
Abstract
Background
mHealth can help with healthcare service delivery for various health issues, but there's a significant gap in the availability and use of mHealth systems between sub-Saharan Africa and Europe, despite the ongoing digitalization of the global healthcare system.
Objective
This work aims to compare and investigate the use and availability of mHealth systems in sub-Saharan Africa and Europe, and identify gaps in current mHealth development and implementation in both regions.
Methods
The study adhered to the PRISMA 2020 guidelines for article search and selection to ensure an unbiased comparison between sub-Saharan Africa and Europe. Four databases (Scopus, Web of Science, IEEE Xplore, and PubMed) were used, and articles were evaluated based on predetermined criteria. Details on the mHealth system type, goal, patient type, health concern, and development stage were collected and recorded in a Microsoft Excel worksheet.
Results
The search query produced 1020 articles for sub-Saharan Africa and 2477 articles for Europe. After screening for eligibility, 86 articles for sub-Saharan Africa and 297 articles for Europe were included. To minimize bias, two reviewers conducted the article screening and data retrieval. Sub-Saharan Africa used SMS and call-based mHealth methods for consultation and diagnosis, mainly for young patients such as children and mothers, and for issues such as HIV, pregnancy, childbirth, and child care. Europe relied more on apps, sensors, and wearables for monitoring, with the elderly as the most common patient group, and the most common health issues being cardiovascular disease and heart failure.
Conclusion
Wearable technology and external sensors are heavily used in Europe, whereas they are seldom used in sub-Saharan Africa. More efforts should be made to use the mHealth system to improve health outcomes in both regions, incorporating more cutting-edge technologies like wearables internal and external sensors. Undertaking context-based studies, identifying determinants of mHealth systems use, and considering these determinants during mHealth system design could enhance mHealth availability and utilization.
Introduction
The emergence of digital systems, as well as the widespread availability and use of mobile phones worldwide, present a notable opportunity for improving access and equity to healthcare services. In order to enhance the delivery of high-quality medical care, mobile health (mHealth, according to WHO) applications offer tremendous potential for technology integration into clinical services. 1 It is a crucial component of eHealth, which is the secure and affordable application of information and communication technology to serve the disciplines of health and related ones. 2
The benefit of mHealth is that it can promote innovative forms of care by overcoming organizational, temporal, and geographic constraints, and it can help keep healthcare systems viable. By enhancing treatment, empowering patients, increasing adherence, providing patient-centered care, reducing medical costs, and streamlining the use of health resources, mHealth has the potential to improve the delivery of high-quality healthcare. It also increases the opportunity to deliver more consistent, coordinated, and efficient healthcare when and where it is needed and increases access to health services to isolated or underserved communities. 3
Additionally, depending on the demands made by the various health conditions, mHealth can be used for many facets of healthcare, including remote monitoring, consulting, diagnosis, reminding, informing, and patient treatment. It is obvious that more than ever, mHealth may provide a solution to many of the current healthcare issues.
Despite the enormous promise and adaptability that mHealth could offer, a number of obstacles prevent various mHealth systems from being implemented, used, or scaled up in different regions or by different users. These potential obstacles include, among others, a lack of policy and institutional frameworks, low mobile phone penetration, low acceptance among healthcare professionals and patients, regulations surrounding data security, and insufficient procedures for quality evaluation. 4
Regardless of the fact that we are in an era where the global healthcare system is being further digitalized, the availability and use of mHealth systems in developed and developing countries differ significantly. The potential benefits of mHealth in enhancing healthcare delivery and improving health outcomes are widely acknowledged. However, there remains a lack of evidence regarding their availability and utilization in both Europe and Sub-Saharan Africa (SSA). Additionally, it remains unclear whether any disparities or gaps exist in terms of their availability and use between these two regions. The main aim of this study is to review the literature focusing on differences between the availability and use of mHealth systems between Europe and SSA and to give recommendations on how mHealth can help to tackle future health issues in both regions.
The rationale for undertaking this study is to conduct an extensive and impartial evaluation of the current literature on the use and availability of mHealth systems in both Europe and SSA. This review will identify any gaps and research needs in the field, and provide a more reliable evidence base to inform decision-making and shape the design and implementation of mHealth projects. These findings can guide policymakers and stakeholders in making informed decisions about resource allocation to address these inequalities and improve overall access to mHealth technologies.
