
Abstract
Introduction
With the widespread use of mobile devices and the rapid development of mobile networks, connecting mobile personal health record (mPHR) apps to wearable devices to collect personal health data for analysis and community activities has become a trend for health promotion. Therefore, the present study aims to explore the vital factors that impact the sustained usage of mPHR apps.
Objective
In this study, we identified social lock-in as a major research gap in the current era of social media and the Internet. Therefore, to explore the effects of mPHR apps on continued app usage intention, we combined technology fit (individual-technology, synchronicity-technology, and task-technology fit) and social capital (structural, relational, and cognitive capital) to develop a novel study model.
Methods
The purpose of this research is to investigate the willingness to participate in the mPHR apps. It collected 565 valid users’ responses through the online questionnaire with a structural equation modeling approach.
Results
That technology and social lock-in significantly affected the willingness of users to continue using mPHR apps (β = 0.38, P < 0.001) and that the effects of social lock-in (β = 0.38, P < 0.001) were more pronounced than those of technology lock-in (β = 0.22, P < 0.001).
Conclusions
The technology and social lock-in generated by technology fit and social capital had positive effects on continued app usage and the effects of both types of lock-in on continued app usage varied among different participant groups.
Keywords
Introduction
The emergence of new technologies and rising health awareness have led to increasing demand for personal health record (PHR) systems. Regularly reviewing one’s PHR is essential for staying informed about one’s health status. With the proliferation of mobile devices, mobile personal health record (mPHR) apps that provide various health records, including exercise, sleep, and heart rate records, have become commercially available. However, despite their availability, most of these apps have low usage rates and users tend to stop using them over time. Therefore, it is crucial to understand the factors that drive people to continue using mPHR applications. A deeper understanding of these factors can help promote continued app usage that can help them track their own long-term health status.
Previous studies have often investigated app usage intention from the perspective of technology characteristics and how useful a technology is. However, in the current era of social media and the Internet, people have become more concerned about what their friends are using and whether they can connect with their friends for mutual benefit. For example, Line is considered the communication software with the largest market share in Taiwan, although it does not offer the best technology. This is because if everybody is using Line, this forces others to use it as well. This highlights the importance of the Internet and social media relationships and how they outweigh technology. Another major factor for usage intention is social lock-in.
Several studies have explored new technologies by referencing the technology acceptance model (TAM) and diffusion of innovation theory. However, although these studies have considered the importance of product design, they did not address fit from the perspective of social capital. Therefore, in this study, we investigated the willingness of users to use technology by referencing the technology fit theory, by considering the three categories of technology fit (i.e. individual-technology fit [ITF], synchronicity-technology fit [STF], and task-technology fit [TTF]), and by adding three types of social capital (i.e. structural, relational, and cognitive capital). Generally, participants form and link structural capital to social structure; 1 create relational capital by interacting with each other over time; and use relational capital to explain and understand different matters, reach a consensus, and achieve cognitive capital. 2 Here, we attempted to answer the following questions: (1) How does technology fit affect technology lock-in? (2) How does social capital affect social lock-in? (3) What are the effects of technology and social lock-in on continued app usage? (4) What are the effects of technology and social lock-in on different user groups? We also performed an empirical study with structural equation modeling (SEM) to investigate and analyze mPHR app users and explore the effects of technology and social lock-in on continued mPHR app usage for different users.
Theoretical background
Mobile personal health record
The rapid development of new technologies, such as fifth-generation technology, Bluetooth, Wi-Fi, and the Internet, has driven the application of mobile networks in preventive health care. According to a report by Research And Markets, 3 the global mobile health market size is expected to reach $311.96 billion by 2027, growing at a CAGR of 33.5% from 2020 to 2027. The increasing adoption of smartphones and the growing need for remote patient monitoring are some of the key factors driving the growth of the mobile health market, including mPHRs applications.
Furthermore, the global PHR market size was valued at $2.16 billion in 2020 and is expected to grow at a compound annual growth rate (CAGR) of 19.5% from 2021 to 2028. 4 This growth can be attributed to factors such as increasing adoption of digital technologies, government initiatives to promote the use of personal health records, and rising healthcare expenditure.
Overall, the use of mPHRs applications is expected to continue growing globally in the coming years. 5
For instance, the Apple Health app provided by Apple integrates data from multiple health care sources to allow its users to view their aggregated health data. 6 Other mPHR apps, which provide data such as long-term exercise, diet, and health index records, have also become increasingly prevalent. Advanced mPHR apps can even access AI big data to offer personal health analyses and advice.
In addition, the use of mPHR applications has the potential to improve patient engagement and self-management. With the convenience and portability of mobile devices, patients can easily access their health information and track their progress towards health goals. mPHR applications can also facilitate communication between patients and healthcare providers, allowing for more timely and efficient health care delivery.7,8 Overall, the integration of mobile networks and PHR applications has the potential to revolutionize preventive health care and improve health outcomes for individuals. 8
Other mPHR apps, which provide data such as long-term exercise, diet, and health index records, have also become increasingly prevalent. Advanced mPHR apps can even access AI big data to offer personal health analyses and advice. In general, mPHR data transfer and exchange are divided into three types: (1) data sharing among medical institutions, (2) individuals sharing their personal health data with their health care providers, and (3) individuals sharing their personal health data on health-related social networks. 9
Although a large number of individuals have experiences in using mPHR services, most mPHR apps have low market shares and low long-term usage rates. Therefore, popularizing such apps and encouraging people to continue using them are an urgent matter.
In this study, we define mPHR as a multimedia application that connects through wearable devices such as Apple Watch, Garmin wristbands, Xiaomi wristbands, etc. for real-time monitoring of data, providing assistance in recording exercise, diet, and health check records, and even offering personal health analysis and suggestions.
The key lies in its mobile nature, such as being able to count the number of steps and calories burned at any time, or monitoring heart rate. Therefore, wearable devices must connect data to the mobile app at all times, which then instantly connects to the cloud through the mobile networks for real-time data feedback to users. Continuous, real-time, and instant monitoring through mobile networks is essential, such as detecting blood pressure through Apple Watch and sending alerts via the mobile app. We investigated how mPHR apps can be used to help users track their own health status and identified the major factors that promote continued mPHR app usage.
