
Abstract
Objective
To facilitate the older adults with knee pain to perform exercises and improve knee health, we proposed the design of a machine learning-based system for lower-limb exercise training that features three main components: video demonstration of exercises, real-time movement feedback, and tracking of exercise progress. At this early stage of design, we aimed to examine the perceptions of a paper-based prototype among older adults with knee pain and investigate the factors that may influence their perceptions of the system.
Methods
A cross-sectional survey of the participants’ (N = 94) perceptions of the system was conducted using a questionnaire, which assessed their perceived effects of the system, perceived ease of use of the system, attitude toward the system, and intention to use the system. Ordinal logistic regression was conducted to examine whether the participants’ perceptions of the system were influenced by their demographic and clinical characteristics, physical activity level, and exercise experience.
Results
The participants’ responses to the perception statements exhibited consensus agreement (≥ 75%). Age, gender, duration of knee pain, knee pain intensity, experience with exercise therapy, and experience with technology-supported exercise programs were significantly associated with the participants’ perceptions of the system.
Conclusions
Our results demonstrate that the system appears promising for use by older adults to manage their knee pain. Therefore, it is needed to develop a computer-based system and further investigate its usability, acceptance, and clinical effectiveness.
Introduction and background
Numerous kinds of novel technologies have been developed in recent years to help older adults manage their health conditions. However, older adults face unique challenges to using these technologies, such as computer illiteracy. In this study, we introduced older adults to a paper-based prototype of a machine learning-based lower-limb exercise training system for knee pain, designed by our research team, and examined their perceptions of the prototype. We then identified aspects that should be considered in the design of such novel technology to improve its utility for older adult end-users.
Exercise therapy for older adults with knee pain
Knee pain, often caused by osteoarthritis, is highly prevalent in older adults1,2 and significantly reduces their physical function and quality of life.3,4 Exercise therapy is recommended for reducing knee pain and improving functional status (e.g., muscle strength and joint flexibility).5–10 Individuals are usually required to receive face-to-face exercise sessions at clinics and perform prescribed exercises remotely at home or in the community. However, this traditional mode of delivering exercise therapy has at least two main limitations: regular visits to clinics are time-fixed and costly, and physical therapists can only provide minimal supervision for remote exercise sessions.
Over the past few decades, various technologies (e.g., telephone, mobile application (app), and web technologies) have been used to support the delivery of exercise therapy for knee pain,11–13 and thus the accessibility and affordability of such therapy have been improved. In particular, some exercise programs have tracked exercise performance to record whether individuals have performed exercises and evaluate how well they performed them, based on which physical therapists have modified their supervision. However, these programs have either required individuals to manually input data on the frequency and duration of performing exercises, which is passive and indirect14–16; or have attached wearable sensors to individuals’ bodies to track exercise movements, which can be intrusive and cause discomfort.17–19 Machine learning techniques have also been used for exercise tracking and pose estimation.20–22 For instance, Biebl et al. 23 developed a machine learning-based smartphone app that provided audiovisual feedback for pose correction; however, system usability, user-system interaction, and feedback provision appeared to be limited as the small-sized smartphone had to be placed on the ground and users had to stand about 2 m away from it when performing exercises. Displaying movements, feedback, and users’ exercise performance on small screens that are far away from users could be a barrier to user-technology interaction and technology acceptance and adoption for both general users and people with knee problems who are mostly elderly.24–26
A machine learning-based system for lower-limb exercise training
In light of the limitations mentioned above, we have designed a desktop computer-based, interactive, and user-centered exercise training system to serve as a tool for facilitating lower-limb exercise training. The system allows individuals to (1) perform lower-limb exercises by following video demonstrations, (2) obtain immediate and corrective feedback on exercise movements, and (3) view long-term records of exercise performance. We have also adopted machine learning techniques (i.e., an advanced pose-estimation algorithm) to support motion tracking and provide real-time movement feedback via this system. In a previous pilot study, 27 we created an initial version of the system and collected initial perceptions of it from young and healthy adults. We then improved the system's features and interface design based on the pilot findings. However, the target population's opinions of the improved system, i.e., older adults with knee pain, have yet to be examined. It is necessary to study if our proposed system is well accepted among older adults with knee pain. Without their acceptance, they may be unable to take advantage of the system's benefits for managing and enhancing their knee health.
