
Abstract
Objectives
This study aimed to investigate the associations between eHealth literacy, preferences for financial decision-making, and financial toxicity (FT) in a sample of Chinese cancer patients.
Methods
Eligible cancer patients were invited to participate in a cross-sectional survey from January to April 2021. Three measures (eHealth literacy scale, control preference scale, and COST) were used to analyze patients’ eHealth literacy, decisional preferences, and FT, respectively. Wilcoxon signed-rank test and Kruskal–Wallis H test assessed the differences between population subgroups. Binary logistic and multivariate linear regression models were used to assess the relationships between eHealth literacy, decisional preferences, and FT.
Results
A total of 590 cancer patients completed the questionnaire. We found that high FT was associated with poor ECOG performance, severe cancer stage, and longer cancer duration. Patients who preferred to adopt collaborative attitude toward decision-making showed a significantly higher eHealth literacy. However, there was an inverse relationship between eHealth literacy and a patient-driven attitude toward decision-making in female cancer patients. Regression analysis indicated that patients who were highly educated and actively employed might report a higher eHealth literacy. A significant relationship was found between high eHealth literacy and low FT. However, this relationship became insignificant when the background characteristics of cancer patients were taken into account.
Conclusions
A relationship between enhanced eHealth literacy, preference for collaborative decision-making, and low risk of FT is identified.
Practical implication
Interventions to improve patients’ ability to use quality and reliable web-based information on cancer care should be encouraged.
Introduction
Financial toxicity (FT) refers to subjective financial distress experienced by cancer patients due to their objective out-of-pocket (OOP) medical expenses. This FT leads to impaired quality of life for patients and impedes the delivery of quality health care. 1 Despite recent improvements in early diagnosis and new treatments, cancer patients’ expenses have increased dramatically due to extended life expectancy and effective disease control. 2 As a result, this surge in expenditure on cancer diagnostics, therapeutics, and care has become an obstacle to affordable and accessible cancer care.3,4
Patients with cancer face challenges when trying to search for information about treatment and care costs, as well as understanding all the related financial concepts. Traditionally, medical professional is the primary source of information for patients with cancer to understand their disease, including cost. 5 However, previous studies have indicated that oncologists’ knowledge about cancer cost management is limited.6,7 Patients with cancer are increasingly encouraged to self-search for information about their health conditions, and the internet has become an essential medium for them to receive and share cancer information. 8 However, studies have also shown that many patients with cancer struggle with low health and computer literacy, which affects their ability to search for information and effectively communicate with healthcare providers.9–11 Therefore, providing appropriate support and information via the internet can be essential to empower patients with cancer, improve their ability to make informed healthcare decisions, and address and ease FT. 12
There is a dearth of comprehensive databases that collect information on the cost of care accessed by patients over a sufficient length of time. 13 Cancer treatment can be expensive, and the cost varies greatly depending on cancer type, insurance, hospital charges, expenditure on drugs, travel, childcare, and other necessities.9,10 Since online information about cancer-related costs is unsystematic and fragmented, it can be overwhelming for most cancer patients to keep track of. Therefore, it is vital to increase patients’ knowledge and skills in searching for and using cancer-related healthcare information so that they can effectively navigate the increasingly complex healthcare system. eHealth literacy is an individual's ability to seek out, find, understand, and appraise health information from the internet to address and solve a health problem. 14 Regarding cancer care, patients are increasingly using web-based tools to manage their health. Studies have shown that many cancer patients use internet to seek support, find other opinions on treatment, interpret symptoms, and check their doctors’ advice.10,15,16 However, the relationship between patients’ ability to search cost-related online information and FT has rarely been studied in cancer care.
Shared decision-making can significantly reduce the financial burden of cancer care. 17 Increased involvement in the decision-making process resulted in less conflict, higher satisfaction, and lower costs with decreased use of healthcare services.18–20 In addition, cancer patients who are provided with sufficient information about prognosis and treatment options are more likely to engage in decision-making and adhere to treatments. 21 Training and improving patients’ ability to search for cancer-related cost information and estimate cancer-related costs over time may support patients in playing a more active role by taking into account their needs, preferences, and values in clinical decision-making. 22 Previous studies have also demonstrated that web-based tools, such as online patient decision aids, can help patients with cancer understand their risks, clarify their values and preferences, and make more reasonable clinical decisions.23,24 However, while the use of these tools is well documented, patients’ ability to search for cost-related information, which can encourage them to conduct financial discussions with medical professionals, is rarely reported.
