
Abstract
Throughout the COVID-19 pandemic, a variety of digital technologies have been leveraged for public health surveillance worldwide. However, concerns remain around the rapid development and deployment of digital technologies, how these technologies have been used, and their efficacy in supporting public health goals. Following the five-stage scoping review framework, we conducted a scoping review of the peer-reviewed and grey literature to identify the types and nature of digital technologies used for surveillance during the COVID-19 pandemic and the success of these measures. We conducted a search of the peer-reviewed and grey literature published between 1 December 2019 and 31 December 2020 to provide a snapshot of questions, concerns, discussions, and findings emerging at this pivotal time. A total of 147 peer-reviewed and 79 grey literature publications reporting on digital technology use for surveillance across 90 countries and regions were retained for analysis. The most frequently used technologies included mobile phone devices and applications, location tracking technologies, drones, temperature scanning technologies, and wearable devices. The utility of digital technologies for public health surveillance was impacted by factors including uptake of digital technologies across targeted populations, technological capacity and errors, scope, validity and accuracy of data, guiding legal frameworks, and infrastructure to support technology use. Our findings raise important questions around the value of digital surveillance for public health and how to ensure successful use of technologies while mitigating potential harms not only in the context of the COVID-19 pandemic, but also during other infectious disease outbreaks, epidemics, and pandemics.
Keywords
Introduction
Throughout the COVID-19 pandemic, a variety of new and existing surveillance technologies were leveraged to aid the public health response. 1 Deploying digital technologies (e.g. cell phone geolocation, mobile phone contact tracing applications, closed-circuit cameras, drones) for population surveillance and public data collection was often rationalized by states, public health agencies, and the private sector as an acceptable approach to help mitigate the spread of COVID-19 and to enhance compliance with public health measures. 1 Lyon (2007) defines surveillance as "the focused, systematic, and routine attention to personal details for purposes of influence, management, protection or direction” (p. 14), and the World Health Organization provides a broad definition of public health surveillance as continued watchfulness and the monitoring of events in humans linked to action.2,3 Specifically, public health surveillance consists of passive (data routinely submitted on reportable diseases and programs) and active (purposeful informationseeking of a disease or condition) surveillance. Current surveillance for pandemic and non-pandemic purposes has been sustained through passive and active strategies integrating advanced data analytics and sophisticated technologies. Information gathered through surveillance also improves the efficiency and effectiveness of health services by targeting interventions and documenting their effects on the population. 4
The urgency to mitigate the effects of the pandemic (e.g. disease-related morbidity/mortality, burden on health care services, economic and social impact) has led to a surge of digital technology development to support public health practices.5,6 However, concerns remain that the speed of this response, if not properly governed, may lead to unintended consequences, including threats to privacy and infringement of civil liberties, 7 inequitable surveillance of marginalized groups, 8 and risk of undermining human rights. 9 Furthermore, the rapid pace of pandemic-related technological development and implementation has limited opportunities to consider not only the potential and witnessed consequences of technology (mis)use, but also whether surveillance through these digital technologies is effective in supporting public health goals, such as disease containment. 10
These knowledge gaps limit the possibility of developing and using technologies that are responsive to public health needs while also promoting civil liberties and human rights. To fill these gaps, this study maps the current evidence regarding the utilization of digital technologies for pandemic-related public health surveillance to inform technology design, evaluation, and policy-making. To this end, this scoping review was guided by the following research questions: (1) what digital technologies were used for COVID-19 public health surveillance? and (2) how effective have digital technologies used for surveillance been in supporting public health goals during the COVID-19 pandemic?
Due to the breadth and depth of the literature targeted in this review, this paper focuses on describing what digital technologies were used globally during the COVID-19 pandemic response to address public health and other goals and how such technologies were utilized by states, public agencies, the private sector, and other actors. A forthcoming second scoping review paper will address the short- and long-term implications of digital health surveillance for public health purposes during the COVID-19 pandemic response.
Given the rapid pace of digital technology development and implementation for public health surveillance during the COVID-19 pandemic, the findings of this scoping review fill critical gaps in our knowledge of which technologies are being used for surveillance, how they are used, and factors shaping the success of digital surveillance for public health. This knowledge will be important for informing future decision-making in areas including public health, governance, policy-making, and industry, particularly given the emergence of new infectious disease outbreaks, such as the 2022 mpox outbreak.
Methods
This study followed the five-stage methodological framework described by Arksey and O’Malley 11 and Levac et al. 12 to investigate the peer-reviewed and grey literature on the use of digital technologies for public health purposes during the COVID-19 pandemic. The stages of this methodological framework include: (a) identifying the research question, (b) identifying relevant studies, (c) study selection, (d) charting the data, and (e) collating, summarizing, and reporting the findings.11,12 This review also conformed to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Protocols reporting guidelines in our selection process and in manuscript preparation. 13 A complete description of this study's methodology is reported elsewhere 14 and is summarized below.
Data collection
Peer-reviewed literature search
A literature search was conducted in January and February 2021 to collect English-language peer-reviewed and grey literature from the following databases: Medline (Ovid), PsycInfo (Ovid), PubMed, Scopus, CINAHL, ACM Digital Library, Google Scholar, and IEEE Explore. Additional hand searches of key journals and reference lists identified by our multidisciplinary team of researchers were also conducted to identify publications that were missed during the database searches. Papers were selected for review if the title, abstract, and full paper met our eligibility criteria. See Figure 1 for the search terms developed following consultation with a health specialist research librarian.
