
Abstract
Aims
Cardiac rehabilitation is an essential component of secondary prevention consistently unexploited by most eligible patients. Accordingly, the remote cardiac rehabilitation program (RCRP) was developed to create optimal conditions for remote instruction and supervision for patients to enable successful completion of the program.
Methods
This study comprised 306 patients with established coronary heart disease who underwent a 6-month RCRP. RCRP involves regular exercise, monitored by a smartwatch that relays data to the operations center and a mobile application on the patient's smartphone. A stress test was performed immediately before the RCRP and repeated after 3 months. The aims were to determine the effectiveness of the RCRP in improving aerobic capacity, and correlating the program goals and first-month activity, with attaining program goals during the last month.
Results
Participants were mostly male (81.5%), aged 58 ± 11, enrolled in the main after a myocardial infarction or coronary interventions. Patients exercised aerobically for 183 min each week, 101 min (55% of total exercise) at the target heart rate. There was a significant improvement in exercise capacity, assessed by stress tests, metabolic equivalents which increased from 9.5 ± 3 to 11.4 ± 7(p < 0.001). Independent predictors of RCRP goals were older age and more minutes of aerobic exercise during the first program month (p < 0.05).
Conclusion
Participants succeeded in performing guideline recommendations, resulting in a significant improvement in exercise capacity. Older age and increased volume of first month of exercise were significant factors associated with a greater likelihood to attain program goals.
Introduction
Cardiac rehabilitation (CR) is considered an essential component in the prevention of future heart episodes, re-hospitalizations, and death from all cardiac-related causes.1,2 Despite the documented evidence of the benefits of CR, less than one-third of patients actually begin rehabilitation. 3 Of these, approximately 24% to 50% of patients terminate the program ahead of time and are therefore unable to achieve the desired outcome. 4 The reasons for nonparticipation in rehabilitation programs are diverse. These include objective barriers (such as the remoteness of the medical center, lack of accessible transportation, travel cost, unsuitable work hours, and socioeconomic factors), as well as behavioral and psychosocial reasons.5,6 Remote cardiac rehabilitation programs (RCRP) are typically performed in a patient's environment, using modern telecommunications technology tailored to the characteristics and needs of the individual patient. Thus, RCRP not only overcomes the many aforementioned barriers of traditional CR, but also achieves all the clinical goals set by traditional rehabilitation while simultaneously improving exercise adherence, physical activity levels, as well as reducing the relative cost of treatment.7,8
In previous studies, the successful use of features provided by the RCRP platform in the early stages of the program resulted in better compliance and adherence.9,10 However, we found no mention of how patients’ patterns of workouts and behavior in the first weeks of remote CR affected their subsequent adherence. The purpose of this study was to describe the achievements of the first RCR group within the Israeli Health system and to shed light on how potentially influential the first weeks of participation in the completion of the 3-month program.
Methods
RCRP
The first Israeli RCRP was developed at the Sheba Medical Center. It was approved by the Israeli Ministry of Health as a 3-month rehabilitation program for low-risk patients and is fully covered by the basic health insurance at no cost to patients. Low-risk definition according to the national guidelines is defined as lack of > 5% ischemia per stress or pharmacological single-photon emission computed tomography (SPECT), left ventricular ejection fraction (LVEF) 50% or more, lack of sustained ventricular tachycardia, symptomatic atrial fibrillation of flutter or heart rates (HRs) > 120 beats per minute at rest. Low-risk definition excludes patients after cardiac arrest, heart failure with preserved systolic function and low functional capacity (metabolic equivalents (METs) < 6). A detailed description of our RCRP was published earlier. 11 Briefly, the program combined the use of advanced telecare technologies (platform by Datos Health) and smart wearable devices (mostly Garmin and Apple smartwatches) (Supplemental Appendix A- C) adapted to the characteristics and needs of each particular patient.
The program was geared to motivate the patient to perform workouts at home or in any convenient community facility, to lead a healthy lifestyle, as well as manage their clinical and psychological health. Necessary conditions for RCRP success included both motivational and technological aspects. For example, in addition to receiving automatic encouraging messages and reminders, the patient received a personal weekly call from a CR trainer to discuss the training program and any problems that may have arisen. The patient received necessary technical and clinical support from a multiprofessional care team (physician, psychologist, physiologist, nurse).
