
Abstract
Globally, inadequate healthcare provider (HCP) proficiency with evidence-based guidelines contributes to millions of newborn, infant, and child deaths each year. HCP guideline proficiency would improve patient outcomes. Conventional (in person) HCP in-service education is limited in 4 ways: reach, scalability, adaptability, and the ability to contextualize. Adaptive e-learning environments (AEE), a subdomain of e-learning, incorporate artificial intelligence technology to create a unique cognitive model of each HCP to improve education effectiveness. AEEs that use existing internet access and personal mobile devices may overcome limits of conventional education. This paper provides an overview of the development of our AEE HCP in-service education, Pediatric Acute Care Education (PACE). PACE uses an innovative approach to address HCPs’ proficiency in evidence-based guidelines for care of newborns, infants, and children. PACE is novel in 2 ways: 1) its patient-centric approach using clinical audit data or frontline provider input to determine content and 2) its ability to incorporate refresher learning over time to solidify knowledge gains. We describe PACE's integration into the Pediatric Association of Tanzania's (PAT) Clinical Learning Network (CLN), a multifaceted intervention to improve facility-based care along a single referral chain. Using principles of co-design, stakeholder meetings modified PACE's characteristics and optimized integration with CLN. We plan to use three-phase, mixed-methods, implementation process. Phase I will examine the feasibility of PACE and refine its components and protocol. Lessons gained from this initial phase will guide the design of Phase II proof of concept studies which will generate insights into the appropriate empirical framework for (Phase III) implementation at scale to examine effectiveness.
(1) (a) Conventional education has limited reach to rural HCPs. Pediatric acute care conventional education programs in Mwanza, Tanzania, Helping Children Survive and Essential Child Health Services, have had limited reach to rural HCPs. Our 184-provider survey across PAT's sites demonstrated that newborn or pediatric in-service provider education reaches only 60–70% of providers, with disproportionately less at community health center compared to zonal/regional hospital providers. This is consistent with our previous work in Botswana, where only 11% of community clinic HCPs and 0–29% of district hospital HCPs had ever received pediatric acute care conventional in-service education compared with 74% prevalence of referral hospital HCPs,12–14 as well as other HCP conventional education programs in sub-Saharan Africa.15–17 Possible reasons include 1) limited time for HCPs to attend education due to clinical demands 2) limited financial support to travel to centralized education events and 3) limited instructor, equipment, and space availability to train on site. Costs to deliver conventional education limit scalability. High HCP turnover seen in many LMIC health systems requires a scalable solution to be effective.
18
Costs of delivering pediatric acute care conventional education range from $31 to $90 per HCP per day.19–21 As an example, high HCP turnover limits the effectiveness of the Emergency Triage Assessment and Treatment - Plus (ETAT + ), a 5-day conventional education adaptation of the WHO hospital-based pediatric emergency care course in Kenya.
22
Conventional education does not adapt to the learner. In Tanzania, there are many different cadres (professional types), with wide range of pre-service education, that provide clinical care to newborns and children. These include specialists and medical officers (5 years of education + 1 year of internship); advanced degree nursing (i.e., nurse midwife, 3 years + 1 year internship); nursing officers and clinical officers (3 years), assistant clinical officers, assistant medical officers (2 years), as well as assistant nursing officers, and medical attendants with only weeks or months of pre-clinical education. The bulk of the care is provided by junior medical officers/nurses, who have limited training and experience caring for children with severe illness. In attempting to have a “one size fits all,” programs often have fixed duration and cannot adapt to HCPs’ knowledge gaps and clinical needs, resulting in a “one size fits none.”23,24 This may lead to either decreased effectiveness for HCPs with existing proficiencies or inadequate effectiveness for those with greatest need.13,14,25 Additionally, without educational refreshers, proficiency decreases over time.13,26 Conventional education does not contextualize to the health system. Contextualization of HCP education is required to ensure it engages the learner and can impact care delivery. Facilities that provide acute care for newborns and children in Tanzania range from least resourced outpatient dispensaries, health centers, and district hospitals to greater resourced referral hospitals and zonal/national hospitals. Unfortunately, contextualization of conventional education is often “on the fly” i.e., during delivery, placing the burden of contextualization is on individual instructors or HCPs and often influenced by resource availability, which leads to incomplete and inappropriate education.