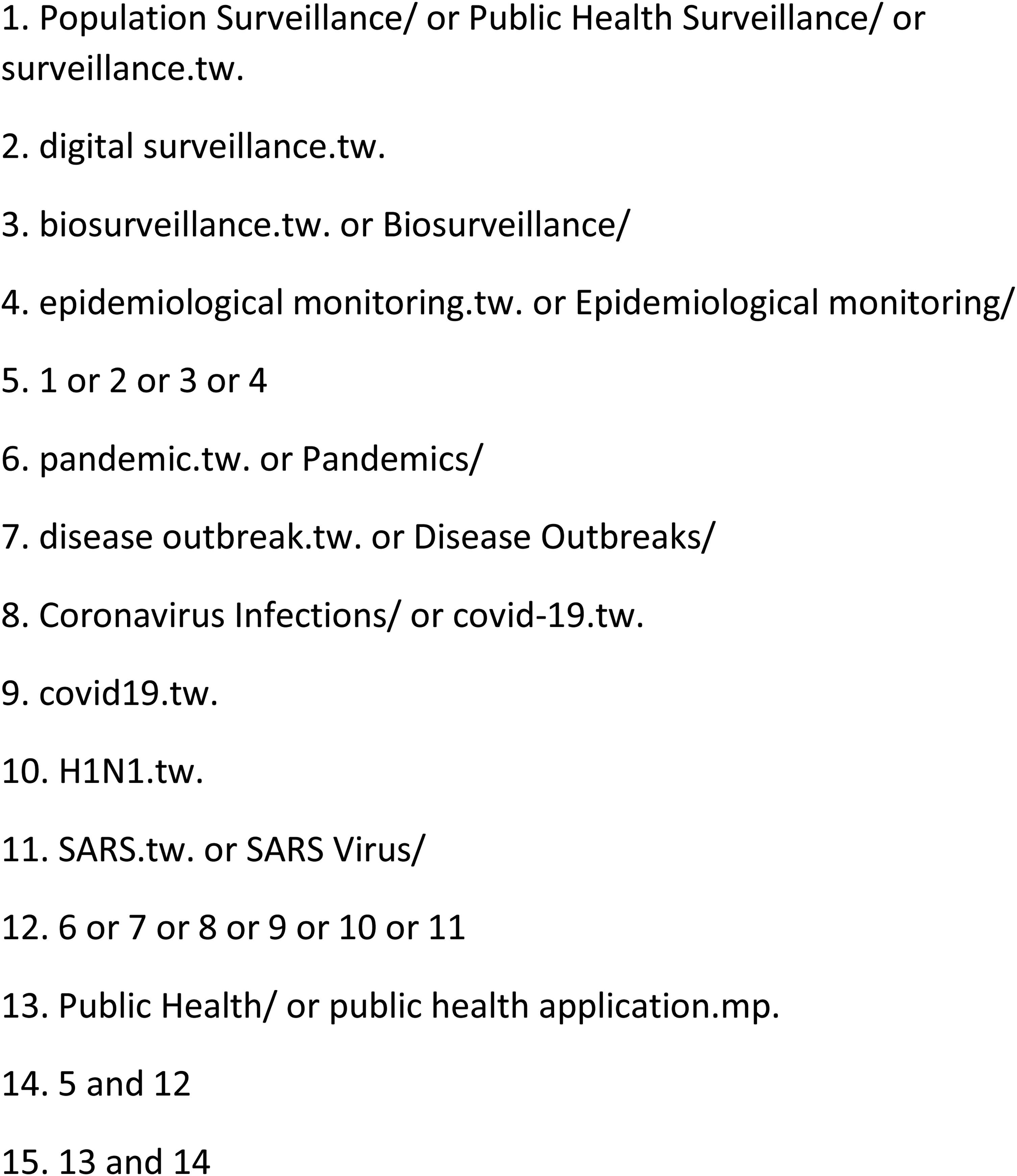
Search terms developed with assistance of health specialist research librarian.
An initial broad search was conducted by one researcher to capture all English-language publications on the use of digital technology during pandemics, epidemics, and outbreaks published between January 2010 and December 2020. Initial search results yielded 18,891 results. Following the removal of 9261 duplicates, 9630 unique documents were retained for title and abstract screening. Documents were retained for full-text review if they met the following inclusion and exclusion criteria during title and abstract screening:
Title or abstract mentioned the use of a digital technology for public health surveillance Public health surveillance focused on monitoring and curbing infectious disease spread Public health surveillance focused on monitoring humans rather than non-human animals Digital technology was explicitly used for surveillance (e.g. data collection for continued watchfulness and monitoring).
Following title and abstract screening by two researchers, 2076 peer-reviewed publications were retained for full review. Publications were included if they met the same criteria applied during title and abstract review. Following a full-text review by two researchers, 888 publications were retained for analysis.
Given the large number of publications retained, for practical purposes, our research team narrowed the sample further by focusing specifically on digital technologies used for public health surveillance from 1 December 2019 to 31 December 2020 during the COVID-19 pandemic. We focused on articles published during this first year to offer a snapshot of early academic and grey literature publications regarding digital surveillance during the COVID-19 pandemic in the face of a paucity of information on the disease itself as well as the potential value and consequences of surveillance measures.