Moreover, the factors that influence perceptions of the system or its effects remain unknown. These factors should be identified to help researchers understand who may be interested in using the system and to tailor it to individual users to optimize their experience. Perceptions of a novel exercise system or program can be influenced by several factors, such as demographic and clinical characteristics, physical activity level, and exercise experience.9,28–30 First, demographic characteristics, such as age and gender, influence individuals’ perceived effects of healthcare technologies on supporting and encouraging exercise.29,30 Thus, the perceived effects of our system may also be influenced by these demographic characteristics. Second, clinical characteristics can be associated with individuals’ perceptions of an exercise system, as individuals with more severe knee pain may experience greater difficulty than those with less severe knee pain with performing exercises, which is a barrier to exercise. 9 Therefore, clinical characteristics may have negative impacts on individuals’ perceptions of our system. Third, it was found that being physically active and performing regular exercises increased adherence to an exercise program among older adults with knee pain, 28 and these factors may also influence the perceived effects of our system.
Objectives of the current study
The present study had two objectives. The first objective was to investigate the perceptions of the design of our system among older adults with knee pain. The second objective was to examine whether the perceptions were influenced by their demographic and clinical characteristics, physical activity level, and exercise experience.
Design of the machine learning-based system for lower-limb exercise training
The system was designed to be run on a computer equipped with a webcam, a monitor, a mouse, and a keyboard. The three main features of the system are its provision of video demonstrations of lower-limb exercises, provision of real-time movement feedback, and tracking of exercise progress (see Figure 1). These features are detailed below.
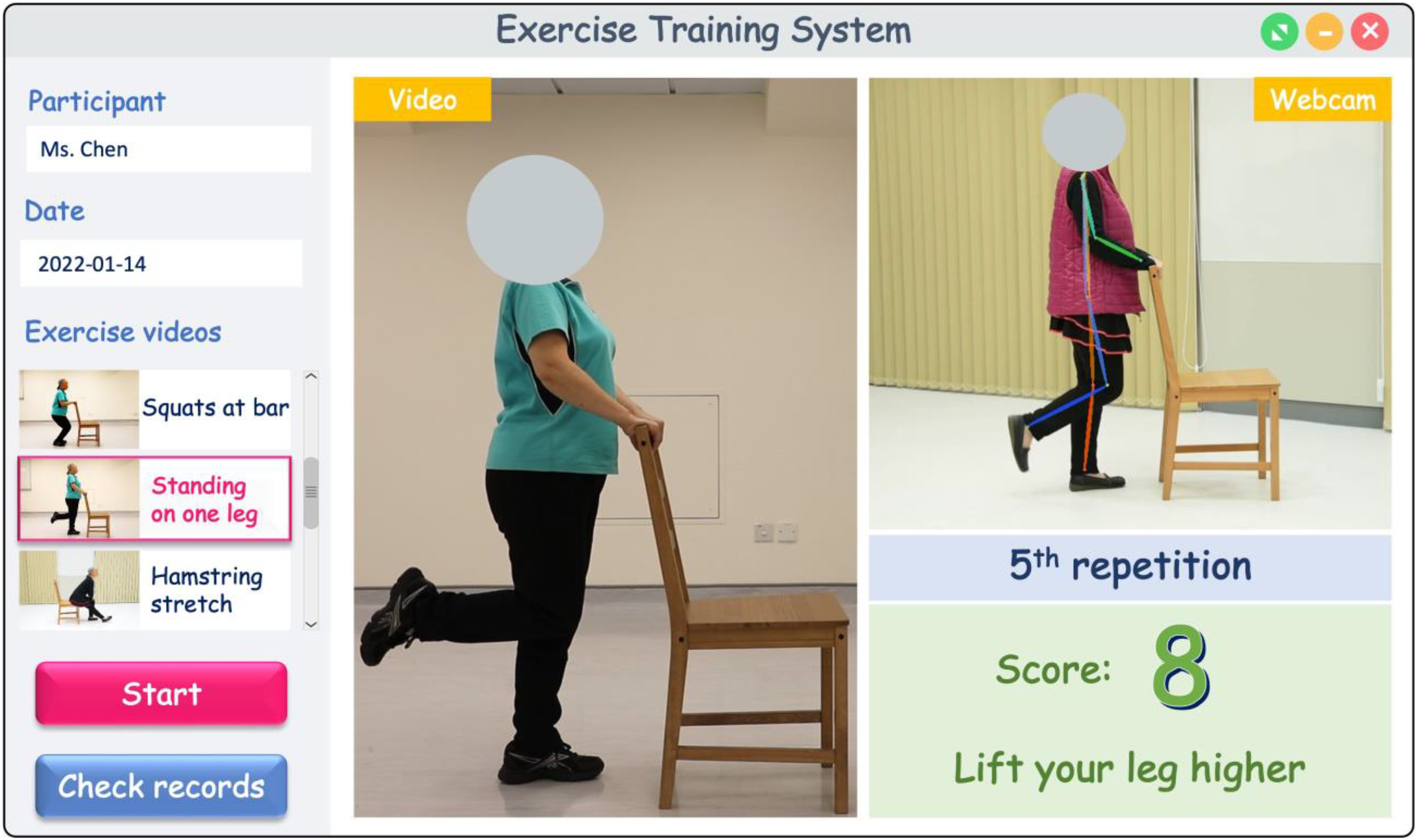
Interface design of the machine learning-based lower-limb exercise training system with three key features: (a) video demonstration of lower-limb exercises, (b) real-time movement feedback, and (c) tracking of exercise progress.
Feature 1 – video demonstration of lower-limb exercises
In our pilot study, 27 the participants mentioned that the system should include more exercise videos with audio instructions. Thus, the current system incorporates several evidence-based, physical therapist-instructed exercise videos with audio instructions that demonstrate lower-limb strengthening, stretching, mobilization, and aerobic exercises. 31 As illustrated in Figure 1, users can scroll up and down to select the exercise videos they wish to view.
Feature 2 – real-time movement feedback
