
Abstract
Objective
Family health can be improved by making home visits with mobile applications. This study was carried out to evaluate the effect of a mobile application and web-based software called Ebe Evimde (My Home Midwife), which was designed by the researchers for use in the postpartum period, on mothers’ self-efficacy and anxiety levels.
Methods
Home visits to 60 mothers in the intervention group, who are over 18 years of age, who have given birth at term, who have no complications in mother and baby, and who are in the second to fifth postpartum days, were made with the online home visits mobile support application Midwifery Home software and their self-efficacy and anxiety levels were evaluated. Mothers were divided into two groups as intervention (60) and control group (60) using a random number table.
Results
While there was a significant difference between the pretest and posttest self-efficacy levels of the intervention group, there was no difference between the pretest and posttest self-efficacy levels of the control group. When the groups obtained from the Postpartum Specific Anxiety Scale were examined, it was seen that there was a negative and very strong significant relationship between the pretest and posttest scores of the mothers in the intervention group, while when the relationship between the pretest and posttest scores of the mothers in the control group was examined; no significant relationship was observed.
Conclusion
The practice of Ebe Evimde (My Home Midwife) had a positive effect on mothers’ self-efficacy and postpartum anxiety levels.
Introduction
The postpartum period, which is defined by the World Health Organization (WHO) as the period up to the 42nd day following birth, is a critical period for both mothers and newborns. 1 It is also a transitional period for women and their families in which they have to adapt to their new physical, psychological and social status. 2 In most developed countries during this transition period, the postpartum hospital stay is generally less than 48 h after vaginal delivery. In Turkey, the standard hospital stay of the mother and the newborn is 24 h after normal delivery and 48 h after a Cesarean section.3,4 However, this period is too short in terms of providing education for the postpartum period, and observing any complications and psychological problems that may occur. With this in mind, home visits are crucial in terms of the early detection of, and interventions in, the difficulties of women who are not otherwise able to adequately access health services, training by midwives on how to care for themselves and their babies, and other personal care services. Home visits during the postpartum period contribute to the protection and promotion of health by providing technical, psychological and therapeutic support for the mother’s home care, education and needs. 5
With the increase in emotional sensitivity caused by giving birth, psychological problems may start or recur and anxiety disorder, which is one of the mental health problems frequently seen in the postpartum period, may develop.6,8 The term “postpartum anxiety” can include clinical psychiatric disorders, as well as general anxiety or phobias. 9 It is a mental state that causes constant and excessive worry, and is characterized by impaired concentration due to increased fears and tension.10,11
The prevalence of postpartum anxiety varies between 2% and 45% in the first postpartum year.
According to some relevant studies, mothers in the postpartum period have stated that the support systems available to them are not sufficient, and that they did not receive adequate training and counseling. In addition, they had difficulties in immediately accessing the information they need.15,16 For this reason, it is crucial to create new ways for mothers and midwives to communicate.15,17 One example of these new ways is the use of mobile applications or “apps.”
With the recent and increasingly widespread use of technology, different methods of care and monitoring have emerged in the healthcare field. 7 Postpartum mobile apps are becoming prevalent and appear to be an effective support system.17,18 In addition, the WHO recommends “promoting self-care through the use of electronic and mobile health applications” in its Mental Health Action Plan 2013–2020 (WHO, 2013). If the care and counseling provided during the postpartum period is sufficient, positive health behaviors increase, maternal stress is reduced and infant health is improved.7,19 In particular, mobile apps that provide quick and accessible individual care and counseling during the postpartum period have been recommended as an effective method for reducing postpartum anxiety. 20
Although mobile health applications have been developed for the postpartum period none of these apps appears to be specifically focused on home visits and postpartum anxiety.18,21,22 In addition, there is a need for innovative tools with a better quality of information and evidence base.23,24 Hence, studies in this area need to be repeated.25,26 When the literature was examined, no study was found evaluating the effect of a mobile support application on mothers’ anxiety symptoms in the postpartum period with a specific focus on home visits.
This study thus aimed to evaluate the effect of a mobile application and web-based software called Ebe Evimde,, which was designed by the researchers for use in the postpartum period, on mothers’ self-efficacy and anxiety levels.
Method
Study design
The study was designed as a randomized, controlled trial study.
