
Abstract
Mobile health applications (mHealth apps) may be able to support people living with chronic obstructive pulmonary disease (COPD) to develop the appropriate skills and routines for adequate self-management. Given the wide variety of publicly available mHealth apps, it is important to be aware of their characteristics to optimize their use and mitigate potential harms.
Objective
To report the characteristics and features of publicly available apps for COPD self-management.
Methods
MHealth apps designed for patients’ COPD self-management were searched in the Google Play and Apple app stores. Two reviewers trialed and assessed the eligible apps using the MHealth Index and Navigation Database framework to describe the characteristics, qualities, and features of mHealth apps across five domains.
Results
From the Google Play and Apple stores, thirteen apps were identified and eligible for further evaluation. All thirteen apps were available for Android devices, but only seven were available for Apple devices. Most apps were developed by for-profit organizations (8/13), non-profit organizations (2/13), and unknown developers (3/13). Many apps had privacy policies (9/13), but only three apps described their security systems and two mentioned compliance with local health information and data usage laws. Education was the common app feature; additional features were medication reminders, symptom tracking, journaling, and action planning. None provided clinical evidence to support their use.
Conclusions
Publicly available COPD apps vary in their designs, features, and overall quality. These apps lack evidence to support their clinical use and cannot be recommended at this time.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of disability, morbidity, and mortality,1,2 negatively impacting people's overall quality of life and well-being.3,4 In 2019, it was estimated that 391.9 million people aged 30−79 years had COPD worldwide, an increase from the reported estimate of 299.4 million in 2017. 5 Although many treatment options are available, the burden of living with COPD is an ongoing challenge, especially in middle to lower class income countries. 6 Individuals with COPD are challenged to live with a progressive condition, have needs beyond pharmacologic therapy, 7 and would likely benefit from ongoing self-management. 4 With greater attention towards addressing patients’ needs, clinicians can employ strategies and provide resources that will empower patients to improve their self-management.4,8
The coronavirus-19 (COVID-19) pandemic presented many challenges to people with COPD including social isolation, decreased physical activity, and increased anxiety.9,10 Not only do they have an increased risk for poor clinical outcomes if infected with COVID-19,11,12 but to mitigate the risk and spread of COVID-19, many of the components of their care became unavailable. Health organizations have endorsed and supported the use of virtual care for COPD to offset accessibility and capacity issues when in-person options were not possible, especially in rural communities.13–17 As a result, there has been rapid adoption of virtual options such as telehealth, a generic term referring to healthcare services delivered digitally and remotely in various formats.18,19 Telehealth interventions are used with increasing frequency to assist with the management of chronic conditions such as mental health, cardiovascular disease, stroke, and diabetes. 19 However, their adoption into COPD care is limited, but continues to grow, especially since the COVID-19 pandemic.15–17 One potential and attractive solution is mobile health applications (mHealth apps), mobile computerized portal available on mobile devices. 20
There are several studies and systematic reviews demonstrating modest benefits of using mHealth apps to facilitate COPD self-management, including improved COPD knowledge and self-care,21,22 reduced hospital admissions, 20 and increased physical activity. 23 Patients from these trials expressed their interest in continuing to use the applications to support their COPD care.8,22,24–26 However, these reports were from the use of COPD apps designed and trialed by researchers and clinicians,21,23,25,27,28 with many not available to the public, 29 and may not be applicable to freely available COPD apps. Features available in public COPD apps vary, with the most common for general education, symptom tracking, reminders or diary keeping. 30 These public COPD apps are easily accessible to those seeking resources to help manage their COPD, but the absence of agreed standards or quality control may allow incorrect information, wide content variation, or inappropriate feedback: all of which are safety concerns that could endanger users’ health.29,31 The rapid growth and continuous changes in the app marketplace have led to the development of tools to assess the quality and effectiveness of mHealth apps.32,33
Many app evaluation tools are available to ensure mHealth apps are verified for their safety, usability, and clinical relevance. 32 In contrast, technical considerations (i.e., last update, privacy, and security qualities) are less likely to be assessed for. 34 However, an actionable evaluation tool called the mHealth Index and Navigation Database (MIND) framework was developed by Lagan et al. 33 to comprehensively assess mHealth apps on their designs and features across multiple domains. The MIND framework was derived from 79 existing app evaluation frameworks, and has excellent interrater reliability (kappa ≥0.75). 32 There are 107 objective questions in the MIND framework, 32 categorized into five assessment domains: 1) Background and access; 2) Data safety and privacy; 3) App effectiveness and clinical foundation; 4) User experience and engagement; 5) Data integration towards therapeutic alliance. The ultimate goal of the MIND framework is to compile mHealth app evaluations onto an open database for mental health apps by the Beth Israel Deaconess Medical Center, Harvard University.32,33 Mental health apps logged in the database have their MIND assessments publicly available, detailing the apps’ characteristics, features, supporting clinical evidence, or endorsement for use. 35 However, the MIND framework can be used and applied into mHealth apps for other chronic diseases and conditions. 32 Therefore, there is an opportunity to evaluate the quality of publicly available COPD self-management apps to provide guidance to health care professionals to determine the apps’ most appropriate use. 33
Objective
The primary objective of this evaluation study was to report the features and characteristics of publicly available apps for COPD self-management using a comprehensive app evaluation framework.