23
Conventional education is not responsive to changes in local epidemiology or care quality issues and requires years or decades for publication cycles to update.23,27,28 Finally, current conventional education is not responsive to system shocks, such as emerging epidemics, or natural disasters.28,29
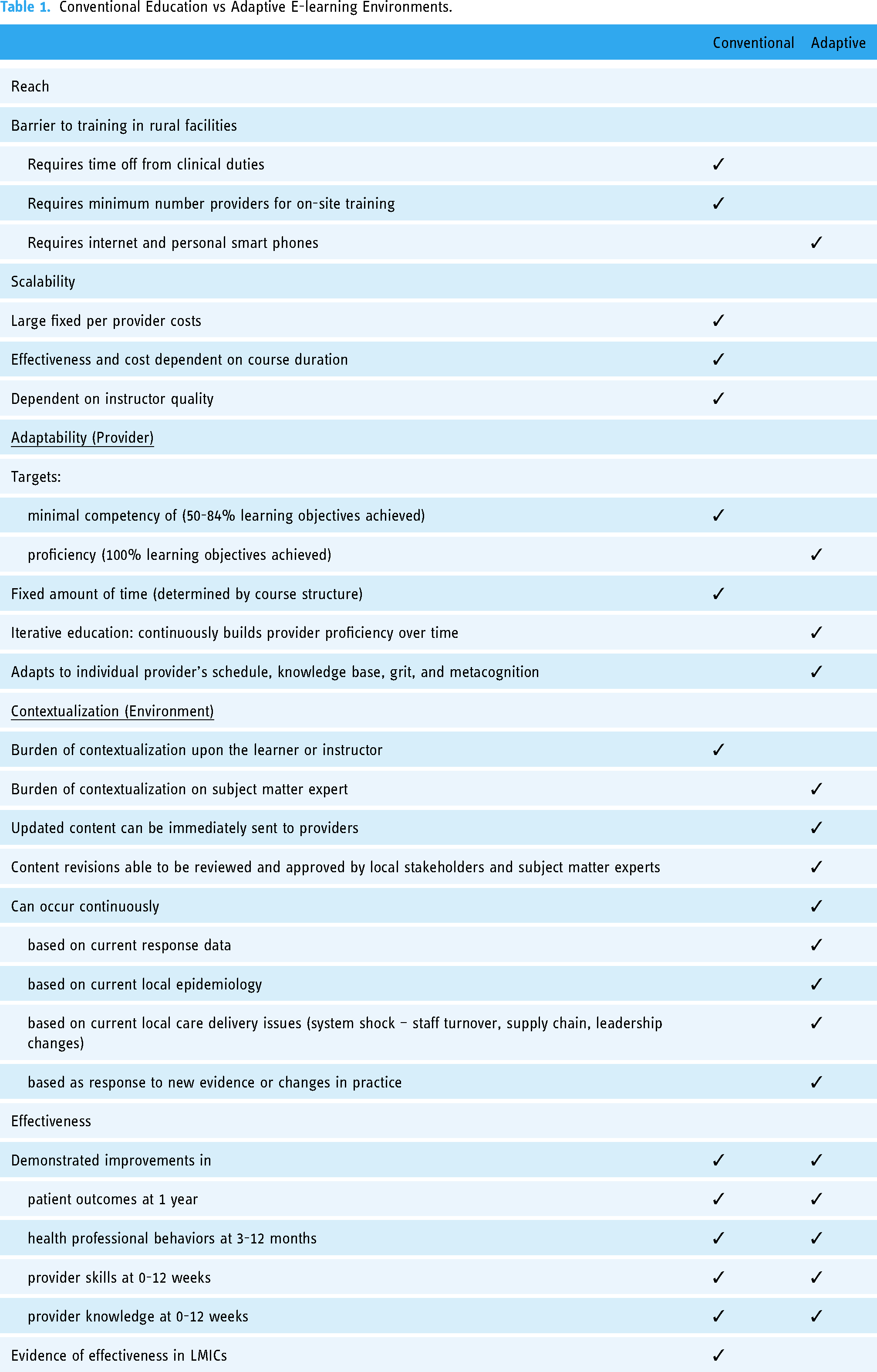
Conventional Education vs Adaptive E-learning Environments.