Task-technology fit
TTF was first proposed by Goodhue and Thompson in 1995 and used to explain the technology and task support capability. It was used to describe users who adopt a technology only for tasks that are suitable for them and that improve their performance. 10
Both task and technology characteristics affect the TTF, which in turn determines the performance and usage rates of users. The degree of fit between a technology and a task is the degree to which technology characteristics meet task demands. 11 Previous studies have mostly emphasized the performance effect of task and technology characteristic fit on users. Other relevant studies have also been performed, for example, on the social-technology fit proposed by Lu and Yang in 2014. Within the temporal/spatial background available at the time, the use of technology was intended to improve task efficiency.
One of the limitations of the TTF is that it does not consider the fit between individuals and tasks. Therefore, Ammenwerth et al. 12 proposed a fit between individual, task, and technology (FITT) framework, which considers the fit among user characteristics (e.g. self-efficacy and motivation), technology (e.g. function, usefulness, and performance), and tasks (e.g. complexity and effort). Their results indicated that the FITT framework was effective13,14 and that achieving a fit between inclusive tasks and individuals is crucial when individuals voluntarily complete tasks.
Several studies have discussed the applications of new technologies with the TTF model. 15 For example, Lu and Yang 16 combined TTF and social networking to explore the purpose of using Facebook among users. The results obtained indicated that Facebook was not intended to meet task needs. Instead, because of the social needs present, social-technology fit was more suitable than TTF for discussions. In another study, Vongjaturapat et al. 17 combined TTF and (Unified Theory of Acceptance and Use of Technology, UTAUT) models to explore the applications of tablet devices in libraries. The results indicated that tablet device guides and search systems can help users more conveniently and quickly access library resources.
Vanduhe et al. 18 combined TTF, TAM, and social motivation (SM) models to investigate the factors influencing knowledge gained from gamification. The results indicated that TAM models can be enhanced by TTF and SM models, TTF models can be used to verify the effects of gamification, and SM models can be used to verify social influence and recognition. In another study, Aljukhadar et al. 15 used TTF to examine the drivers and consequences of users successfully completing tasks in online environments, and the results obtained supported TTF predictions. Therefore, website information quality and ease of use are considered the only major technology factors encouraging users to successfully complete information tasks. Several studies have highlighted a positive correlation between TTF and individual performance.19–22
Further studies are required to gain a deeper understanding of the effectiveness of TTF models in different contexts. So far, how favorable TTF affects the use of mPHR apps and whether TTF affects continued app usage remain unclear. In this study, we described TTF as the extent to which ITF, STF, and TTF allow determining how TTF affects mPHR app usage.
Social capital
Social capital can be traced back to the social exchange theory (SET) in the 1950s. The SET discusses organizational structures based on interpersonal interactions and behavior models.23,24 This theory was established on the basis of interpersonal trust and reciprocity.25,26 According to Bourdieu, 27 social capital is a common capital based on online resources, built on stable, long-term network relationships and created from the constant interactions among members. Nahapiet 28 maintained that social capital is a social structure resource composed of different social structural elements and accumulated through relationships among people, offering people convenience. This social capital plays a critical role in the social relationships and network patterns between organizations and individuals.27–29 According to Putnam, 30 networks, norms, and trust allow people to use social capital to more effectively accomplish their goals in their social lives. By contrast, Ghaffar and Hurley 31 identified social capital as the ability to connect with people and form connections among otherwise unrelated individuals.
In online environments, members interact and exchange information and knowledge to create valuable resources.32,33 Social capital has become a core concept in business, politics, economy, and sociology. 34 Unlike financial and physical capital, which can be easily transferred, and human capital, which can easily flow, social capital is closely related to organizational development and strategies.33,35
Several studies have emphasized the applications of social capital 36 on websites, 37 blogs, 38 and social media platforms.39,40 In addition, various researchers have gradually reached a consensus regarding social capital; that is, the value of social capital stems from the resources generated by individuals participating in social networks. 35 These effects of social capital exist not only among small groups and individuals but also among large-scale enterprises, social media platforms, and even countries.30,35,41 According to Xu and Saxton 36 and Saxton et al. 42 failure to prioritize the accumulation of social media capital, preserve social capital, and translate social capital into organizational outcomes may prevent obtaining meaningful organizational results through social media. Ghaffar and Hurley 31 interpreted social capital as the capability of connecting with people and drawing links between them even in the absence of connections. In another study, Li et al. 32 reported that valuable resources can be shared on the Internet through interactions among people and the exchange of information and knowledge. Habes et al. 43 highlighted a positive correlation between the sharing behavior of Facebook users and social capital.
According to Lee et al., 44 increased usage of social media is associated with increased social capital. Several studies have indicated that the Internet increases the social capital of users, provided that their purpose is to obtain information and form communities. However, if their intention is to seek entertainment and recreation, then the Internet may reduce their social capital.45–47 Hence, when a new technology is used in providing services, the factors affecting social capital are not only the technology itself but also the method of using it.
Several methods can be used to classify social capital. Currently, social capital is generally classified according to capital type, bonding type, and centrality.48–50 Putnam 29 classified social capital into bonding and bridging types. With relevant studies becoming increasingly available, other scholars have divided social capital into bonding, bridging, and linking types.51–55 Bonding social capital is often observed in individuals approving others and having close relationships with others, and it involves trust and cooperation.52–54 However, bonding social capital involves a weak relationship, in which individuals obtain useful information and opinions from scattered personal connections in the absence of emotional support. By contrast, bridging social capital involves a strong relationship, in which members of related communities or groups (e.g. people of the same race, nationality, and religion) form bonds and establish emotional intimacy.29,52,53,56 Linking social capital is a vertical link, in which individuals or organizations clearly and correctly cross online boundaries.52–54
Nahapiet and Ghoshal 33 divided social capital into three dimensions according to resource orientation: a structural dimension, a relational dimension, and a cognitive dimension. The structural dimension focuses on the bonding and networks among individuals, for example, who individuals connect with and how they connect with each other. 57 The relational dimension refers to the creation of assets in interpersonal relationships and the changing of behavior through such assets to achieve a sense of identity or prestige.28,33 The cognitive dimension emphasizes interactions among individuals while sharing knowledge with each other, which produces common languages and symbols over time and makes consistent ideas and visions within networks to form internal norms.33,58,59
Ghahtarani et al. 60 used the structural, relational, and cognitive dimensions and the perspectives of social capital and social interactions to investigate the effects of knowledge and information sharing on the purchase intentions of customers in business environments. Their results indicated that social capital and social interactions affected knowledge sharing and that knowledge sharing affected the purchase intentions of customers. In another study, Kim et al. 61 examined the relationships among perceived benefits, perceived social capital, and social capital across female blog readers. They also examined the effects of relational dimensions on blogging. Their results indicated that social capital, in the structural and cognitive dimensions, facilitated relational dimension development, which in turn affected the level of loyalty of readers toward blog articles.
