
Abstract
The development of information society has deeply changed the style of the healthcare service delivery and medical information access. This study aims to investigate how the information society development affects the efficiency of healthcare system in China, and explore provincial disparities in the impact. Based on the two-stage Data Envelopment Analysis (DEA) framework, this paper uses a panel data from 31 Chinese provinces from 2014 to 2017 to estimate efficiency of healthcare service and analyze the influence of the development of information society on efficiency. With the information society index (ISI) increased from 0.423 to 0.488 during the sample period, the healthcare efficiency experienced a slight decrease from 0.892 to 0.869. Moreover, the pure technical efficiency (PTE) is much lower than the scale efficiency (SE), and thus is the key to enhance the overall technical efficiency (TE). The time-fixed Tobit regression analysis suggests that information society development leads to a significant increase in PTE, but results in a decrease in SE, and therefore has little effect on TE. Further analysis reveals that the impact differs sharply between low-efficiency and high-efficiency provinces. For the low-efficiency provinces, the TE increases significantly with the development of the information society, mainly due to a considerable increase in PTE. In contrast, the TE decreases for the high-efficiency provinces, mainly caused by a decrease in SE. This paper highlights the importance of information infrastructure investment in healthcare system and the application of emerging information technologies to breakout the time and space boundaries of healthcare services in improving overall efficiency. In inefficient provinces, it is also necessary to properly control the growth of healthcare inputs.
Introduction
With the continuous penetration of information technology in various fields, China has made great progress in the construction of the information society. The level of the information society is measured by the Information Society Index (hereafter ISI), which was first introduced by Internet Data Cooperation (IDC) in 1997 and has been further expanded and widely used in the following decades. ISI was evaluated from four dimensions of social aspects: the information economy, the network society, online government, and the digital life, 1 measuring integrated information development level from the cyber-infrastructure construction, information industry structure, information human resource structure, affordability for information payment, e-government and e-business construction, and the application capability of the information technology in people's work, social contact, and daily life. The ISI has a value range of [0, 1], with higher values indicating higher levels of information society development. According to the value of ISI, the level of information society development is divided into five stages: ISI<0.3, representing absolute information poverty; 0.3≤ISI<0.6, representing the transition stage from the industrial society to the information society; 0.6≤ISI<0.8, representing the primary stage of the information society; 0.8≤ISI<1, representing the intermediate and advanced stage of the information society. A report issued by China National Information Centre in January 2018 shows that all 31 provinces (including provinces, autonomous regions, and municipalities directly under the central government) in China have escaped from information poverty by the end of 2017. Five of these provinces have entered the primary or even intermediate stage of the information society. 2
The development of information society in China has driven continuous reform and innovation in the pattern of medical service provision. 3 The use of telemedicine equipment and online medical services has become common, enabling patients to seek medical information and communicate with their preferred physicians through online portals. 4 They can also make appointments for offline hospital visit if a face-to-face diagnosis and physical examination are necessary. Medicines can be delivered to their homes through online pharmacies. Some with chronic diseases can manage their health conditions through internet-based applications with the help of online physicians.5,6 All these may reduce the number of patients in waiting rooms and save time for doctors, therefore having the potential to improve healthcare efficiency.
The issue of healthcare efficiency and its influencing factors has been extensively explored in the past years. Much work has been done to detect the impact of various environmental, economic, and policy factors on healthcare efficiency.7–9 As a country with a population of 1.4 billion, the issue of healthcare efficiency in China has also received a lot of attention from scholars.10–18 Chen et al. 19 evaluated the efficiency of public hospitals in 31 Chinese provinces and reported an increasing trend of efficiency during 2011–2015 and a decreasing trend thereafter. They found that the hospital's performance was dependent on the operational environment such as government subsidy and insurance policy. Cheng et al. 7 examined the efficiency and productivity of Chinese county hospitals in Henna province during the period of healthcare reform, and found that government subsidy, hospital size, and ratio of nurse to physicians can significantly affect the healthcare efficiency. The study of Wang et al. 20 and Li et al. 21 revealed that the IT investment and the utilization of healthcare information technology (HIT) can improve the efficiency in health sector.
Different from previous studies, this paper investigates how the development of the information society, which deeply changes the type of healthcare service delivery, affects the efficiency of healthcare system. The important feature of healthcare service in information society is the significantly increased ability of patients to seek for the second medical opinion and access high-quality medical resources through a variety of online portals. To obtain authoritative medical advices, patients in the past had to travel thousands of miles to visit renowned hospitals far away from home. This kind of unreasonable patients flow has resulted in the problem of the improper utilization of medical resources, making the healthcare service of some developed regions and renowned hospitals overloaded while the medical resource of the less developed regions are underutilized, 17 and therefore has long been considered as the major cause of the inefficiency of the Chinese healthcare system. 22 Nowadays, online medical services and telemedicine enable these patients to access high-quality medical resources in a more convenient and lower-cost way, thus helping reduce unreasonable mobility of remote patients and improve the efficiency of the healthcare system. Besides, the development of the information society facilitated the technical exchanges and cooperation between medical institutions and doctors in different regions. This may lead to the acceleration of the spread of medical technology across regions and the improvement of technical efficiency in the remote and undeveloped areas.
Even though the development of the information society may have the potential to improve the efficiency of healthcare system, the impact may differ across regions. In the process of the exchange of medical information and technology, the developed regions with advanced medical technology provided the medical technology and resources for undeveloped regions through various informatization platforms, while the latter was mainly the beneficiaries of the medical technology diffusion and technical cooperation. Depending on the different roles (technical exporter and technical importer) of each region, there will be some regional variability in the impact of the development of an information society on the efficiency of healthcare services.
Based on the above arguments, this study aims to investigate how the information society development affects the efficiency of healthcare system in China and to explore the provincial variability of its impact. Specifically, we address the following two research questions: (1) Can information society development improve the efficiency of healthcare services? (2) Are there significant regional differences in the impact of information society development on healthcare efficiency?
To address the aforementioned questions, we collected the ISI and healthcare service data of 31 provinces in China from 2014 to 2017. The pooled Data Envelopment Analysis (pooled-DEA) analysis was first used to calculate the efficiency score of healthcare system of each province. Then the time-fixed panel Tobit regression was conducted to analyze the impact of information society development on the efficiency of healthcare services and the provincial disparities in the impact.
The remainder of this paper is structured as follows. Chapter 2 reviews the relevant literature. Chapter 3 constructs the DEA and Tobit models and explains the relevant variables and data. Chapter 4 presents the results of DEA model and analyses the impact of the development of the information society on the efficiency of healthcare services and its provincial disparities. Finally, we present the main findings and conclude the paper with implications and limitations in Chapter 5.
