
Abstract
Introduction
Multidisciplinary tumor conferences are a fundamental component in the treatment of oncological patients. The COVID-19 pandemic and its resulting social distancing restrictions offered the opportunity to compare in-person to virtual multidisciplinary tumor conferences.
Methods
Retrospective analysis of first-time presentations in tumor conferences at a university musculoskeletal tumor center in the time periods from September 2019 to February 2020 (in-person) and May 2020 to October 2020 (virtual).
Results
A total of 209 patients were first-time discussed in one of 52 analyzed musculoskeletal multidisciplinary tumor conferences (105 patients in 25 in-person, and 104 patients 27 virtual meetings). The total number of participants was slightly lower with virtual meetings (p < .001) and more disciplines were represented in virtual tumor conferences (p < .001). With median six consultants present in either, the level of available expertise did not differ between the conference formats (p = .606). Compared to in-person tumor meetings, the patients were discussed earlier in the virtual conferences (p = .028). The interval between first presentation to biopsy was significantly shorter after virtual tumor conferences (median 4 vs. 7 days, p < .001). There was no significant difference in the interval between initial presentation and resection (p = .544) among the two conference formats.
Conclusions
The implementation of virtual tumor conferences appears to have had a positive effect on timely diagnosis and multidisciplinarity during tumor conferences. This may result in better decision-making and treatment of patients with musculoskeletal tumors and could be routinely implemented into cancer care.
Introduction
Primary tumors of the connective tissue and musculoskeletal system can be associated with aggressive local destruction of tissue and unfavorable survival.1,2 As there exists a multitude of different histological sub-types and as these usually represent very rare entities, their management requires a high degree of expertise in the diagnostic workup and treatment. Multidisciplinary tumor conferences (MTCs) have proven to be a beneficial component in the treatment of tumor patients.3–6 This accounts in particular for the rare primary tumors of the musculoskeletal system. 7
MTCs create a setting in which doctors and others involved in the care of tumor patients can discuss the best diagnostic and therapeutic options and develop an individual plan for each patient.8,9 MTCs bring together specialists from a variety of disciplines, such as oncology, surgery, radiology, pathology, radiation therapy, and nuclear medicine3,10–12 with up to 20 and more participants.
In view of the outbreak of the COVID-19 pandemic, in-person tumor conferences had to be reconsidered. As did several other institutions, our university hospital has implemented virtual MTCs.13–17 In these virtual MTCs, specialists can communicate and share images by means of online-conferences and discuss patients as in a normal in-person MTC. 18
This allows the avoidance of direct contact in the sense of the necessary hygiene requirements in view of a pandemic and at the same time enables the conference participants to stay at different locations - including outside the hospital. 18 Prior to the COVID-19 pandemic, virtual MTCs were not routine. Therefore, not much is known about the quality compared to in-person MTCs.
Hence, this study aimed to compare in-person musculoskeletal MTCs to virtual ones regarding patient and participant number, multidisciplinarity, level of expertise, and individual patient flow. This knowledge is relevant for the decision whether to return to in-person MTCs, to continue with virtual MTCs or to redesign the conferences.
Methods
A monocentric retrospective study was conducted at a certified university musculoskeletal tumor center through review of charts. This study was approved by the local institutional ethics committee (Ethikkommission der Medizinischen Fakultät an der Universität Leipzig, reference 537/20-ek). During the COVID-19 pandemic, the authors’ institution switched from in-person tumor conferences to virtual conferences via video calls (Skype Business, Skype Technologies S.A.R.L, Luxembourg City, Luxembourg). The equipment for virtual conferences was first provided in March 2020 but it took until end of April 2020 before the conferences could be held without relevant technical problems.
Inclusion criteria comprised age ≥ 18 years with a suspected malignant tumor and first discussion in either the period from September 2019 to February 2020 (in-person) or the period from May 2020 to October 2020 (virtual). The period from September 2019 to February 2020 for the control group was chosen as this were the 6 months just before the pandemic had arrived in our hospital in order to avoid biases secondary to new medical staff, changed guidelines and structural changes within the hospital not related to the pandemic.