In the present study, social capital indicated that the relationship networks of individuals or social units using mPHR apps can be transformed into actual and potential resources. Because no studies have yet explored the effects of mPHR apps on the basis of social capital theories, we used the three-dimension concept of social capital proposed by Nahapiet and Ghoshal 33 as our theoretical foundation.
Research model and hypotheses
To explore the key factors affecting continued mPHR app usage among users, we developed a theoretical framework based on a TTF model and social capital. Figure 1 shows the proposed research model with technology and social lock-in. We proposed that the three dimensions of ITF, STF, and TTF are relevant for explaining relevant technology fit and that the three dimensions of structural, relational, and cognitive capital are relevant for explaining relevant social capital.

Proposed research model.
Technology fit and lock-in
Among different individuals, the mPHR app technology lock-in generated by ITF relies on ITF-related factors. These factors include whether the technology functions match the individuals’ habits and abilities, whether these habits and abilities match the assessment indices, and whether these assessment indices match the health goals. 62 For this purpose, technology is used to collect personal data, health records, behavioral data, and smart physical fitness data from users over time to design mPHR apps that can match their living habits, determine their physical fitness, allow them to be independent and burden-free, and meet their needs. Because mPHR apps accumulate the personal records of users over time, they create technology lock-in effects that discourage such users from switching to other mPHR apps. Therefore, we proposed the following.
Individual-technology fit positively affects technology lock-in.
Generally, STF implies that all measurement devices are compatible and synchronized, which makes mPHR apps reliable, timesaving, easy to implement, and efficient. 63 However, directly connecting mPHR apps to multiple devices is technically difficult and requires license fees to be paid to the device manufacturers, resulting in data asynchrony problems for several similar mPHR apps available on the market. High-tech, high-cost synchronization technology creates technology lock-in effects, which discourage users from switching to other mPHR apps. Therefore, we proposed the following.
Synchronicity-technology fit positively affects technology lock-in.
TTF refers to how mPHR app functions match user tasks to be performed; 64 that is, technology can help users improve their health. When mPHR apps complete tasks such as identifying food and offering exercise and health management advice, propose diversified health goals, and provide gamified task interactions and smart consultation services, users start experiencing TTF and technology lock-in effects, which discourage them from switching to other mPHR apps as long as the current app functions meet their expectations. Therefore, we proposed the following.
Task-technology fit positively affects technology lock-in.
Social capital and lock-in
Social capital was originally used to describe relational resources in personal relationships. These resources are useful for the development of individuals in social communities and social organizations. Several studies have applied this concept to various social phenomena. 65 In this study, we defined social capital as the sum of the actual and potential resources embedded within, available through, and derived from the network of relationships of an individual or a social unit.33,66 These resources of social communities and networks are influenced by the participants connected in the networks. 2 Several researchers have discussed bridging and bonding by using bonding capital 29 or network centrality, degree centrality, closeness centrality, betweenness centrality, and eigenvector centrality with individuals as nodes.32,61 In the present study, we adopted the three-dimension concept of social capital (i.e. structural, relational, and cognitive capital) proposed by Nahapiet and Ghoshal 33 as our theoretical foundation.
Structural capital
The structural dimension of social capital refers to the connection pattern, such as who to reach and how to reach them, among the different members of a network. 33 mPHR apps are used to strengthen network ties and configurations in organizations, triggering social lock-in. In other words, social capital is derived from the network ties of users. 67 When mPHR app users communicate with each other, participate in health promotion activities, or share health promotion information with each other on their mPHR apps, their bonding and interactions create social lock-in effects. Therefore, we proposed the following.
Structural capital positively affects social lock-in.
Relational capital
The relational dimension of social capital forms over time through interactions 2 , making it an interpersonal-relationship-based capital. 65 Ko and Cho 68 found that social factors and information sharing are important factors that influence the intention to use mPHR. Their study showed that if a participants’ family and friends use a PHR system, they are more likely to use it themselves. Furthermore, the study also revealed that one of the primary purposes of participants using a PHR system is to share personal health information with others, including healthcare facilities, providers, and other users.
Users develop close relationships, collective consensuses, norms, and trust in their organizational and social systems by constantly interacting with other users on mPHR apps.69,70 mPHR app users also develop personal relationships, mutual respect, mutual trust, high reciprocity, personal friendships, and personal interactions with other app users, resulting in social lock-in effects, which drive them to manage their health together. Therefore, we proposed the following.
Relational capital positively affects social lock-in.
Cognitive capital
The cognitive dimension of social capital refers to group members explaining and understanding matters together to reach a consensus. 2 This dimension can help realize meaningful communication among individuals; provide a reference or framework for behaviors and actions 2 ; and promote common knowledge, shared culture, and shared goals. When mPHR app users interact with each other, they use common or professional terms, intelligible communication methods, easy-to-understand narrative forms, shared health promotion goals and values, and similar health management methods (or task indices). Therefore, we proposed the following.
Cognitive capital positively affects social lock-in.
Continued usage
Several studies have explored the strategies used to influence the continued app usage of users experiencing technology lock-in. These strategies include continued usage due to favorable technology quality and continued usage due to social norms (i.e. because most people are using said technology, other users are forced to use the same technology). 71 Technologies featuring favorable quality, data that can be continuously accumulated, accurate smart assessments, and functions that meet people's needs trigger technology lock-in, increasing the willingness of users to continue using the same technology. Therefore, we proposed the following.
Technology lock-in positively affects continued usage.
Social lock-in uses network externalities, including participation, trust, and exchange externalities, to enhance the attractiveness of mPHR apps. If social capital can help approve or support strong and weak bonding 72 and encourage different people and people with the same health mindset to use mPHR apps, 73 then this may allow such individuals to meet new people from different communities, 74 which results in a collective effect for everyone using the app and creating social lock-in. Therefore, we proposed the following.
Social lock-in positively affects continued usage.
Research methods
We employed SEM for testing and used AMOS 22 to assess relevant convergent and discriminant validity and verify the study hypotheses and structural model framework.