Literature review
Healthcare efficiency and DEA
The optimal use of healthcare resources in the provision of healthcare services is referred to as "healthcare efficiency." The most popular efficiency analysis approaches used by researchers in the literature on healthcare efficiency were DEA and other DEA-based methodologies. Charnes et al. 23 sought to estimate the productivity and efficiency of public sector and non-profit organizations utilizing numerous inputs and outputs, and they established the nonparametric approach known as DEA. This model, named after the initials of the three authors, is known as the Charnes, Cooper and Rhodes (CCR) model, which simply considers continuous returns to scale (CRS). Following their work, Banker et al. 10 developed a model assuming variable returns to scale (VRS) called the Banker, Charnes and Cooper (BCC) model. Using the BCC model, scale efficiency (SE) and pure technical efficiency (PTE) can be used to decompose the efficiency score (TE). They are related as TE = PTE × SE. A reduction in both PTE and SE leads to a reduction in TE. For an inefficient DMU, we can determine, based on the magnitude of the efficiency values of PTE and SE, whether the inefficiency of the DMU is mainly due to technical or scale factors, thus providing a clear direction for improving efficiency. In the early 1980s, DEA was first adopted by Sherman 24 to measure hospital efficiency of seven US hospitals. Since then, the healthcare efficiency analysis has received extensive attention and has been widely used to evaluate the productive performance of hospitals,25,26 nursing houses,26,27 and healthcare systems. 28 O’Neill et al. 29 and Kohl et al. 25 systematically reviewed studies related to hospital efficiency and found that most early studies came from US and Europe, while in recent years the number of publications from Asia increased vastly. During these years, DEA models have experienced a constant diversification, from the two original BCC 30 and the CCR 23 models to the more complex derivate models such as SBM, 31 Malmquist DEA, network DEA, 32 fuzzy DEA, 33 etc. The combination of DEA model and Stochastic Frontier Analysis (SFA) are recently proposed by some researchers to balance the weakness and strength of each model. 34 Furthermore, On the basis of the efficiency scores resulting from the basic DEA model, the post-DEA statistical analysis could be implemented to address more comprehensive management questions.35,36 For example, Lin et al. 11 conducted a spatial autocorrelation analysis using the efficiency scores to investigate the spatial correlation of health services efficiency.
To conduct a meaningful DEA analysis, the selection of input and output variables is of great importance. Ozcan 37 categorizes the inputs into three clusters, including capital investments, labor resources and Operating expenses. As an important resource for healthcare service process, labor input was generally measured by the number of medical staff, nurses, non-medical staff, overall staff, etc.38–42 The most preferred capital-related inputs included the number of beds and capital assets.43,44 And the inputs related to operating expenses included the total expenditure 35 the total operating cost, 45 etc. As for the output variables, the most common selection was the number of the inpatients and the number of the outpatient visits. 46 Several studies also included quality indicators such as mortality rate as output variables. 43
This article used the fundamental BCC model, which was adapted from earlier studies, to calculate the effectiveness of the healthcare systems in 31 Chinese provinces. The input variables include the number of beds, the number of healthcare professionals, the total amount spent on healthcare, and the total value of healthcare assets. The total number of inpatient and the total number of outpatient visits are the output variables.
Influencing factors on healthcare efficiency
Promoting healthcare efficiency is important to improve social wellbeing. A number of studies have been carried out to detect the impact of various environmental, economic, and policy factors on healthcare efficiency. Previous DEA studies employed various post-DEA methods to test the impact of external factors on efficiency, such as regression analysis, statistical test, resampling methods, correlation analysis, etc. Among these methods, the regression models were reported as the most commonly used post-DEA method, in which the estimated efficiency scores obtained from DEA are regressed on external factors.8,47 Due to the punctured feature of the efficiency scores (ranged from 0–1), Tobit model was considered more suitable than OLS model and widely adopted.7,9,16,48 To compare the health expense efficiency of 21 emerging countries and its determining factors, Zhou et al. 9 conducted the two-stage DEA-Tobit analysis, including in which the research and development (R&D) expenditure, number of physicians, education, GDP per capita, and corruption as the focused influencing factors. The empirical results demonstrated that the increase of R&D expenditure and physicians can significantly enhance the healthcare efficiency, while corruption generated the negative effect on efficiency. Özgen Narcı et al. 49 employed the VRS-DEA model to calculate the technical efficiency of 1103 Turkey hospitals and then analyzed how the market completion, population intensity, health insurance, and physician-to-population ratio affected the hospital technical efficiency. However, only the health insurance ratio indicated the significant positive relationship with hospital efficiency. Cheng et al. 7 and Chen et al. 19 examined the driving forces of Chinese healthcare productivity change at the hospital level and the provincial level, respectively, and found that population density, price of health service, and government subsidy significantly affected health efficiency. Ibrahim and Daneshvar 50 found the healthcare efficiency greatly improved in Lebanon from 2000 to 2015 due to the health system reform. Their research demonstrated that the reduction in expenditure was not necessarily accompanied by the decreased healthcare efficiency, given the technical aspects of healthcare system improved. Moreover, previous literature also reported the significant impact of the hospitals’ non-profit ownership,51–55 the extent of hospital specialization,54,56 poverty, 57 education level,9,16,58,59 urbanization level, 16 unemployment ratio, 59 and population age structure,51,60 even though some researchers came to the opposite conclusions.
As the widely implementation of healthcare information technology (HIT) in health sector, several studies have been conducted to investigate the effect of HIT use on healthcare performance. Li & Collier 61 found that HIT improved clinical quality and hospital financial performance. Wang et al. 20 also reported the positive relationship between IT investment and hospital financial performance. Li et al. 21 conducted a nationwide study in China to estimate how the adoption of HIT affects regional healthcare performance. The results revealed that the HIT utilization can improve the efficiency of the regional healthcare system. However, in their study, the healthcare information technology is limited to EMRs (electronic medical records) and PACS (picture archiving and communication system). The impact of the information society development, which deeply changes the type of healthcare service delivery and promotes the wide application of digital health, remains unanswered. This article aims to fill this gap. Following the prior literature, we adopt the classical two-stage analysis framework, which includes the first-stage BCC-DEA analysis and the second-stage Tobit regression.
Materials and methods
DEA models
DEA is by far the most commonly used model for analysing the efficiency of hospitals and healthcare systems. As in most areas of the economy, the relationship between input use and output in the health sector is not linear. So it is necessary to account for possible variable returns to the inputs used (VRS). 62 In addition, the outputs of a healthcare system are more difficult to estimate and control for the managers of healthcare organizations and healthcare policy makers. Therefore, an input-oriented DEA model is preferable to an output-oriented DEA model. Therefore, in the first stage, we used the input-oriented CCR and BCC models to estimate the efficiency of the provincial healthcare system. The mathematic input-oriented CCR model can be presented as below: 30
Objective function:




In the model, there are j DMUs, and each DMU has i inputs and m outputs.