To this end, an additional set of inclusion and exclusion criteria was applied during this secondary screening, and publications were retained for analysis if they met the following criteria:
Publication date between 1 December 2019 and 31 December 2020 Title or abstract explicitly included any of the terms “coronavirus,” “COVID-19,” “SARS-CoV-2,” or “severe acute respiratory syndrome coronavirus.”
Following secondary screening by two researchers, a final sample size of 147 publications was retained for analysis. At all points during the screening process, in cases where these two researchers disagreed regarding inclusion or were uncertain whether a publication met the inclusion criteria, a third researcher read the full text and, following discussion with the two researchers, determined whether to retain the text for analysis.
Grey literature search
Our team, which included interdisciplinary researchers and a health research librarian, guided our search of the grey literature through the selection of relevant organizational websites that explore policies related to digital technology for health surveillance purposes. These included the Ada Lovelace Institute, Human Rights Watch, and the Munk School. A search of the websites of these organizations was conducted manually in January and February 2021 with the internal search tools on each website to retrieve potentially relevant current and archived documents. One researcher searched these websites using the same search protocol utilized to search the peer-reviewed literature, yielding a total of 141 publications.
Grey literature documents were reviewed independently by two researchers based on the same inclusion and exclusion criteria used to screen the peer-reviewed literature. In total, 74 documents were retained for analysis. Additionally, five conference proceedings found during the search of the peer-reviewed literature were retained as grey literature, for a total of 79 documents retained.
See Figure 2 for the PRISMA chart detailing this study's identification and screening process.

Study selection process.
Data analysis
Inductive coding analysis was conducted on each publication in this sample to identify dominant themes and patterns. 15 Five researchers convened to discuss identified themes and findings from a review of 10 randomly selected publications, and, from this, an extraction table was generated. An analysis of five additional publications further refined the data extraction table. Five reviewers piloted the data extraction process, discussed findings for consistency of analysis, and collaboratively reviewed all retained documents for data extraction and analysis related to: (a) authors, (b) author location(s) based on affiliated institution(s), as identified in publications, (c) study aim or objective, (d) methodology and research design, (e) countries or regions identified, (f) types of digital technology identified, (g) intended or stated outcomes of digital technology use, (h) target population(s), (i) unintended (or not explicitly stated) or predicted outcomes and implications of technology use, and (j) theoretical analysis, arguments, discussions, and debates. In an iterative fashion, findings were presented to the larger interdisciplinary research team for further analytical discussion; this approach ensured that interdisciplinary insight was applied to the findings from a range of expert perspectives. The research team consisted of experts in nursing, medicine, public health, epidemiology, surveillance, geography, health information science, law, bioethics, policy, knowledge translation sciences, critical theory, and sociology of health. The strength of this iterative approach to data analysis was the generation of findings informed by a diversity of expertise and multiple perspectives. Furthermore, regular comparison of analyses using the extraction table during weekly meetings ensured shared understanding among researchers and consistency in data analysis. We also ensured data analysis was rigorous through techniques well-suited to qualitative research, including ensuring dependability through comparisons of researchers’ analyses of the data and attending to potential biases through reflexive discussions. 16
Results
Of the 147 peer-reviewed publications in this sample, the majority were commentaries (n = 39) and reviews (n = 39), including reviews of the literature on the use of digital technologies for public health surveillance and predicted or witnessed implications of surveillance. Other publications included analyses (n = 27), reports (n = 8), empirical studies (n = 24), legal reviews (n = 3), and one policy analysis paper. The grey literature publications (n = 79) included commentaries and opinion pieces (n = 33), video and audio recordings or transcripts of meetings, conferences, and panels (n = 8), news reports of digital technologies used during the COVID-19 pandemic (n = 33), and conference proceedings (n = 5).
To better understand the international breadth of the literature, we identified the listed authors of each peer-reviewed publication, noted their affiliation(s) (typically a university, think tank, or non-profit organization), and identified the location of their affiliation(s); authors of more than one publication were only counted once. Given the lack of location or affiliation information for authors of grey literature publications (including, in some cases, no author information), analysis of authors’ locations was limited to the academic literature. By far the most common country of affiliation was the USA (n = 156), followed by the UK (n = 91) and India (n = 40). Many authors were also affiliated with institutions in China (n = 28), Australia (n = 28), Singapore (n = 27), Spain (n = 25), Italy (n = 24), Germany (n = 21), and Brazil (n = 20). Other affiliations included Japan (n = 19), the Democratic Republic of Congo (n = 16), Switzerland (n = 16), Taiwan (n = 15), Canada (n = 14), Ireland (n = 12), South Africa (n = 11), and Iran (n = 9). While many authors were affiliated with European (n = 230) and North American (n = 172) institutions, comparatively fewer were associated with institutions from regions including Africa (n = 31), South America (n = 20), and Central America (n = 0).
Global use of digital technologies for surveillance during the COVID-19 pandemic
Descriptive overview
Our review of the literature found a total of 90 countries or regions in which the use of at least one digital technology for public health surveillance during the COVID-19 pandemic was identified. Some of the most frequently used technologies included: (a) mobile phone devices and applications—particularly applications intended to support contact tracing, (b) mobile phone tracking through technology including Bluetooth and GPS, (c) drones, (d) temperature scanning technologies, and (e) wearable devices. While a wide variety of digital technologies used for public health surveillance were identified in the literature, these technologies were not always clearly defined or described. Terms such as “big data,” “AI,” and “mobile app” were not always defined, which complicated efforts to precisely identify what digital technologies were used globally for surveillance purposes during the COVID-19 pandemic.