Sampling and data collection
The purpose of this study was to identify the factors that contribute to the continued usage of the mPHR app among users in Taiwan. To achieve this goal, the survey was restricted to individuals who had previously used the mPHR app. Participants were solicited through a web-based survey because the mPHR is virtual. All participants were solicited through a web-based survey because most of them are Internet users. According to Tan and Teo, 75 online questionnaires offer several advantages over offline, paper-based questionnaires. Online questionnaires are associated with lower costs and faster responses and are not restricted by geography. We used Surveycake (https://chief.surveycake.biz/s/MvoZl) to construct our web-based survey and placed several survey messages on popular health and sports websites, relevant Facebook pages, and Taiwan's health-related bulletin board systems. Those who clicked on the questionnaire URL were led to the survey.
In our questionnaire survey, it is important to note that participation in the survey was entirely voluntary, and participants were explicitly informed about the purpose of the study and their rights as respondents. Before proceeding with the questionnaire, participants were required to provide their informed consent by acknowledging their understanding and agreement to participate. Participants who did not provide consent were excluded from the survey. The survey was designed to ensure the privacy and confidentiality of respondents’ information, and the data collected were used solely for research purposes.
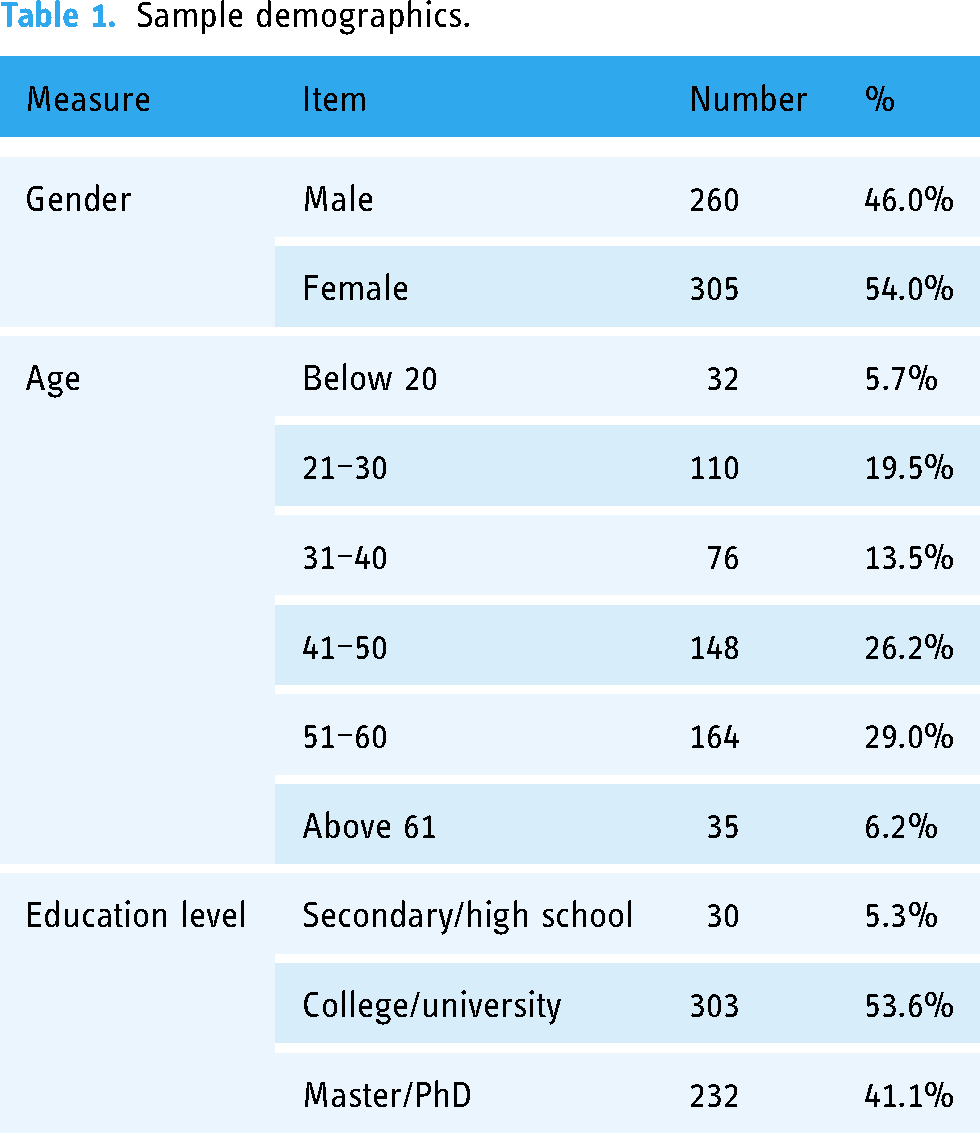
A total of 565 complete and valid responses were obtained, corresponding to 260 (46%) male and 305 (54%) female respondents. The largest age group was 41–60 years of age, accounting for 52.2% of all respondents. Most of the respondents had either undergraduate (53.6%) or graduate (41.1%) degrees. Table 1 summarizes the demographics of the respondents.
Sample demographics.
Variable measurement
The aim of this research is to investigate the continued use intention of mPHR applications. Specifically, the study aims to examine respondents’ experiences with or use of mPHR applications, which are multimedia applications designed for smartphones or tablet devices that combine mobile apps, and wearables devices provide recording assistance for activities such as exercise, diet, and health checkups, and some even provide personal health analysis. Examples of such applications include the Apple Watch app, Xiaomi Watch app, Garmin Watch app, and others that are available on smart devices.