Then, we add the constraint condition
Objective function:




As defined by Farrell (1957), technical efficiency (TE) refers to the degree to which the production process of a production unit reaches the technical level of the industry. 63 The TE scores calculated from the DEA model ranged between 0 and 1. When TE=1, the production from the DMU is efficient, i.e., producing the maximum outputs with a given inputs or producing a given amount of outputs with a minimum amount of inputs. In our input-oriented model, TE=1 means a province can produce a given amount of healthcare outputs (the number of outpatients and discharged inpatients) with the minimum healthcare inputs. If TE is less than 1, the production is inefficient.
The TE that can be calculated from the CCR model is the overall efficiency, while the PTE calculated from the BCC model refers to pure technical efficiency. When PTE equals to 1, the production is technically efficient, otherwise is technically inefficient. If TE and PTE are not equal, this indicates inefficiency of the scale. The scale efficiency (SE) can be calculated using the Formula (3):

The selection of inputs and outputs is crucial for a meaningful DEA analysis. In previous studies, labor, capital investment and healthcare expense are the main categories of hospital healthcare inputs. 37 Kohl et al. 25 reviewed 262 papers of DEA applications in healthcare and found the number of medical staffs were the most widespread used inputs. The total number of overall medical personnel and other technical personnel were used by Mestre et al. 65 and Baray and Cliquet. 66 Other researches, however, used sub-groups of medical staffs such as physicians, pharmacists, administrative staffs, etc. as input variables.19,67–69 As for the capital inputs, the number of hospital beds, the number of medical equipment such as CT, MR, and other infrastructure were used by Stefko et al., 70 Zhong et al., 18 and Mousa and Aldehayyat 40 to directly reflect the fixed assets investments. Chirikos and Sear 71 use the capital cost for patient care centers and the capital cost for assets, building and land to represent the nonlabor related inputs in hospital production. Hu et al. 51 use the fixed assets to reflect the capital investment and estimate the efficiency of Chinese healthcare system. Li et al. 21 used the net assets input, defined as the assets of the hospital minus all liabilities, and represents the capital size and economic strength. Furthermore, healthcare expense, which represents the operating expenses, was used by Ahmed et al. 72 to measure the efficiency of health systems in Asia, and by Xenos et al., 35 Bulter and Li, 36 Friesner et al., 73 Silwal et al., 42 and Hsieh et al. 74 to measure the efficiency of hospitals in many countries.
Regarding the output variables, the most widely adopted in previous studies were the number of hospital outpatients, inpatients and surgeries. Zhong et al. 18 and Gao & Wang 75 use the number of outpatients and emergency visits, the number of discharged inpatients as the two output variables of DEA model. Chen et al., 19 Sun et al. 76 included the surgical operations as an output variable. Besides, the number of inpatient days, 7 the number of average nursing days 70 were also used. Aside from these most frequently used output indicators, the quality-related outputs have been gradually attracted researchers’ attention in recent years.8,37,77 The healthy life expectancy at birth and the mortality rate were commonly used by many researchers such as Ahmed et al., 72 Tiemann, 78 and Han and Lee. 54
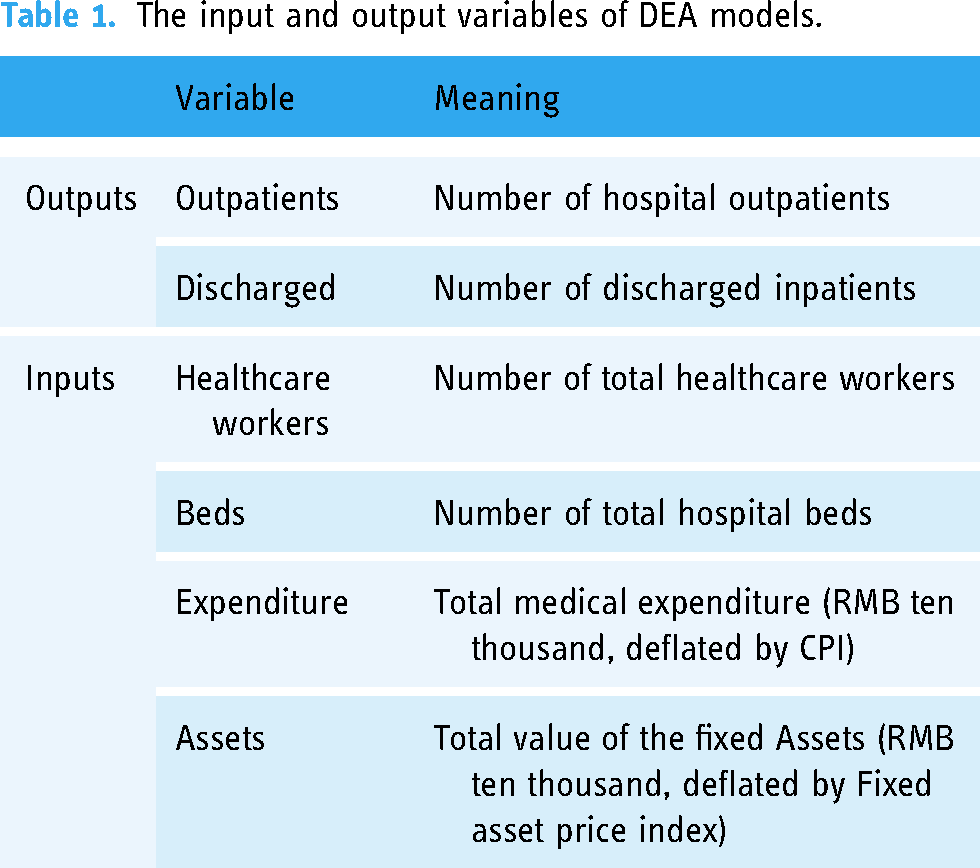
By reviewing the related literature18,22,51 and considering the availability of data, we select four input variables and two output variables. The four input variables are (1) Healthcare workers, i.e., the number of healthcare workers involved in the healthcare production process, including health professionals such as practicing physicians, practicing assistant physicians, registered nurses, laboratory technologists, pharmacists, health supervisors and trainee medical staff; (2) Beds, i.e., the number of hospital beds; (3) Expenditure, i.e., the total medical expenditure includes all expenditure incurred by medical institutions in carrying out medical operations and other activities and financial assistance expenditure; (4) assets, i.e., the total fixed assets value. To eliminate the disturbance caused by price fluctuations, the total medical expenditure and the fixed assets value are deflated by CPI and the fixed asset price index. The output variables used in this study are the number of hospital outpatients and the number of discharged inpatients, which were the most commonly used inputs by previous researchers. Table 1 presents all the input and output variables of DEA models.