Methods
We systematically searched for COPD self-management apps in both Apple and Google Play (Android) app stores. These two app stores were chosen as they have the biggest collections of apps, with over two and three million apps available for download in Apple and Google Play, respectively. Eligible apps were assessed using the mHealth Index and Navigation Database (MIND) framework (described in detail below). 32
Search strategy
The research team, comprised of healthcare researchers and professionals with expertise in COPD, determined the key search terms. The keywords used for the searches were: COPD, chronic obstructive pulmonary disease, chronic bronchitis, emphysema. The keywords were kept broad for the purposes of ensuring that any COPD-directed app was found for screening. The two app stores were searched on December 2021 and search results were updated regularly (search results re-checked every 1–2 months) until August 2022. All searches were performed in Toronto, Canada.
Inclusion and exclusion criteria
Apps were included if they incorporated features aimed at facilitating self-management for people with COPD i.e., activities for self-help or to support patients’ understanding and skills in managing health. 36 In addition, mHealth had to be patient-facing, available in English, and free to download. Only free to download apps were included as the aim was to evaluate easily accessible apps, as associated cost with mHealth use is a reported barrier to their adoption.26,37 Apps were excluded if they were designed primarily for healthcare providers rather than public use. Additional exclusions included app restriction by countries or regions, technical issues (unable to download after two attempts by both reviewers), non-COPD related apps (i.e., for other health conditions), and apps that were non-health or wellness related. Non-COPD-related apps were defined as apps that did not provide exclusive self-management features or education for people living with COPD. Apps that were designed to target users with any lung condition, not explicit to COPD, were excluded, as the aim was to assess apps that were clearly designed for people living with COPD.
Screening and app selection
Results for each search term in both app stores were recorded. Microsoft Excel was used to organize and track the search results and screening process. Duplicate apps were removed prior to screening by the two independent reviewers (SQ and AB). Each app was screened against the inclusion criteria by the two reviewers independently, using the app stores’ descriptions and screenshots to determine the app's suitability for further assessment. Apps were labeled for inclusion or exclusion, with a reason provided for exclusion. Discrepancies in the app's eligibility or exclusion reasons were discussed and agreement was reached.
App evaluation
Apps that met the inclusion criteria after reviewers’ deliberation were downloaded onto cell phones (Google Pixel 3, Android version 12 and iPhone, iOS version 16). Reviewers independently evaluated content and features using the extraction data sheet guided by the components outlined in the MIND framework. After individual assessments, results were compared, and discrepancies were resolved by discussion.
Mhealth Index and navigation database (MIND) evaluation framework
Although the formulation of the MIND framework stemmed from the need to verify the quality and features of mental health apps for clinical use, this evaluation tool could be used for apps in other health fields.32,38 Clarification for each MIND question was previously published by Lagan et al. 32 and these descriptions were used to facilitate reviewers’ data extraction.