Throughout the 18 months of the program, we collected data on behavior patterns, training, and goal achievements from the first low-risk group of 306 patients, 81.5% men, aged 57.59 (±10.62) rehabilitating under the RCR at Sheba Medical Center in Israel. Basic characteristics, including a complete medical history, risk factors, and laboratory tests were collected. Training patterns were obtained via the smartwatch and then analyzed prospectively by the platform for 24 weeks. Objective improvement of an individual's functional capacity was assessed as the change between the first (2–3 weeks before starting rehabilitation) and the second (post 3 months of rehabilitation) exercise stress test (ergometry) using the same protocol and environment. Satisfaction with the program and care received was recorded and assessed using a questionnaire.
The main objective was to gauge the effectiveness of the RCRP protocol for any changes in exercise capacity assessed by treadmill exercise stress test using Bruce or modified bruce protocol based on patient baseline functional capacity (history and impression) as assessed by the exercise physiologist. The same protocol was used for the second stress test after the 3-month program. The relative assessment of patients’ adherence and achievement of the main “exercise goals” of the rehabilitation program, was also recorded. The “exercise goals” of the program were defined as the: (a) training performance of at least 150 aerobic minutes per week, of which; (b) 120 min in the target HR, set by the exercise physiologist; (c) two strength training sessions per week (after the first month); and (d) at least 8000 steps per day. And 100% achievement of these goals was considered satisfactory adherence. The individual target HR was determined in accordance with the recommendations of the national cardiac rehabilitation guidelines, based on the stress test results of each patient.
The study's second objective was to describe the differences in the baseline characteristics of patients that attained program goals versus the ones who did not. We conducted a retrospective analysis and comparison dividing all patients into two groups: those who achieved the main “exercise goals” of RCR and those who did not. The “exercise goals” for this comparison were specified as: (a) completion of the full 3-month program; (b) achievement of 600 aerobic minutes in the third month of the program (150 min weekly times 4 weeks); (c) achievement of 400 min in the target HR (120 min weekly times 4 weeks) in the third month.
The third objective was to identify potential independent predictors to better achieve the aforesaid exercise goals. We aimed to assess whether variables such as age, gender, baseline exercise capacity, indication for rehabilitation, use of the program's mobile app, as well attaining goals (150 aerobic minutes per week and 120 min in the target HR) in the first month of the program, could serve as predictors for better future adherence during the third and final month of the program.
Evaluation of the patient's exercise performance was evaluated using the following exercise parameters:
The total number of weekly minutes of aerobic exercise (aerobic minutes). The number of weekly aerobic minutes in the target HR. The weekly percentage of training sessions at the target HR (preferably at least 70% of the total training time). The weekly workout intensity (preferably at least 70% of the patient's individual maximum aerobic capacity, based on the stress test). The assessment of perceived exertion on the Borg scale (patients were instructed to train within 12–14 moderate to vigorous on the scale). Number of daily steps. The number of weekly entries to the RCRP mobile phone application (patients were instructed to use the mobile app at least once every 1–2 days).
Statistical methods
Baseline characteristics are presented as median, mean ± standard deviation (SD), or percentages as appropriate and comparisons were performed according to data type and its distribution. Characteristics of patients according to goals reached or not reached were compared using chi-square test for categorical data, and two-sided student t-test or Mann-Whitney tests for continuous data, as appropriate.
A paired sample t-test or Wilcoxon signed-rank test were used, according to the normality verification, in order to assess the differences between numeric values pre-RCRP and post-RCRP.
The effect size of the Delta between the METs pre-RCR and post-RCR were calculated as the difference of the METs means divided by the square root of the mean of the METs SD square.
A logistic regression model was constructed using the best subset method in order to determine independent predictors for the completion of the two program exercise goals during the third month of the program. The first goal was to reach 600 or more total aerobic minutes (any HR) per month, whereas the second goal was to reach 400 or more activity minutes in the individually designated target HR zone per month. The following covariables were introduced in the multivariate model using the best subset method: age, gender, pre-rehabilitation METs, and indication for CR. Predictions were based on patients’ performance in the first month and some demographic data. Age and gender were taken as base features of all the models. For the predictive models, all the patients that dropped out of the program during the first month were excluded.