The input and output variables of DEA models.
After the TE, PTE, and SE have been calculated, we constructed the year-fixed panel Tobit regression model to analyze the relationship between the information society development and the efficiency of healthcare system (See formula 2).
We also included a series of economic and environmental factors as control variables. The economic factor includes income per capita (income) and inflation rate (inflation rate), which was commonly used in previous studies to control for the impact of economic differences on efficiency. The environmental factors can be further grouped into two groups, i.e., the external environmental factors and the internal environmental factors. The former group includes three factors that are independent of healthcare system, i.e., population density (PopDensity), urbanization level (urbanization), and age structure of population (ratio of youth and older). The latter group includes two factors that are related to the characteristics of the regional healthcare system, i.e., ratio of public hospitals (public) and the cover rate of medical insurance (Insurance). YEAR is a series of dummy time variables that control for the impact of the unobservable time-related variables. All the variables involved in Tobit model are defined in Table 2.
Definition of key variables in Tobit model.

2014 was the starting year of China's online medical development. Since 2014, online medical users have grown rapidly. The level of development of the information society in different regions can partly reflect the cross-regional disparities in digital health environment and the ability of users to obtain medical information and knowledge. Therefore, 2014 is selected as the starting year of the study in this paper. In addition, because the provincial information development level index data (ISI score) has not been publicly released since 2018, this article mainly selects the 2014–2017 data for research, which allowing us capturing the ISI impact on healthcare efficiency improvement. We take the provinces in mainland China as the DMUs. The data of the input and output variables of 31 provinces were collected from the China Health and Family Planning Yearbook 2015–2017 and the China Health Statistics Yearbook 2018. The ISI data were extracted from the China Information Society Development Report 2016 and the China Information Yearbook 2017. The data of control variables in Tobit model were obtained from the China Statistics Yearbook 2015–2018. Ultimately, we have a panel dataset of 31 provinces over a 4-years period from 2014–2017. Table 3 summarizes the input and output variables of DEA model in 2014–2017 separately.
Summary statistics of input and output variables.

Summary statistics of input and output variables.
As Table 3 shows, the healthcare inputs have increased continuously since 2014. To depict the growth trends in healthcare inputs and outputs, we calculated the growth rate of each variable in each year and drew a line graph (Figure 1). Specifically, the mean amount of the fixed medical assets of 31 provinces increased by more than 13% each year, and the annual increase of the number of the medical staff and the number of hospital beds increased by 5%∼7%. Compared with 2014, the mean number of healthcare workers in 2017 increased by about 45000, and the mean value of fixed medical assets increased by more than 50%. However, the considerable increase in inputs has not been matched by the growth of the healthcare outputs on the same scale. Figure 3 shows that the mean number of outpatients and discharged patients only increased by about 3% and 7% each year, respectively. We have also plotted the population growth trend for 2015–2017 in Figure 1. The population growth rate is only 0.5%-0.7%. Therefore, the contribution of population growth to the growth of medical inputs and outputs is limited.

The growth trend of medical inputs and outputs and population in 2015–2017.
Moreover, it should be noted the big difference between the maximum and the minimum values of the input and output variables, which indicates the unbalanced distribution of healthcare resource and healthcare utilization across 31 provinces. Table 4 summarizes the main variables of Tobit model. Note that the difference between the lowest ISI and the highest ISI is about 0.52, indicating the huge gap in terms of the level of information society development across regions. This provides us the potential to observe how the healthcare efficiency is affected by the development of information society.
Descriptive statistics of variables of Tobit model.

Note: The descriptive statistics was calculated based on all sample data in 2014–2017.
Results of the DEA models
We used DEAP 2.1 software to estimate the efficiency scores for each province using DEA models. 79 Two options are considered in this study for dealing with panel data using DEA methods. The first option is to pool the data for all provinces using a DEA model (pooled DEA). In this way, we can construct a global production frontier for all DMUs and compare each province with the most efficient province on this production frontier. Considering the same set of reference DMUs, efficiency scores can be used for both cross-sectional and sequential comparisons.80,81 Another option is to run the DEA model in a separate 4-year period (separate DEA). In this way, we construct four separate production fronts for each year, with each province compared to the best performer in the same year. Given that the reference DMUs differ from year to year, the efficiency scores from the separate DEA are better suited for cross-sectional comparisons over the same period. Logically, the efficiency scores obtained from the separate DEA model may be equal to or greater than those obtained from the pooled DEA model, as each DMU only needs to be compared with the best practice in a single period. 82 Specifically, the efficiency score of the Separate-DEA in a single year may only be equal to the score of the Pooled-DEA if the best performers on the global frontier are all in that year.