Further criteria were no discussion within the last 5 years in our institution's multidisciplinary musculoskeletal tumor conference and consent to use of medical data for research purposes. We excluded patients with: metastases within 5 years of first tumor diagnosis or who had been discussed before and who were just listed for follow-up (N = 52), patients with a local recurrence or with a known histological diagnosis prior to the conference (N = 127), patients with a suspected benignant tumor and without a biopsy (N = 111). Other exclusion criteria comprised lack of outpatient appointment at our institution prior to the conference (N = 17), non-consent to use of medical data and other reasons (N = 2).
In order to assess the different MTCs composition and level of expertise, the number of participants, the presence of different disciplines and the number of consultants in each tumor conference during discussion of the cases were recorded.
To evaluate how the different tumor conference modalities influenced the individual patient flow, time intervals between first presentation at our institution and first tumor conference discussion, first biopsy, and tumor resection were analyzed and calculated by retrospective chart review.
Statistical analysis
All data were recorded in an Excel database (Microsoft Corp., Washington, DC, USA) and exported to SPSS 21.0 (SPSS Inc., Chicago, IL, USA) for statistical analysis. Data are reported as medians with the minimum and maximum value (range). Non-parametric tests were used to compare differences of medians across and between the two groups. The level of significance was defined as p < .05.
Results
A total of 209 patients were discussed for the first time in one of 52 musculoskeletal tumor conferences (105 patients in 25 in-person MTCs, and 104 patients in 27 virtual MTCs) (Table 1). Based on the initial imaging, 34 of the lesions were classified as benign (16.3%) and 175 lesions as potentially malignant and a biopsy was performed (83.7%, Figure 1). In patients where a malignant tumor was histologically confirmed, a tumor conference had been performed median 1 day (range, 0–19) after first presentation and a biopsy median 7 days (range, 1–22) after first presentation (Table 2).
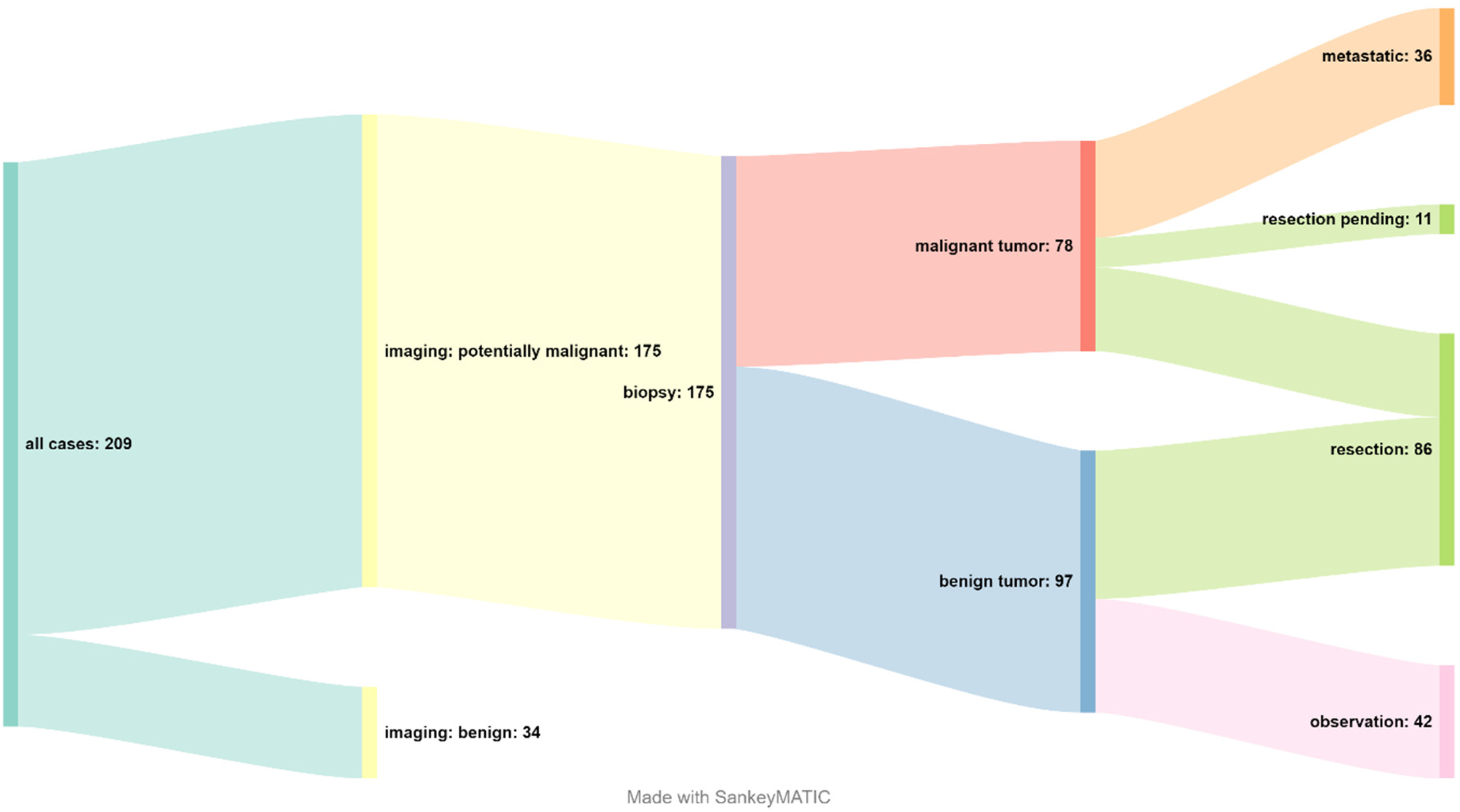
Patient flow Sankey diagram.
Presence of different disciplines, participants, and consultants in the tumor conference during discussion of the cases.
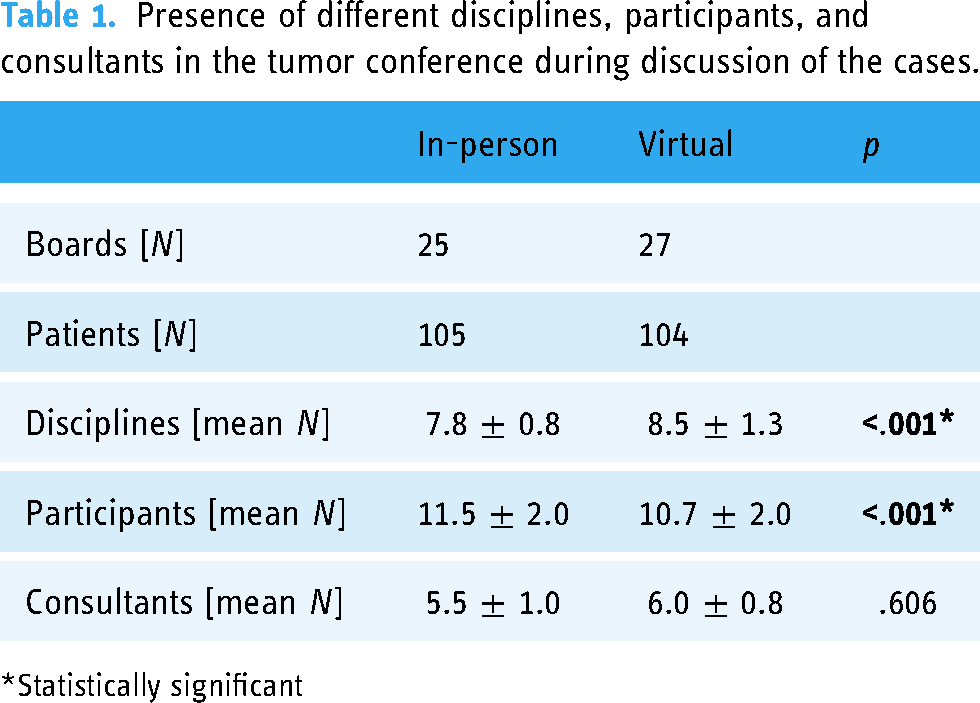
Statistically significant
Waiting times of patients with a malignant lesion in days.