Several questions in the MIND framework required evaluators to retrieve information externally from the app platforms. Questions under the App origin, characteristics, and accessibility asked for the app's size, operating system, ratings, release date, last update, and ratings, information available on the app's download page of the app marketplace. Another question requiring external resources to answer was related to Privacy and Security. The readability of the apps’ privacy policies was calculated using an online readability calculator.32,39,40 The recommended readability test outlined in the MIND framework is the Flesch–Kincaid grade level (FKGL), a commonly used scale by healthcare professionals to identify reading level appropriate resources for patients.32,41 The FKGL determines text readability using the average sentence length and word length and the derived score provides an estimated grade level matching the U.S. education grade level. 42 For example an FKGL score of 8.0–8.9 means the text is readable to people who completed grade 8.41,42
Data extraction and assessment
For each question, responses were recorded as 0 for no; 1 for yes; 2 for unsure or unknown; 3 for not applicable. Since the MIND framework does not provide a final rating score, a rating scale was utilized by the reviewers to grade the apps’ potential in clinical use. However, user ratings from either the Apple or Google Play stores were extracted as part of the MIND framework assessment. In addition, reviewers provided each app a score to demonstrate their endorsement or lack of, using a 5-point Likert scale. This rating scale was developed by Camacho et al., as part of their mHealth app assessment and implementation framework, for raters to grade apps for their potential clinical use. 38 The scores ranged from 1 – “I would not recommend this app to anyone” to 5 – “I would recommend this app to everyone.” 38 Means and their respective ranges were calculated and total app counts and percentages were reported for each question.
Results
Search results
A total of 1316 apps from the Google Play Store and 152 apps from the Apple App Store were found using the different search terms at two different time points. After 491 duplicates were removed, 977 were screened by the two reviewers. Using the apps’ descriptions and screenshots to determine eligibility, 964 apps were excluded. A total of 13 apps were eligible and downloaded for further assessment. Five of the apps required sign-up with an email address to gain access to the information and features; a mutual email address was used to create a shared account for reviewers to access these specific apps. However, one app became unavailable during the data collection phase and only one reviewer assessed the app (myCOPD Assistant by Revitality LLC). The process of searching and including apps for assessment is illustrated in Figure 1.

Flow diagram of the app search and selection at each stage. * Apps that were not targeted towards people living with COPD (i.e., for other diseases or conditions); ‡These apps were identified in the initial search in December 2021 but were no longer available on the Google Play or App store in August 2022 for screening.
App origin, characteristics and accessibility
The summary of the app origins and accessibility characteristics is described in Tables 1 and 2. Of the 13 identified apps, seven were available from the Google Play Store only and the remaining six were available on both app stores. The minimum operating system required for each of the apps differed: the minimum Apple iOS noted is 9.0 and for Android, 4.0.3. Apps were released on the Google Play and Apple stores from as early as 2013, up to 2020. Only two apps were updated within the last 6 months (as of June 2022) and the remainder (11/13) were last updated from half-a-year up to 5 years ago. Although included apps were free to download, two apps had one-time, in-app purchases to access certain functions or information.
Highlight of non-content and common content features of the assessed apps.

✓- Yes; Blank – no; NA – not applicable; UA - unavailable
†Self-management criterion was satisfied if it fulfills the definition outlined by Lagan et al., 2020 30
‡Reference tool defined as an app that only provides education and references (defined in the supplementary materials by Lagan et al., 2020 30 )
※Apps unavailable on either app stores as of January 2023 (weblinks no longer accessible, unless otherwise indicated)
A total of 13 apps were assessed, of which six were unavailable on Apple store.
Details of the apps’ origin and functionality, including their date of release and updates.