The digital surveillance technologies identified in the literature can be distinguished along several axes. One distinction of note was between technologies that required user interaction or participation, such as mobile applications for proximity tracking or symptom screening, as opposed to technologies working in the background, including closed-circuit television (CCTV) cameras, social media, and web search analysis. Digital technologies used for surveillance also differed in origin: some technologies, including CCTV cameras, were in use prior to the pandemic and were repurposed for digital surveillance for public health purposes. Others, including many mobile contact tracing applications and the Apple–Google programming interface to support digital proximity tracking, were created specifically to respond to the COVID-19 pandemic. Some technologies consisted of hardware—e.g. CCTV cameras, drones, and digital thermometers—while others were primarily forms of software, e.g. mobile phone applications and facial recognition technology.
Table 1 lists all technologies identified in the literature (and, where noted in the literature, the country or region where the technology was used) and categorizes technologies as either hardware or software and as either passive or active surveillance (or both). The table also identifies whether each technology was specifically created or substantially modified for use during the COVID-19 pandemic or whether its use preceded the pandemic. As indicated, only two technologies were significantly modified for use during the COVID-19 pandemic—mobile phone applications, which were largely designed to support digital contact tracing, and the Apple–Google application programming interface (API). Otherwise, all other technologies were simply repurposed for public health surveillance without significant alteration.
Technologies used for digital surveillance during the COVID-19 pandemic identified in the peer-reviewed and grey literature.

Note: CCTV: closed-circuit television; API: application programming interface; QR: quick response.
Most of the digital technologies identified in the review of literature were used by states and their agents (e.g. public health agencies), including private–public partnerships, such as state use of the Apple–Google exposure notification system, a programming interface that supports the development of applications to facilitate digital contact tracing.5,8,17–185 Other users included employers,26,33,55,65–67,72,75,101,102,114,186–191 who used technologies including thermal cameras in the USA, 67 mobile applications in the USA and the UK,31,89,101,130 and wearable devices in the USA102,130,186 to track employees, clinicians, and researchers in clinical settings25,29,65,71,76,81,82,114,189,190,192–194 (e.g. use of a web-based staff surveillance system in a hospital in Singapore 26 and use of a mobile application and wearable wristband in Spain 189 to track disease spread and contacts among hospital staff).
Targeted populations
Populations targeted for digital surveillance tended to comprise either an entire population in a given geographic region (e.g. entire population of a specific country), as reported by a majority of studies (n = 213),5,7,8,17–25,27–56,58,60–63,65–80,82–97,99–123,125–152,154,156–185,187,188,191,193–239 or a smaller targeted group of individuals, including travelers, people in imposed quarantine, health care staff and patients, and marginalized groups (e.g. racialized communities, migrants, lesbian, gay, bisexual, transgender, queer (or sometimes questioning) communities, gender minorities) (n = 54).21,26,27,29,31,32,37,44,49,51,52,55,57,59,64,65,67,71,74–76,81,89,91,94,98,101,102,123,124,130,131,137,138,141,142,145,146,150,154,157,172,173,176,179,186,188–190,192,194,236,237,240
Intended or stated use of technology
The most frequently reported intended use of COVID-19-related digital technology was for active public health surveillance related to identifying individuals infected with COVID-19 and/or presenting symptoms and their contacts, i.e. contact tracing (n = 155).7,8,17,21,24,27,35–37,41–43,45–47,49–56,59,63,66,68–79,81,83–85,87–90,93–123,125,126,128,129,131–143,147–150,152–157,159–170,172–185,187,190,191,194,195,199,201,207,214,218–222,224,225,227,231,235–238 Other intended outcomes included informing states’, public health agencies’, and individuals’ responses to the pandemic through information obtained by monitoring, predicting, and modelling disease spread (n = 70),17,18,23,27,28,33,35,38,41,44,55,57,59,61,63,65,68,70–74,76–78,86,90,91,97,98,102,103,106–108,113,115,133,141,158,174,175,177,185,188–191,196,198,204–206,208,210–212,215–217,223,224,226–230,236,237,239 monitoring and ensuring compliance with public health measures, e.g. enforcing quarantine and controlling movement (n = 66),17,18,21–23,27,28,31,32,34,35,37,40,43–49,52,53,55,56,68–72,74,75,77,83,92,94,95,97,99,102,104,108,111–113,116,120,130,131,137–139,141,142,145,146,150,157,172,173,176,203,206,208,226,231,237 and informing direct provision of health care services and allocating resources, e.g. monitoring disease spread among health care staff (n = 45).23,26,35,44,52,55,65,67,68,71,74,76,78,80–82,90,96,102,104,113,127,138,140,158,177,188–190,192–194,200,206,208,209,212,214,217,223–225,230,231,237
Thematic analysis of the literature
There are three overarching themes identified within this scoping review that provide insight into the overall effectiveness of surveillance through digital technologies to respond to the COVID-19 pandemic. The first theme, Successful Use of Digital Technologies for Public Health Surveillance, relates to the value of digital technologies and whether use of digital technologies for surveillance during the COVID-19 pandemic was successful in achieving intended outcomes. A second theme, Factors Shaping Successful Use of Surveillance Technology, relates to discussions within the literature regarding the factors shaping the potential success of technology use for public health purposes. These factors are associated with five subthemes: uptake of digital technology; technological capacity and errors in technology; scope, validity, and accuracy of data; guiding legal frameworks; and infrastructure to support technology use. A third theme, Techno-Solutionism and Resource Allocation, warns against techno-solutionism by drawing on skepticism regarding the value of digital technologies for surveillance and the paucity of evidence of success.