These limitations may explain why conventional education is not more effective at increasing provider proficiency. The median effect size of conventional education alone is only 7.3% (IQR: 3.6–17.4). Even under ideal conditions, combined with longitudinal self-study education or peer-to-peer education, the improvement in provider clinical care only improves by 24% and 25%, respectively.20,26 These effect sizes remain modest in absolute terms given the low baseline clinical performance of 40%–60%.5,20,25,30
(b) (c) Potential to Increase Reach. AEEs may reach HCPs where equipment requirements and other impediments exist for conventional education.34–36 Eighty-five percent of Tanzania's population is covered with at least a 3G network and 14% of the population has active mobile broadband subscribers.
37
In our initial feasibility studies, all 21 medical and clinical officer interns had smartphones with data plans, and 19 reported a preference to use their mobile phones for e-learning over tablets or computers.38,39 Course delivery of AEEs encourages scalability. While course development costs are fixed, course delivery costs are minimal compared to conventional education. AEEs can be time-independent, allowing HCPs the needed educational exposure to achieve proficiency. E-learning does not require significant time off from clinical duties or travel, nor the need for minimum participants for classes. Further, web-based course delivery eliminates instructor quality variability. AEEs adapt to the learner. AEEs are iterative; they assess not only the HCP's correct responses but also their awareness of being correct/incorrect (metacognition), and ability to work through challenging topics (grit). Such software can determine optimal pacing and sequence of content continuously, building HCP proficiency and confidence over time. Moreover, AEEs analyze HCPs’ performance and knowledge gaps to serve up brief refresh packages repeated over time to maintain HCP proficiency. This calculation is individualized, and as HCPs use the technology regularly (e.g., monthly, quarterly), it becomes increasingly precise in determining what material to reinforce and when to support it. Contextualization is done during course design by content and context experts. Updated content can be released immediately to HCPs, and aggregate response data can be used to refine program content based upon HCP proficiencies and gaps. This creates the potential of a responsive HCP education that can both identify and address proficiency gaps at a local or individual level in near real-time, while maintaining the ability to disseminate new or revised evidence-based guidelines at scale. (2) (a) Broadened pediatric acute care content. Our original content scope was restricted to our Helping Children Survive conventional in-service education learning objectives (severe pneumonia, airway, oxygen therapy, severe dehydration/shock, triage/systematic assessment). PAT and Ministry of Health feedback led to expansion to 283 learning objectives over nine assignments and includes essential newborn care, sick newborn care, severe malaria, severe anemia, and severe malnutrition. Use PAT as subject matter experts for content development and Tanzanian national treatment guidelines as primary source materials. National guidelines represent the product of a contextualization of international guidelines by local subject matter experts. In Tanzania, the PAT represents the subject matter experts of Newborn and Pediatric Acute Care. Use of non-contextualized materials has been identified as a barrier to effective HCP education.
23
By incorporating PAT supervision into content development, discrepancies were discovered prior to and reviewed to ensure local contextualization was accurate and appropriate. This alignment of content development with existing expertise infrastructure proved critical for adoption and ownership. Award continuing professional development (CPD) credit. The Medical Council of Tanganyika (MCT) is the national regulating body for medical, dental, or allied health professionals in Tanzania. Awarding CPD credit utilizes existing infrastructure to maintain provider's registration while fulfilling MCT's mission to “to improve performance, develop, maintain and update knowledge, skills and attitudes in order to provide safe, ethical, legal and effective care to patients, clients and community.”
40
(b) (c) (d) (e) (f) (g)

Adaptive e-learning environments.
PACE content.

Our PACE learning engineers are responsible for course content development. Learning engineers develop content with input from PAT subject matter experts and Area9 Lyceum education design team to ensure contextualized, high-quality content. Learning engineers are based in Tanzania and complete training in the concepts of adaptive learning and authoring in Rhapsode™ through self-directed learning modules and development of an adaptive e-learning module with remote supervision by Area9 Lyceum education design team.