A p value < 0.05 was considered statistically significant and all tests were two sided. Statistical analyses were performed using the statistical software R foundation version 4.1.2.
Results
The study included data from the first 306 consecutive patients to complete RCRP. The patients joined the RCRP within 1 to 2 months after discharge from the hospital. Characteristics of the study group are summarized in Table 1.
Baseline characteristics of study population.
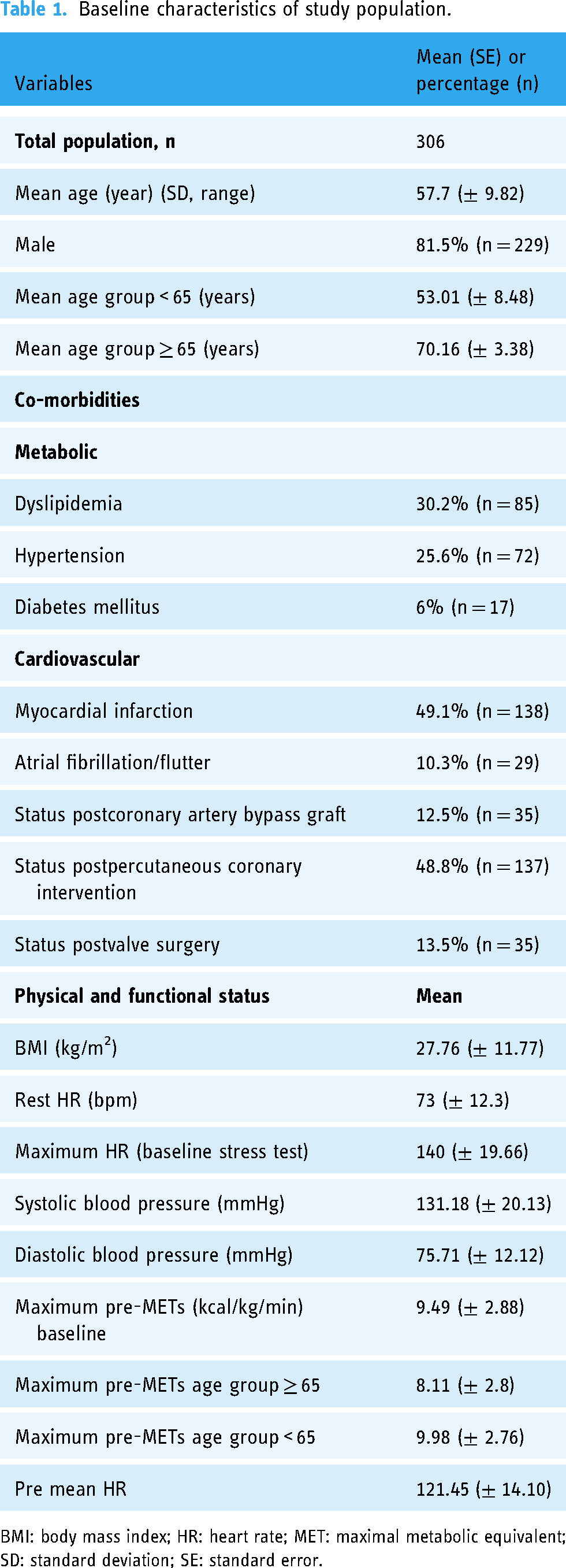
BMI: body mass index; HR: heart rate; MET: maximal metabolic equivalent; SD: standard deviation; SE: standard error.
Another comparison, shown in Supplemental Appendix D, presents the characteristics of the study group, 306 patients that participated in the RCRP, with the characteristics of a group of patients that completed a traditional center-based CR program (CCRP).
A total of 26% of this group were over 65 years of age. The main indications for CR were myocardial infarction (49%), percutaneous coronary interventions (48%) and coronary bypass surgery (12.5%). Participants had a preserved or normal systolic function and no high-risk criteria such as significant ischemia, effort angina, clinically significant ventricular arrhythmia, heart failure, or any evidence of clinical instability (mandatory national criteria to the RCRP entry). Participant adherence in the program, from the RCRP group, was 3.6 months on average, compared to CCRP participants that reached an average of 3.7 months in the rehabilitation program (Supplemental Appendix E).
