
Abstract
Background
In 2018, 26.6 million people were living with HIV in sub-Saharan Africa. Palliative care services are recommended for people living with HIV at all stages from diagnosis through to end-of-life. However, the provision of palliative care in sub-Saharan Africa is limited, leading to little or no access for the majority of patients. Digital technologies in sub-Saharan Africa present an opportunity to improve access to palliative care for people living with HIV in the region. This review synthesised literature on digital health interventions for palliative care for people living with HIV in sub-Saharan Africa and assessed their effects on patient outcomes.
Methods
Literature searches were conducted in MEDLINE, Embase, PsycINFO and Global Health. Inclusion and exclusion criteria were applied. Two independent reviewers conducted study screening, data extraction and quality appraisal. A narrative synthesis was performed to draw together and report findings across heterogeneous studies. Reporting of this review follows the Preferred Reporting Items for Systematic Review and Meta-Analysis checklist.
Results
Out of 4117 records, 25 studies were included, covering 3592 people living with HIV, across 21 countries. Studies included three randomised controlled trials, three qualitative, three pre- and post-test, two observational, two case series, six cross-sectional and six mixed methods studies. Telemedicine was the most reported digital health intervention, with 12 studies demonstrating the effectiveness of digital health interventions.
Conclusion
Emerging evidence suggests digital health interventions can be effective in facilitating patient-provider communication and health professional decision-making as a part of palliative care for people living with HIV. There is a need for further development and evaluation of digital health interventions alongside determining optimal approaches to their implementation as a part of palliative care provision in sub-Saharan Africa.
Introduction
In 2018, 37.9 million people were living with HIV (PLWH) globally and 26.6 million (68%) were from sub-Saharan Africa (SSA). 1 Antiretroviral therapy (ART) has transformed the HIV pandemic into a chronic disease. 2 There is a need for palliative care for PLWH as it is an integral part of HIV care from diagnosis to end of life. 3 PLWH have a high prevalence of psychological and physical symptoms, including worry, anxiety, depression, diarrhoea, constipation and insomnia. 4 When accessed, palliative care can improve patient outcomes across multiple domains. 5 Palliative care involves the prevention and relief of physical, emotional, social or spiritual suffering associated with any chronic or life-threatening illness, is fundamental to health and human dignity and is a basic human right. 6 Palliative care is an essential service within universal health coverage 7 ; in 2014, a World Health Assembly Resolution called on national governments to carry out actions to develop and strengthen palliative care. 8
Despite the need for palliative care and its positive impact on patient outcomes, coverage in SSA is greatly below need, 9 driven by a multitude of factors including unavailability, isolated services, limited funding, lack of inadequate policy and inadequate referral practices. 10 The application of digital health approaches as health systems strengthening tools has been highlighted through WHO guidance. 11 The application of information and communication technologies systems can be used to deliver one or more digital health interventions including, for example, systems for client communication, telemedicine, health management information and electronic medical records. 12 Digital health technologies can be leveraged through existing palliative care models in SSA (see Table 1) to improve access to palliative care by reaching patients in remote areas, 13 providing e-learning to healthcare providers 14 and routinely collecting data to inform policy. 15 SSA is the fastest growing consumer market for mobile phone services with 456 million unique mobile subscribers in 2018 (44% penetration rate) and is estimated to reach 623 million subscribers (50% penetration rate) by 2025. 16 Digital innovation in SSA is being driven by mobile phones. 16
Three models of palliative care in SSA.