Methods
To study the use and availability of mHealth systems in SSA and Europe, a systematic review is performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 updated guidelines. 5 To make an objective comparison, the process for article search and selection was done in the same way for SSA and Europe, using the same search query (except for the words Europe and SSA) in the same databases with the same inclusion and exclusion criteria. Since this study relied on a review of secondary data obtained from published articles, the need to obtain patient consent was considered unnecessary. The study did not utilize any identifiable patient information.
Search approach
Four databases were used for the literature search: Scopus, Web of Science, IEEE Xplore, and PubMed. The search query was (“Mobile health” OR mHealth OR telehealth OR telemedicine OR “Wearable devices”) AND (“Sub Saharan Africa”) AND (Use* OR Practice OR Implementation* OR Enactment OR Application OR Operation OR Employment OR Execution OR Development OR Growth OR Expansion OR Advance OR Progress OR Change).
For Europe it is the same search query, except the search term “Sub Saharan Africa” is replaced by “Europe.” For both search queries the results were filtered, such that only articles from 2000 and onwards were given. The last date each database was searched was on December 2021.
Screening process
A title and abstract screening were performed in succession by two reviewers. The inclusion and exclusion criteria used in the screening process can be seen in Table 1. All articles that discussed the proposal, development, or implementation of a specific mHealth system were included for analysis.
Inclusion and exclusion criteria for article selection.

From each of the articles, the following data was then extracted and entered in a Microsoft Excel worksheet (the full data table for SSA and Europe can be obtained as a supplementary file. In the first column, the lead author of each included article is mentioned. In the next columns the items of each of the five categories listed in Table 2 were then be marked by 0 or 1 (only the 1's are shown in the data table), for example, if an article mentioned the development of an app-based mHealth system, a 1 was allocated to the “App” column, and so on. The data was sorted by lead author name. All included articles are also referenced in the bibliography.
Data extracted for analysis.

Results