The design of Ebe Evimde
The frequency of the follow-ups determined by the Ministry of Health of the Republic of Turkey regarding the postpartum period home visits includes three home visits: initially, between the 2nd and the 5th day following the birth, then between the 13th and the 17th day, and then between the 30th and the 42nd day. 3 These home visits should take approximately 1–1.5 h. During this process, the midwife should be able to have a holistic discussion in the comfort of the family home in order to diagnose and identify problems and make any necessary plans, and she should also be able to easily access previous home visit data when needed. With Ebe Evimde, “home visits” can be easily conducted online by midwives via mobile devices or web-based applications. In addition, individuals can search for any queries they have after their online home visits through the “Frequently Asked Questions” tab. The midwife can also be reached 24/7 via the “Ask for Support” button when needed. According to some observers, the implementation of home visits is becoming increasingly difficult due to safety concerns, midwives’ workload, difficulties in finding addresses, weather conditions and the period of the pandemic.2,18 The use of the Ebe Evimde application for online home visits saves time, as well as cutting the costs associated with transportation, administration and storage of written records. On the integration of digital technologies into the postnatal process, the My Home Midwife application can be used to affect mothers’ self-efficacy and anxiety levels.
Financial support and pilot study
An application was made to the Scientific Research Projects Coordinator of the university where the research was conducted for financial support for the design of Ebe Evimde. After the project was approved, the researchers collaborated with a software company to create the Ebe Evimde app and the necessary infrastructure was completed. The app was intended to be used as a system that provides mutual interaction between midwives, mothers and their families. Therefore, based on the hypotheses of the study, a pilot study was conducted with 10 mothers to evaluate the effectiveness of the app. During this process, online home visits were conducted by the researcher using the app. After the final checks, the necessary revisions were made, and the design was finalized. (The Ebe Evimde app can be accessed at https://www.ebeevimde.com.)
How the system works
Mothers first log in to the system as users, and then their user data is uploaded. This data is then transferred to an “administration panel” designed for the researchers. The user and the midwife subsequently schedule and have an online home visit at an appropriate time. Before the end of the 42nd day, the mothers have their final follow-up online home visit.
An example scenario is presented below (Figure 1)