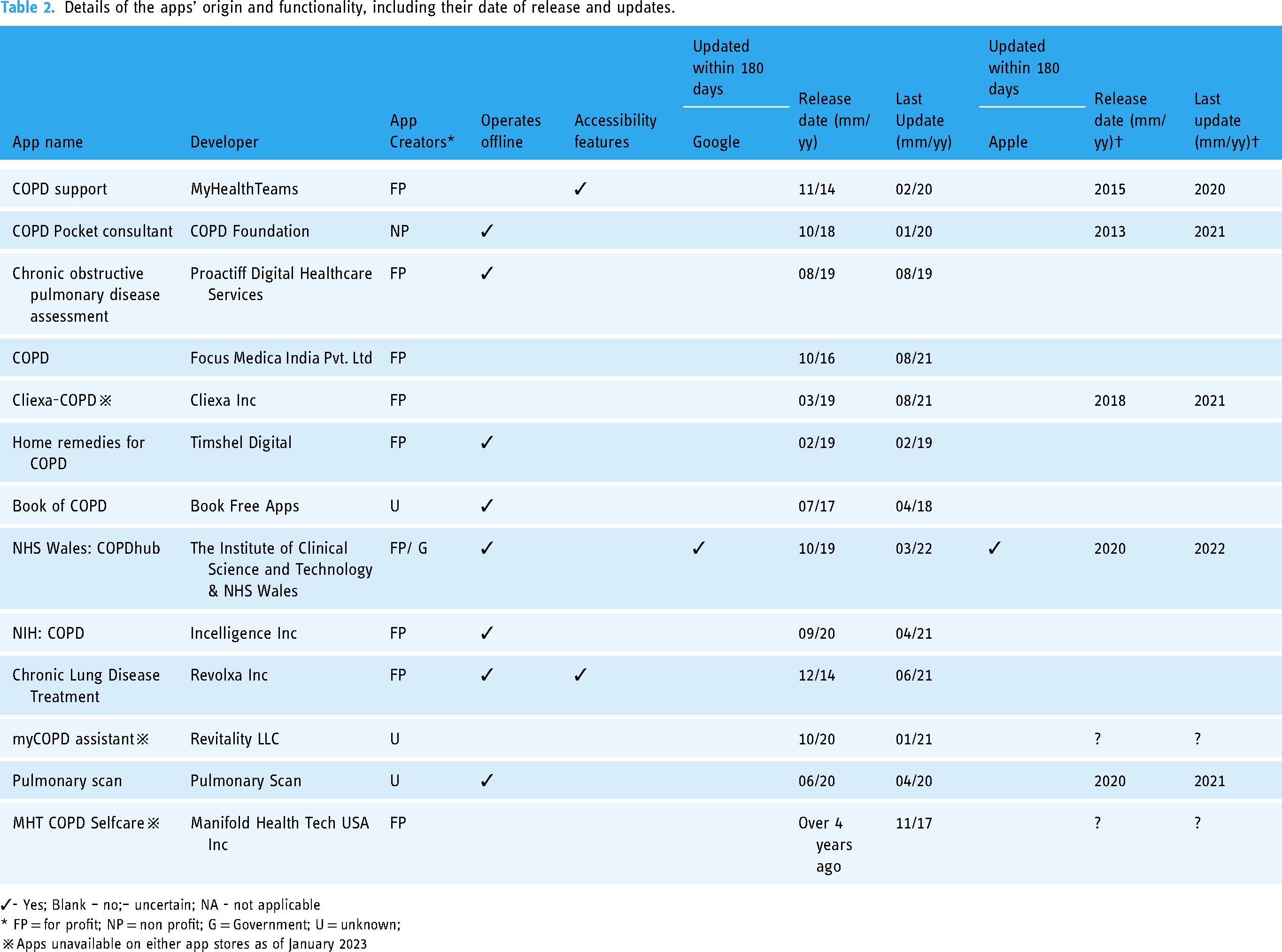
✓- Yes; Blank – no;– uncertain; NA - not applicable
* FP = for profit; NP = non profit; G = Government; U = unknown;
※Apps unavailable on either app stores as of January 2023
Apps were developed by for-profit organizations (8/13), non-profit organization (1/13), or were of unknown origin (3/13). One app was collaboratively designed by a government agency with a for-profit organization. Many apps could function online and offline (8/13), where features and data entry did not rely on internet connection to operate. Two apps incorporated accessibility features, allowing for text size adjustments, voice-to-text within the app or provided instructions to modify their phone settings.
Privacy and security, and data interoperability
Privacy, security and data interoperability characteristics and qualities are summarized in Table 3. Nine out of the 13 apps had privacy policies available on the developers’ website or within the app store's description. Apps’ privacy policies had FKGL scores ranging from 10 to 17, with a mean of 13.8, illustrating the high reading level required to understand the privacy policy.
Details on the apps’ privacy and security; and data interoperability and integration.