China has a high disparity in healthcare expenditure in the world. 25 To address this, the government introduced three public health insurance schemes in the late 1990s. Urban employee basic medical insurance (UEBMI), a compulsory scheme financed by payroll taxes from both employers and employees; urban resident basic medical insurance (URBMI), a voluntary scheme for urban residents without formal jobs or unemployed. Additionally, new rural cooperative medical scheme (NCMS), a voluntary scheme for the rural residents. By the end of 2021, there were approximately 1.36 billion (96.5%) people enrolled in such three schemes. These schemes improved health outcomes, but there are still low levels of quality service coverage and high out-of-pocket expenditures (around 60%) for severe and long-term conditions like cancer. 26 Most anti-cancer drugs are not covered by public insurance and the reimbursement rate for outpatient service is relatively low (around 50%). 27 Additionally, the reimbursement mechanism is complex which calculated based on patient's insurance type, family registration, and income level. 28 Cancer care costs have increased to over RMB 80 billion each year, 29 placing a heavy burden on national healthcare expenditure and causing financial catastrophe for individuals.
Cancer care is a lifelong process. The expenditure estimate is an ongoing and dynamic task. The internet makes it easy for cancer patients and their families to search for and update information; and improving eHealth literacy can empower them to discuss their preferences with medical professionals when making decisions, exchanging information, and developing plans to reduce the detrimental effects of the financial burden on their life. 30 Despite this, there is no research reporting on cancer patients’ ability to search for reliable web-based financial information. Empirical evidence is also lacking regarding the association between cost-related eHealth literacy and FT; the association between preference in decision-making and FT; as well as the associations between sociodemographic characteristics, mental health status and clinical characteristics and FT, eHealth literacy and preference in decision-making. Therefore, the objective of this study was to conduct a preliminary investigation of these associations in patients with cancer.
Methods
Participants and data collection
A cross-sectional survey was conducted to collect data from the oncology department at two tertiary-level hospitals in China from January to April 2021. The inclusion criteria were: (1) ≥18 years; (2) have no cognitive problems; (3) have a life expectancy ≥ 24 months; (4) Eastern Cooperative Oncology Group (ECOG) performance status 0–3; (5) must have stage I, II, III or IV of the disease at the time of enrolment; (6) at therapeutic or follow-up phase of treatment; and (7) be able to give informed consent. The research team collaborated with the chief doctors of the oncology department, and two research nurses were assigned as responsible persons in the ward to manage data collection in the two hospitals. All eligible patients were invited to participate in the study during the survey. Patients who agreed to participate in the survey were approached by the appointed research nurse and invited to complete a hardcopy questionnaire.
Measures
Ehealth literacy scale (eHEALS)
The eHEALS was used to measure patients’ eHealth literacy. 31 It has eight items rated on a five-point Likert scale. The sum score of the eHEALS ranges from 8 to 40, where a higher score indicates greater perceived eHealth literacy. In this study, the eHEALS was revised to investigate cancer patients’ ability to search and use web-based cost-related information (e.g. I know what cancer cost-related resources are available on the internet). The internal consistency reliability of the revised eHEALS was satisfactory (Cronbach's alpha = 0.97).
The control preference scale (CPS)
The 1-item CPS was used to assess patients’ general preference for clinical decision-making based on five statements from active to passive decision-makers. 32 Three types of roles, patient-driven, collaborative, and clinician-driven attitudes, were identified from these five statements for further analysis.
Comprehensive score for financial toxicity (COST)
The COST was used to evaluate the financial wellbeing of cancer patients. The COST comprises 12 items. All items are rated on a 5-point Likert scale, where 0 = not at all and 4 = very much. A higher score indicates a lower FT. The internal consistency reliability of the COST was satisfactory (Cronbach's alpha = 0.88) in this study.
Depression anxiety stress scales-21 items (DASS-21)
The DASS-21 was used to assess the prevalence of psychological symptoms of depression, anxiety and stress. 33 Final scores for the three subscales (depression, anxiety, and stress) can be calculated separately. In this study, the internal consistency reliability of the three subscales was satisfactory, with Cronbach's alpha of 0.89, 0.84, and 0.87, respectively.