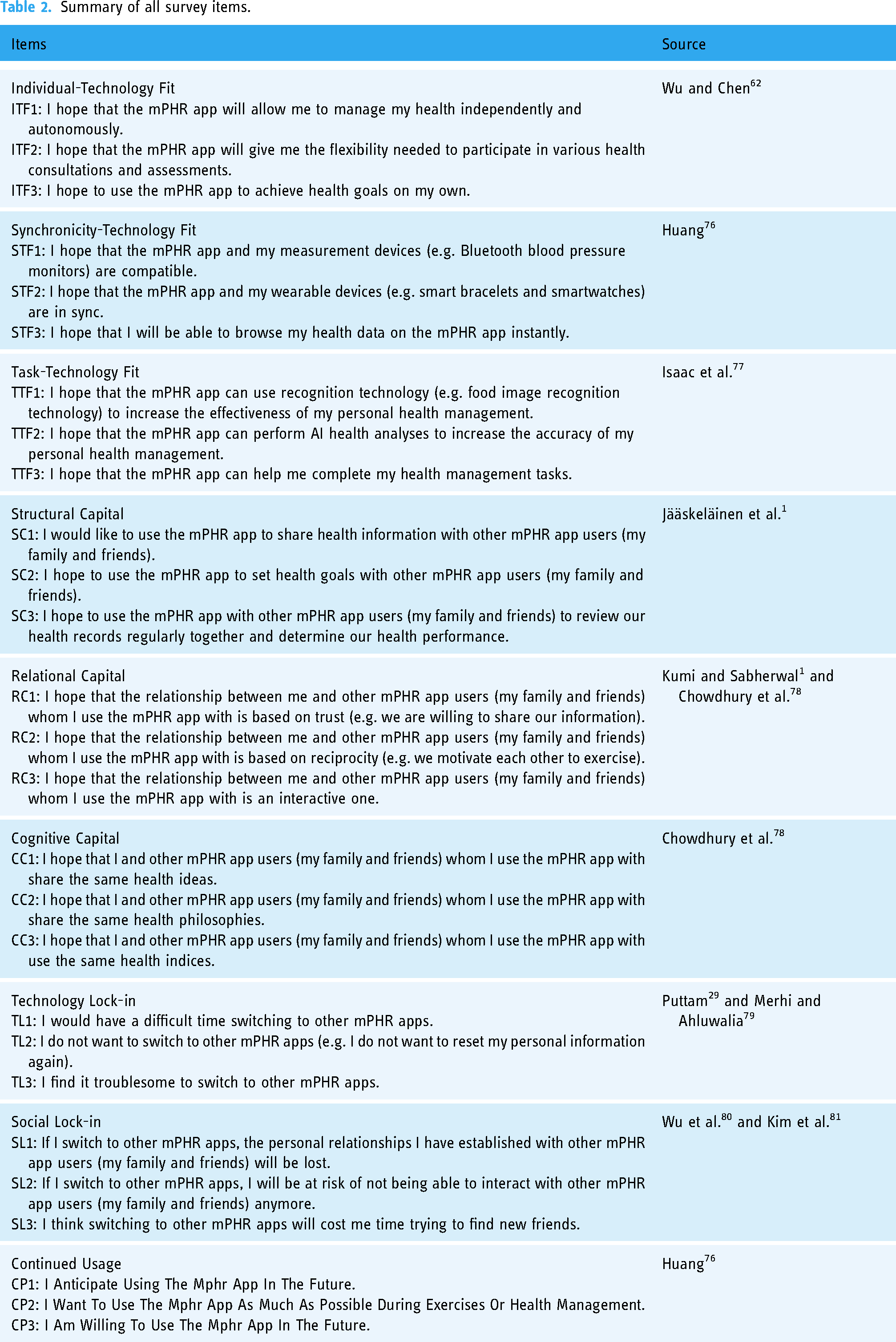
The data collected through this questionnaire will only be used for academic analysis and will not raise any privacy concerns. All survey questions are based on your actual experience and personal cognition. Additionally, it should be noted that all survey questions in this study were measured using a 5-point Likert-type scale, with responses ranging from 1 (strongly disagree) to 5 (strongly agree). Table 2 summarizes all the survey items.
Summary of all survey items.
Tests of the measurement model
Our study had a sample size of 565, which was calculated based on the number of observed variables in the SEM model. The observed variable sample size is the sum of the sample size of all observed variables in the SEM model. This method is usually used in studies with existing samples and can be calculated using the following formula: Sample Size = (Number of Indicators × 10) / Minimum Sample Size per Indicator. Where Number of Indicators refers to the total number of observed variables in the SEM model, and Minimum Sample Size per Indicator refers to the minimum sample size required for each observed variable, which is usually 5–10 observed samples. It depends on the number of questions in the questionnaire. It is recommended that the number of pre-test samples should be 3–5 times or 5–10 times the number of subscale questions that are the most pre-examination questions.82,83 There are 27 questions in this research, which have reached the standard.
Based on the formula for sample size calculation, which suggests a minimum sample size of 27 multiplied by a factor of 10, the required sample size for this study would be 270. However, it is worth noting that the final sample size for this study was 565, which exceeds the recommended standard. This larger sample size allows for a more robust and representative analysis of the research variables, enhancing the generalizability and reliability of the study findings. The increased sample size also provides greater statistical power to detect potential relationships and effects within the data. Therefore, it can be concluded that the final sample size of 565 participants in this study meets and surpasses the recommended standard, ensuring the validity and accuracy of the research results.
To test the measurement model, AMOS 22 was used for confirmatory factor analyses. Overall model-fit indices were adapted to the benchmarks of Hair et al., 84 revealing adequate fit to the collected data, χ2/df = 2.245 (≦3), goodness of fit index (GFI) = 0.923 (≧0.9), adjusted goodness of fit index (AGFI) = 0.889 (≧0.8), normed fit index (NFI) = 0.953 (≧0.9), comparative fit index (CFI) = 0.973 (≧0.9), and (root-mean-square error of approximation) RMSEA = 0.047 (≦0.08).
Cronbach's α and composite reliability (CR) were used to assess the internal consistency of the model. Hair et al. 84 recommended a minimum Cronbach α value of 0.7. The CR standards are as follows: (1) all indicator factor loadings should exceed 0.5, 84 (2) the CR value should exceed 0.6, and (3) the average variance extracted (AVE) value should exceed 0.5. 85 Table 3 summarizes the analysis results.
Statistics of construct items.

FL: factor loadings; CR: composite reliability; AVE: average variance extracted; SD: standard deviation; α: Cronbach's α.
According to Fornell and Larcker, 85 to achieve discriminant validity, the AVE values of the dimensions themselves should be greater than the square of the correlation coefficients of the other dimensions. As shown in Table 4, the square of the correlation coefficients of the other dimensions was greater than the AVE value of only one of the dimensions. Therefore, a bootstrap was used to calculate the 95% confidence interval of the correlation coefficients among the dimensions. None of the correlation coefficients contained 1, indicating that the dimensions of the measurement model were different and verifying their discriminant validity. These results indicated that this measurement model exhibited favorable reliability, convergent validity, and discriminant validity.