All PACE program personnel require a medical (MD) or nursing (RN) degree and experience working in the Tanzanian health system. In addition, effective communication skills and, either formal or informal health education and/or IT skills, are required.
(h) (i) (j) (k) (3) (4) (a) Internet connectivity and mobile phone access - The utilization of computers as an educational supplement, particularly self-study in-service education using computers, is recognized as a significant research gap in provider education in low- and middle-income countries due to the increasing accessibility of personal computers and internet-based education programs.
26
Although 85% of Tanzania has at least 3G, and all our HCP pilot subjects own smartphones, the effect of geographical (rural) or functional (cost and accessibility) barriers on web-based education remains uncertain. As the growth of internet is exponential, this barrier is not expected to exist in the future.48,49 If these issues prove to be significant, alternatives may include creation of a phone application to alleviate the need for continuous connectivity. Providing supplemental data plans to reduce the costs of internet access as a barrier is another alternative.
50
(b) Learners’ privacy is protected as Rhapsode™ is GDPR compliant including in encryption, data security, and permanent data deletion, nevertheless, there is always the potential for data privacy breach. (c) Inadequate in-person support: COVID-19 prevented the project team from providing direct project support to HCPs from February 2020 to October 2021. Attempts to enroll participants remotely were moderately successful with screening, but implementation and maintenance of PACE were poor.38,39 Our current configuration attempts to minimize administrative infrastructure, but the optimal HCP cohort size per PACE coordinator is unknown. (d) Currently, the capacity of our PACE content development team is inadequate for utilizing it as a means of ongoing quality improvement. We anticipate this will become feasible with further experience and revisions to our workflow. (e) Lack of integration with skills training. Currently, PACE does not integrate hands-on practical skill training such as airway or fluid resuscitation management. Rhapsode™ Activity can incorporate skills assessments using either direct observation, and video review by an educator or self-review. These skills will continue to be delivered through conventional in-person education. Integration of blended learning may further increase its impact through use of mentor outreach and local facilitation through PACE personnel, CLN mentors, or peers. (f) Lack of integration with provider performance. CLN's initial detailed clinical audit forms were piloted and adopted at the zonal hospital in 2019 and intended to be used for PACE provider proficiency as well as patient outcomes. CLN's clinical audit was discontinued in 2020 and never implemented at other CLN sites in part due to the national transition to an electronic medical record (EMR) which included the elimination of paper forms. The assumption that this data would be found in the EMR has not yet been realized. Currently, Mwanza's EMRs lack the structured format of the standardized pediatric admission forms to ensure pediatric-specific documentation on admission and during hospitalization is completed. Additionally, we are unable to obtain any degree of standardized output from the EMR CLN's existing limited clinical auditing prevents associating an HCP's PACE proficiency with their clinical proficiency. This limits optimal contextualization as well as adaptivity.

Clinical Learning Network.
Discussion
In highly resourced settings, e-learning has been shown to be as good as conventional education. Non-adaptive eLearning programs have improved patient outcomes when compared to no intervention and are at least as effective as conventional education.33,51–53 Adaptive e-learning, which builds on this by using response data to create models of individual learner pathways and adjusts sequencing and learning resources to optimize effectiveness, has shown moderate to large positive effects on both knowledge (SMD 0.70; 95% CI−0.08- + 1.149, Z = 1.76, p = 0.08) and skills outcomes (SMD 1.19, 95% CI 0.59–1.79, z = 3.88 p < 0.001) when compared to other educational methods. 32 Similar results have been seen in provider trainee 32 and non-provider populations.54–57 Interestingly, using blended education that includes adaptive and face-to-face education in non-provider populations, achieves similar outcomes but 25% faster than adaptive approaches alone. 58
In low- and middle-income countries (LMICs), where HCP in-service education resources are limited, adaptive e-learning may overcome this limitation, but studies are needed. The WHO Digital Guideline Group's priority research raised the following question “For professional health workers, does adaptive eLearning, compared to conventional education alone, improve [outcomes].” 8 Tuti et al. conducted a multi-center, multi-LMICs, RCT examining “adaptive immediate feedback” vs standard immediate feedback across HCPs who provide clinical care to newborns and showed no significant difference. The adaptivity was significantly limited by its logic model (Bayesian vs more complex logic models incorporating metacognition and response time), functionality (used to determine level of detail of feedback vs. adjusting course content and sequencing), and granularity (feedback of an entire module/scenario vs individual objectives). 59 Notably, Tuti had completion rates of 43%, higher than completion rates of massive open online courses (MOOC) of 7%–15%.60,61