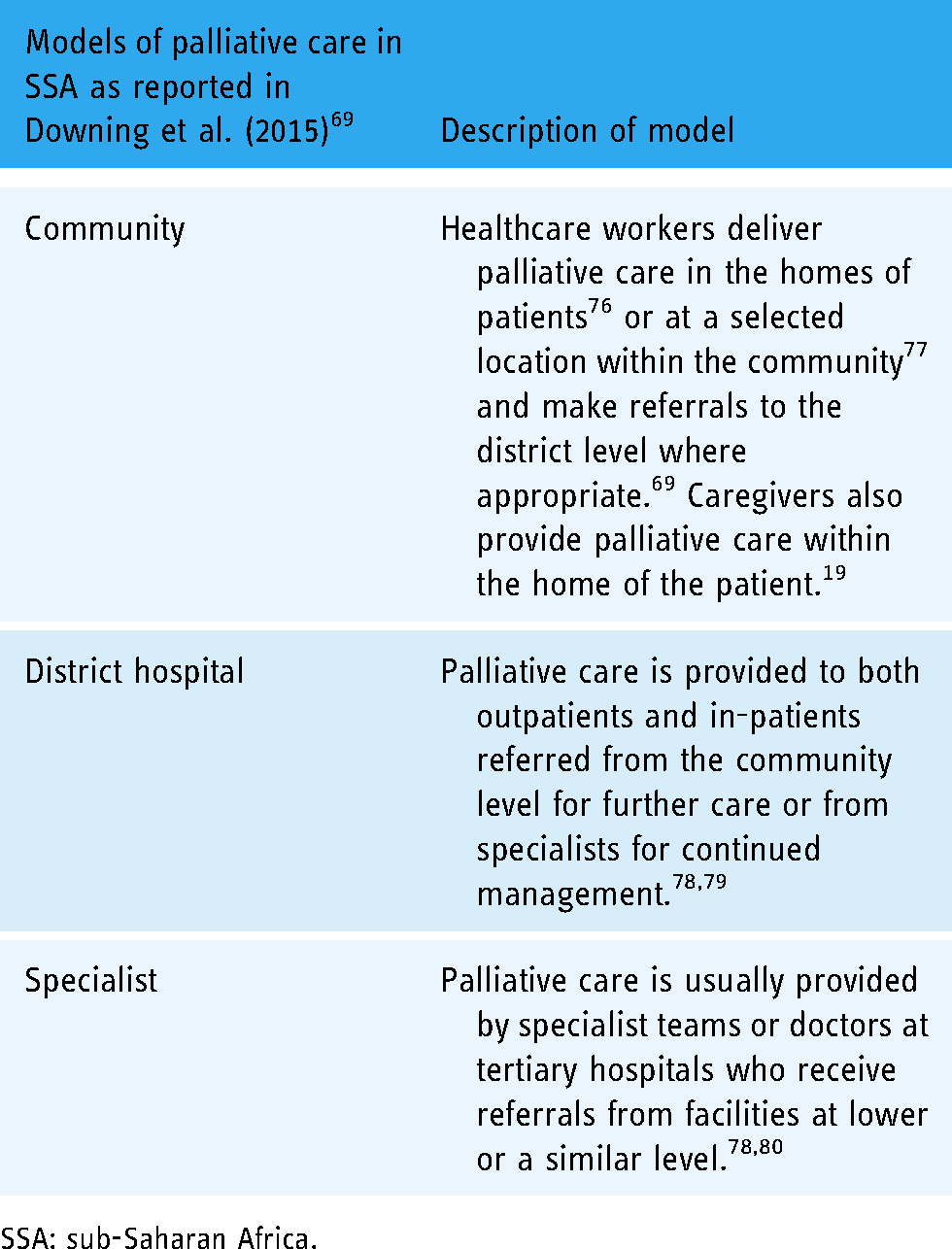
SSA: sub-Saharan Africa.
The Essential Palliative Care Package for Universal Health Coverage 17 highlights digital health as an approach to increasing access to palliative care services. A systematic review 18 of literature up until 2015 found that in SSA, mobile phones are starting to be used to improve access to palliative care by enabling patients to communicate with providers,19–21 to encourage patients to adhere to appointments 22 and for health provider education. 23 However, the evidence underpinning digital health for palliative care in SSA is still underdeveloped. 24 Emerging evidence suggests the potential of digital technologies to support PLWH with self-management, medication adherence and facilitating communication with health professionals.25,26 However, to date, there have been no reviews with a focus on digital health approaches for palliative care among PLWH in SSA. This review addresses the gap by synthesising existing literature to date and reporting on the effectiveness of digital health interventions on patient outcomes.