After selecting an exercise video and clicking on the “Start” button (the red button in Figure 1), the system automatically plays the video and instructs users to follow the video to perform exercises. A webcam is used to capture and record the user's exercise movements. A machine learning-based human pose estimator 32 extracts the skeletal data of the user's poses in each frame, i.e., positions of key points on the user's body (e.g., head, shoulder, hip, knee, and ankle) for application in motion tracking. After the completion of one repetition of an exercise, the similarity level between the user's poses and the physical therapist's predetermined target poses is calculated and then converted to a standardized exercise performance score ranging from 0 to 10, with a higher score indicating better performance. The score is presented in green (indicating good performance) or yellow (indicating poor performance). In addition, the participants in the pilot study suggested that when the system detects incorrect movements, it should provide real-time, informative, and customized instructions on how to perform correct movements. 27 Thus, if the current system detects deviations between the poses or motion trajectories of a user and those of a physical therapist, it provides real-time textual and auditory instructions to aid the user to make immediate corrections. For example, if a user following the exercise video to perform “standing on one leg” does not lift his/her leg as high as the physical therapist lifts her own leg, the system detects the deviation and then presents the instruction “lift your leg higher” on the screen (see Figure 1). After the completion of all repetitions, an overall performance score is calculated and presented on the screen.
Feature 3 – tracking of exercise progress
The participants in the pilot study indicated that a new feature was required to help users track their exercise progress. 27 Thus, in the current system, users can click the “Check records” button (the blue button in Figure 1) to check all of the exercises they have performed and their performance scores for those exercises. This allows users to keep track of their exercise performance and be aware of their progress over a long period.
Methods
Study design
We used a cross-sectional questionnaire to survey older adults with knee pain to obtain their perceptions of our system. We demonstrated the design of the interface of our system (as presented in Figure 1) in the form of a paper-based prototype incorporated into the questionnaire, verbally introduced the details of the features, and then administered the questionnaire to collect data. This study was approved by the Human Research Ethics Committee of the University of Hong Kong (reference number: EA200327).
Participants
Ninety-four participants were surveyed from July to December 2021. The following inclusion criteria were used: (i) aged ≥50 years, (ii) responding “yes” to the question “During the past 12 months, have you had pain in or around your knee(s) on most days for at least a month? (by most days, we mean more than half of the days in a month),” (iii) able to speak and read Chinese, and (iv) able to provide written informed consent.