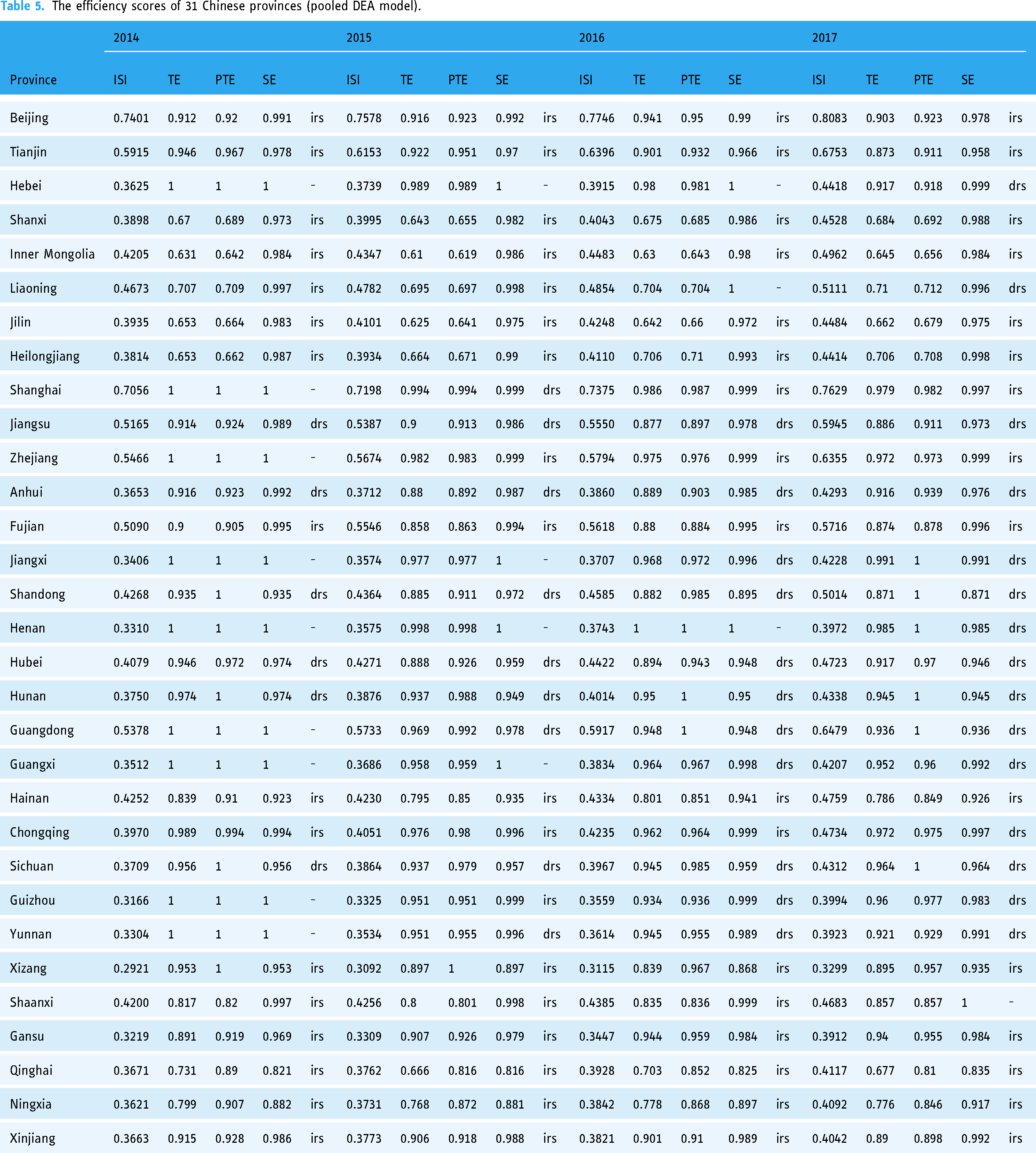
In this paper, we run the pooled-DEA model and the separate-DEA model separately and then compare the efficiency results of the two models. The estimation results of pooled DEA models are presented in Table 5. Table 5 shows that 10 out of all 124 observations (about 8%) were efficient and fell on the production frontiers. They were Hebei (2014), Shanghai (2014), Jiangsu (2014), Zhejiang (2014), Henan (2014, 2016), Guangdong (2014), Guangxi (2014), Guizhou (2014), Yunnan (2014). It can be easily found that most of the efficient DMUs were those from 2014, indicating that productivity may have decreased over time.
The efficiency scores of 31 Chinese provinces (pooled DEA model).
The efficiency scores of 31 Chinese provinces (pooled DEA model).
The performance of healthcare services varies considerably by province. In the 124 observations, 17 (13.7%) had TE scores below a minimum of 0.7. They were Shanxi (2014, 2015, 2016, 2017), Inner Mongolia (2014, 2015, 2016, 2017), Liaoning (2015), Jilin (2014, 2015, 2016), Heilongjiang (2014, 2015), and Qinghai (2015, 2016). These provinces (except Qinghai) have PTE scores below 0.7 and SE scores above 0.97. The results suggest that the relatively low PTE is the main reason for the lower efficiency of healthcare in these provinces.
In addition, we can see from Table 5 that in 2015, 16 inefficient provinces were in a phase of increasing scale returns and 6 were in a phase of decreasing scale returns. In 2017, the numbers were 15 and 15 respectively. 9 provinces experienced a transition from increasing scale returns to decreasing scale returns. They are Hebei, Liaoning, Jiangxi, Henan, Guangdong, Guangxi, Chongqing, Guizhou, and Yunnan. This means that they should control healthcare investment in order to reach efficient scale in the coming years.
To intuitively observe the national trend of efficiency change, we calculated the mean value of TE, PTE, and SE of 31 provinces in each year and then illustrated in Figure 2. As expected, the lines of mean TE, PTE, and SE all showed a slightly downward trend. The mean value of TE decreases from 0.892 to 0.869, although the ISI experienced an increase from 0.423 to 0.489 during the sample period. Moreover, the PTE (around 0.89) is much lower than SE (around 0.97), suggesting that enhancing PTE is the key to improve the overall technical efficiency (TE) in China.
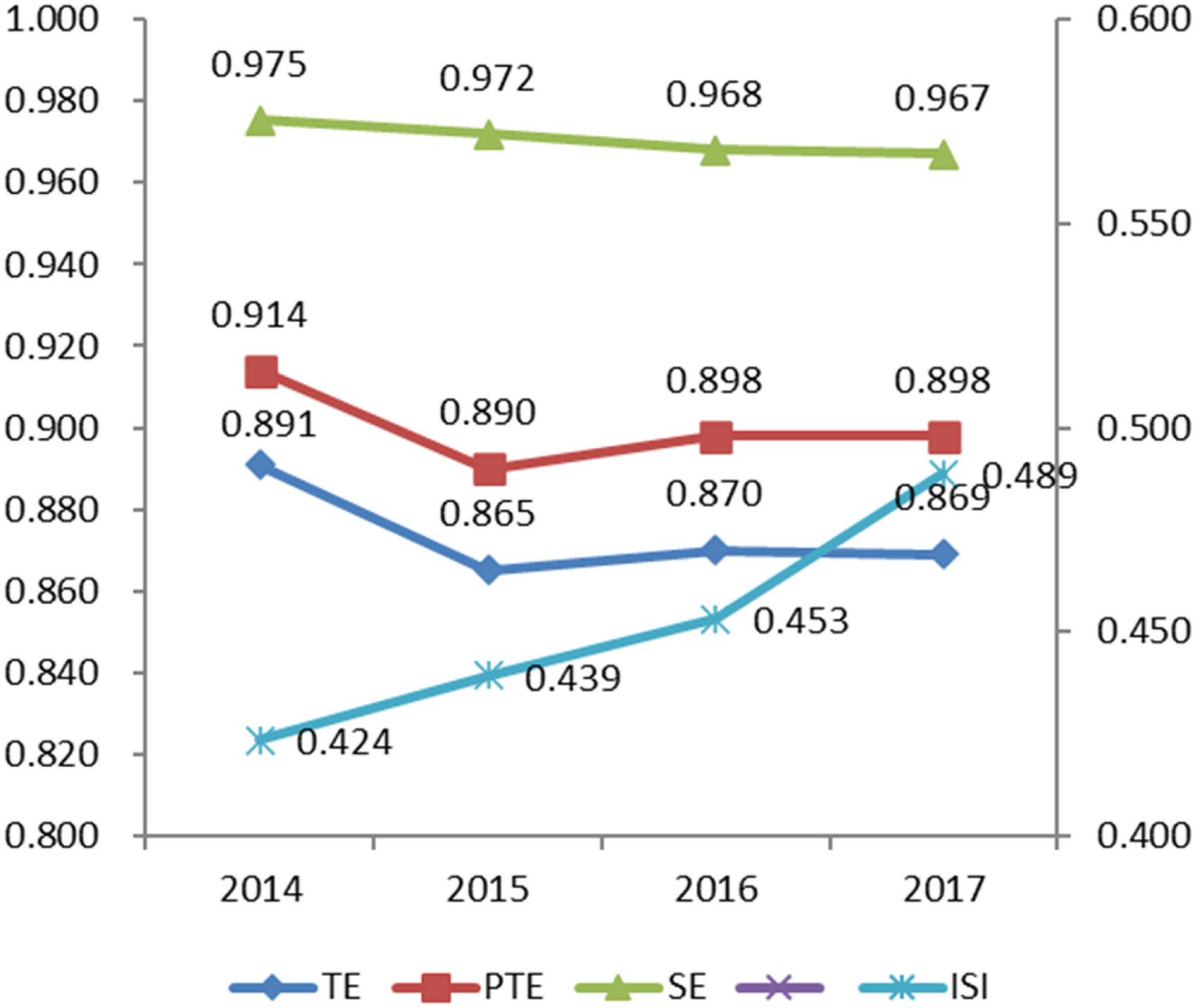
Mean value of te, PTE, se, ISI of 31province from 2014–2017. Note: TE, PTE and SE represented the mean value of technical efficiency, pure technical efficiency and scale efficiency scores of 31 provinces respectively.