Statistical analysis
Descriptive analysis was used to describe cancer patients’ background characteristics. The mean and standard deviation (SD) of the eHEALS and COST scores and the proportion of response on the CPS were presented and stratified by patients’ ECOG performance status (0, 1, ≥2), frequency of hospital admission (how many times in the last 12 months), cancer stage (I–IV), duration of cancer (years after formal diagnosis), and mental health status (outcome of the DASS-21). The mean of the eHEALS and COST sum scores were presented as stratified by patients’ decisional preference (the outcome of CPS) and affordability for cancer care. Two items (annual family income and annual cancer-related cost) were used to calculate this concept. Patients were asked to indicate their family income and cancer cost in the last year on a 5-point Likert scale response (e.g. ≤50,000 RMB per year), respectively. Affordability of cancer care was calculated as the patients’ family income minus their cancer treatment-related costs. Positive and negative results were defined as “cost of cancer care less than family income” and “cost of cancer care more than family income,” respectively. Wilcoxon signed-rank test, Kruskal–Wallis H test, and Chi-squared test were used to examine the differences in eHealth literacy between FT and CPS population subgroups, separately.
Binary logistic regression analysis was used to assess the patients’ decisional preference association with eHealth literacy and FT. The dependent variable was CPS, recategorized as a binary outcome (preference for collaborative and non-collaborative decision-making, including patient- and clinician-driven attitude). For model 1, the targeted independent variable was the result of the eHEALS, which was categorized into two groups, low and high eHealth literacy (≤median and >median). For model 2, the targeted independent variable was the COST, which was categorized into two groups, low and high FT (≤median and >median). Four multivariate linear regression models were developed to predict the relationship between (1) eHealth literacy (dependent variable: eHEALS) and patients’ background characteristics (model 3); (2) FT (dependent variable: COST) and patients’ background characteristics (model 4); (3) eHealth literacy and FT without adjustment (model 5); and (4) eHealth literacy and FT, adjusted by patients’ background characteristics (model 6). All statistical analyses were performed using R, and a p-value ≤ 0.05 was considered statistically significant.
Results
Patients’ characteristics
Table 1 shows the background characteristics of the patients. A total of 590 participants (response rate = 93.4% [590/632]) completed the survey and provided valid responses. Among them, 55.3% (n = 326) were male, 69% (n = 404) were over 50 years old, and 25.1% were actively employed (n = 148). A total of 32 types of cancer were reported with liver cancer patients comprising approximately 23.6% (n = 139) of the total, bowel cancer patients comprising 11.7% (n = 69), and breast cancer patients comprising 9.5% (n = 56). The top 11 types of cancer accounted for 79.8% of all patients.
Participants’ characteristics and stratified by home registry.

Outcomes of eHealth literacy, decisional preference, and FT
The mean score (SD) for eHEALS was 23.4 (7.4), and for COST it was 13.5 (8.7). Patients who reported frequent hospitalizations had significantly higher eHealth literacy and lower FT than those who reported fewer hospitalizations. High FT was associated with poor ECOG performance, severe cancer stage, longer cancer duration, and poor mental health status. Around 67% (n = 391) of patients tended to adopt a collaborative attitude towards clinical decision-making, whereas 2.6% (n = 15) preferred patient-driven decision-making and 30.5% (n = 178) preferred clinician-driven decision-making (Table 2).
Mean of eHEALS and COST and responses of CPS.

A total of 267 patients did not provide information about cancer stage.
Association between eHealth literacy, ft, and decisional preference
Figure 1 presents the mean eHEALS and COST scores for patients who reported different decisional preferences and abilities to afford cancer expenditure, stratified by gender. A statistically significant correlation was observed between collaborative decision-making attitude and high eHealth literacy. However, a relationship between high eHealth literacy and patient-driven decision-making preferences was only observed in female patients. No statistically significant association was found between FT and decisional preference. Additionally, male patients who believe they can afford cancer care have reported a lower degree of FT than those who reported that they cannot afford cancer care.

Relationship of affordability with eHealth literacy, financial toxicity, and decisional preference; and stratified by sex (high eHEALS score indicate high eHealth literacy; high COST score indicate low FT).
Ehealth literacy, FT, and decisional preference by cancer type
The mean eHEALS and COST scores for patients with the 11 most commonly reported cancers in this study are presented in the upper part of Figure 2. Patients with bladder and thyroid cancer reported higher eHealth literacy and lower FT than patients with other cancers, respectively. The bottom part of Figure 2 shows that more than half of patients (53.7%–84%) preferred a collaborative attitude to decision-making in clinical practice. Approximately 2% to 5% of patients with five cancer types preferred a patient-driven attitude toward decision-making, and the proportion of patients who showed clinician-driven attitude ranged from 16% to 46.3%.