✓- Yes; Blank – no;– unable to verify; NA - not applicable
EMR = electronic medical record; PHI = personal health information
* Collection of data pertaining to the user's personal characteristics and contact information
†A feature that refers to the apps’ ability to provide users with help, i.e., hotline phone number, if the user's data is concerning, defined by Lagan et al., 2020. 30
※Apps unavailable on either app stores as of January 2023.
Four out of nine apps with privacy policies did not require data entry from users as their main features were for COPD education. From the remaining five apps with privacy policies, four apps declared the data use and purposes while one app did not provide this information. Personal health information (PHI) was defined as any identifiable information such as name, date of birth, or health information, 32 and only four apps had clear specifications about data de-identification, anonymization, and storage on servers. Two out of the five apps explicitly stated that collected data and its usage complied with the Health Insurance Portability and Accountability Act (HIPAA). Details about apps’ security system (3/5) and data sharing with third parties (2/5) were rarely mentioned. None of the apps were equipped with features to respond to potential harm or safety concerns.
Many apps were not designed to maximize data interoperability and integration. Two of the 13 apps describe they could be used with users’ healthcare providers, or in conjunction with their treatment plans (4/13). Two apps mentioned that collected data could be exported and one of them stated data can be sent to users’ electronic medical records (EMR).
Evidence and clinical foundation
Apps’ evidence and clinical foundation details are described in Table 4. Most apps (10/13) had features as advertised on their download page. None of them had feasibility, usability, or efficacy studies to support their use. A few apps (5/13) provided users with a warning of use, that users should not replace medical assistance with the apps. 32 After trialing the apps, reviewers found that nine apps provided outdated (updates not within 6 months of this review), incorrect or misleading information about COPD and were classified as potentially harmful 32 as they contained information not aligned with known published guidelines and standards of care. Additionally, two apps did not provide clear information or resources for their content. Whereas NHS Wales: COPDHub by The Institute of Clinical Science and Technology and COPD Pocket Consultant App by the COPD Foundation do allow users to refer to resources provided by licensed healthcare professionals, or from the GOLD guideline, 2 respectively, but the remaining (11/13) apps did not provide information or direct their users to additional resources from known COPD management guidelines.
Apps’ evidence and clinical foundation details.

✓- Yes; Blank – no; NA – not applicable;
*Studies that have demonstrated the specific apps’ effectiveness, usability, feasibility etc.
**The impact factors of the journals where the peer-reviewed publications were published (in prior column).
†Potential harms criterion was satisfied if the app made recommendations that did not align with known guidelines, or provided false information, as defined by Lagan et al., 2020. 30
‡Apps with disclaimers stating that app usage does not replace medical care – if mentioned, this assessment criterion was met.
※Apps unavailable on either app stores as of January 2023
Six apps had relevant documents describing their qualities and characteristics. COPD Pocket Consultant App, created by the COPD Foundation, was described in a document by the COPD Foundation (non-profit organization in the US) highlighting its features and potential for healthcare plans. 43 COPD Pocket Consultant App was also assessed in two separate studies by Sleurs et al. 44 and Bricca et al. 45 Cliexa-COPD by Cliexa Inc. was assessed in Bricca et al. 45 and four other apps (COPD by Focus Medica India Pvt. Ltd; Book of COPD by Book Free Apps; Chronic Lung Disease Treatment by Revolxa Inc.; MHT COPD Self-care by Manifold Health Tech USA Inc.) were assessed by Sleurs et al. 44
App inputs, outputs, engagement styles, and features
Specific details of each apps’ features and engagement styles are outlined in Table 5. Most apps required input from their users using surveys (7/13) and diary logs (3/13). Access to users’ geolocation, camera, external devices, contact lists, or social media accounts was required in different apps. For app outputs, several provided notifications (5/13), reminders (4/13), numerical (6/13), and visual (4/13) summaries.
Information apps require and return to users (input and output), and their overall engagement style (method of relaying information to users).

✓- Yes; Blank – no; NA – not applicable;
※Apps unavailable on either app stores as of January 2023
Common features to supplement the apps’ engagement are shown in Table 1.
Several apps (7/13) engaged with their users by seeking data through questionnaires, usually for COPD symptoms and diagnoses. Apps relayed their information and features using a variety of methods, including chats, videos, and audio functions.