Successful use of digital technologies for public health surveillance
The authors varied in how they measured and defined success. Some empirical studies evaluated a technology's success based on quantitative improvements in key performance indicators. For instance, an empirical study of a symptom screening application used in Thailand found the application was successful in reducing strain on the health care system as fewer people contacted health care providers regarding their symptoms. 29 Other analyses of surveillance technologies used during the pandemic operationalized success as higher recovery rates with reduced impact on the economy, 237 increased speed of case identification, 94 increased accuracy in detecting and predicting disease spread, 228 and reducing COVID-19-related morbidity and mortality rates.98,205,208
The utility of digital technologies for public health surveillance during the COVID-19 pandemic was debated across the literature. Some researchers argued that digital technologies may have value for public health purposes specific to understanding or predicting disease spread, contact tracing, ensuring physical distancing, and enforcing quarantine, including three empirical studies on modelling and prediction of disease spread,196,198,200 and nine other studies found value in aggregated data sets for modelling and predicting disease spread.90,204,206,210,213,215,216,228,230 The authors of five studies indicated that technologies such as digital contact tracing tools (e.g. mobile phone applications, mobile phone tracking) had an impact on reducing COVID-19 disease spread.47,75,80,121,184 A few also offered some support for the use of self-reported data requiring voluntary consent.29,30,207
However, in many publications (n = 42), the authors expressed significant reservations towards the use of technology and offered doubts regarding their effectiveness for public health purposes for reasons listed in the second theme below.8,28,36,40,43,53,58,63,67,87,89,101,124,125,127,130,131,133,134,136–140,142–146,148,149,163,170,172,180–182,191,193,202,218,226 The authors of several publications (n = 32) weighed the benefits of surveillance against potential and witnessed harms when evaluating the success of digital technology use for public health surveillance.18,20,23,24,31,36,37,40,49,50,60,65,66,68,76,79,90,93,98,103,107,108,113,114,117,119,125,127,135,186,195,199 Parker et al., 119 for example, questioned how we might evaluate the moral importance of saving lives and how risks to privacy and liberty should be weighed against the scale of suffering presented not only by the disease itself but also by the use of restrictive public health measures (e.g. capacity limitations, closures, etc.) intended to reduce disease spread. 119
Many authors also oriented to the question of whether to use digital technologies for public health surveillance as a trade-off between benefits and costs, e.g. trade-offs between compromising democratic principles, such as the right to privacy, and mitigating the impacts of the COVID-19 pandemic.23,41–43,46,55,99,100,117 Conversely, Christou et al. 45 framed the idea of a trade-off as a false dilemma and argued instead that public health goals and the protection of fundamental rights are intertwined. Technology design was also conceived by some authors as a trade-off between utility, privacy, and data security.32,40,51,53,73,102,107,120,241 Bluetooth technology, for example, was highlighted in several studies as a means of supporting contact tracing that, although potentially more inaccurate than other technologies, such as GPS, would better preserve individuals’ privacy and data security because it can be operated through a decentralized model that retains data to the user's mobile phone rather than aggregating data in a central database.32,40,51,53,102,111,120
Factors shaping successful use of surveillance technology
Uptake of digital surveillance technologies
Authors of many publications (n = 41) identified participation in digital surveillance and technology uptake across targeted populations as a key factor shaping the success of digital surveillance.7,18,20,23,28,36,42,43,46,55,63,66,68–70,72,74,76,78,84,85,87,89,90,93,100,101,103,106–108,115–117,164,189,219,224,231,238,242 Some authors attributed the limited success of mobile contact tracing applications in countries including France, South Korea, and Singapore to low rates of usage by individuals,20,72,84,87,89,238 while others suggested that technologies deployed in clinical settings to monitor staff 189 and surveillance networks to track disease spread 23 have limited value due to low rates of participation. Low uptake was attributed to several factors deterring individuals from using technologies, including issues with limited mobile phone battery “life,”40,42,72,84,89,167,238 limited access to technology including smartphones and inadequate Internet connection,8,18,20,24,25,31,32,36,61,64,87,129,134,163,167,195,207,225 users’ concerns around data privacy and security,63,89,100,121 and lack of trust that digital surveillance has value for mitigating COVID-19.10,21,46,84,100,102,126,129,133,136,167,186,218,235 In contrast, one study identified Northern Ireland's mobile contact tracing application, developed and promoted by the state, as an example of an application that was successfully deployed with high rates of participation. 121 The authors attributed high uptake to the government's attention to local needs, care taken to build public trust, dedication to ensuring data privacy, and daily updates provided by political representatives.
