings. 50 The results, shown in Table 10 (columns 3-4), indicate that individuals with disabilities under 60 years old experience more substantial health improvements. Therefore, SCC appears to have a more pronounced impact on the health of non-retired individuals with disabilities than on retired individuals.
Selection effect (Retirement and age).

Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
Household composition
There are significant differences in household composition among individuals with disabilities, and a more supportive household composition provides both emotional support and practical assistance in daily life for middle-aged and older disabilities, thereby enhancing their ability to cope with life's challenges. 51 To examine the differential impacts of household composition on health improvement of middle-aged and older disabilities in the context of SCC, this paper conducts heterogeneity analyses based on marital status and the number of children. Table 11 (columns 1-2) reports the heterogeneous effects of SCC by marital status, revealing that the health improvement effect of SCC is more pronounced among married middle-aged and older disabilities. Columns 3-4 report the heterogeneous effects of having children, showing that SCC has a more significant health improvement effect among those who have children. These results suggest that health benefits of SCC are greater for middle-aged and older disabilities who have a more supportive household composition.
Selection effect (Marriage and children).

*, **, and *** denote significance at 10%, 5%, and 1% levels. Note: Incorporating the Chinese Marriage Law, we divide marital status into two subsets: married status and other marital statuses (including unmarried, divorced, or widowed).
Welfare analysis
Disease not only affects individuals’ health but also generates a range of indirect effects, such as increased healthcare costs and reduced work performance. Therefore, focusing solely on the health effects of SCC may overlook the broader economic benefits associated with health improvements. To more comprehensively assess the welfare effects of SCC on the middle-aged and older disabilities, and capture the long-term benefits of improved health, this paper analyzes healthcare costs and labor market performance.
On the one hand, assuming that medical costs are a direct consequence of illness, individual AME is used as the dependent variable, with regression results reported in Table 12 (column 1). The results show that SCC significantly reduces medical expenses. Specifically, compared to non-SCC pilot cities, the AME of those in SCC pilot cities are reduced by approximately 1533.118 yuan on average. On the other hand, assuming that labor market performance is an indirect effect of illness, the regression results are presented in columns 2-3, using job loss due to illness (Job-Leave) and annual wage (Wage) as explanatory variables. These results indicate a significant reduction in sickness-related unemployment. Additionally, compared to non-SCC pilot cities, the annual wages of those in SCC pilots increase by an average of approximately 23,438.980 yuan.
Welfare analysis.
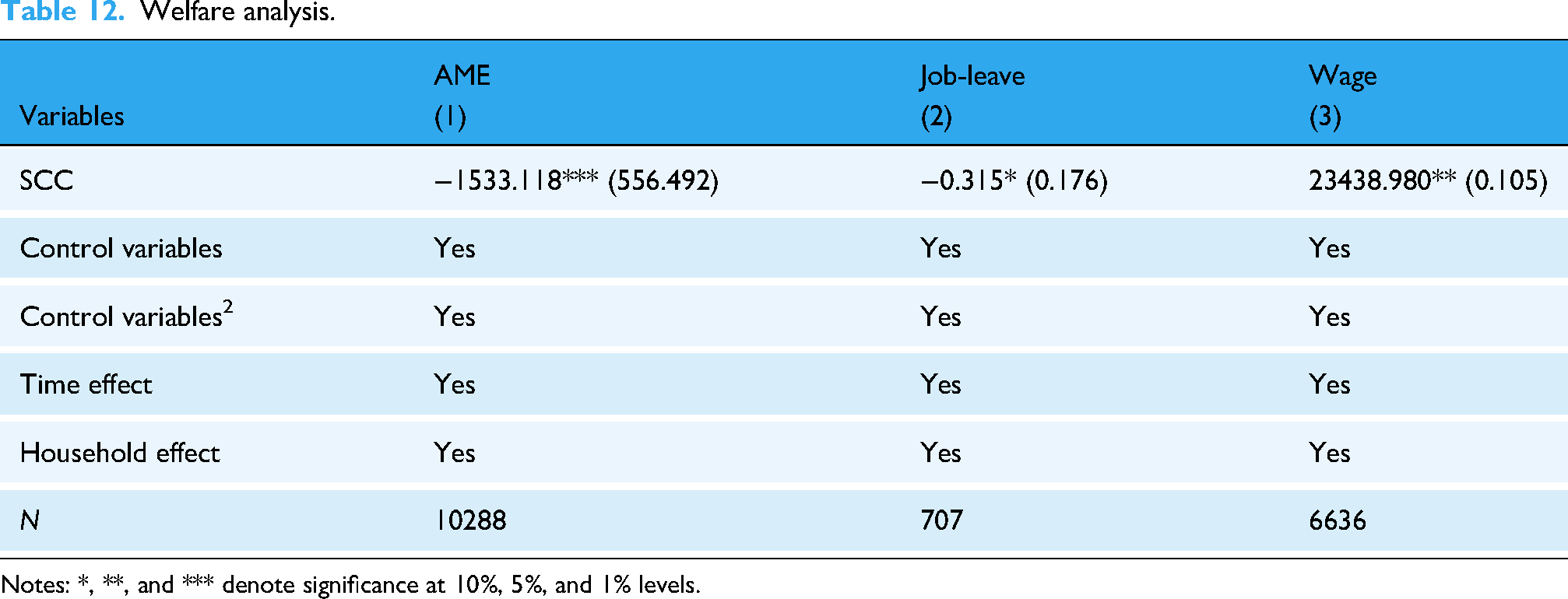
Notes: *, **, and *** denote significance at 10%, 5%, and 1% levels.