The researcher fills out the data collection form regarding the intervention group and demonstrates the system to the individual. The data collection form filled out by the users is transferred to the server and saved in the system. The user and the researcher schedule and conduct online home visits as appropriate. In addition to the online home visits, mothers can find reliable and accurate answers by searching for the subjects they are interested in using the “Frequently Asked Questions” tab in the app. If they need to, they can reach the researcher 24/7 using the “Ask For Support” button and request a meeting. All user-related data are kept in Ebe Evimde's database.

System scenario.
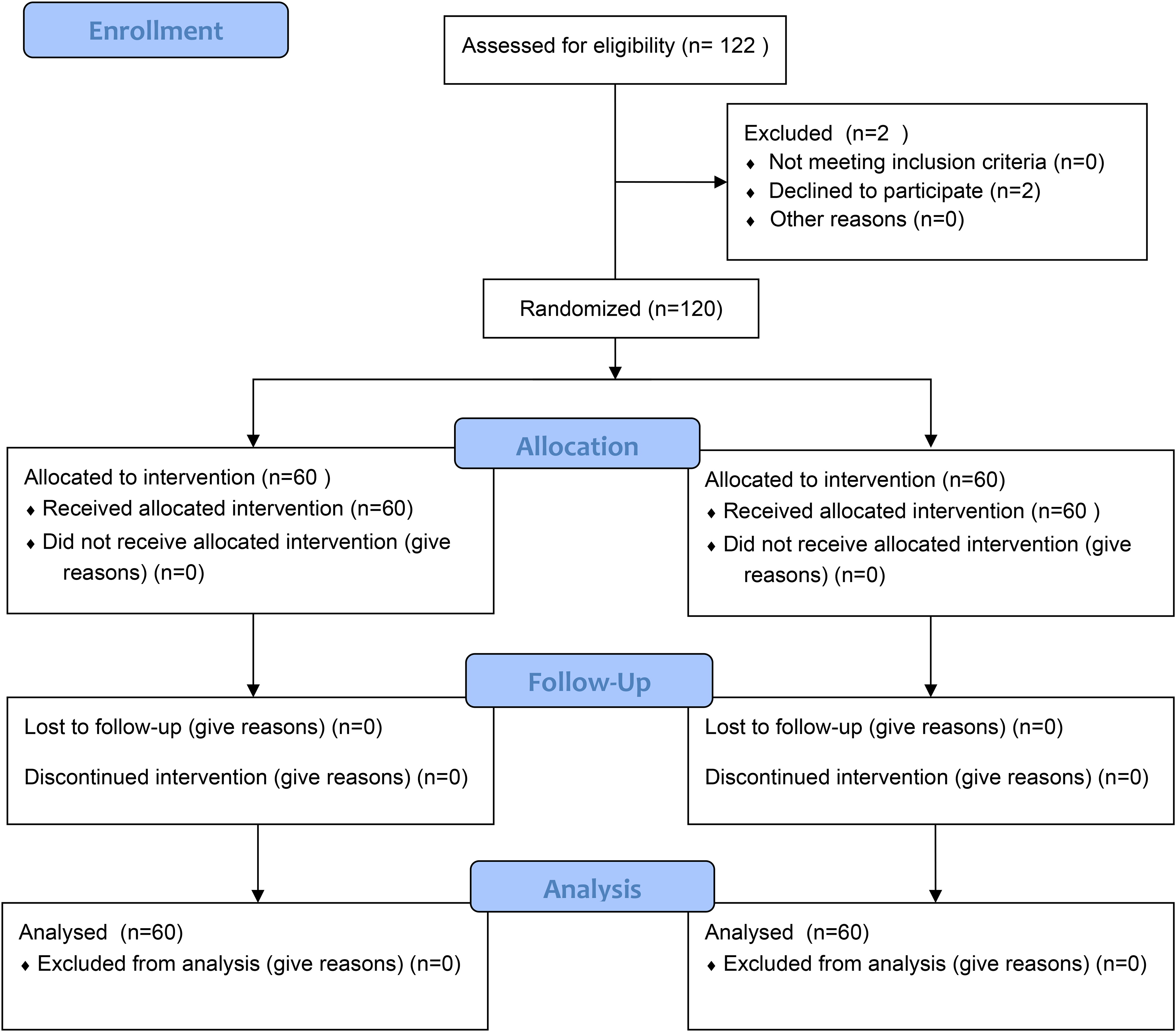
The Consort diagram.
Data collection tools
The Sociodemographic and Obstetric Characteristics Information Form, the Mother's Self-Efficacy Form and the Postpartum Specific Anxiety Scale (PSAS) were used to collect data.
The Sociodemographic and Obstetric Characteristics Information Form was created by the researcher following a review of the relevant literature. It was administered to women who met the criteria in the early postpartum period (6 h after normal delivery, 12 h after Cesarean section). The form consists of 30 questions in total, including 11 questions about sociodemographic characteristics (age, educational status, employment status, monthly income, family type, presence of social support, relationship status with the spouse, readiness for the postpartum period, feeling safe as a mother, level of coping with difficulties) and 19 questions regarding the characteristics of the pregnancy and birth (whether the pregnancy was planned or not, the type of birth, which pregnancy it was, the baby's gender and birth weight, when the baby was breast-fed, the state of being stressed before the birth and whether the birth itself had created stress).
The Mother's Self-Efficacy Form was created by the researcher and administered to women who met the criteria in the early postpartum period (6 h after normal delivery, 12 h after Cesarean section). The form consists of a total of 23 questions, which evaluate the mother's self-efficacy about the activities and issues in the postpartum period (bleeding, nutrition, defecation, urination, exercise, sleep and rest, canker sore, diaper rash, jaundice, navel care, eye care, massage, kangaroo care, sucking positions, breastfeeding techniques, signs of infection, dangerous situations). The information compiled for the form was sent to academics who were experts in their fields and midwives working in the hospital for their opinions. The experts were asked to rate each topic and report their recommendations, if any. To test content validity, each item was scored as “appropriate” (3 points), “appropriate but should be adjusted” (2 points) and “inappropriate” (1 point). Opinions from at least three experts are required to ensure content validity. 27 The content validity index developed by Waltz and Bausel (1981) was calculated with the scores obtained after the expert opinions, and the validity of the content was tested. For a scale to have sufficient content validity, its CVI must be above 0.80. 27 In this case, the CVI value of the Mother's Self-Efficacy Form was calculated to be 1, which was sufficient.