Discriminant validity.
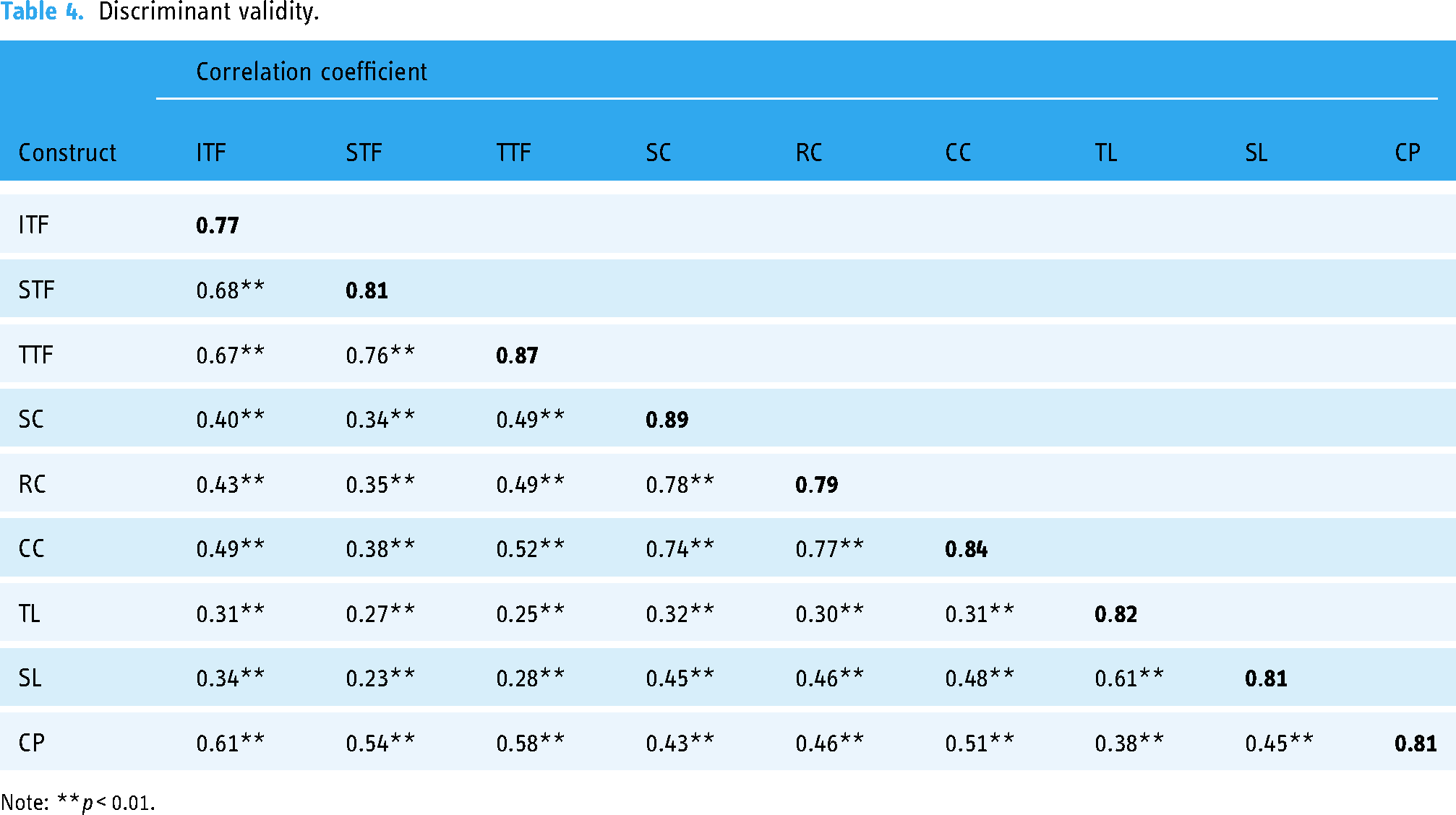
Note: **p < 0.01.
Results of the structural model
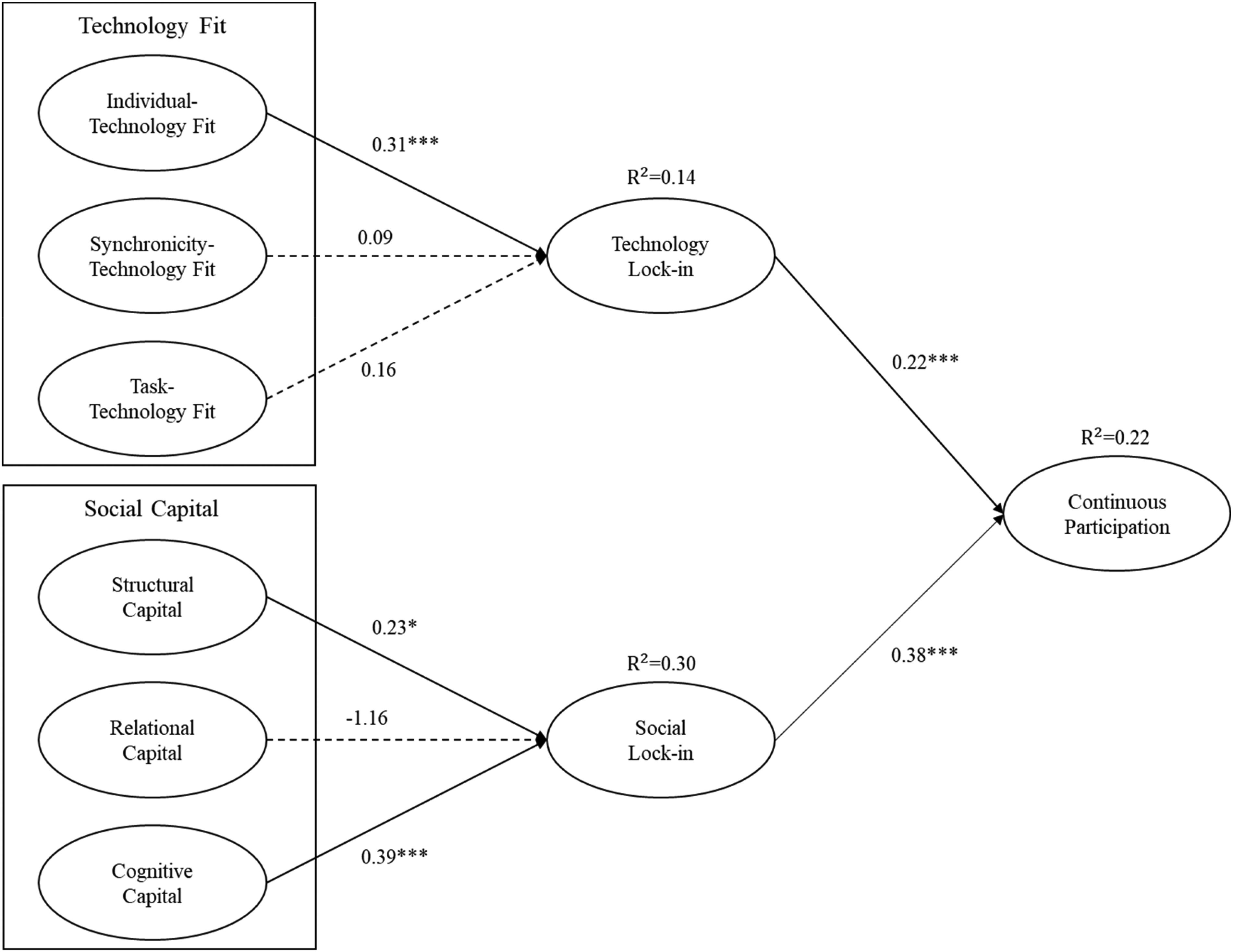
SEM was used to test the structural model in AMOS 22, and the results are presented in Figure 2. The algorithm results provided an R2 value, which constituted 22%, 14%, and 30% of the variance in continued usage, technology lock-in, and social lock-in, respectively.