To determine if adaptive e-learning is effective in improving care quality, its implementation strategy needs to be defined and refined. It is crucial to determine which aspects of the implementation strategy are acceptable to stakeholders and which need to be revised to normalize adaptive e-learning by HCPs. Aspects of the intervention design that were acceptable to the stakeholders included the use of principles of co-design, plan to integrate with CLN's clinical auditing and multilevel stakeholder engagement, its simple and easy user interface, and content sizing. The value of co-design principles and multilevel stakeholder engagement have been identified in previous interventional development studies,62,63 including the Clinical Learning Network. Use of CLN's infrastructure to develop and explicitly describe health system leaders’ and HCPs’ defined roles during the Phase I studies of PACE, obviated the need for an additional external leadership infrastructure, while simultaneously providing actionable work within CLN aligned with its overall goals. PACE modules capitalized on an easy-to-use interface using established Mayer's e-learning principles, right sizing of content, Bloom's Taxonomy, and established local guidelines. These factors combined with minimal infrastructure and disturbance of clinical care, were key acceptability drivers for us and seen previously.63,64 It is important that e-health interventions have a positive impact on clinical management to be successful, 65 and aligns with our use of clinical auditing as long-term measurement goal. Knowledge assessments should be used as an intermediate marker of PACE efficacy when linked to provider proficiency and patient outcomes. By utilizing existing quality improvement metrics as indicators of education effectiveness, the requirement for test development, implementation, and monitoring is eliminated, reducing the need for additional data collection and management.
We used principles of co-design and feedback from stakeholders over time to refine our empiric implementation strategy. Aspects of the intervention design that needed revision prior to pilot testing included our content development workflow, local capacity to develop content, and our support for e-learning. Our initial content development workflow was led and developed externally and was presented for CLN approval. Through serial stakeholder meetings, feedback, and collaboration with PAT, CUHAS and governmental leadership, PACE program transitioned to a facilitator of CLN priorities, supervised by local subject matter experts. This expansion of PACE allowed it to better address local priorities, leading to an increase in stakeholder participation in content development. Approval was also shifted to subject matter experts within PAT. This greater involvement throughout all stages of development led to fewer revisions as content was approved during its creation.
A major component of PACE implementation strategy is local capacity to develop education content. Local capacity is a known bottleneck to e-learning.71 Local educational design and implementation capacity is an intrinsic component of PACE which allows for optimal contextualization. We initially underestimated the amount of effort and supervision required. Our approach was altered to have PAT assume the responsibility of recruiting, supporting, and supervising learning engineers. Currently, our approach involves utilizing four senior PAT members who volunteer as learning engineers. More work is needed to determine the optimal local capacity framework for learning engineering.
Finally, we identified that in-person support to providers is needed and the predominant communication with our stakeholders is text messaging, not e-mail. Our initial support for HCP was remote and largely email-based. Through early piloting, we identified that remote orientation to PACE was insufficient, and most communication is done via WhatsApp. Consequently, the position of PACE coordinator was established to provide on-site orientation to PACE and follow-up. Additionally, a unique integration between WhatsApp and our REDCap database was developed to monitor provider follow-up.
Implications for future research and sustainability
Adaptive E-learning Environment Enhanced Learning Health Systems hold tremendous promise to address the HCP education gaps that currently limit the provision of high-quality care in LMICs. The potential of AEEs to scale up, increase reach, and adapt to systems may drive this paradigm shift. We are currently in phase I (define and refine) are using a mixed methods approach to determine feasibility and normalization of our current methods. Once refined, Phase II (proof-of-concept) will allow us to determine if there is a clinically significant signal seen through a clinical audit. Phase III and IV studies (efficacy and effectiveness) will enable us to determine if provider education improves care, patient outcomes, and cost-effectiveness. Future studies will clarify important characteristics of education content, the education environment, work environment, and provider characteristics. This will allow optimization of efficiency and effectiveness of in-service provider education for all types of providers in all types of settings.