The search query for the SSA articles yielded a total of 1020 articles of which 831 articles remained after removal of duplicates. The search query for the Europe articles yielded a total of 2477 articles of which 1605 articles remained after the removal of duplicates. After title and abstract screening, 593 articles for SSA were excluded, leaving 238 articles for further screening. 1201 articles for Europe were excluded, leaving 404 articles for further screening. The remaining articles were then assessed for eligibility for further analysis. After eligibility screening, 86 articles for SSA and 297 articles for Europe,6–386 were selected for analysis. The PRISMA flow diagram for both SSA and Europe can be found in Figures 1 and 2.

PRISMA flow diagram for mHealth articles related to SSA.

PRISMA flow diagram for mHealth articles related to Europe.
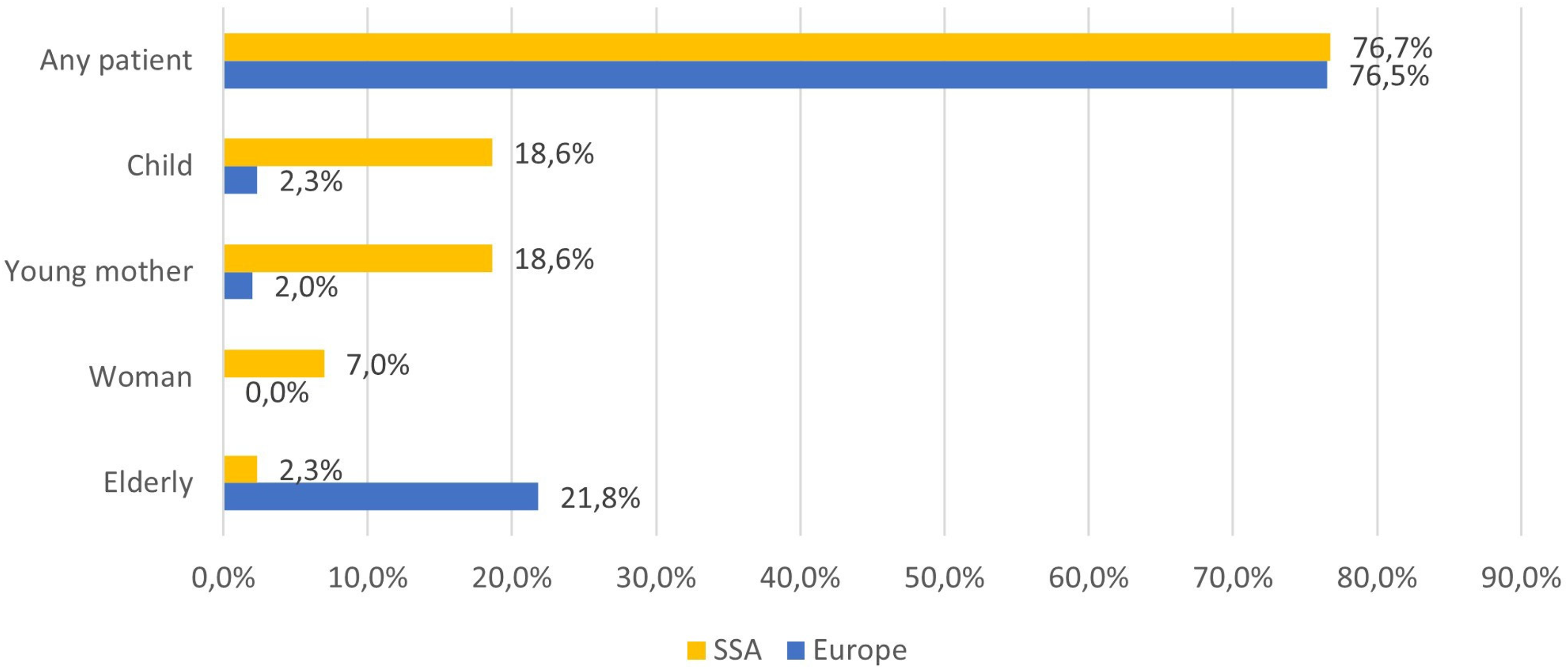
For each of the selected articles, information was extracted on five different categories: the type of mHealth system; the goal of the mHealth system; the patient; the health issue; and the development stage of the mHealth system (cf. Table 2). The complete table of data extracted from each individual article can be obtained in the research data for SSA and Europe. An overview of the results is given in Table 3. Note that within one article sometimes more than one item per category was covered—for example, when the goal of the mHealth system is monitoring and informing—such that the numbers of the items within a category do not always add up to the total number of articles.
Overview of results of the analysis.
In the following sections, the relative results of each of the five categories are presented and discussed. Again, it should be noted that percentages of items within each category could add up to more than 100% since more than one item per category is possible for one mHealth system.
Type of mHealth systems
The first category of information extracted from the articles was the kind of mHealth system that was used. The relative number of results for each kind of mHealth system is presented in Figure 3.

Type of mHealth system used in sub-Saharan Africa (SSA) and Europe.
Goal of mHealth systems
The second category of information extracted from the articles was the goal of the mHealth system. The relative number of results for each type of goal is presented in Figure 4.

The goal of the mHealth system used in sub-Saharan Africa (SSA) and Europe.
The mHealth system's intended patient population
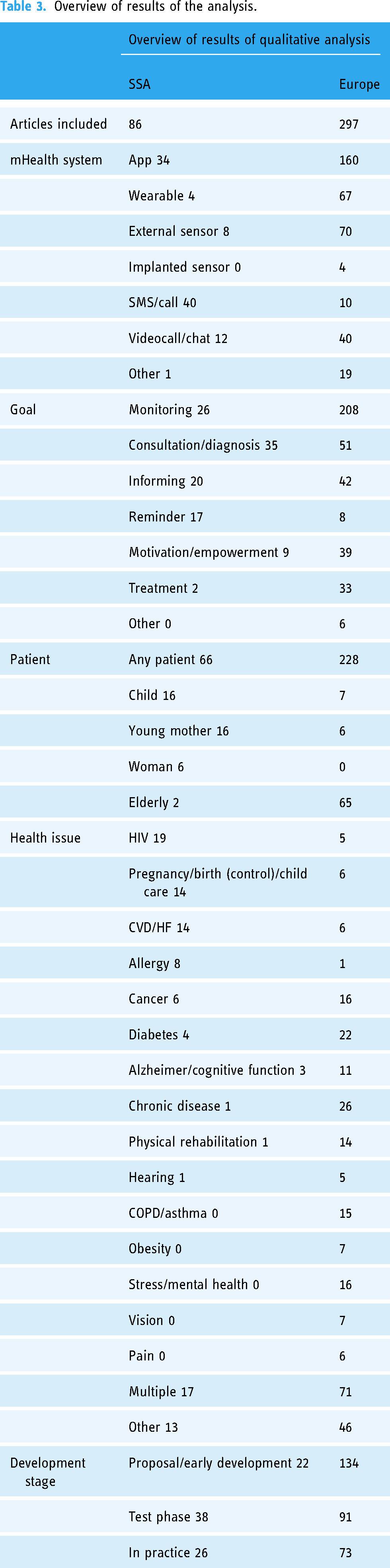
The third category of information extracted from the articles was the patient the mHealth system was used for, more specifically the age and gender of the patient. The relative number of results for each type of patient is presented in Figure 5.