Methodology
Objectives
This review addresses two questions: (a) What digital health interventions are being used to provide palliative care to PLWH in SSA? (b) What is the effectiveness of identified digital health interventions on patient outcomes? A population, intervention, comparator, outcomes and study (PICOS) framework was used to structure the review. This included people living with HIV in SSA (population), digital health (intervention/exposure), usual care or no comparator (comparison), physical, psychological, social or spiritual symptoms, a focus on quality of life, patient satisfaction with palliative care services, and other patient outcomes relevant to palliative care (outcomes). This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 27 A full protocol is registered in PROSPERO (reference number: CRD42020182695).
Eligibility
Included studies included PLWH, a digital health intervention (defined broadly as the use of information and communications technology in support of health and health-related fields 28 ) involving palliative care patients and/or providers, reported patient outcomes and were conducted in SSA. Studies with or without comparators were also included, alongside studies where digital health was part of a combined intervention package. Any study design or setting (e.g. community and hospital) was included. Articles published in any language were eligible for inclusion. Studies were excluded if they had patients with diseases other than HIV, no digital health intervention, did not report patient outcomes and were conducted outside SSA. Studies with digital health interventions used in HIV prevention, testing, ART adherence and viral load monitoring were excluded except when the intervention was explicitly used to support palliative care for PLWH. Studies were also excluded if they did not report primary data.
Search of studies
Search strategies (see Supplementary Material 1) were developed with guidance from information specialists at the university of the lead author. Literature searches were conducted in MEDLINE, Embase, PsycINFO and Global Health on 22 May 2020 with no limit on publication date. The search strategies were adapted with relevant Boolean operators and search characters for each database. A combination of search terms for ‘HIV’, ‘Digital Health’ and ‘sub-Saharan Africa’ was used to capture all digital health literature in HIV care for the SSA region. Combinations of MeSH terms and keywords were used to search the databases. EndNote X9 was used to store and manage the references exported from the databases alongside identifying and removing duplicate citations.
Study selection and data collection
Two reviewers (CM and MJA) independently reviewed titles and abstracts against the inclusion and exclusion criteria. Full-text articles were sought for the included studies and their content was assessed against the inclusion and exclusion criteria. Any disagreements between the two reviewers were resolved through discussion. KN reviewed the final list of the selected studies. Figure 1 presents the PRISMA flow diagram 27 for this review. A data extraction form was developed based on the Cochrane Collaboration 29 and converted into an Excel spreadsheet. The spreadsheet was used to extract and store data from the included studies (see Supplementary Material 2). CM extracted the data. The data were checked by MJA and KN. A WHO template for Classification of Digital Health Interventions version 1.0 30 was used to categorise digital health interventions. A Template for Intervention Description and Replication (TIDieR) 31 was used to extract details of each intervention included in the review (see Supplementary Material 3).

PRISMA flow chart for the systematic review.
Risk of bias assessment
The Mixed Methods Appraisal Tool 32 was used to assess the risk of bias for the individual studies (see Supplementary Material 4). CM appraised the studies and MJA reviewed the appraisal. Any discrepancies were resolved through discussion. KN cross-checked the final appraisal.
Statistical analysis
Due to the heterogeneity of the included studies, a descriptive synthesis 33 was used to summarise the included studies. This was followed by a classification of the digital health interventions by the WHO taxonomy 30 and descriptions of the interventions according to the TIDieR checklist. 31 A framework for the development of complex interventions 34 was also used to describe the stages of development of digital health interventions described in included studies.
Results
In total, 4117 records were identified. After de-duplication, 2207 articles remained. The articles were screened and a full-text review carried out for 43 articles. Following full-text review, 25 articles were included in the review. Included studies used quantitative (n = 22) and qualitative (n = 3) study approaches (see Figure 1).