We then ran the DEA model on each separate year. To make the table clear, only the TE scores are reported in Table 6. From Table 6, we can see that the efficiency scores of the separate DEA model are higher than those of the pooled DEA model. This is consistent with the results of several previous empirical DEA studies.83–85 The mean value of TE increases each year from 0.892 to 0.910. note that the mean value of TE for 2014 is 0.892, which is roughly comparable to the mean value of the pooled DEA model. The reason for this is that most of the best performers on the global frontier were in 2014. This could also explain why the mean TE for the 2015–2017 individual DEA model is higher than the pooled DEA model ---- When all years are pooled together, the global benchmark for the 2015–2017 DMU may be more difficult to achieve than the individual benchmark for a single year. The results suggest that healthcare efficiency has declined over the four years analyzed. This decline can be explained by China's liberalization of investment in non-government hospitals from 2014 to address the problem of “poor access to healthcare.” 86 A series of policies to encourage private healthcare investment led to an increase in the number of healthcare inputs in the following years. As mentioned earlier, this did not result in the rise of the output at the same rate. As a result, the decline in the output–input ratio led to a relatively lower efficiency score in 2015–2017 than in 2014.
The technical efficiency of 31 Chinese provinces (separate-DEA model).

Despite the decline in efficiency across the healthcare system, this is not a bad thing, as it indicates that the problem of “difficult access” to healthcare in China has been alleviated to some extent. With the increase in healthcare resources per capita, patients’ healthcare needs can be better met and the overall healthcare environment can gradually improve.
To further detect the potential relationship between the efficiency and ISI, we draw a scatter plot (Figure 3) using the efficiency scores and ISI. Figure 3 shows that In general, regions with higher ISI generally have higher efficiency values. The distribution of efficiency scores in areas with lower ISI is relatively complex, suggesting that efficiency scores are more likely to be influenced by other factors. In the next Tobit analysis, we further explore the impact of ISI on healthcare efficiency and its regional variability by adding some columns of control variables to control for the influence of exogenous factors.

The scatter plot of efficiency scores and ISI.
Total impact of information society development on healthcare efficiency
Considering that the DEA results will be used in the Tobit regression analysis (which means that the efficiency score of each DMU will be compared not only with the DUM for the same period, but also with DMUs from different periods), it is preferable to use the efficiency results from the pooled DEA model. The Tobit regression was conducted using all 124 samples with STATA 12.0. The main results are reported in Table 7. The coefficient for ISI in column (1) is negative but statistically insignificant, suggesting that the information society development has little effect on TE. However, further regression analysis reports the weak significant positive coefficient (see column (2)) and strong negative coefficient (see column (3)) for ISI respectively. This means that the development of information society can improve the PTE of Chinese healthcare system but decreased the SE in the meanwhile. Specifically, for every 0.1 increase in the level of development of the information society, PTE increases by 0.046, and SE decreased by 0.037. Given that TE=PTE*SE, and the complete opposite direction of the influence of ISI on PTE and SE, it is reasonable that the ISI impact on TE is insignificant.
Total impact of information society development on healthcare efficiency.

Total impact of information society development on healthcare efficiency.
Standard errors in parentheses ***p<0.01, **p<0.05, *p<0.1
Existing studies on the relationship between information transmission and technology diffusion can well explain the significant positive impact of information society development on PTE. Hayek 87 points out that the diffusion of technology depends to a greater extent on the efficiency of information transmission in society. With the continuous development of information society, the efficiency of information dissemination has been greatly improved and the cost has been reduced, thus accelerating the technology diffusion. Xue et al. 88 analyzed the impact of broadband network facilities on enterprises’ technology diffusion by using data of Chinese listed companies from 2008–2017. The results found that the improved network infrastructure not only facilitates the diffusion of technological knowledge from listed companies to their internal subsidiaries, but also promotes technological cooperation with other external companies. Specifically for this study, the development of the information society has not only facilitated medical technology and management innovation, but also facilitated the diffusion of medical technology. In the age of the information society, people work and live in a highly networked manner. Communication and learning through online meetings and teleconsultations, and technical exchanges and cooperation between medical institutions and doctors are becoming more frequent and efficient, enabling the rapid diffusion of advanced medical technologies in different regions. This is an important reason why the development of the information society has been able to drive up the purely technical efficiency of society's overall healthcare services.
Besides, our results report the negative effect of the ISI on SE. Other things being equal, the development of information society further reduced the scale efficiency. From an input point of view, the problem of inadequate / redundant healthcare inputs has become more outstanding as the Information society evolves. The possible reason may be the substitution effect of the online healthcare input on offline healthcare input in the production process. Prior literature indicated the implementation of the online healthcare system decreased the patients’ office visits by about 10.3% in the rates of visits, or 0.25 visits per member per year. 89 When the online input invested by social non-medical institutions (e.g., the online healthcare service provider Haodf.com, Chunyu Doctor, etc.) increased greatly, the increased offline input may become redundant. This may cause the decreased returns to scale in offline hospital health services.