AMOS 22 results for the structural model.
The path coefficient among the constructs and the significance of each hypothesis were examined. Figure 2 shows the final model paths of hypothesis testing. The results indicated that ITF (β = 0.31, P < 0.001) positively affected technology lock-in, hence supporting H1a. However, the hypotheses that STF (H1b) and TTF (H1c) affect technology lock-in were rejected. Both structural capital (β = 0.23, P < 0.05) and cognitive capital (β = 0.39, P < 0.001) had a considerable effect on social lock-in, hence verifying H2a and H2c. However, because decentralized value exchange did not affect 3D interactivity, H2b was rejected. Similarly, because relational capital did not affect social lock-in, H2b was rejected.
Finally, the results indicated that technology lock-in (β = 0.22, P < 0.001) and social lock-in (β = 0.38, P < 0.001) considerably affected continued usage, hence supporting H3 and H4.
Subgroup effects of user level
As shown in Table 1, the participants were divided into three age groups (under 30, from 31 to 50, and above 51 years of age) to compare the effects of technology and social lock-in on continued usage. The results obtained are presented in Figure 3.

Results of multiple group analysis.
Discussion
In this study, we investigated the factors that affect the willingness of users to continue using mPHR apps. The results indicated that technology and social lock-in significantly affected the willingness of users to continue using mPHR apps (β = 0.38, P < 0.001) and that the effects of social lock-in (β = 0.38, P < 0.001) were more pronounced than those of technology lock-in (β = 0.22, P < 0.001).
The study model results further indicated that, among the three technology fit dimensions, only ITF had considerable effects on technology lock-in. Path analysis revealed that neither STF nor TTF exhibited considerable effects on technology lock-in. However, as shown in Table 4, the bivariate correlation coefficient between STF and technology lock-in and that between TTF and technology lock-in were 0.27 (P < 0.01) and 0.25 (P < 0.01), respectively, indicating significant correlations. This implies that STF and technology lock-in and TTF and technology lock-in may exhibit spurious correlations and that their effects can be realized only through ITF.
Among the dimensions of social capital, both structural and cognitive capital had considerable effects on social lock-in, with the effects of cognitive capital being greater than those of structural capital. By contrast, relational capital did not have any considerable effects on social lock-in. Although relational, cognitive, and structural capital all had high correlation coefficients, at 0.77, 0.78, and 0.74, respectively (two-star levels), the construct validity results confirmed that the three dimensions were independent of each other and should not be viewed as one dimension.
The correlation coefficients of relational, cognitive, and structural capital were high. However, the variance of relational capital was explained. From the perspective of correlation coefficients, in multivariate paths, the paths affect each other. The data obtained herein indicated that relational capital had a spurious correlation with structural capital or with cognitive capital and that cognitive and structural capital were directly correlated with social lock-in. In other words, the users continued to use mPHR apps because of the close relationships between them and their families and friends. The effects of such relationships on social lock-in may be due to the effects of cognitive or structural capital.
If the data shared by users benefit them, they will continue to use the system. However, if not, they will stop using the system. Several studies have indicated that users who share systems with their families and friends are likely to continue using these systems.86,87 However, in the present study, we determined that these effects are not direct; that is, users are locked in if they only experience mutual benefit.
We investigated whether technology or social lock-in affected continuous mPHR app usage among different participant groups. The participants were divided into three age groups: under 30, from 30 to 50, and above 50 years of age. Those under 30 years of age were classified as the first Internet generation, with an R2 value of 0.48, indicating the substantial effects of social lock-in on their continued mPHR app usage. However, technology lock-in did not have any effect on their continued mPHR app usage. This was because these participants were highly familiar with the Internet and mobile phone technology and therefore did not have any problems switching to other mPHR apps. Thus, they were more concerned with social capital than with the inconvenience of technology shifts.
Those aged 30 to 50, who were introduced to the Internet era after they had started working, were also familiar with the Internet and mobile phone technology and did not have any problems switching between technologies. For this group, who also valued social capital, the effects of technology and social lock-in on their continued mPHR app usage were considerable. However, the effects of social lock-in were greater than those of technology lock-in.
Those aged above 50, who had an R2 value of 0.22, were introduced to the Internet era after they had retired. Both technology and social lock-in strongly affected their continued mPHR app usage. Although this group valued social capital, their unfamiliarity with new technologies and mobile phone technology rendered technology switches difficult, resulting in technology lock-in having greater effects than those of social lock-in.
Conclusions
The results of this study underscore the presence of technology and social lock-in, which are influenced by technology fit and social capital, and their positive impact on continued app usage. Furthermore, the effects of these lock-in factors on continued app usage were found to vary among three age groups: individuals under 30, those aged 30 to 50, and those above 50 years old.