Characteristics of included studies
Studies included a total of 3592 PLWH. Sample sizes of the studies varied from 10 35 to 2458. 36 Included studies were conducted in 21 countries: South Africa (n = 5), Kenya (n = 4), Botswana (n = 3),37–39 Nigeria (n = 3),40–42 Uganda (n = 2),43,44 Gabon (n = 1), 35 Ghana (n = 1), 45 Lesotho (n = 1), 46 Malawi (n = 1), Zimbabwe (n = 1) 47 and multiple countries (n = 3).36,48,49 Studies included three randomised controlled trials (RCTs),41,43,50 three qualitative studies,47,51,52 three pre- and post-test studies,42,44,53 two observational studies,49,54 two case series,35,36 six cross-sectional studies37–39,48,55,56 and six mixed method studies.40,45,46,57–59 Most studies were published in 2019 (n = 6),48,49,53–55,57 followed by 2018 (n = 4),36,40,56,59 2015 (n = 4)41,44,50,51 and 2017 (n = 3).45,46,52 Table 2 summarises the characteristics of the included studies, and Table 3 provides further details of study characteristics. All data extracted from the studies are available in Supplementary Material 2.
Summary of study characteristics.

PLHIV: people living with HIV.
The number of key informants who were also participants in the study is not reported.
Only 22 were PLHIV. The study also had 21 men who have sex with men (MSM) and 14 sex workers.
Excludes 202 treatment supporters.
Excludes 11 medical personnel.
The first study had 60 participants, and 33 participants of the second study were drawn from the first study.
2458 teleconsultations were done, and only 5.5% (N = 134) were for neurological issues, which was the focus of the study.
The study had 615 participants. Only 246 were HIV-infected children.
Detailed characteristics of included studies.

Appraisal of included studies
Using the MMAT tool (see Supplementary Material 4), studies were grouped as qualitative (n = 3),47,51,52 RCTs (n = 3),41,43,50 quantitative non-randomised (n = 8),37,39,42,44,53–56 quantitative descriptive (n = 5)35,36,38,48,49 and mixed methods (n = 6).40,45,46,57–59 Most studies met four to five criteria for their study design. Only three studies36,41,56 met three or fewer criteria.36,41,56
Identification and description of the studies
WHO classification of digital health interventions
There were 13 studies40–48,51, 53, 57, 58 with digital health interventions targeted at clients as primary users and 12 studies35–39,49,50,52,54–56,59 with interventions targeted at healthcare providers as primary users. There were no digital health interventions targeted at health system managers or data services. For digital health interventions targeted at clients, targeted client communication41,42,46,48 and client-to-client communication40,53,57,58 were the most common ways clients accessed palliative care. Using the WHO classification, the digital health interventions used to provide palliative care to PLWH in SSA were categorised into 9 categories: targeted client communication,41,42,46,48 client to client communication,40,53,57,58 personal health tracking,43,44,47 citizen-based reporting, 45 on-demand information services to clients, 51 health care provider decision support,50,56,59 telemedicine,35–39,49,54 referral coordination, and laboratory and diagnostics imaging management. 55 Across all approaches, telemedicine was the most commonly reported in the included studies35–39,49,54 (see Table 4).
WHO classification and summarised TiDieR descriptions of digital health interventions used to deliver palliative care to PLWH in SSA.

Description of digital health interventions aligned with the TIDieR checklist
Summarised TIDieR descriptions of the digital health interventions are provided alongside alignment with WHO classification in Table 4. Detailed descriptions are provided in Supplementary Material 3.
Stage of digital health intervention development
There were four studies44,48,51,52 at the development stage. The second largest number of studies (n = 10)35,36,38,40,44,46,47,51,58,59 were at the feasibility and piloting stage. The largest number of studies (n = 12)37,39,41–43,49,50,53–57 were at the evaluation stage. Only one study 45 reported research at the implementation stage (see Figure 2).

Stages of digital health interventions.