The mHealth system's intended patient population is in sub-Saharan Africa (SSA) and Europe.
When looking at the target patients of the mHealth systems, we see that for both regions about three-quarters of all mHealth systems were not targeted at a specific type of patient. However, it must be noted that while not specifically mentioned, some of these mHealth systems were in fact clearly targeted towards a specific group of patients, for example, when the tackled health issue occurs mostly in elderly people.
If we look at the other patient groups, we see a big difference between SSA and Europe. The patients of the remaining mHealth systems in SSA are mostly children and young mothers. In Europe the patients of the remaining mHealth systems are elderly. This clearly coincides with the respective demographic age structures and corresponding health issues of both populations. SSA has a very young population with very high child mortality. Europe has a very old population where aging is a major health issue.
The big difference between the two regions—that is, mHealth systems used in SSA focus more towards consultation or diagnosis; informing and reminding, and mHealth systems used in Europe focus more towards monitoring—is quite logical if we take a look at what health issues the mHealth systems are used for.
Health issues addressed by the mHealth systems
The fourth category of information extracted from the articles was the health issue tackled by the mHealth system. The relative number of results for each type of health issue is presented in Figure 6. The most common health issues that were tackled by the mHealth systems in SSA were HIV (22,1%) and pregnancy/birth (control)/child care (16,3%), followed by CVD/HF (10.5%), allergy (9.3%), cancer (7.0%), and diabetes (4.7%). The stated health issues coincide well with the major causes of mortality and disease burden as seen when we assessed the health status of SSA. However, mainly lower respiratory infections, enteric infections, and malaria, which are major causes of mortality and disease burden, are clearly missing in the reported health issues addressed by mHealth systems. However, the major causes of child death are not addressed very well. Currently, only 16.3% of the reported mHealth approaches were targeted toward pregnancy, birth, and child care, and none of the other mHealth approaches were specifically targeted toward pneumonia, diarrheal diseases, or malaria in SSA. The most common health issue that was tackled by the mHealth systems in Europe was CVD/HF (23.2%), followed by chronic diseases (8.7%), diabetes (7.4%), and cancer (5.4%). These health issues coincide very well with the major causes of mortality and disease burden in Europe.

Health issues tackled by the mHealth system in sub-Saharan Africa (SSA) and Europe.
Development stage of the mHealth systems
The fifth and final category of information extracted from the articles was the development stage of the mHealth system. The relative number of results for each type of health issue is presented in Figure 7.

The development stage of the mHealth system in sub-Saharan Africa (SSA) and Europe.
When comparing the development stage, we see that on average mHealth systems in SSA are further in the development stage than in Europe. This is explained by the used mHealth technologies.
Discussion
We see that for SSA the major kind of mHealth systems that are reported are apps and SMS or call-based systems. These results are quite logical if we look at what the mHealth systems are mostly used for (the goal of the mHealth system). Notably, the adoption of wearable mHealth systems is still quite low in SSA.
In Europe, the vast majority of mHealth systems are apps, followed by wearables and external sensors. Examples of external (wearable) sensors are weight scales, heart rate sensors, smart blood pressure devices, etc. These results are again very straightforward if we look at what the goal of these mHealth systems is and what health issues they are used for.
In both regions, we also see a substantial number of videocall or chat-based mHealth systems. Many of these can be accounted to the Covid-19 pandemic, where videocalls and chat were a welcome and necessary alternative to face-to-face contact between the patient and medical personnel.
In SSA, the main goal of the mHealth systems was consultation or diagnosis followed closely by monitoring, informing, and reminding. The kind of mHealth systems used for consultation/diagnosis, informing, and reminding were mainly SMS or call-based (34.3%; 60.0%; and 100%, respectively), hence explaining their large share as seen in the previous section. Monitoring is mostly done by app-based mHealth systems (61.5%).