Of the total 20 potential features listed in the MIND Framework, 11 were observed (Table 1). The most common feature was education (9/13), followed by medication reminders (4/13), action plans (3/13), tracking and teaching exercises (2/13), journaling (2/13), connecting to peers (2/13), breathing and mindfulness exercises (1/3), and connecting to healthcare providers (1/13).
App ratings
The reviewers’ ratings for each app are mentioned in Table 6. The reviewers’ ratings for these apps ranged from 1 “I would not recommend this app to anyone” to 4 “there are many people to whom I would recommend this app”. One app, myCOPD assistant (Revitality LLC) only has one reviewer's rating as the app was no longer available for the other reviewer by the time of their assessment. Only two apps were rated 4 (“there are many people to whom I would recommend this app”), with the remainder of apps having scores of 3 or less. The average rating for all assessed COPD apps was 2.04, indicating the unlikeliness of these public COPD apps to be highly recommendable. And despite hundreds of downloads, two apps had public ratings available; COPD Pocket Consultant App by COPD Foundation had five star ratings from nine users on the App store compared to 3.8 star ratings from 24 reviewers on the Google Play store, and Chronic Lung Disease Treatment by Revolxa Inc. had 4.8 star ratings from 22 users on the Google Play store.
Final app ratings between the two reviewers.

A – Reviewer 1; B – Reviewer 2
*Download information not provided on the App store
※Apps unavailable on either app stores as of January 2023
An average score of all the apps was calculated; many apps were poorly designed, with inadequate peer-reviewed information to be endorsed for use. App and Google Play store ratings are included as well, if available.
Discussion
This study highlighted the variability in mHealth app designs, characteristics, and credibility. Features differed among apps, with education and medication reminders being the most common. Most apps did not clearly identify their sources of information, some of which provided incomplete information or secured their information behind pay-walls. 31 These public COPD apps were deemed inadequate and unsuitable for self-management use. Many did not reference credible information,31,34 or provide frequent updates in parallel with emerging evidence,46,47 or support data sharing with relevant clinicians.9,18,22 They also did not align with resources such as peer networking and self-monitoring that would enforce positive behaviors,30,48 and there was no evidence to determine the effect of their use on behavioral changes. 34 Generally, most apps cannot be recommended for use, and two apps had limited user ratings on their respective pages despite hundreds of downloads.
COPD self-management has been defined by the personalized, multi-component process of engaging and supporting patients to adapt their behaviors and skills to adequately manage their disease. 36 Therefore, features that provide feedback and support patients’ understanding of their disease and self-management were identified to be useful in past studies.20,26,46,47 However, the evaluated apps in this study do not have past studies to support their clinical effectiveness. Most public COPD apps provided features to educate their users of the disease, and possible management options. However, education alone is insufficient for COPD self-management, 49 as the absence of the necessary interactive planning, personalization, and support possibly would not elicit behavioral changes.46,50 Although several public COPD apps had features for symptoms screening and monitoring, they did not provide interactive feedback to help guide and support users to make appropriate behavioral changes and self-care plans. It is crucial for apps to incorporate components of feedback and collaboration into their features to potentially impact users’ health outcomes. 49 These are major contributors to empowering behavioral changes,23,51 improving health-related quality of life,52,53 physical activity, 54 and overall satisfaction. 55 Unfortunately, these apps were likely not adequately equipped to provide the level of interactive feedback needed to support personalized COPD management.