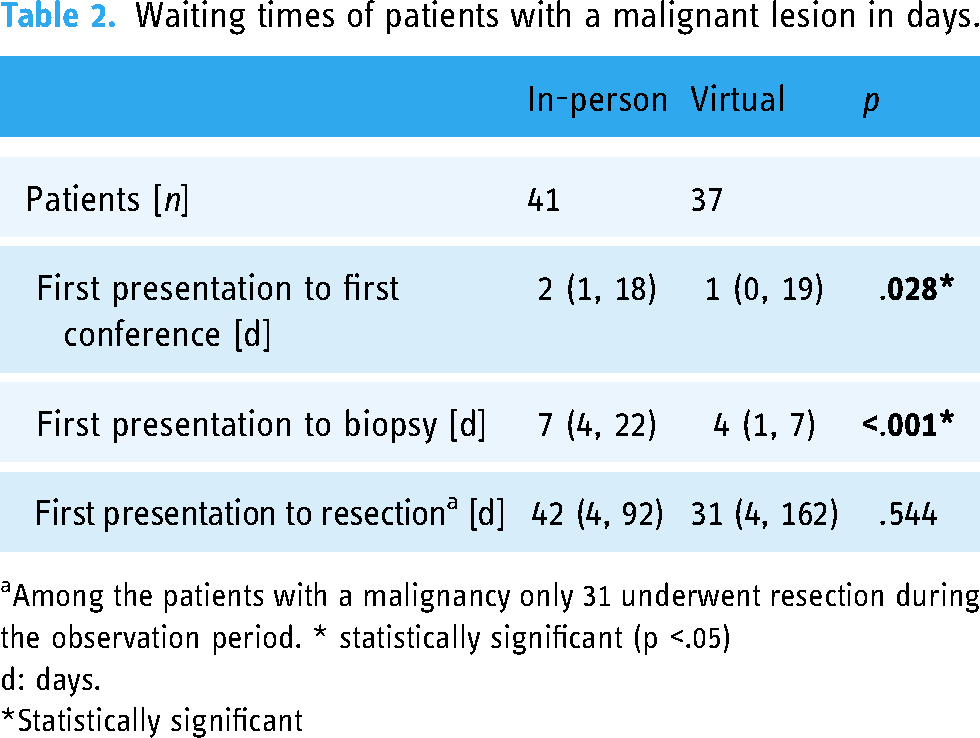
Among the patients with a malignancy only 31 underwent resection during the observation period. * statistically significant (p <.05)
d: days.
Statistically significant
Definitive histologic evaluation revealed benign tumors in 97 (55.4%) of the biopsied patients and malignancy in 78 (44.6%). Among the patients with malignancy, 36 (46.1%) already had distant metastases. Resection was performed in 86 patients, of whom 31 (36.0%) had malignant lesions and 55 (64.0%) had benign tumors.
Differences between in-person and virtual tumor conferences
While the number of total participants was slightly lower with virtual tumor conferences (p < .001, Table 1), more disciplines were represented compared to in-person tumor conferences (p < .001).
The level of available expertise did not differ between in-person and virtual tumor conferences with median 6 consultants representing their specialties with each of the modalities (p = .606). Looking at the waiting times of patients who revealed to have a malignant lesion, the patients were discussed earlier in the virtual conferences (p = .028, Table 2). Furthermore, cases discussed in the virtual conferences could be submitted to biopsy earlier than those discussed in in-person conferences (median 4 vs. 7 days after first presentation, p < .001, Table 2). The interval between initial presentation and resection did not differ significantly (p = .544) among the two conference modalities.