Regarding the control variables, login come has negative but insignificant coefficient in column (1). While many empirical findings in the literature suggest that higher incomes increase the demand for healthcare and consequently the efficiency of healthcare,58,59Audibert et al. 90 found in her study that an increase in income in rural areas leads to a decrease in the efficiency of healthcare. This is because higher incomes increase the ability of people in rural areas to pay, thus increasing the flow of patients to technologically advanced areas. Our findings are consistent with Audibert et al. 90 to some extent. Considering that Audibert et al. 90 focused only on the rural regions, further explore should be conducted to see if the negative impact of income growth is only on undeveloped provinces with limited medical resources. We will discuss this issue in the next subsection.
Both ratio of youth and older and PopDensity have significant and positive coefficients in column (1) and column (2), suggesting the healthcare efficiency positively relates to the population density and the of to youth and older population. Insurance had a significant negative effect on TE, and this was mainly caused by a decrease in SE. This finding is consistent with Martine (2013) who found that an increase of the coverage of the New Rural Cooperative Medical Scheme in China caused the decrease in the efficiency of Chinese rural healthcare system. The reason is that the high insurance coverage may induce the soft budget constraint and lead to the less control of medical cost, and thus decrease the SE and TE.
Our results also show that public has negative effect on PTE, indicating the higher ratio of public hospitals may decrease the pure technical efficiency. Prior literature have examined the impact of hospital ownership on healthcare efficiency, and reached inconsistent conclusions. A study of hospitals in the Ghana region showed that public hospitals are significantly more efficient than private hospitals. 52 This finding is contrary to Kakeman et al. 53 and Hu et al. 51 who focus on the healthcare efficiency of Iran and China and conclude that the private hospitals are more efficient. Some other studies show that there is no significant difference between public and private hospitals in terms of healthcare efficiency. 56 Thus, the impact of the ration of public hospitals on healthcare efficiency also varies regionally depending on the country's healthcare policy and supervisor mode. Our results are consistent with Hu et al. 51 suggesting that the private hospitals would have higher PTE in Chinese healthcare environment.
The insignificant coefficients on urbanization and inflation rates in Table 7 suggest that higher levels of urbanization and inflation have a smaller impact on efficiency.
In order to further test the provincial disparities of the ISI impact on healthcare efficiency, we now categorize 31 provinces into three groups according to their efficiency score in 2014. Group 1 has 10 provinces with relatively lower efficiency score (<0.9) in 2014 and the average efficiency score was 0.74. These provinces are Heilongjiang, Neimeng, Jilin, Shanxi, Liaoning, Shaanxi, Qinghai, Ningxia, Hainan, and Gansu. Group 2 includes Fujian, Beijing, Jiangsu, Xinjiang, Anhui, Shandong, Tianjin, Hubei, Xizang, Sichuan, Hunan, and Chongqing. All these provinces got efficiency scores between 0.9 and 1. Group 3 includes 9 efficient provinces (efficiency score=1) in 2014. They are Hebei, Shanghai, Zhejiang, Jiangxi, Henan, Guangdong, Guangxi, Guizhou, and Yunnan. We then test the provincial heterogeneity in the ISI impact by conducting Tobit regression model for the three groups, respectively. Table 8 reports the main results.
Provincial disparities of the ISI mpact.

Provincial disparities of the ISI mpact.
Standard errors in parentheses ***p<0.01, **p<0.05, *p<0.1.
For Group 1, ISI exhibits significantly positive impact on TE (p<0.1) and PTE (p<0.05), and significant negative impact on SE (p<0.05). For every 0.1 increase in the ISI, PTE will rise by 0.114. Although SE will simultaneously fall by 0.034, there will still be a relatively significant increase in its overall technical efficiency (around 0.078). This means that, for those provinces whose healthcare efficiency is relatively lower, the information society development can greatly improve the technical efficiency of the healthcare systems, and this is mainly caused by the increase of the PTE. However, the impact of ISI on TE, PTE, and SE were statistically insignificant for Group 2, and had even a significant negative effect for Group 3. The results suggest that information society development cannot improve the healthcare system efficiency for those high-efficiency provinces.
The above analysis shows that there are significant regional differences in the impact of information society development on efficiency. The possible reason may be the technology spillover effect associated with technology diffusion. Provinces in Group 3 were all on the production frontiers, and thus were the most efficient in technology and the scale of production. As the information society developed, these provinces could share the healthcare technology with others more efficiently, which could generate positive technology spillover effect to other provinces. In this process, the pure technical efficiency (PTE) of these provinces remains unaffected while the low-efficiency provinces (Group 1) could benefit a lot in PTE improvement. This is consistent with our results that the PTE of provinces in Group 1 increased greatly as the ISI become higher.
However, the technology spillover can simultaneously cause the “demand loss” of the high-efficiency provinces. Due to the technology improvement, the previous lower-efficiency provinces could be more competitive and attractive for local patients, and therefore could partly reduce the unreasonable patient flow. Moreover, as information technology developed, healthcare specialists in high-efficiency regions could directly provide healthcare services for remote patients through online healthcare platform or telemedicine system, which may further increase the “demand loss” effect. As a result, the “SE” of those high-efficiency provinces decreases as their ISI increases. The results in column 9 of Table 8 show a negative effect of ISI on SE. Although this result is not significant, it is still a main contributor to the significant decrease in TE in Group 3.
Due to the small sample size of each group and the relatively close levels of the independent variables within the same group, most of the effects of the control variables on the groups were small or insignificant. Some variables remain consistent with the total effect. The variable of our interest is logincome. As can be seen in Table 8, log(income) has a significant negative effect on efficiency (TE and PTE) of Group 1 provinces. Most of the provinces in the inefficiency group are remotely located, have backward medical technology and lower income. Therefore, our results further confirm and extend the findings of Audibert et al. 90 that economic growth in underdeveloped areas leads to patients seeking better quality healthcare services, thus reducing healthcare efficiency. In contrast, logincome has a non-significant effect on Group2 and a significantly positive effect on Group3. This suggests that for provinces with relatively advanced economies and medical technology, the increased demand from income growth can lead to a full use of available medical resources.
Main findings
This paper focuses on the impact of information society development on healthcare efficiency and the disparities of this impact across provinces. A classical two-stage DEA framework is constructed to address the research questions, including the first-stage input-oriented BCC-DEA analysis and the second-stage time-fixed effects panel Tobit regression analysis. Based on the panel data of 31 Chines provinces from 2014–2017, this study generates several meaningful findings.