PACE's current sustainability is dependent on both support for operation and development, as well as research. Long-term funding sources may be influenced by its utility to the HCPs and the health systems it serves. PAT has incorporated PACE permanently into its national Continuing Professional Development offerings. HCPs may provide support for PACE if it proves a reliable mechanism for continuing professional development. Finally, health systems may employ the integrated PACE CLN model to demonstrate commitment to quality and maintain accreditation.
Conclusion
HCP proficiency is critical to improving patient outcomes, and adaptive e-learning environment may overcome intrinsic barriers to conventional education in low- and middle-income countries. We used principles of codesign to develop PACE to improve provider proficiency in newborn, infant, and pediatric care in Mwanza Tanzania. PACE currently includes 283 learning objectives over 9 assignments. Future research and training include the completion of a phase Ib study to refine PACE for strength and efficiency. We will capitalize on our flexible and progressive development framework to develop an adaptive e-learning in-service provider education implementation strategy that improves provider proficiency, patient care quality, and ultimately newborn and child survival.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180471 - Supplemental material for Development of pediatric acute care education (PACE): An adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180471 for Development of pediatric acute care education (PACE): An adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania by Peter Andrew Meaney, Adolfine Hokororo, Theopista Masenge, Joseph Mwanga, Florence Salvatory Kalabamu, Marc Berg, Boris Rozenfeld, Zachary Smith, Neema Chami, Namala Mkopi, Castory Mwanga and Ambrose Agweyu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231180471 - Supplemental material for Development of pediatric acute care education (PACE): An adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania
Supplemental material, sj-docx-2-dhj-10.1177_20552076231180471 for Development of pediatric acute care education (PACE): An adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania by Peter Andrew Meaney, Adolfine Hokororo, Theopista Masenge, Joseph Mwanga, Florence Salvatory Kalabamu, Marc Berg, Boris Rozenfeld, Zachary Smith, Neema Chami, Namala Mkopi, Castory Mwanga and Ambrose Agweyu in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231180471 - Supplemental material for Development of pediatric acute care education (PACE): An adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania
Supplemental material, sj-docx-3-dhj-10.1177_20552076231180471 for Development of pediatric acute care education (PACE): An adaptive electronic learning (e-learning) environment for healthcare providers in Tanzania by Peter Andrew Meaney, Adolfine Hokororo, Theopista Masenge, Joseph Mwanga, Florence Salvatory Kalabamu, Marc Berg, Boris Rozenfeld, Zachary Smith, Neema Chami, Namala Mkopi, Castory Mwanga and Ambrose Agweyu in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the Pediatric Association of Tanzania; the Tanzanian Ministry Of Health, Community Development, Gender, Elderly and Children, Regional and Council Health Management Teams for participating in stakeholder meetings, Géraldine Jossellin-Duval for her leadership and mentorship of the PACE Learning Engineering Team; Enock Diocles, Hanston Ndosi, Denis Albert and Agnes Hassan for their organizing of participants and site work in Mwanza; Christine Joyce, Michael Alfonzo, Jose “Jojo” Ferrer, Segolame Setlhare, CLN mentors and facilitators for their valuable feedback on the initial versions of PACE and its refinements.
Contributorship
PAM, ZHS, AH, JRM, TM, and AA researched literature and conceived the study. PAM, ZHS, AH, JRM, TM, and AA were involved in protocol development, gaining ethical approval. All authors were involved in recruitment and data analysis. PAM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
BR and MB are compensated by Area 9 Lyceum as Senior Learning Architect and Medical Director, respectively.
Ethical approval
The ethics committee of Stanford University and Tanzania's National Institute of Medical Research approved this study (REC number: #60379, NIMR/HQ/R.8a/Vol.IX/3990, respectively). All participants provided written informed consent prior to enrolment in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Laerdal Foundation for Acute Medicine [grant number NA], and Maternal Child Health Research Institute at Stanford University [grant number NA].
Guarantor
PAM.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.