Privacy violations through shared data with third parties are an important concern in the implementation of mHealth apps.18,56 This requires users to be cautious as to how they use and share their data, demonstrating the importance of apps having easily understandable and transparent privacy policies. 32 Although many of the apps reviewed included privacy policies (9/13 apps), most were not described sufficiently to meet the security suggestions outlined in the MIND assessment, 35 nor did they identify compliance with Health Insurance Portability and Accountability Act (HIPAA) or its equivalent. Privacy policies provided also required a literacy level of graduate high school (mean FKGL 13.8), even though publicly available information should be at FKGL 8. 42 The effectiveness of the publicly available COPD apps evaluated in this study had not been verified in the clinical setting and only five of the 13 apps stated that their apps should not replace medical care. Such issues of credibility and clinical evidence are frequently of concern to clinicians and patients in knowing which apps might be the most useful in self-management.26,31,34
There are a few studies that have assessed public apps for patients living with chronic lung diseases, and reported on their quality and usability using several different measurement tools. In a previous study evaluating apps for chronic lung diseases, Sleurs et al. 44 included a total of 15 COPD-targeted apps (searched in November 2017), where five were available for assessment in our study. Although Sleurs et al. developed and used the Patient Empowerment through Mobile Technology Index to assess app quality, similar to our results, they found the apps to have overall poor quality. 44 In another review of public apps designed for chronic diseases (searched October 2020), two out of 10 COPD apps were mutually included.37,45 Using the Mobile App Rating scale (MARS) and App Behaviour Change Scale (ABACUS), Bricca et al. reported mediocre quality with poor potential to elicit behavioral changes.37,45 Other studies have evaluated public apps for specific symptoms experienced by people living with lung diseases, such as breathlessness 29 and promoting mindfulness. 57 Six apps designed for people experiencing breathlessness with a variety of health conditions were assessed for their usability and compliance with industry standards related to data usage, confidentiality and security, using the MARS and Health on the Net (HON) Code, respectively. 29 Most of the apps were available on the Android platform, and have features to support education (3/6), exercise recommendations (3/6), and less commonly, medication reminders (1/6), symptoms tracking (1/6), and referrals to healthcare providers (2/6). 29 The authors reported fair usability, but apps were likely to lack the ability to support behavioral changes to decrease people's breathlessness, and none of the apps were completely compliant with the HON code. 29 Similarly, in the study by Owens et al., nine public apps (searched May 2017) designed for promoting mindfulness strategies in people living with chronic lung diseases were poor, with app content not in alignment with scientific evidence. 57 Neither apps reviewed by Owens et al. and Sunjaya et al. were exclusive to COPD self-management, but both demonstrate the poor quality, limited usability and overall lack of details toward privacy and security in public apps.29,57 These findings are similar to our results, where public apps are lacking in high quality,29,44,45,57 but our study was unique for assessing mHealth apps targeted towards complete COPD self-management and reviewed qualities beyond their features and basic security characteristics, using one framework.
There is one study that has evaluated apps using the MIND framework; the authors evaluated diagnostic and screening apps for perinatal mental health. 39 Most apps were developed by for-profit companies (10/14), with only half of them accessible on both mobile platforms, and the common feature was education (6/14) and only one app referenced a peer-reviewed study. 39 In regards to privacy and security characteristics, 11 of 14 apps had privacy policies with an average FKGL 12.3 and two apps claimed to be compliant with HIPAA. 39 Between our studies, there is the need for current mHealth apps to be assessed for their clinical effectiveness and to improve data protection and sharing, 39 irrespective of their intended user population. In contrast to other usability and quality assessment scales mentioned above,29,44,45 the MIND incorporates all of these elements into one large framework, demonstrating its comprehensiveness in multiple domains. 35 The broad applicability of the MIND framework in our study and Spadaro et al. 39 demonstrate its valuable information in guiding the development and improvement of future mHealth apps in mental health and COPD self-management.