Technological capacity, limitations, and errors in technology
The authors of numerous publications (n = 59) focused on the capacities of digital technologies and how limitations and technological errors impacted the success of digital surveillance during the COVID-19 pandemic.18,24,28,32,36,40,42,45,46,51–55,59,60,63,65,67,68,70,72–76,84,89,93,102,103,105,108,111,113,114,118,120,124,125,127,128,131,134,145,146,149,182,183,193,194,199,202,213,219,220,226,227,243 Bluetooth technology, which was widely used (e.g. in the USA, the UK, Switzerland, India, Poland, Indonesia, Germany, France, Australia, Canada, and Singapore) to support proximity and location tracking, was described in many studies as inaccurate.24,28,32,45,53,63,74,75,105,202 While Bluetooth was favoured by many countries for its short-range wireless technology that allowed for decentralized contact tracing between users’ mobile phones, it also has a greater potential for false positives, as signals pass between walls or floors of a building and therefore do not accurately detect contacts between users.45,53 GPS technology, which was used in countries including the USA, Norway, Bahrain, and Kuwait to support proximity and location tracking, was also described as imprecise, particularly in crowded areas.28,53,75,202
Likewise, while thermal cameras were used (e.g. by cruise lines, grocery stores, jails, warehouses, hospitals, hotels, and government agencies in countries including China, Thailand, the USA, Singapore, Italy, the UK, and Australia) to detect elevated temperatures as a proxy for identifying fever as a symptom of COVID-19, one study found thermal cameras to be inaccurate at detecting fevers and noted that thermal cameras cannot distinguish causes for elevated temperature including menstrual cycle, pregnancy, and substance use. 67 Some authors also discussed technological errors that may compromise the effectiveness of digital surveillance,40,42,45,46,60,145,182,199,202 including errors in a Russian mobile phone application that required people infected with COVID-19 to send digital photographs of themselves as proof that they were quarantining at home. Errors barring users from taking and sending photographs resulted in fines.145,146
Scope, validity, and accuracy of the data
Authors of many publications (n = 52) highlighted the importance of collecting valid, generalizable, and accurate data for public health purposes.8,18,20,23–25,28,30,31,36,40,49,54,55,59,60,63,72,73,75,87,90,92,93,96,97,99,100,103,105,108,111,118,120,127,142,144,146,163,188,195,202,206,217,221,223–226,231,237,239 Some authors argued that statistical errors, including sampling and measurement errors, limit the epidemiological value of data gathered through digital surveillance (e.g. Google Trends search data to monitor disease spread rely on a biased sample of people who use Google as a search engine, who have Internet access, and who have digital literacy skills).63,118,210,215,226 Three studies examined the use of analytical tools, including artificial intelligence, big data analytics, and machine learning, for monitoring and predicting disease spread, and found that their accuracy was limited by the unavailability of high-quality data in standardized formats.195,206,226 Other authors cautioned that data from participatory/self-reported surveillance technologies, e.g. mobile symptom screening applications and web surveys, may be biased, contain errors, or fail to capture other patterns of disease spread and population movement.30,217
Several authors focused on the digital divide—a gap between those who have access to digital technologies and those who do not 90 —as a potential barrier to the collection of accurate, representative, and generalizable data on all populations. Mobile applications, for instance, were found to exclude groups with limited access to smartphones, such as low-income populations,24,231 people with low digital literacy skills, 202 groups whose access to technology may be erratic, 36 technology non-adopters due to religious and other reasons,54,221 children, 75 people living in rural or remote locations with minimal or no Internet access, 75 older adults who are less likely to own a smartphone, 83 migrant workers, 83 disabled people, including those with low vision and difficulties with motor control, 83 and people who are not housed or who are precariously housed. 97
The authors also identified highly vulnerable groups who live in conditions incompatible with digital surveillance, such as migrant workers, who may not have access to technology or Internet connectivity. 8 Other examples included people in countries such as Canada for whom smartphones are not accessible, despite the fact that these people are often those who have been most affected by the COVID-19 pandemic, such as racialized non-white people.163,167 Members of marginalized groups may also be wary of using surveillance technologies given long histories of inequitable surveillance and monitoring, including undocumented migrants and racialized non-white people.72,97 Some authors suggested that a lack of data on these underrepresented groups may exclude vulnerable groups from consideration in public health decision-making.124,142,167 While large datasets may be valuable for predicting disease spread and identifying disease clusters, aggregated data may also obscure social realities. For instance, one editorial from the grey literature argued that location data used to detect mobility patterns do not reveal why individuals are moving, particularly in the case of marginalized groups seeking shelter, traveling to food banks, escaping overcrowding, and accessing supports and services. 144
Guiding legal frameworks
The rapid pace of technological development, evaluation, and deployment in the context of the COVID-19 pandemic has meant that in many countries and regions, digital technology use has outpaced legislation and legal frameworks. Authors of several publications (n = 50) found that legal frameworks regulating the collection, storage, use, and sharing of health data are vital for supporting efficacious and ethical digital surveillance.6,21,23,24,27,28,31,36,40,55,58,60,66,71,73–75,78,82,88,90,107,108,115,120,123,127,128,131,134,137,138,140,141,147,151,170–173,180,182,186–188,191,195,209,229,235
The USA, for instance, was criticized for its lack of adequate privacy protections and insufficient federal laws around digital surveillance, particularly in the case of digital technologies used by private firms, which are not bound by the USA Health Insurance Portability and Accountability Act of 1996.24,55,75,229 In contrast, one study described the South Korean government's quick movement to revise their information privacy laws as essential to clearing the way for the rapid deployment of digital surveillance technologies. 27 While abrupt changes in government surveillance powers may risk abuses of individuals’ rights and increased monitoring and social control, the authors argued that within South Korean culture, state surveillance and data mining have been publicly accepted because they serve the greater good.