In Europe, we see that almost 70% of mHealth systems are used for monitoring. The main goals identified through the analysis coherence given the health issues for which the mHealth systems are used in both regions. Monitoring in Europe is mainly done by apps (55.3%), wearables (29.8%), and external sensors (28.4%). Note that the percentages add up to more than 100% because several mHealth approaches used more than one system, for example, a mHealth approach with both an app and an external sensor.
The majority of mHealth systems did not mention a specific patient, but when they did, children (18.6%), young mothers (18.6%), and women (7.0%) were the most frequent. HIV (22.1%), pregnancy/(birth) control/child care (16.3%), CVD/HF (10.5%), allergy (9.3%), cancer (7.0%), and diabetes (4.7%) were the most common health issues addressed by mHealth systems in SSA. However, it must be noted that while not specifically mentioned, some of these mHealth systems were in fact clearly targeted towards a specific group of patients, for example, when the tackled health issue occurs mostly in elderly people. If we look at the other patient groups, we see a big difference between SSA and Europe. The patients of the remaining mHealth systems in SSA are mostly children and young mothers. In Europe, the patients of the remaining mHealth systems are elderly.
The difference in target health issues of mHealth between the two regions can be partly attributed to the difference in demographic structure. SSA has a very young population with high child mortality, hence the large share of pregnancy, birth, and childcare-related mHealth approaches. Europe has an old population, where aging is a big issue, hence the large share of age-related diseases—like CVD, HF, and cancer—targeted by mHealth systems.
In SSA a large amount of the mHealth systems is SMS based. This is an older technology, which is easily implemented. In Europe, more mHealth systems are used with newer technology, such as wearables and implantable sensors. Since there is less experience and know-how on the use and implementation of those novel technologies, the development process of mHealth will take longer.
The finding that mHealth systems in SSA did not address major causes of child mortality, lower respiratory infections, enteric infections, and malaria, while European mHealth focused on health issues related to major causes of mortality and disease burden in that setting, has significant implications. This discrepancy suggests that mHealth systems may not be effectively addressing the most pressing health issues in SSA, which could result in negative consequences for human health in the region.
Conclusions
The healthcare challenges faced by SSA and Europe are not equivalent. They may differ in terms of prevalence, severity, or other factors. mHealth can be a valuable tool for overcoming these challenges. By enabling remote monitoring, diagnosis, treatment, and informing patients with a variety of diseases, mHealth can aid medical professionals. In our examination of mHealth availability and use in SSA, we discovered that SMS/call-based systems (46.5%) and apps (39.5%) were the most common. The mHealth systems’ primary objectives were consultation/diagnosis (40.7%), monitoring (30.2%), informing (23.3%), and reminding (19.8%). When looking at the target patients of the mHealth systems, we see that for both regions about three-quarters of all mHealth systems were not targeted at a specific type of patient.
In the analysis of the use and availability of mHealth systems in Europe, we found that most used mHealth systems use apps (53.7%), followed by external sensors (23.5%) and wearables (22.5%) (the percentages add up to more than 100% because some mHealth system makes use of more than one technology, e.g., an app and an external sensor). The most common goal of the mHealth systems by far was monitoring (69.8%), followed by consultation/diagnosis (17.1%) and informing (14.1%). While the majority of mHealth systems did not mention a specific patient, in the ones that did the most common were elderly (21.8%). The most common health issues that were tackled by the mHealth systems in Europe were CVD/HF (23.2%), chronic diseases (8.7%), diabetes (7.4%), cancer (5.4%), stress/mental health (5.4%) and COPD/asthma (5.0%). In our qualitative analysis, we found that other studies reported very similar results. The stated health issues addressed by mHealth coincide very well with the major causes of mortality and disease burden in Europe.
The difference in health issues addressed by mHealth between the two regions can be partly attributed to their different demographic structure. SSA has a very young population with high child mortality, hence the large share of pregnancy, birth, and childcare-related mHealth approaches. Europe has a very old population, where aging is a big issue, hence the large share of age-related diseases—like CVD, HF, and cancer—targeted by mHealth. The recent COVID-19 pandemic increased the pressure on healthcare even further with setbacks on progress in immunization coverage, malaria, tuberculosis, vaccines, and claiming the lives of front-line healthcare workers around the world. In addition to these setbacks, COVID-19 and the need for social distancing demanded the use of remote healthcare solutions in many divisions of general healthcare.