eHEALS and COST mean score for patients with the most reported cancer types (high eHEALS score indicate high eHealth literacy; high COST score indicate low FT).
Results of regression analyses
The results of the relationship between decision-making preferences and eHL and FT, adjusted for patients’ background characteristics, are presented in Table 3. Model 1 showed that, after adjusting for background characteristics, patients with high eHealth literacy were 1.6 times (p < 0.05) more likely to report preferring a collaborative attitude toward decision-making than patients with low eHealth literacy. However, there was no statistically significant association between FT and decisional preference (model 2: odds ratio = 1, 95% confidence interval: 0.71–1.4).
Logistic regression on binary response of the CPS.

*p < 0.05.
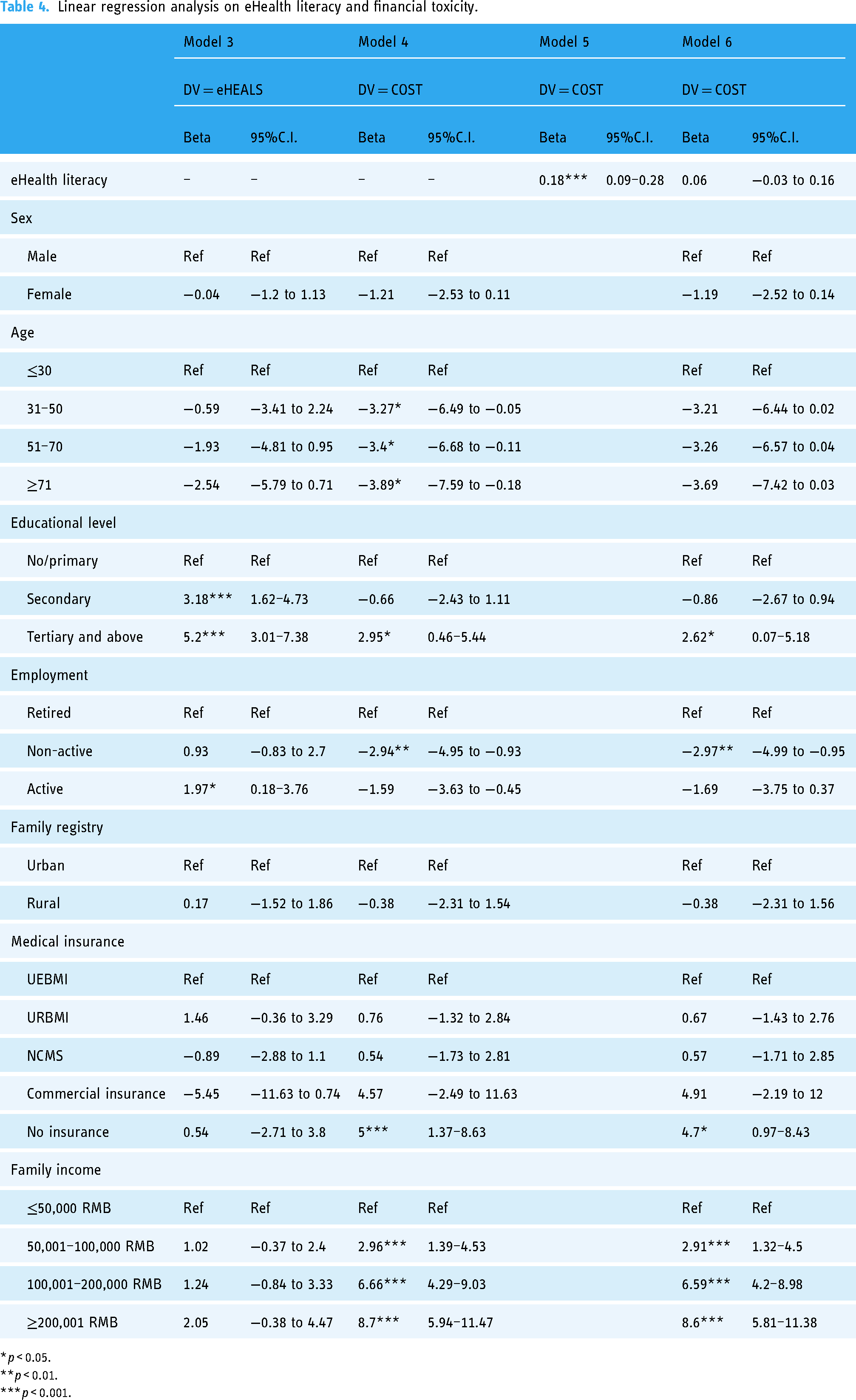
According to Table 4, model 3 showed that patients who had high education levels and were actively employed had a high level of eHealth literacy. Patients who were older and non-actively employed reported a high FT. In model 4, patients who were highly educated and had a high family income reported a low FT. Model 5 demonstrated that there was a significant association between high eHealth literacy and low FT. However, in model 6, after adjusting for patients’ background characteristics, this relationship became insignificant.