Some authors argued that existing regulations around digital surveillance are fragmented and that wide variations between countries and regions present a barrier to establishing a global, responsive standard for data collection for public health.66,71,90 The establishment of national and global legal frameworks was identified as particularly urgent in the case of newer or rapidly developing technologies deployed during the COVID-19 pandemic.23,24,40,60,66,71,74,75,78,90,108,120,128,134,137,147,182,188,191,209,229 One study, for example, described machine learning as still in its infancy and called for greater legal oversight as the risks associated with machine learning are still not fully known. 191 Others warned that risks associated with digital surveillance, including risks to privacy and civil rights, change over time, necessitating strong regulations that will remain relevant in the face of rapid changes.24,108,191
Infrastructure to support technology use
The authors of several publications (n = 44) identified adequate infrastructure as essential to successful digital public health surveillance during the COVID-19 pandemic.18,21,23,24,26,28,31,36,40,43,55,61,64,70–76,78,82,90,96,103,111,113,119,122,127,128,134,147,151,184,188,191,199,201,202,205,207,232,237 Included in definitions of adequate infrastructure were essential features of public health responses to COVID-19 (e.g. mass testing for COVID-19, consistent reporting of case counts, ability for infected individuals to isolate, fully integrated public health systems, and manual contact tracing).18,23,24,36,40,43,55,72,119,122,127,134,184,191 Researchers also identified critical components of economic, social, cultural, technological, and environmental infrastructure imperative for successful use of digital technologies. These included national health information technology infrastructure to support data sharing across institutions and regions, sufficient funds, Internet infrastructure and technology availability, and internationally supported and standardized protocols for data sharing.18,23,61,73,74,76,78,96,111,119,151 Several authors argued that while digital surveillance can augment traditional public health measures and infrastructure for responding to public health crises, they cannot replace them.70,75,184,202,205,207
Existing infrastructure was identified as a key factor in the success of digital surveillance in several countries. One study attributed China's successful containment of COVID-19 disease spread to a syndromic surveillance system used in the province of Hubei that quickly integrated non-traditional data sources (e.g. social media data) with existing databases. 64 Another study examined the use of digital technologies (e.g. GPS location tracking, credit card transaction data, CCTV cameras, and highway electronic toll systems) in Taiwan to support contact tracing and track disease spread. This study found that Taiwan's existing public health infrastructure, developed following the SARS outbreak in 2003, was critical to the success of these digital surveillance measures. 59
Techno-solutionism and resource allocation
Given the limited evidence demonstrating clear value of digital technologies used for public health surveillance during the COVID-19 pandemic, some authors (n = 28) included warnings against techno-solutionism: unchecked belief in the value of technological solutions to address or resolve social and public health problems without considering their repercussions or the risks of diverting resources from proven public health measures to technology development and use.25,28,41,42,54,55,59,64,69,81,87,103,118,119,123,126,128,134,135,144,148,182,184,191,209,221,222,232 One author also used the term “digitalism” to caution against an “unchecked and misguided belief in extreme digital connectivity without considering the attendant repercussions on science, human rights, and everyday practices of democracy.” (p. 462) 209 Another author warned that faith in technology as a panacea may lead to dismissal of social concerns that should be addressed at the level of policy, including questions around how data are used and who is excluded from use of digital technologies. 221
Several authors argued that digital surveillance had, at best, a negligible impact on mitigating the COVID-19 pandemic, referencing examples including the UK government's development of a mobile phone application to support contact tracing that was originally endorsed by the state as a solution to escaping lockdown measures but was increasingly deemphasized due to its marginal impacts.28,55,118,128,182,209 Given the limited success of many forms of digital surveillance, some authors questioned whether a focus on technological solutions is advisable at the risk of diverting resources from proven public health measures, including traditional contact tracing and widespread disease testing.8,25,40,44,144 As implementation of digital surveillance was also found to be resource intensive, e.g. necessitating specialized skills and bearing high monetary costs, some authors cautioned that the cost effectiveness of digital surveillance must be carefully considered, including a study that highlighted the high operating costs and specialized personnel required to analyze data collected from mobile phones. 69 Others suggested that use of resource-intensive technologies, including big data analytics and artificial intelligence, may not be feasible in resource-limited settings.44,65,144,212
Discussion
In this scoping review of the peer-reviewed and grey literature, we explored the use of digital technologies for public health surveillance during the COVID-19 pandemic. This review focused on publications from the first year of the COVID-19 pandemic to provide a snapshot of questions, concerns, discussions, and findings emerging from the academic and grey literature at that pivotal time. Overall, we identified a wide variety of digital technologies used across 90 countries and regions for various pandemic-related applications, including digital contact tracing, symptom monitoring, tracking and predicting disease spread, enforcing quarantine, and promoting physical distancing.
While publications reviewed in this sample identified many digital technologies used for pandemic surveillance, these technologies were not always clearly defined or explained. We often found it difficult to precisely determine what was meant by terms such as “big data,” what exactly these technologies were, and how they were being used for surveillance. Vague descriptions of technologies with few details of their functioning using catch-all terms such as “big data,” “AI,” or “mobile apps” complicated efforts to precisely identify technologies and their uses. There is a need to consider what is meant by the terms “digital technology” and “digital surveillance” and how to classify or define technologies for data collection, processing, and use.