Despite our search for apps relevant to COPD self-management, many irrelevant apps to COPD management were found. This could be due to using multiple key terms to search the app marketplaces for thoroughness and the possibility of apps using COPD-related terms as key words in their descriptions. It is unclear whether this strategy was used to promote their apps’ visibility,58,59 but it did increase the risk of confusion for misinformation. We also noted more apps on Google Play store than on the Apple store, possibly due to the differences in the terms required by these organizations for developers to release their apps onto their platforms and to promote their products. 60
With the app marketplace rapidly evolving, 56 three of the originally included apps became unavailable over the duration of this study. This fluidity makes it difficult for potential users to be up to date on the number and content of public apps. 56 This dynamic change in apps availability has been addressed in mental health self-management by the creation of a public database of evaluated apps. Harvard Medical School in partnership with Beth Israel Deaconess Medical Center host the online MIND database, where clinicians and users can find the most appropriate mental health apps, previously validated by MIND assessments completed by trained raters.32,35 Similarly, public COPD apps also evolve and change over time, necessitating a feasible solution to ensure and maintain their credibility and qualities.44,57
This study showed the inadequate state of the quality of public COPD apps’ and their use for self-management. As many of the public apps assessed in this study did not provide these features mentioned in the literature or outlined in the MIND framework, COPD app developers need to be conscientious of incorporating the support needs of people with COPD, so features and resources are aligned with patients’ needs for better self-care.3,7,48 Areas of app improvement include the need for referencing credible information,31,34 providing consistent and relevant updates in parallel with the emerging evidence,46,47 improved privacy and security for data protection, 56 and the ability to share data with relevant clinicians.9,18,22 There should be considerations to include the need for reading level appropriate content, goal personalization, peer networking, and self-monitoring to enforce positive behaviors.30,48,57 Apps should also allow for content customization to meet individual users’ needs, and enable users’ family or caregivers to be involved with the app. 47 The MIND framework outlined many possible features and engagement styles for apps to interact with their users, serving as a guide for developers to incorporate potential features that will encourage patient engagement with their healthcare providers, and provide personalized feedback in the forms of alerts, reminders, education or coaching to facilitate behavioral changes for improved disease control.30,46 Additionally, apps need to be user-friendly for successful implementation. 26 Furthermore, collaborations between COPD app developers, researchers, and healthcare systems are necessary to ensure the safe integration of features, content, and adoption into healthcare plans. 46 Public COPD apps are readily accessible and show promise in facilitating COPD self-management; however, strategic plans and regulations are required to ensure their credibility and safe integration. 34
Strengths and limitations
Study strengths included minimizing bias by two reviewers independently screening and assessing all apps before discussing their findings, minimizing bias. There is significant variability in quality assessments for mHealth apps, and emphasizing the need for evaluations to address the clinical impact and behavioral change mechanisms. 34 As the MIND framework was derived from 79 frameworks focused on general and specific disease domains including asthma, heart failure, mental health, and pain management, 32 many aspects of the apps’ characteristics and features were reported. 32 This comprehensive assessment would not have been possible with other frameworks, as they commonly reviewed the effectiveness of apps and their features, often missing other important design elements such as privacy and security characteristics.44,61 Lastly, the MIND framework was originally developed to assess public apps for mental health. 35 However, we decided to apply this comprehensive framework onto another category of mHealth apps, those meant for COPD self-management. To our understanding, this is the first time the MIND framework was applied in this context.
Limitations are only including mHealth apps in English that were free to download, as cost can be an accessibility barrier.26,37,45 It may be possible for paid apps to be of higher quality with features that would have meaningful impact on users’ self-management. Additionally, we were unable to evaluate several apps in the Apple or Google Play stores as they were restricted to study participants enrolled in ongoing clinical studies.23,51,55 Lastly, app stores are not designed for research-based structured searches, 62 it is challenging for searches to be updated and replicated for future studies. 39 We noticed that search results were inconsistent, where the order of apps appeared differently despite using the exact keywords. This is likely due to regional restrictions, and search algorithms are driven for promotion and commercial profit in certain geographical locations, influencing the retrieved app results.59,62 Instead of displaying the total number of apps for each search term, both Apple's and Google's app stores required the reviewers to blindly scroll through the results list until it stopped loading, indicating all apps for a specific keyword were shown. Being unable to see the total for each keyword made it challenging for reviewers to revisit the search at another time, a common challenge reported in another scoping review. 39
Conclusions
COPD apps in the public marketplace have inadequate qualities and features to address privacy concerns and insufficient information to demonstrate their credibility or effectiveness for self-management. Publicly available COPD apps should be used with caution as many have the potential to cause harm to their users.
Footnotes
Funding
This work was supported by the Canadian Lung Association - Breathing as One: Allied Health Research Grant. SQ received financial support from the Canadian Lung Association (Allied Health Fellowship) and Canadian Respiratory Research Network (Studentship) for this research work. DB holds a National Sanitarium Association (NSA) Chair in Respiratory/Pulmonary Rehabilitation Research.
Research ethics and patient consent
Not applicable. This study did not involve human subjects.
Authorship
All authors designed the study; or collected, analyzed, or interpreted the data; and drafted or critically revised the article and approved the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Guarantor
SQ & DB