Questionnaire
The questionnaire used in this study comprised items covering the following domains:
Demographic characteristics
These comprised age, gender, and education level.
Clinical characteristics
These comprised duration and laterality of knee pain during the past 12 months; knee pain intensity during the past 12 months, measured by the 11-point numeric pain rating scale (NPRS) (ranging from 0 “no pain” to 10 “worst imaginable pain” 33 ; diagnosed knee diseases (i.e., osteoarthritis, rheumatoid arthritis, and gout); experience with physical therapist-led exercise therapy for knee pain during the past 12 months; and experience with technology-supported exercise programs (for example, via telephone call, mobile app, or computer software).
Physical activity level and exercise experience during the past 7 days
These comprised four generic items that were adapted from the short-form International Physical Activity Questionnaire (IPAQ).34,35 Based on the IPAQ scoring protocol, the participants’ physical activity levels during the past 7 days were considered as high, moderate, or low. We also asked the participants whether they had performed exercises in the previous 7 days.
Perceptions of the system
We examined the participants’ perceived effects of the system (on exercise performance, knee health, and exercise adherence), perceived ease of use of the system, attitude toward the three system features, and intention to use the system (see Table 1). The questionnaire items were adapted from the technology acceptance model (TAM) and relevant studies in the health IT domain.36–38 The participants’ perceptions were captured by indicating their level of (dis)agreement with items about the above-mentioned aspects on a 7-point Likert scale, ranging from 1 “very strongly disagree” to 7 “very strongly agree.”
Questionnaire items used to examine the participants’ perceptions of the machine learning-based lower-limb exercise training system.

Data collection
Our research assistants randomly approached potential participants in public areas, introduced the study protocol to them, and determined their eligibility. Those who were eligible and willing to participate provided their written informed consent. Subsequently, the research assistants administered the questionnaire to the participants via face-to-face interviews. Upon completing the interview, the participants each received HK$20 in cash as compensation for their time.
Data analysis
Descriptive statistics were calculated for all of the variables measured in the questionnaire. In particular, for each item of the perceptions, we calculated the percentage of participants whose responses were “very strongly agree,” “strongly agree,” or “agree.” We regarded 0%–50% as indicating no consensus, 51%–74% as indicating a majority view, 75%–99% as indicating a consensus, and 100% as indicating unanimity.39,40 Furthermore, we used ordinal logistic regression to examine the associations of the participants’ demographic and clinical characteristics, physical activity level, and exercise experience with their perceptions of the system, with each item measured on a 7-point Likert scale. A p-value of less than 0.05 was considered to indicate statistical significance. Data analysis was performed using IBM SPSS Statistics 25.
Results
Sample characteristics
Table 2 presents the data of our sample (N = 94), i.e., the participants’ demographic and clinical characteristics, physical activity levels, and whether they had performed exercises during the past 7 days.
Characteristics of the sample (N = 94).

SD = standard deviation, NPRS = numeric pain rating scale.
Perceptions of the system
The participants’ perceptions of our system are shown in Table 3, and the agreement level of each item is presented in Figure 2. More than 75% of the participants responded with “very strongly agree,” “strongly agree,” or “agree” to all of the items, indicating that consensus agreement was achieved. Specifically, more than 90% of the participants agreed that it was a good idea that the system provides real-time movement feedback (92.6%), that the system would be easy to use (91.5%), and that it was a good idea that the system includes exercise videos instructed by a physical therapist (90.5%). In addition, 80.9% of the participants agreed that it was a good idea that the system tracks exercise progress. However, fewer participants agreed that the system would have positive effects on their knee health (78.7%), improve their performance of lower-limb exercises (77.7%), or promote exercise adherence (75.5%). Overall, 86.1% of the participants stated that they intend to use the system in the future if they have access to it.

Percentage of participants who responded “very strongly agree,” “strongly agree,” or “agree” to each item on perception (N = 94).
Perceptions of the machine learning-based lower-limb exercise training system (N = 94).