We also identified themes across the literature related to the success of digital technologies in responding to the pandemic and some of the factors that might impact the efficacy and value of digital surveillance. The authors raised concerns related to the limitations of digital surveillance technologies and questions related to the overall value of using digital technologies to mitigate the COVID-19 pandemic. Also highlighted across many of the publications was the question of risks versus benefits or the trade-off between mitigating the impacts of COVID-19 and costs to individuals’ rights. As was argued in one study, 45 it is possible that framing digital surveillance as a zero-sum trade-off is a false dilemma and that, instead, public health goals can be supported by attending to questions of privacy, data security, and cultivating public trust. Given concerns raised by many authors around the limited success of digital surveillance and the risks of techno-solutionism, there is an urgent need to consider the potential costs associated with using digital technologies for surveillance when their value may be negligible. The potential and witnessed implications of digital surveillance, e.g. impacts on human rights and civil liberties, are discussed in a subsequent paper.
We found that many authors shared concerns around the surveillance of marginalized groups and the collection of valid, accurate, and generalizable data to inform public health decision-making. Several authors noted that without data on disease spread within marginalized communities, such as racialized non-white people, older adults, people living in poverty, refugees, and migrant workers, it may be difficult to implement public health measures that equitably respond to the needs of these groups during a public health crisis, particularly given that many of these groups were inordinately impacted by COVID-19 and public health measures. However, we also identified discussions of the potential risks of digital surveillance to marginalized communities, including undocumented migrants and racialized non-white people, who have historically been targets of heightened surveillance. These risks of harm may be particularly acute in the case of individual-level, highly granular, and detailed data collected as opposed to the use of aggregated and anonymized datasets. There is a pressing need to consider how accurate and valid data might be collected to effectively design public health interventions to protect vulnerable groups while also mitigating the risks associated with surveillance. Cultivating trust among groups rightfully wary of surveillance is also critical.
As the world continues to witness infectious disease outbreaks—e.g. the 2022 mpox outbreak and growing concerns around the H5N1 virus—knowledge regarding the use of digital technologies for public health surveillance will be critical. Other emerging reviews, including a scoping review of academic and non-academic literature by Francombe et al., 244 provide important insights into digital innovations used to respond to the COVID-19 pandemic. Likewise, recent studies have attended to the equitable design and use of digital surveillance technologies during the COVID-19 pandemic, 245 ethical dimensions of digital surveillance during crises, 246 and how the COVID-19 pandemic has prompted an intensification of various forms of surveillance. 247 Our study contributes to this literature through a qualitative, thematic analysis that identifies factors shaping the success of digital surveillance for public health and debates and tensions within the literature, particularly as these findings and discussions emerged in the first year of the pandemic. We also identify gaps in existing knowledge, including an urgent need to develop a shared understanding of terms such as “AI” and to more clearly define how successful use of digital technologies for public health surveillance might be understood. Addressing these gaps will be critical for informing future decision-making around digital surveillance.
Limitations
While our review produced valuable insights into the nature of digital technology used for surveillance during the COVID-19 pandemic, this study had several limitations. In focusing our scope on literature that detailed the use of digital technologies during the COVID-19 pandemic, we may have missed key developments that occurred before the pandemic and how they may have changed over time. Limiting our focus to literature published between December 1, 2019 and December 31, 2020 may also have excluded important developments in digital surveillance after this time period. Additionally, including only English-language documents may have limited our capacity to analyze the use of digital technologies through a global lens. Finally, as the COVID-19 pandemic continues and other outbreaks emerge, this publication represents an early appraisal of existing knowledge. Nonetheless, the rapid pace of technological development and research on digital surveillance highlights the urgency of reviewing this literature.
Conclusions
In this scoping review of the literature, we explored the global use of digital technologies for surveillance during the COVID-19 pandemic. Our review identified technologies used in 90 countries or regions. These technologies were used primarily by the state and its agents and most commonly targeted the general population for purposes of contact tracing and predicting and modelling disease spread. Our review also uncovered themes related to factors impacting digital surveillance, the perceived success of digital surveillance, and warnings against techno-solutionism given the paucity of evidence of successful digital technology use for combating the COVID-19 pandemic.
These findings raise important questions regarding the use of digital technologies for public health surveillance and how to balance potential benefits and harms, the infrastructure and resources needed to successfully develop and use digital technologies for surveillance, the role of digital surveillance in integrated public health responses, the factors that continue to shape the outcomes of digital surveillance, and how these questions intersect with concerns around equity and ethical use of technology for surveillance. While this scoping review is specific to the COVID-19 pandemic, the findings have implications for public health surveillance of future outbreaks, epidemics, and pandemics. As digital technologies are increasingly deployed as surveillance measures during public health crises, the concerns, limitations, and tensions raised in the literature will continue to play a pivotal role in future forms of digital health surveillance.
Footnotes
Acknowledgment
We would like to thank Meagan Stanley for her assistance in designing the search protocol for this review.
Contributorship
LD, LC, BH, JH, JJS, MJS, AK, JB, SS, TNC, JS, JG, and MN conceived and designed the study. LC and MN researched and reviewed the literature. LD, LC, BH, DF, and MN contributed to data analysis. LC, LD, and BH wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the University of Western Ontario FHS Research Grant 2020 grant number N/A
Guarantor
LD
Research ethics and patient consent
The study is a review of the literature and did not require research ethics approval or patient consent.