Reported efficacy and effectiveness of digital health interventions
Both efficacy and effectiveness of digital health interventions are reported in 13 of the 25 included studies.37,39,41–44,49,50,53–57
A full RCT 41 assessed the efficacy and a pre-post-test study 42 assessed the effectiveness of targeted client communication: (a) delivery of acceptance and commitment therapy through SMS was efficacious in improving psychological flexibility of pregnant HIV-positive women, 41 and (b) mobile phone counselling was also effective in improving psychological outcomes of undisclosed HIV positive youth. 42
A mixed methods and pre-post-test study evaluated the effectiveness of client-to-client communication53,57: (a) providing psychosocial support to HIV-positive youth through mobile phones was effective in getting them to commence ART and complete viral load tests, 57 and (b) peer psychosocial support through a social media platform was effective in improving adherence intentions for HIV positive youth. 53
A pilot RCT 43 assessed the efficacy and a pre-post-test study 44 assessed the effectiveness of personal health tracking interventions.43,44 Computer rehabilitation therapy was efficacious in improving the neurocognitive skills of HIV-positive children. 43 Computer rehabilitation therapy was also effective in improving neurocognitive skills of HIV-positive children. 44
The effectiveness of healthcare provider decision support interventions was assessed in a cross-sectional study, 56 and the efficacy of healthcare decision support interventions was also assessed in a pilot RCT 50 : (a) a mobile phone application was effective in diagnosing neurocognitive impairment in HIV-positive patients, 56 and (b) HIV counselling through a digital platform was efficacious in improving psychosocial outcomes of HIV positive adults. 50
Two cross-sectional studies37,39 and two observational studies49,54 assessed the effectiveness of telemedicine interventions: (a) teledermatology was not effective in diagnosing and recommending treatment for skin conditions of PLWH, 37 (b) remote diagnosis of cervical cancer in HIV-positive women was effective, 39 (c) teleultrasonography was effective in supervising medical personnel that diagnosed HIV associated tuberculosis 54 and (d) a remote quality assurance centre was effective in helping neurodevelopment evaluators maintain the quality of their testing. 49
A prospective cross-sectional study assessed the effectiveness of a laboratory and diagnostics imaging management intervention. 55 A portable electrocardiogram (ECG) device was effective in generating readable ECGs in patients with the World Health Organisation AIDS Clinical Staging (WACS) of 1 only. 55 Table 5 details included studies outlining the efficacy and effectiveness of digital health interventions for provision of palliative care in PLWH in SSA.
Efficacy and effectiveness of digital health interventions for provision of palliative care in PLWH in SSA.

Discussion
There is an emerging evidence base of good quality research to inform digital health interventions for the provision of palliative care to PLWH in SSA. In SSA, digital health has been used to provide palliative care to PLWH through targeted client communication, client-to-client communication, personal health tracking, citizen-based reporting, on-demand information services to clients, healthcare provider decision support, telemedicine, referral coordination and laboratory and diagnostics imaging management. Most interventions were at the stages of feasibility, piloting and evaluation. Of the included studies, efficacy was reported across three studies and effectiveness across 10 studies for digital health interventions seeking to improve intended outcomes. Whilst previous research has focused on SMS interventions, 60 there are now multiple, broader digital health approaches being developed and tested to support patients with HIV and palliative care needs. However, further evidence is needed to understand how the effectiveness of interventions is realised and how they can best be integrated into the routine delivery of palliative care services.
Telemedicine was the most researched digital health intervention for palliative care in PLWH. A human resource gap in SSA, particularly at the primary care level, has been highlighted 61 with telemedicine posing a potential approach to addressing the shortage of expertise. However, the use of telemedicine was limited to provider-to-provider communication in a clinical setting making it mostly applicable to the district hospital and specialist palliative care models. In SSA, there is scope to explore telemedicine in the provision of palliative care for PLWH by extending its use to facilitate provider-client communication. In developed countries, telemedicine has been used to remotely manage pain and other symptoms, expanding the reach of palliative care services. 62 It has also been used to coordinate patient care, minimising utilisation of outpatient services 63 while improving the provider–client relationship. 64 Such an approach, encouraging telehealth programs to enable, for example, families to virtually visit and partake in health decisions with loved ones, has been a recommendation of the World Health and Palliative Care Alliance in response to the COVID-19 pandemic. 65 Critical to expansion to approaches is the need to accommodate low digital health literacy for both providers and patients, alongside other known barriers including the cost of delivering telemedicine and telecommunication and infrastructure challenges (e.g. intermittent electrical supply, limited mobile phone network coverage), especially in rural areas. 66 Additional, research is needed in SSA to determine the cost, available infrastructure for digital health, and acceptability of telemedicine among patients and providers.