Factors influencing perceptions of the system
The associations of the participants’ demographic and clinical characteristics, physical activity level, and exercise experience with their perceptions of the system are presented in Appendix. When compared to participants with less severe knee pain, those with severe knee pain were more likely to agree that using the system would improve their exercise performance (odds ratio [OR] = 1.47, 95% confidence interval [CI]: 1.08 to 2.01, p = 0.02) and that it was a good idea that the system gave real-time movement feedback on lower-limb exercise performance (OR = 1.49, 95% CI: 1.06 to 2.08, p = 0.02). Furthermore, when compared to participants who had no prior experience with technology-supported exercise programs, those who had prior experience were more likely to express a greater intention to use the system (OR = 3.03, 95% CI: 1.04 to 8.81, p = 0.04).
However, compared with younger participants, older participants were significantly less likely to agree that it was a good idea that the system provided real-time movement feedback on the performance of lower-limb exercises (OR = 0.92, 95% CI: 0.87 to 0.98, p = 0.01). In addition, male participants were less likely to think the system would be easy to use than female participants (OR = 0.31, 95% CI: 0.11 to 0.84, p = 0.02). Moreover, compared with the participants with a shorter duration of knee pain, the participants with a longer duration of knee pain were less likely to agree that using the system would improve their performance of lower-limb exercises (OR = 0.30, 95% CI: 0.12 to 0.80, p = 0.02) or that it was a good idea that the system gave real-time movement feedback on the performance of lower-limb exercises (OR = 0.27, 95% CI: 0.09 to 0.76, p = 0.01). Furthermore, the participants who had physical therapist-led exercise therapy for knee pain were less likely than those who had not to agree that the use of the system would improve their exercise performance (OR = 0.29, 95% CI: 0.11 to 0.78, p = 0.01).
There were no significant associations observed between the participants' perceptions and the other variables, including education level, laterality of knee pain, diagnosed knee diseases, physical activity level, and exercise experience during the past 7 days.
Discussion
Main findings
This study examined the perceptions of participants—who were older adults with knee pain—on the design and utility of a machine learning-based system for lower-limb exercise training. Most participants intended to use the system if they had access to it; agreed that the system would be easy to use; and agreed that it was a good idea that the system could feature videos instructed by a physical therapist, provide real-time movement feedback on the performance of exercises, and keep track of users’ exercise progress. In addition, most of the participants agreed that the system would improve their exercise performance, promote their exercise adherence, and increase their chances of improving their knee health; however, more than 20% of the participants held a neutral or negative point of view regarding these aspects. This might have been because the participants had not used our system and many had had no experience with such technology-supported exercise programs, so that they might have been unaware of the potential benefits of our system.
We identified some factors that influenced the participants’ perceptions of our system, as detailed below.
Knee pain intensity and duration
We found that, when compared to participants with less severe knee pain, those with severe knee pain were more likely to have positive attitudes toward the system's features and value the system's potential to facilitate their exercise training. According to the self-care information technology acceptance model developed in our earlier study, 41 these positive attitudes may be attributed to their high level of health consciousness; that is, they were concerned about their knee condition and tended to take actions to manage it. For instance, people with severe knee pain are more likely to seek treatment attention than those with mild pain. 42 As a result, such health-conscious individuals are more likely than others to be enthusiastic about using our system for lower-limb exercise training. In contrast, people who have experienced longer durations of knee pain are more likely to delay seeking treatment than those who have experienced shorter durations of knee pain because they tend to wait for pain to lessen. 43 Thus, in the future, we need to stress the importance of exercise therapy and raise their health consciousness in order to promote acceptance of our system among older adults with mild but chronic knee pain.
Experience with technology-supported exercise programs
Our findings showed that individuals who had prior experience with technology-supported exercise programs were more likely to intend to use our system than those who had not.This could be because when people are introduced to a new system, they often think about comparable systems they have used in the past to decide their intention to use the new system. 44 Furthermore, older individuals may have had less exposure to technology and may have more technology anxiety than other people, therefore our participants' prior experience with technology-supported exercise programs greatly influenced their intention to use our new system. 45 This suggests that we should help people in learning to use and becoming familiar with our system so that they are not afraid of it and are more likely to use it.