Linear regression analysis on eHealth literacy and financial toxicity.
*p < 0.05.
**p < 0.01.
***p < 0.001.
Discussion
Principal findings
This study provides empirical evidence that a high FT was associated with more depression, anxiety, and stress symptoms among cancer patients, and those who were young, highly educated, and had a high family income were more likely to report a lower FT. A significant relationship was observed between high eHealth literacy, a high educational level, and active employment status. In addition, we found a significant relationship between high eHealth literacy and low FT; however, this relationship became insignificant when the background characteristics of patients with cancer were considered. Moreover, most patients with cancer reported high eHealth literacy and desired a collaborative approach to decision-making with medical professionals in clinical practice; however, no statistically significant relationship between decisional preference and FT was observed. Nevertheless, it may be necessary to encourage patients with cancer to engage in decision-making. An individual's financial status influences complex decisions regarding when and how to seek healthcare. Additionally, the frequency of FT among patients with cancer could also increase, especially in those experiencing escalating therapy, advanced stages, and frequent hospitalization.
Comparisons with previous studies
Our study observed a lower mean eHEALS score than that in the general Chinese population, 31 but a score similar to that reported in a recent systematic review of studies targeting Chinese patients with cancer. 34 This result reflects the fact that online cancer cost information may be inadequate. This, in turn, limits the ability of patients with cancer to search for relevant information and requires further investigation. However, studies assessing eHealth literacy among patients with cancer are limited. The mean eHEALS score in our study was similar to the outcomes reported in Japan, 35 Canada, 11 and Germany, 10 which confirmed that globally, cancer patients do not get enough support for searching and using reliable web-based information. Furthermore, cancer patients in our study reported a lower COST score than those in Japan, 36 the US, 37 , Italy, 38 and Brazil, 39 which may reflect that compared to other countries, China's inadequate universal healthcare system and low ceiling amount for high-cost cancer-related medical expenses contribute to a high FT. 40
Previous studies have not reported the association between eHealth literacy and FT. Our findings show that a strong ability to search for cost-related information on the internet is associated with low FT among cancer patients. While no research has studied the impact of eHealth literacy on cost control, efforts to use online information to reduce the financial burden of cancer care have been reported. For example, Hlubocky et al. developed an internet-based assessment method to measure FT and suggested new ways to follow up on distress in long-term cancer survivors. 41 The official website of the National Institute of Health provides information on cancer drugs, including their price, to facilitate decision-making. Fisher et al. indicated that cost-related health literacy could be an essential component of oncology training to assist in controlling cancer care costs. 42 Given that a massive volume of health resources is currently available on the internet, eHealth literacy is increasingly recognized as an essential ability to help patients improve their financial capability in managing their health. 43
In this study, cancer patients with high eHealth literacy reported a strong preference for adopting a collaborative attitude toward clinical decision-making. Previous studies have shown that adequate health literacy is significantly associated with a preference for patient-involved decision-making.44–46 The internet is a valuable and practical source of up-to-date, evidence-based information for patients with cancer. 47 Our study results further demonstrate that improving eHealth literacy can encourage patients with cancer to engage in the decision-making process. Although several studies have used the CPS as a valid measure for assessing decisional preferences in cancer research, 48 some weaknesses have been reported owing to its one-item design. Future studies should use cancer-specific decision-making preference tools instead.