Firstly, the results of the DEA analysis show a slight decrease in efficiency from 0.892 to 0.869, although ISI increased from 0.423 to 0.489 during the sample period. Moreover, PTE is much lower than SE, suggesting that enhancing PTE is the key to improving the overall technical efficiency (TE) in China.
Secondly, the time-fixed Tobit regression analysis suggests that information society development leads to a significant increase in PTE, but results in a decrease in SE, and therefore has little effect on TE. Specifically, for a 0.1 increase in the ISI, PTE increases by 0.046 and SE decreases by 0.037.
Thirdly, further analysis reveals that the impact differs sharply between low-efficiency and high-efficiency provinces. For the low-efficiency provinces, the TE increases significantly with the development of the information society, mainly due to a considerable increase in PTE. In contrast, the TE decreases for the high-efficiency provinces, mainly caused by a decrease in SE.
Finally, the results show that economic growth has a significant negative impact on efficiency in low-efficiency provinces, while can increase efficiency in high-efficiency areas. The reason might be that the growth in economy increases the patient flow from remote areas to developed regions, thus decreasing the TE in low-efficiency provinces which are mostly in remote and underdeveloped areas.
Implications
This study makes contributions to both theory and practice. From the theoretical perspective, this study enriches the research findings in the field of healthcare efficiency and health management by empirically examining the relationship between information society development and healthcare efficiency. Although existing literature has analyzed the impact of external environmental factors on healthcare efficiency from economic, demographic and educational perspectives, few have focused on information society development as a factor. To our knowledge, this research is among the first empirical studies to investigate how the information society development affects healthcare efficiency and the variability of this impact across provinces.
The findings of this study provide an empirical basis for healthcare policymakers and health administrators to address the current situation of healthcare service in China and improve the healthcare efficiency. Our results suggest the key to improving the overall technical efficiency (TE) in China is enhancing PTE. Given the significant effect of information society development in increasing PTE, especially in low-efficiency provinces, more investment in information infrastructure of healthcare system should be made in low-efficiency areas. As information society development index reaches a higher level, the time and space boundaries of medical services could be greatly reduced and therefore improve the PTE in low-efficiency provinces and then the overall TE in China. Moreover, considering that the information society development has negative effect on SE of low-efficiency provinces, the proper control of the increase in healthcare inputs in these areas is also necessary.
Limitations
There are several limitations to this paper. Firstly, as scholars have pointed out, the two-stage model used in this paper has its limitations such as biased estimators, and the necessity to impose parametric assumptions. Conditional efficiency measures may help to obtain more reliable results.91,92 Due to the time limit and data constraints, we do not conduct conditional efficiency measures as supplementary. Future work may try to combine different models to balance their strength and weakness, to generate reliable estimators. Secondly, this study used the exogenously determined outputs (hospital outpatients and discharged inpatients), which mainly depend on unpredictable healthcare demand and are out of the control of DMU. 47 This might limit the production possibilities of a DMU. As suggested by Nepomuceno et al. 91 future research could include the exogenously determined outputs as non-discretionary inputs to generate robust estimates. Thirdly, due to the availability of data for some variables, only panel data from 2014–2017 are selected for research. Thus, the results can only reflect the short-term trend of healthcare efficiency change and ISI impact. We did not include the number of technical equipment such as CT and MR as inputs because of the provincial data was not available. The investment healthcare technologies can generate great impact on healthcare efficiency. 93 The lack of technology-related inputs in DEA model may result in the higher efficiency scores for those developed provinces with more technical devices. Future research including investment related to these technologies will be better. Fourth, we are unable to capture the quality of outputs at the provincial level for the time being. As China's healthcare system is currently facing mainly the problem of "difficult access," this paper focuses only on quantitative output variables. This suggests that for a given level of input, the efficiency score only reflects the increase/decrease in the number of hospital visits. Although the DEA results report a decrease in overall efficiency over the data period, the overall healthcare environment may have improved over time as a result of a decrease in the output–input ratio (an increase in healthcare resources per capita) and patients’ healthcare needs may have been better met. However, does a reduction in efficiency imply a reduction in undesirable outputs such as mortality? This question remains unexplored in this paper. Finally, Given the widespread use of online healthcare service, how does the overall efficiency of the dual-channel (online and offline) healthcare delivery system change with the development of information society? Future research focusing on these questions could enrich the literature and help provide a better understanding of the effect of information society development on the efficiency of healthcare system.
Conclusions
In this study, the classical two-stage DEA was used to estimate the efficiency of the healthcare system in 31 provinces of China from 2014–2017. Input variables included the number of healthcare workers, the number of hospital beds, total healthcare expenditure and gross fixed assets. The output variables included the number of inpatients discharged and the number of outpatients. The results showed a slight decrease in overall efficiency from 0.892 to 0.869. In addition, pure technical efficiency was much lower than scale efficiency and was therefore key to improving overall efficiency.
In the second stage, Tobit regression analysis was used to examine the impact of the development of the information society on healthcare efficiency. A range of economic and environmental factors were used as control variables. The results showed that the development of the information society led to a significant increase in PTE, but resulted in a decrease in SE and therefore had a small impact on TE. Further analysis revealed that this impact differed significantly between inefficient and efficient provinces. For the inefficient provinces, TE increased significantly with the development of the information society, largely due to the large increase in PTE. Conversely, TE declines in the more efficient provinces, mainly due to a decline in PTE.
The findings of this study highlight the importance of investment in information infrastructure in inefficient areas, and the importance of applying emerging information technologies to break through the temporal and spatial boundaries of healthcare delivery to improve overall efficiency. Appropriate controls on the growth of healthcare inputs in inefficient provinces are also necessary.
This paper focuses on the impact of the development of the information society on reducing cross-regional differences in healthcare efficiency. Future research could incorporate HIT-related inputs and quality-related outputs into the DEA to gain more insight into the quality performance implications of HIT and information society development.
Footnotes
Acknowledgments
The authors would like to sincerely thank the editor and reviewers for their kind comments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research project on Humanity and Social Science of the Ministry of Education in China, (grant number 18YJCZH052)
Ethical approval
Not applicable, because this article does not contain any studies with human or animal subjects
Author contributions
Conceptualization: Yuanrong Hu. and Shengkang.Lu.; methodology: Yuanrong Hu. Yongqing Li. and Ying Wang ; statistical analysis: Yuanrong Hu. and Ying Wang; Data curation, Yuanrong Hu. and Shengkang.Lu.; writing—Yuanrong Hu. and Ying Wang; writing—review and editing, Yuanrong Hu. And Yongqing Li All authors have read and agreed to the published version of the manuscript.”
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Yuanrong Hu