Experience with physical therapist-led exercise therapy
Our findings indicated that compared with participants who had not previously received physical therapist-led exercise therapy for knee pain, those who had were less likely to agree that the use of our system would improve their exercise performance. This might have been because the latter participants preferred for a therapist to guide them by manually moving limbs and explaining which muscles they should use—which is something the system cannot do—to help them improve their exercise performance. 46
Gender
We found that the female participants were more likely than the male participants to agree that the system would be easy to use. This is consistent with the fact that compared with men, women were found to perceive it as easier to use technology in the context of exercise. 29 This is important for further implementation of the system, as women's decisions in technology use and adoption can be strongly influenced by their perceptions of ease of use. 47
Age
Although this study focused on older adults, the ages of the participants ranged from 50 to 89; and age was found to influence the participants’ attitude toward the feature design of our system. To use the features, people need some skills in operating a computer and webcam. However, compared with younger people, older people tend to have fewer computer skills and experience greater anxiety in using digital technologies. 29 This might have been why older participants in our study did not show positive feelings toward the design of the features.
Implications for system design and development
Our findings have several implications for healthcare technology design and development, particularly exercise training systems. First of all, when designing a paper-based prototype, it should include all of the main features and should be clearly presented (e.g., use plain language for non-expert users and use large font size for older adults), allowing end-users to understand the design more easily and provide more feedback on the design.
Our findings also provide implications for the design of feature design in exercise training systems. First, with the support of video demonstration, individuals using our system to perform exercises would be able to garner a clear understanding of the required type, speed, and range of motion. Therefore, designers of such healthcare technologies could consider the use of video demonstration to improve instruction on exercise training delivered via these technologies. Second, the provision of real-time movement feedback in our system would serve as continuous and instant supervision for individuals performing exercises, which may reduce demands on physical therapy staff. Third, the tracking feature in our system could help individuals monitor long-term changes in their exercise performance and enhance their exercise adherence. Some data visualization tools, such as a calendar circling the days on which individuals have performed exercises, could be adopted to improve the feature design.
Last, in addition to knee pain, such machine learning-based exercise training systems could be used to improve the delivery of exercise therapy for other diseases, such as chronic musculoskeletal pain, stroke, and physical impairment caused by injuries or surgeries.
Implications for research
This study also has implications for future research. First, while a paper-based prototype can be useful for understanding user opinions about a new health information system, an interactive, computer-based prototype is essential to allow realistic interactions and improve our knowledge of users’ thinking. Second, the usability48–51 and acceptance52–54 of our system should be evaluated, as poor system design and individual non-acceptance of a system can limit its implementation. Third, the clinical effectiveness of our system is unknown. Experiments (such as randomized controlled trials) are needed to assess our system’s ability to improve relevant health outcomes such as knee pain, physical function, and quality of life.
Limitations
The study has limitations. First, over 90% of the participants showed a moderate or high level of physical activity, and over 70% had performed exercises during the previous 7 days. It is possible that the perceptions of people who have a low level of physical activity and have not performed exercises regularly would be different from those of our sample. Second, this study focused on the paper-based prototype of the system, but the perceptions of the actual system remain uncertain and should be examined further.
Conclusions
In this study, we examined the perceptions of older adults with knee pain regarding a paper-based version of a machine learning-based system designed to support lower-limb exercise training. Most older adults had positive opinions about the system’s perceived effect, perceived ease of use, and features, and they intended to use it if given an opportunity. These results show that it is worthwhile to continue the effort to develop and implement a computer-based version of the system for exercise training and knee pain management. Moreover, the usability and acceptance of the system and its efficacy in improving health-related outcomes warrant further investigation.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231186069 - Supplemental material for Perceptions of a machine learning-based lower-limb exercise training system among older adults with knee pain
Supplemental material, sj-docx-1-dhj-10.1177_20552076231186069 for Perceptions of a machine learning-based lower-limb exercise training system among older adults with knee pain by Tianrong Chen and Calvin Kalun Or in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank Mr Jason Wong and Mr Felix Lo for their assistance in data collection.
Contributorship
TC and CKLO designed the study, developed the research protocol, and gained ethical approval. TC recruited the participants, performed the data analysis, and wrote the first draft of the manuscript. Both authors edited the manuscript and approved its final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Human Research Ethics Committee of the University of Hong Kong (reference number: EA200327).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Seed Fund for Basic Research of the University of Hong Kong (grant number 201910159250; principal investigator: CKLO).
Guarantor
CKLO
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.