Discussion
Due to the COVID-19 pandemic and resulting contact restrictions many tumor conferences were transitioned to a digital meeting.13–17
The purpose of the present study was to compare in-person and virtual MTCs analyzing participant number, multidisciplinarity, level of expertise, and individual patient flow.
Our data suggest an advantage of virtual tumor conferences regarding the number of participating disciplines, time from first visit to tumor conference and time from first visit to biopsy. These findings show that switching to virtual MTCs at least has no negative effects on the logistics of cancer care.
The number of patients discussed in our MTCs was almost the same in in-person and virtual MTCs. A recent study found that the number of presentations in a comprehensive cancer center decreased by up to 9.4% after the switch to virtual MTCs during the COVID-19 pandemic compared to the equal time span in 2019. 19 Kiong et al. showed a reduction of 27.4% in the total number of cases presented at MTCs. 16
In contrast, another study reported no significant difference in patient numbers in virtual tumor conferences in 2020 compared to in-person tumor conferences during the same period in 2019. 15 Different studies even reported a 20% and 22% increase in patients with the introduction of virtual MTCs.13,14 Therefore, more patients had been discussed in virtual tumor conferences.
A significant increase in multidisciplinarity was observed after the transition to virtual MTCs. Even though a previous survey on virtual neuro-oncological tumor boards reported an unchanged participation rate of individual disciplines, 20 it may be that virtual MTCs allow experts of different disciplines to take part in different MTCs simultaneously. In our study, there was a significant reduction in time from first visit to MTC and from first visit to biopsy. This could benefit cancer patients but is not consistent with other studies which found no significant change in duration between first visit to in-person and virtual MTC.14,16
In our study, we saw a decrease in participants from 11.5 in in-person tumor boards to 10.7 in virtual MTCs. In contrast to our data, Davis et al. found a 46% increase in participants after implementing virtual meetings. 13
A key limitation of this study is its retrospective design and the lack of follow-up examinations to assess the long-term impact of virtual tumor conferences on cancer patients.
Furthermore, the results may not be generalized because they reflect practice at a single institution.
We analyzed data from September 2019 to February 2020 and May 2020 to October 2020. Both periods of time are equally long. However, we did not compare the same months in 2019 and 2020 and, thus, cannot rule out seasonal effects.
Further studies on this topic will be required to assess the final effect on patient outcome.
The COVID-19 pandemic and its resulting contact restrictions have shown the validity of virtual meetings, such as tumor conferences. This study is a first step to evaluate advantages of a transition from in-person MTCs to virtual MTCs. With the possibility of future pandemics, virtual tumor conferences might become more feasible and should be routinely implemented in clinical practice. 21 Furthermore, the participation of medical experts or health care personal in more remote areas could be facilitated by virtual meetings. This might contribute to an improved treatment of cancer patients worldwide.
Due to this positive experience our institution will be permanently discussing tumor patients in hybrid conferences which can be attended both in-person and virtually.
Conclusion
In this retrospective case series, the transition to virtual MTCs seemed to have had a beneficial effect on timely diagnosis and multidisciplinarity during tumor conferences. Virtual MTCs may, therefore, accelerate decision-making and treatment in patients with musculoskeletal tumors.
Footnotes
Contributorship
VH performed most of the data acquisition and participated in literature research, designing the study and drafting the manuscript. JP, NS, and ER participated in literature research, gaining ethical approval and revised the manuscript. CH participated in designing the study and revised the manuscript. GO performed the statistical analysis and participated in literature research, designing the study and drafting the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the medical faculty of the University of Leipzig approved this study (Ethikkommission der Medizinischen Fakultät an der Universität Leipzig, reference 537/20-ek).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Georg Osterhoff