The PSAS was developed by Fallon et al. to evaluate anxiety symptoms particular to the postpartum period. 13 It consists of 51 items and has four sub-dimensions. These sub-dimensions are Maternal Competence and Attachment Anxieties (items 1–15), Infant Safety and Welfare Anxieties (items 16–26), Practical Infant Care Anxieties (items 27–33) and Psychosocial Adjustment to Motherhood (items 34–51). The scale was adapted into Turkish by Duran in 2019, and the Cronbach alpha coefficient was found to be r = 0.91. When the items were analyzed as a four-factor structure, as in the original scale, it was observed that they were grouped under different subscales. Since many items of the scale (items 1–3, 1–16, 18 and 19) had shifted to a different group, it was decided that the Turkish version of the scale should be one-dimensional. When the factor loads in each factor were examined, it was determined that the factor loads of the 1st, 2nd, 15th and 46th (English) items were below 0.30. For this reason, these four items were not included in the Turkish form and were removed from the scale. In other words, the Turkish version of the scale was thus created as one-dimensional and with 47 items. The lowest score that can be obtained from the scale is 47 and the highest score is 188. Those who score 73 and below on the scale have low postpartum anxiety levels, a score between 74 and 100 indicates a medium level, while those who score 101 and above have a high level of postpartum anxiety (APPX.III). Lastly, the pretest and posttest Cronbach alpha values of the scale were found to be 0.96 and 0.99, respectively. 28
Data collection and randomization
Pre-intervention
The data were collected between October 2021 and February 2022. In addition, the pretest data were collected from mothers on the hypothesis that mothers’ anxiety levels would decrease and their self-efficacy levels would increase at the end of the 42nd postpartum day after using the Ebe Evimde app. Mothers who had a full-term (according to the ACOG 2013 definition of between 39 weeks 0 days and 40 weeks 6 days of pregnancy 29 ) birth at the Gynecology and Children's Hospital of the University where the study was conducted, who had a single, healthy newborn and who did not develop any postpartum complications, constituted the intervention and control group of the study.
G-Power 3.1 package program was used to calculate the sample size. The sample size was determined by Power analysis in line with the two-way p-value. In the study, the effect size was calculated as 0.6691891 with a power of 0.9530667 and a significance level of 0.05, and the sample size was calculated as 120 mothers, 60 intervention and 60 control. Using a random numbers table, 60 mothers selected by simple random sampling method formed the control group and 60 mothers formed the intervention group. Mothers were divided into two groups as intervention and control group using a random number table.
Intervention Group Inclusion Criteria:
18 years of age or older and had a vaginal or cesarean section at term Has a phone and internet connection with Android or IOS Baby with a normal birth weight and an APGAR score of 8 or higher No postpartum complications Speaks and understands Turkish Primiparous and multiparous Is 2–5 days postpartum Be illiterate Presence of any complications in the mother or newborn at the end of labor (the newborn being in intensive care) Presence of anomalies in the newborn Presence of chronic disease in the mother Presence of a disability in the mother (physical, mental, visual, hearing, etc.) Presence of multiple babies Being diagnosed with anxiety and depression Having undergone a high-risk pregnancy (gestational hypertension, gestational diabetes)
Intervention Group Exclusion Criteria:
Intervention
Postpartum online home visits mobile support application was installed on the phones of the mothers in the control and intervention groups who agreed to participate in the study. Sociodemographic and Obstetric Characteristics Information Form, Maternal Self-Efficacy Form, PSAS were collected through the mobile application. Three online home visits were made to the intervention group within the first 42 days. Between the 30th and 42nd days, after the last online home visit to the mothers in the intervention group, the Mother's Self-Efficacy Form and PSAS scores were re-measured via the mobile app during a video call with the mothers. The control group continued to receive only routine health care.
Post-intervention
The questions were read out by the researcher and the mothers answered the questions. In the same time period, the mothers in the control group were also video-called, and their scores for the Mother's Self-Efficacy Form and PSAS were re-measured. On the 42nd day of the mothers in the control group, Maternal Self-Efficacy Form and PSAS scores were measured again through the mobile application. After the posttest was taken from the mothers in the control group, the mobile health application was made available to the mothers for one month.
The consort diagram is given in Figure 2.