Although previous studies have confirmed that cost-related health literacy, including cost control, is a key component of high-quality cancer care,49,50 our study found that patients who were able to afford cancer care showed low FT and high eHealth literacy. Cancer treatments are lengthy and expensive. Patients often meet their deductible soon after diagnosis but still must pay significant costs due to high healthcare expenses and co-insurance. Therefore, we suggest that the reimbursement system be reformed to restructure the benefit design for hospital-based cancer services and include an OOP maximum to help alleviate the financial burden. Without an OOP maximum, most cancer patients would be responsible for a large portion of the treatment costs. With the high coverage of public health insurance and rapid increase in cancer mortality in China as well as the rise in private insurance coverage, it is necessary to address this issue at the policy level to ensure the sustainability of the healthcare system. Developing eHealth literacy could equip patients with the knowledge and skills to use the internet to understand the available information and manage their financial risks.
Our findings are consistent with those of previous studies showing that cancer patients with a high financial burden are more susceptible to mental health problems.51,52 For example, Chen et al. demonstrated that patients who experienced a delay in cancer care due to financial burden had a 4-fold increase in the odds of reporting anxiety. 53 Lentz et al. found that 22% to 64% of cancer patients reported stress or worry about paying their medical bills. 2 Additionally, a slightly higher proportion of patients who preferred to make decisions alone reported depression or anxiety symptoms. Although previous studies have indicated that shared decision-making may improve patients’ depression, this relationship has been insufficiently studied 54 and rarely reported in Chinese patients with cancer. Therefore, further interventions to assess the impact of eHealth literacy on improving shared decision-making and mental health status should be encouraged, considering that improving eHealth literacy can contribute to maintaining good psychological well-being. 55
Interestingly, when the background characteristics of patients with cancer were considered, the significant relationship between eHealth literacy and FT vanished. Although similar findings have never been reported in previous studies, the impact of sociodemographic factors on eHealth literacy and the FT has been reported. For example, Abbott et al. found that patients with cancer tend to experience FT if they have a lower socioeconomic status, such as residing in a rural setting or facing geographical barriers. 56 A recent study indicated that Chinese adults with a higher socioeconomic status had high eHealth literacy and sought more web-based information. 57 Additionally, it demonstrates the importance of considering the interaction between individual and contextual factors in conceptualizing eHealth literacy for managing FT among cancer survivors. In this study, we found that the relationship between eHealth literacy and FT could be affected by contextual and social determinants of health such as income, education, and employment. According to Norgaard et al., 58 the effectiveness of eHL is not determined solely by an individual’s abilities and resources but also strongly depends on the context and complexity of the systems involved, which is consistent with our findings.
Based on our findings, we suggest the inclusion of eHealth literacy and FT tests in routine cancer care. The outcomes can identify cancer patients with low eHealth literacy and high FT, which can help medical professionals tailor the care plan to provide them with training and education to enhance their ability to search and use reliable online information to understand their health status and improve their financial capability for self-care.
Limitations
Several limitations must be addressed. First, all the questionnaires were self-completed by patients, which may have led to recall bias. Second, selection bias may have affected the generalizability of our findings, given that all patients were Chinese and recruited from only two hospitals. Third, considering the insufficient number of patients reported living with some types of cancer, we did not examine the relationship between FT, eHealth literacy, and decisional preferences in patients stratified by cancer types, which may affect the generalizability of our findings. Last, we did not collect background information on cancer patients who did not use the internet to manage their health in the survey. This could potentially affect the generalizability of our findings.
Conclusions
This study shows that high education and active employment were associated with a high eHealth literacy in cancer patients; and those who were young, highly educated, and with high family income tended to report a low FT. We observe a positive correlation between higher eHealth literacy and a lower risk of FT. However, further research is necessary to examine how and why this relationship varies among patients with different types of cancer, socioeconomic statuses, or at different stages of treatment. Additionally, developing interventions to enhance cancer patients’ ability to search and use quality web-based information on controlling cancer cost are worthy of study.
Footnotes
Acknowledgments
The authors thank all participants who join in the survey and complete the questionnaire.
Availability of data and material
Derived data supporting the findings of this study are available from the corresponding author on reasonable request.
Contributorship
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study protocol and informed consent were approved by the Human Research Ethics Committee of the Chinese University of Hong Kong (Ref. No.: SBRE-20-137).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Natural Science Foundation of Guangdong Province 2023 project of Research on the Formation Mechanism of Health Behavior in Epidemic Situations Based on PADM Mode (2023A1515011124); Grant from Philosophy and Social Sciences of Guangdong College for the project of Public Health Policy Research and Evaluation Key Laboratory (2015WSYS0010); and Public Health Service System Construction Research Foundation of Guangzhou, China (2021-2023).
Guarantor
RHX.
Informed consent
Informed consent was obtained from all participants.