It is important to explore the potential for mHealth systems to address these health issues in SSA and ensure that mHealth systems are designed and implemented effectively in these areas. Addressing these gaps could lead to better health outcomes and a reduction in child mortality rates in SSA. Countries should develop a clear policy framework and allocate sufficient budgets to address these issues, as mHealth should not be considered a luxury but a basic necessity. It is a cost-effective way to deliver healthcare services, and it can help to fight poverty by facilitating the effective and efficient use of resources.
The healthcare challenges in different regions require unique and tailored approaches and solutions. To improve the availability and utilization of mHealth systems, it is recommended to conduct context-specific studies that identify the determinants that affect the use of these systems. These factors should then be taken into account during the design phase of mHealth systems. This approach can help address the unique healthcare challenges faced by different regions and populations and ensure that mHealth systems are designed and implemented in a way that maximizes their potential impact.
Limitations of the study
The limitation of the study is the potential impact of non-standardized data collection and reporting practices across various regions and countries. Additionally, there may be a number of mHealth implementations that have not been documented or reported in scientific literature. Given that this study is based solely on secondary sources, it is possible that some important information may be overlooked. Moreover, differences in healthcare systems and cultural variances could influence the use and implementation of mHealth technologies across different regions, further complicating the investigation. Future works should aim at exploring the potential of qualitative research methods to gain a deeper understanding of the cultural and contextual factors that impact the implementation and use of mHealth technologies and provide a more comprehensive understanding of the implementation and use of mHealth technologies in different contexts.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180972 - Supplemental material for mHealth in sub-Saharan Africa and Europe: A systematic review comparing the use and availability of mHealth approaches in sub-Saharan Africa and Europe
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180972 for mHealth in sub-Saharan Africa and Europe: A systematic review comparing the use and availability of mHealth approaches in sub-Saharan Africa and Europe by Genet Tadese Aboye, Martijn Vande Walle, Gizeaddis Lamesgin Simegn and Jean-Marie Aerts in DIGITAL HEALTH
Supplemental Material
sj-xlsx-2-dhj-10.1177_20552076231180972 - Supplemental material for mHealth in sub-Saharan Africa and Europe: A systematic review comparing the use and availability of mHealth approaches in sub-Saharan Africa and Europe
Supplemental material, sj-xlsx-2-dhj-10.1177_20552076231180972 for mHealth in sub-Saharan Africa and Europe: A systematic review comparing the use and availability of mHealth approaches in sub-Saharan Africa and Europe by Genet Tadese Aboye, Martijn Vande Walle, Gizeaddis Lamesgin Simegn and Jean-Marie Aerts in DIGITAL HEALTH
Supplemental Material
sj-xlsx-3-dhj-10.1177_20552076231180972 - Supplemental material for mHealth in sub-Saharan Africa and Europe: A systematic review comparing the use and availability of mHealth approaches in sub-Saharan Africa and Europe
Supplemental material, sj-xlsx-3-dhj-10.1177_20552076231180972 for mHealth in sub-Saharan Africa and Europe: A systematic review comparing the use and availability of mHealth approaches in sub-Saharan Africa and Europe by Genet Tadese Aboye, Martijn Vande Walle, Gizeaddis Lamesgin Simegn and Jean-Marie Aerts in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank all individuals who directly or indirectly contributed to this research.
Contributorship
Genet Tadese Aboye co-conceived the study with Jean-Marie Aerts and Gizeaddis Lamesgin Simegn. Genet Tadese and Martijn Vande Walle designed and implemented the search strategy. The title and abstract screenings were performed by Genet Tadese Aboye and Martijn Vande Walle. Genet Tadese Aboye and Martijn Vande Walle both contributed to the data synthesis and extraction processes. Genet Tadese Aboye and Martijn Vande Walle drafted the manuscript, which was revised by all authors. Jean-Marie Aerts and Gizeaddis Lamesgin Simegn supervised the review process and critically revised the manuscript for significant intellectual content. At all stages of the manuscript's development, all authors discussed the findings and read and approved the final version.
Data availability
The data extracted from the included studies is available and is provided as an attachment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
None.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
GTA
Registration and protocol
The review was not registered.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.