Theoretical contribution
Overall, this study offers the following contributions. First, several studies have primarily used the technology fit theory to explore technology usage intentions. However, they did not address fit from the perspective of social capital. Here, we used three social capital dimensions (i.e. structural, relational, and cognitive capital) to examine the structural capital formed and maintained by participants in a social structure, hence establishing the research model of this study.
Second, we successfully used a combination of TTF and social capital theory to investigate the antecedents of continued usage for mPHR. This allowed us to offer a better understanding of how the two dimensions of technology fit and social capital play a key role in continued mPHR app usage among users. These two theories can be incorporated into mPHR app study methods to facilitate relevant future studies in other domains.
Third, we identified the vital factors of continued usage in mPHR. We determined that the most notable factors affecting continued usage in mPHR are technology and social lock-in. The primary factor for the influence of technology lock-in was ITF, and the primary factors for the influence of social lock-in were structural and cognitive capital. In addition, the effects of cognitive capital were greater than those of structural capital.
Fourth, neither STF nor TTF had any considerable effects on technology fit. However, from a bivariate correlation coefficient perspective, the two variables were substantially correlated, implying that they may have spurious correlations that can be realized only through ITF. Although relational capital did not directly affect social lock-in, the related correlation coefficients revealed that relational capital may have indirectly affected social lock-in through cognitive or structural capital.
In conclusion, past research contributed to the growing body of literature on technology and social capital in promoting health and wellness. Lee et al.’s 88 review and Zhou et al.’s 89 study highlight the potential of mobile health apps in improving health outcomes but also underscore the importance of user involvement and customization to increase engagement and adoption. Kumi and Sabherwal’s 2 study sheds light on the positive impact of social capital and absorptive capacity on performance outcomes in online communities. Our study adds to this literature by examining the positive effects of technology and social lock-in on continued app usage, and how this varies among different participant groups. These findings suggest that technology fit and social capital are important factors to consider in designing and promoting the sustained usage of mobile health apps. Further research is needed to better understand the complex interplay between technology, social capital, and individual behaviors in promoting health and wellness.
Managerial implications
The results obtained in this study may be used by related industries to understand the factors affecting continued mPHR app usage among users, modify technologies and products related to mPHR apps, and stimulate the usage intention of users. These endeavors will allow industries to more easily and quickly introduce their technologies and products to the market and increase the prevalence of such technologies and products, hence achieving the goals of economic efficiency and reducing health care costs for the public and the government. The model results obtained herein indicated that both technology and social lock-in had considerable effects on continued mPHR app usage. Therefore, when designing and promoting mPHR apps, firms should not only enhance existing technological functions but also consider and target the social capital of the users.
ITF had the most pronounced effects on technology lock-in. When using mPHR apps, users care most about independently managing their own health through autonomy indicators, health counseling, and health assessments. Thus, to satisfy the new technology requirements of users, firms should provide effective, easily accessible, multifunctional devices that can monitor health data, such as electrocardiographic data and data on sleep quality, blood oxygen saturation, activity (pedometers), and calorie consumption. In this study, both structural and cognitive capital had considerable effects on social lock-in, and the effects of cognitive capital were greater than those of structural capital. Therefore, when designing mPHR apps, firms should design functions that allow users and their families and friends to develop identical health philosophies or health indices, such as health index sharing and group challenges, to achieve continued mPHR app usage.
Finally, firms should design different products and market them according to the various demands of different age groups. For example, for users under 30 years of age, firms should focus on social lock-in. For users aged between 30 and 50, firms should focus on both social and technology lock-in, with more focus on social lock-in. For users above 50 years of age, firms should focus on technology lock-in.
Limitations and future research
Despite its useful findings and implications, this study has the following limitations. First, the study participants were limited to those who use mPHR apps. Therefore, future studies should target other mobile Internet applications and examine the main factors affecting them.
Second, we used quantitative methods to explore the factors affecting continued mPHR app usage among users and distributed an online questionnaire to a large and demographically diverse sample.
Third, our results indicated that STF and TTF were highly correlated and exerted their effects only through ITF. Although relational capital did not directly affect social lock-in, the correlation coefficient results indicated that relational capital indirectly affected social lock-in through cognitive or structural capital. This finding may serve as a hypothesis in future studies.
Fourth, we utilized quantitative methods to investigate the factors that influence the continued usage of mPHR applications. To avoid potential bias that could affect the results, we distributed an online questionnaire to a large and diverse sample. However, relying solely on the questionnaire may not be sufficient to comprehensively assess the intentions of participants using mPHR applications. This is because individual users may assign different weights to the various factors that determine their intention to use the application, and the survey itself may be prone to self-selection bias. 90 Therefore, we recommend adopting an interview-assisted quantitative perspective in future studies.
Fifth, because we used a convenient sample from a province in Taiwan, the results obtained herein cannot be extended to other geographical locations. Therefore, future studies should compare the attitude of Taiwanese people with that of people from other countries.
Finally, in future research, collecting relevant usage data and anonymizing it can provide deeper insights into the sustainability of mPHR usage.
Supplemental Material
sj-docx-1-cet-10.1177_20552076231181216 - Supplemental material for Which are the vital factors of mobile personal health records applications that promote continued usage? A perspective on technology fit and social capital
Supplemental material, sj-docx-1-cet-10.1177_20552076231181216 for Which are the vital factors of mobile personal health records applications that promote continued usage? A perspective on technology fit and social capital by Yao-Yuan Liu, Hsi-Peng Lu and Chiao-Shan Chen in DIGITAL HEALTH
Footnotes
Acknowledgments
The author team would like to acknowledge the non-author members of the advisory committee for sharing their experience and perspective to help shape this review.
Contributions
YYL conceived the study; YYL and HPL conducted literature searches and project administration the research. Analyzed the data with support from CSC. YYL and CSC wrote the first draft of the manuscript; all authors reviewed and edited subsequent versions and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The objective of this study was to explore the willingness of consumers to continue utilizing MPHR apps. The survey was conducted among individuals who had previously utilized relevant apps and were asked to rate their own awareness level using a Likert scale ranging from 1 to 5, no personal information or data related to human experiments was gathered during the survey. Given that this study is a scoping review of the existing research model, ethics committee approval was not required. It is worth noting that our questionnaire survey involved user APP ordinary, rather than patients, and we did not collect any personal health or privacy data from them. Hence, there is no need for an IRB or disclaimer certificate.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
YYL.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.