Statistical analysis
The study data were transferred to the computer, and statistical analysis was conducted using the SPSS 23 (Statistical Package for Social Science) statistics software. The data evaluation used descriptive statistics (frequency, percentage, mean, standard deviation, min-max values) in dependent and independent groups, two-way ANOVA, the t-test in independent and dependent groups, chi-square analysis and correlation analysis.
Ethical approval
Each stage of the study was carried out following ethical principles. Before the application, permission was obtained from the Ethics Committee and the Sivas Cumhuriyet University Health Services Research and Application Hospital. The participants were informed that the data would only be used within the scope of the study, that they did not have to provide their names, and that confidentiality would be ensured. Only women who agreed to sign the informed consent form were included in the study. The form was read out in front of the participants, and their written consent were obtained. In addition, the study complied with the ethical principles in the Declaration of Helsinki.
Results
Table 1 presents a comparison of the descriptive characteristics of mothers in both groups. The mean age of the mothers in the intervention group was 30.03 ± 4.05 years. About 43.3% of them were high school graduates, 63.3% were unemployed, 90% had a moderate monthly income, 96.7% lived in a nuclear family, 51.7% received social support from people around them during their postpartum period, 76.7% of them had moderately good relations with their spouses, 53.3% of them did not feel ready for the postpartum period, 55% felt self-confident in the postpartum period, 91.7% evaluated their ability to cope with difficulties as moderate and 15% were regular smoker. On the other hand, the mean age of the mothers in the control group was 30.83 ± 3.91 years. About 45% of these women were high school graduates, 60% were unemployed, 85% had a moderate monthly income, 85% lived in a nuclear family, 63.3% received social support from people around them during their postpartum period, 75% of them had moderately good relations with their spouses, 56.7% did not feel ready for the postpartum period, 51.7% felt self-confident in the postpartum period, 93.3% evaluated their ability to cope with difficulties as moderate and 15% were regular smokers.
Characteristics of participants.

*p-values are considered significant less than 0.05.
Table 2 presents a comparison of pregnancy and delivery characteristics of mothers in both groups. 61.7% had a normal delivery, 66.7% evaluated their delivery as moderately good, 41.7% did not have a previous history of pregnancy, 43.3% did not have any living children other than the baby, 80% had a male baby, 53.3% of them had children with a birth weight of 3000–3499 g, and the average birth weight of their baby was 3.421 ± 153.0 g, 58.5% of them breastfed their baby in the first 30 min to an hour after birth, 75% of them had not experienced any stressful events in the process until labor, 86.7% of them had not had any upsetting family problems recently, 61.7% of them had children between 0 and two years of age and there was an average gap of 1.91 ± 1.95 (0–6) years between their youngest child and their baby, 78.3% received midwifery education, while 68% of those trained received nutrition education and 64.6% received breastfeeding education.
Pregnancy and delivery characteristics of participants.

**More than one option is marked.
In contrast, of the mothers in the control group, 55% had a normal delivery, 66.7% evaluated their delivery as moderately good, 43.3% had no previous history of pregnancy, 43.4% had no children other than their babies, 58.3% had a male baby, 61.7% of them had children with a birth weight of 3500 g and above and the average birth weight of their baby was 3.491 ± 224.97 g (3.100–42.00 g), 55% breastfeed their baby in the first 30 min to 1 h after birth, 80% did not experience stressful events until labor, 93.3% did not have any recent problems in the family, 55.9% of them had children between 0 and two years of age and there was an average gap of 2.43 ± 2.91 (0–12) years between their youngest child and their baby, 66.7% of them received training from midwives, while 59.5% of those who received training received nutrition and 54.4% breastfeeding training. There was a significant difference between the mothers in both groups in terms of family type and baby's gender (p < 0.05). However, there was no significant difference in variables such as age, educational status, monthly income, type of birth, postpartum period characteristics, characteristics of the baby and educational status in the postpartum period (p > 0.05; Table 1 and 2).
The distribution of the pretest and posttest scores of the mothers from the Mother's Self-Efficacy Form is given in Table 3. There was a significant difference between the pretest and posttest self-efficacy levels of the intervention and control groups.
Comparison of pretest and posttest mother self-efficacy of postpartum mothers in experimental and control groups.