The second most researched digital health interventions for palliative care were targeted client communication and client-to-client communication. The underlying theme across both categories was the use of digital health to provide psychosocial support to PLWH, with a great need for psychosocial support reported previously among PLWH. 67 Studies conducted in several SSA countries found the prevalence of mental illness among PLWH to be 19% or higher. 68 This review found that the use of digital health psychosocial interventions among PLWH occurred in both community and clinical settings, suggesting their potential appropriateness across different models of palliative care in SSA (i.e. community, district and specialist). 69 Digital health interventions that provide counselling and peer support may be an approach to supporting psychosocial symptoms among PLWH in SSA, with a number of the interventions having demonstrated acceptability and effectiveness in assessing, monitoring and treating severe mental illnesses in LMICs. 70
The literature on the use of digital health to support palliative care in SSA is at an early stage and there remains a need to understand the needs and preferences of PLWH and the services delivering palliative care to inform the requirements of digital health interventions. A review 71 of successful approaches for scaling up digital health interventions in LMICs found that interventions that align with need are more likely to be adopted and engaging for end-users. In addition, understanding user needs helps reduce health inequalities by ensuring the engagement of vulnerable groups from the outset. 72 Alongside determining user needs, future research exploring digital health for PLWH in SSA needs to explore the mechanisms that underpin and mediate any changes to outcomes arising from interventions. Exploring such mechanisms in well-established digital health approaches (e.g. telemedicine) may offer intervention agnostic insights that could inform the development of less common approaches that have value for PLWH in SSA. Such findings may also have relevance beyond the SSA region as the lack of an evidence base and end-user involvement in digital health interventions for PLWH is an issue across many LMICs. 73 Within this review, only one study 41 developed a digital health intervention underpinned by an existing theory. Exploring opportunities for applying and developing underlying theories that can inform digital health intervention development is a crucial next step in developing the research field. 74 Furthermore, exploring cost-effectiveness evaluation of digital health interventions that have demonstrated effectiveness in improving patient outcomes is necessary to facilitate scale-up and wider adoption, with cost a central consideration for government decision-making around intervention adoption. 75
Strengths and limitations
To our knowledge, this is the first systematic review to explore the role of digital health in palliative care for PLWH in SSA. This review utilised robust search strategies with broad inclusion criteria, including any study design. This review is, however, limited by the fact that no searches were undertaken in grey literature databases and that hand-searching was not done due to time limitations. As a result, while we are confident of the inclusion of a wide body of literature, it may not reflect the entirety of relevant research literature.
Conclusion
Research into the use of digital health interventions to support palliative care for people living with HIV in SSA is developing. However, there is a lack of a theoretical underpinning to many interventions, the mechanisms through which interventions lead to change in patient outcomes are not clear, and most reported interventions have not progressed to a stage of implementation as part of routine care. Future research should focus on embedding theory into intervention development for PLWH, exploring the potential of additional digital health interventions beyond primarily telemedicine approaches, and aligning intervention development with the wider regional need for the expansion of palliative care provision.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076221133707 - Supplemental material for The role of digital health in palliative care for people living with HIV in sub-Saharan Africa: A systematic review
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076221133707 for The role of digital health in palliative care for people living with HIV in sub-Saharan Africa: A systematic review by Christopher Mwase, Kennedy Nkhoma and Mathew J Allsop in Digital Health
Supplemental Material
sj-docx-2-dhj-10.1177_20552076221133707 - Supplemental material for The role of digital health in palliative care for people living with HIV in sub-Saharan Africa: A systematic review
Supplemental material, sj-docx-2-dhj-10.1177_20552076221133707 for The role of digital health in palliative care for people living with HIV in sub-Saharan Africa: A systematic review by Christopher Mwase, Kennedy Nkhoma and Mathew J Allsop in Digital Health
Footnotes
Acknowledgements
CM would like to acknowledge Chevening Scholarships, the UK government's global scholarship programme, funded by the Foreign, Commonwealth and Development Office (FCDO) and partner organisations for making it possible for him to study in the UK.
Author contributions
CM and MJA conceived the review, completed data searches, extraction and initial synthesis of findings. KN supported planning, analysis and interpretation. All authors contributed to the writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not required because this study retrieved and synthesised data from already published studies.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Guarantor
MJA.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.