It should be noted that the above analysis provides a conservative estimate of the individual welfare effect of SCC, amounting to US$3448.65 (24,972.098 yuan). This estimate primarily reflects direct measurable effects, as other hidden costs associated with illness—such as emotional distress, reduced productivity, and long-term health consequences—are difficult to observe and quantify. Therefore, the welfare effect presented here represents a lower bound, and when these additional factors are considered, the overall benefits of SCC on middle-aged and older disabilities may be even greater.
Limitation of the study
Despite the robustness of our findings and the comprehensive methodological approach adopted, several limitations should be acknowledged. First, due to the centralized designation of pilot cities by the government, SCC implementation is treated as a binary variable. While variation in intensity could provide additional insight, consistent and comparable data on implementation strength across cities and years are not available, which remains a potential direction for future research. Second, our analysis focuses primarily on middle-aged and older disabilities, limiting the generalizability of the results to other vulnerable or marginalized populations who may experience different barriers or benefits from SCC-related interventions. Finally, while we identify key mechanisms such as infrastructure accessibility, household income, the study doesn’t capture potential psychological or community-level mediators, which could also play a role in shaping health outcomes in digitally transforming environments. Future research should consider integrating more granular policy implementation data, leveraging qualitative methods to uncover deeper social dynamics, and extending the analysis to other population groups and health dimensions to build a more holistic understanding of SCC's inclusive impact.
Conclusion
As the digital wave reshapes the future of cities, SCC is emerging as a key driver for improving public health and bridging social gaps through its inclusive power. Based on the SCC policy, we utilized CHARLS database and employed double machine learning method to examine the impacts of SCC on the health of middle-aged and older disabilities and its dynamic effect. Furthermore, we explore the underlying mechanisms and heterogeneity of these effects to provide a comprehensive understanding of the inclusive potential of digitalization.
The results indicate that SCC significantly enhances the health of middle-aged and older disabilities, and the improvement in health doesn’t come at the expense of increased healthcare spending. In the long term, the positive health effect increases year by year. The baseline estimation passes a series of robustness tests, including event study, sample selection bias, short-term effect, eliminate concurrent policy interference, reset the double machine learning model, and instrumental variable method. Mechanism analysis reveals that SCC promotes health improvements through three key channels: enhancing the accessibility of living infrastructure, increasing household income. Heterogeneity analysis reveals that there are unequal selection effects in impact, the health-enhancing effects of SCC on middle-aged and older disabilities are more pronounced among non-retired individuals and those with a more extensive household composition. Finally, welfare analysis shows that SCC reduced their health-care expenditures and improved labor market performance, with a conservatively estimated welfare benefit of US$3448.65.
In light of our empirical findings, policymakers should focus on three targeted areas to maximize the inclusive health impact of SCC for middle-aged and older disabilities. First, SCC is found to significantly improve ADL without increasing healthcare expenditure, and our welfare analysis estimates a substantial benefit of US$3448.65 per person. This suggests that increased investments in accessible infrastructure and community-based digital health services can be both cost-effective and welfare-enhancing. Second, the channel analysis highlights that SCC promotes health by improving infrastructure accessibility and increasing household income. Thus, complementary policies such as subsidies for co-residential caregiving and digital financial inclusion programs could further strengthen these effects.54,55 Third, heterogeneity analysis indicates that the health benefits are more pronounced among non-retired individuals and those in larger households. Therefore, targeted employment support and policies promoting digital literacy among vulnerable subgroups are critical to ensure equitable access to SCC's benefits.56,57 Collectively, these empirically-based recommendations support a more inclusive and health-promoting SCC.
Footnotes
Abbreviations
Acknowledgments
The authors would like to thank the communities and their residents for their kind cooperation and for facilitating the development of this study.
Ethics approval and consent to participate
The Liaoning University and Peking University Biomedical Ethics Committee approved this study (IRB00001052-11015) and waived informed patient consent owing to the use of deidentified data. The research process complies with the Declaration of Helsinki.
Author contributions
HZ, QL, and ZC contributed to the conception and design of the work. HZ performed the analysis and interpretation of the data and drafted the work. HZ and ZC provided substantial review and editing for content. All authors have reviewed and agreed to the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.