The lowest and highest scores obtainable from the PSAS are 47 and 188. The mothers in the intervention group scored 147.18 ± 14.66 in the pretest and 59.50 ± 12.64 in the posttest. The mothers in the control group scored 156.88 ± 17.19 in the pretest and 118.21 ± 27.28 in the posttest. The intra- and intergroup comparisons of the PSAS of the mothers are presented in Table 4. When the scores for the PSAS were examined, it was found that the PSAS pretest mean score of the postpartum mothers in the experimental group was slightly lower than that of the postpartum mothers in the control group, and there was a significant difference between the groups in terms of the PSAS pretest mean scores of the postpartum mothers in the experimental and control groups (p < 0.05).
PSAS pretest and posttest mean comparison of mothers in experimental and control groups.

It was found that the PSAS posttest mean score of the postpartum mothers in the experimental group decreased more with the effect of the postpartum mobile support application compared to the postpartum mothers in the control group, and there was a significant difference between the groups in terms of the PSAS posttest mean scores of the postpartum mothers in the experimental and control groups (p < 0.05; Table 4), there was a negative and very strongly significant relationship between the pretest and posttest scores of the mothers in the intervention group (r = −0.878, p = 0.001; Table 5). This finding indicated that the postpartum mobile support application applied to postpartum mothers in the intervention group significantly reduced the level of anxiety.
The relationship between PSAS pretest and posttest scores of postpartum mothers in the experimental and control groups.

Pearson correlation analysis applied, *p < 0.05.
Discussion
The results of this study, which was conducted to examine the effect of the Ebe Evimde app used for online home visits of mothers in the postpartum period on mothers’ self-efficacy and anxiety levels, were evaluated in reference to the relevant literature. In addition, the intervention group was assessed by organizing online home visits at regular intervals until the 42nd day after birth via the app. The women in the intervention group benefited from the content prepared for the postpartum period, being able to use the “Frequently Asked Questions” tab whenever they wanted, and they could get help from the researcher with the “Ask For Support” button (14 mothers used this button). The topics they sought support about were breastfeeding, danger signs and general care of the baby. All the mothers in our study decided to breastfeed, yet some difficulties were encountered in breastfeeding during the first 42 days. The topics regarding breastfeeding included problems caused by bad advice from relatives and friends and having too much information given all at once. Providing access to adequate health information during the postpartum period can reduce maternal stress and improve infant health.2,17 Although most of the women who requested support in the study were given discharge training, they were not able to learn all the information as there was too much of it—an “information overload”—as well as due to issues such as the mother's degree of pain and the effectiveness of the support systems. The problems that mothers in our study sought support for in breastfeeding were as follows: “My mother-in-law says that my milk is low, how can I find out?,” “Should I use a bottle and a pacifier?,” “How can I tell if my baby is hungry?,” “How do I know if my baby is breastfeeding incorrectly?,” “I have difficulty while breastfeeding, what should I do?,” “Why should I only give breast milk to my baby?,” “Should I take special care of my breasts?,” “My nipples are sore, is there any method to treat this other than medication?” and “I was given vitamin D, can I breastfeed while using it?” In general, studies have reported that providing mothers with appropriate information about breast milk and breastfeeding affects breastfeeding behavior and reduces anxiety levels7,15,22,30,31 The problems that mothers sought support for in the “Danger Signs” topic were as follows: “I was told that my bleeding should decrease gradually, but I changed more pads compared to yesterday. Why?,” “My baby did not defecate today, is that normal?” and “My baby is not breastfeeding and I’m afraid they will starve, should I give them formula?” In addition, the problems for which support was requested related to general care of baby care were as follows: “Should I use alcohol while taking care of my baby's belly button?,” “My baby has small pimples on his skin. Why?,” “My baby's poop overflowed all the way up to his waist, what is the problem?,” “Is it normal for my baby to have swollen breasts?,” “I’m going to give my baby a bath, is there something I should do to the belly button after the bath?” Mothers have increasingly been using the internet to find information about infant care, and may sometimes access unreliable information. 32 In this study, the use of the “Ask For Support” button ensured that the mothers could reach the health professional whenever they wanted and receive reliable information when they needed it. According to our observations, the intervention group in our study preferred to receive answers to their questions directly from the researcher with the “Ask For Support” button, rather than reading the information in the app. In another study, it was emphasized that parents should be able to ask questions when problems arise, get help when necessary, know that they can get support 24 h a day and improve their sense of self-efficacy, and that follow-up should continue in the postpartum period. 15 Yet, it was observed that the intervention group in our study preferred to receive answers to their questions directly from the researcher with the “Ask For Support” button instead of reading the information. Again, the mothers could not find the time to read the “Frequently Asked Questions” content we prepared due to changes they experienced in the postpartum period, including fatigue, insomnia, anxiety levels, etc. With this app, we gave mothers the opportunity to get the exact information from a reliable source when needed. Accordingly, there was a significant difference between the groups in terms of self-efficacy after using the postpartum mobile support application (p < 0.05). In our study, the mothers in the intervention and control groups increased their self-efficacy after postpartum via the mobile support application, similar to the study of Shorey et al., where they found that mobile health apps improved parental self-efficacy. 18 In another similar study, it was reported that the self-efficacy of the parents increased thanks to information they received over a period of time.15,17 Correspondingly, the individuals increased their self-efficacy as a result of the helpful content found in the app, similar to Shorey et al.'s study, where individuals’ self-efficacy increased when answers were received from a healthcare professional and their concerns were met. 18 The current study also shows that the mobile support app had a significant effect in reducing the anxiety levels of mothers in the intervention group. As a result of these findings, the hypothesis that the “Postpartum Online Home Visit Mobile Support Application has an effect on the anxiety level of postpartum mothers” was accepted. In addition, postpartum anxiety is the most common mental problem in mothers during pregnancy and the postpartum period.6,8 While postpartum anxiety can lead to distress and anxious moods, it can also lead to failure to establish a healthy bond between mother and baby, and low self-efficacy.33,35 As stated in various studies, postpartum anxiety is seen in between 12 and 20% of mothers at a clinical level.28,36,38 According to the results of the study conducted by Bingöl et al., mothers in the at-risk group should be assessed for anxiety during the postpartum period. 39 For this reason, it is crucial to evaluate the anxiety status of mothers in the postpartum period. One of the results of a systematic review examining the effectiveness of mobile health apps for improving antenatal and postnatal care in low and middle-income countries was that mobile applications for the postpartum process could be improved. 40 Moreover, the self-care and self-respect of mothers using mobile applications improves and their anxiety levels decrease when they use apps developed specifically for the postpartum period15,22,30,31,41 On this topic, Ashford et al. found that the anxiety levels of mothers who used and did not use mobile applications decreased after an 8-week evaluation. 42 Similarly, in another study, it was stated that the frequency of postpartum anxiety decreased from 18% to 15%. 12 In conclusion, the results of this study are compatible with the literature.
Conclusion
The Ebe Evimde system, designed to be used for online home visits, contributed to the effective and efficient management of these visits. With regard to the hypotheses, it was found that Ebe Evimde increased mothers’ self-efficacy levels and reduced the effect of postpartum-specific anxiety levels. In addition, the Ebe Evimde app can be used by midwives working in rural locations and family health centers. It is believed that the app will make a significant contribution to the development of public health in the long term. By using Ebe Evimde, families can receive their services comfortably and efficiently from midwives during online home visits.
Limitations of the study
The results of this study cannot be generalized because it was only conducted with mothers who gave birth in the obstetrics and delivery room of a Maternity and Children's Hospital in one city in the Central Anatolian Region of Turkey. In addition, the small number of mothers in the sample is an important limitation. There is a need to develop online home visit applications and multi-center studies and engage in more comprehensive research.
Footnotes
Acknowledgments
We would like to thank the mothers who agreed to participate in the study, the software company that provided services to the study, and the Scientific Research Projects Coordinatorship of Sivas Cumhuriyet University for their financial support. This study is the master's thesis of the first author, conducted under the supervision of the second author. This study was presented as an oral presentation at the 2nd International Congress of Medicine, Health and Communication Sciences held as a hybrid in Turkey on October 5–8, 2022 and received the first prize for oral presentation.
Contributorship
Merve Ayşe Bozkurt—Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Validation; Visualization; Roles/Writing—original draft; Writing—review and editing. Büşra Cesur—Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Roles/Writing—original draft; Writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approved by the Sivas Cumhuriyet University Ethics Committee (ethical decision no: 2020-11/29) and the Sivas Cumhuriyet University Health Services Research and Application Hospital (05.03.2021-19980).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the design of Ebe Evimde (Project No: SBF-2021-086) was provided by the Scientific Research Projects Coordinatorship of Sivas Cumhuriyet University
Guarantor
MAB