The changes in exercise capacity
Following the RCR intervention, there was a significant and clinically meaningful improvement in exercise capacity, expressed by change in METs, assessed by pre-exercise and post-exercise stress tests using the same exercise protocol (Figure 1). Stress tests were performed by the same team of physiologists using the same treadmills, under the same conditions. The effect size of the exercise capacity improvement was 0.35.
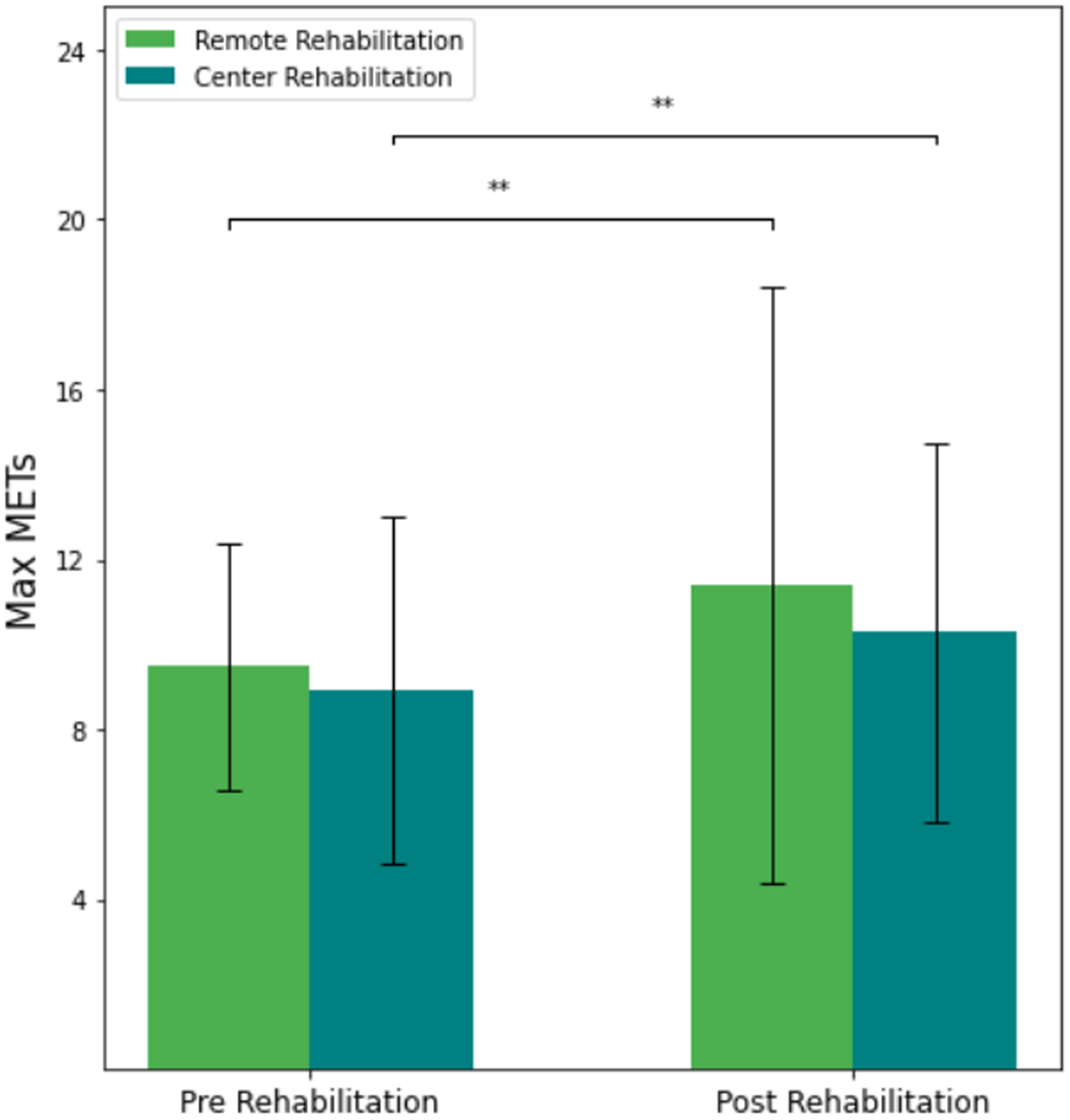
Changes in metabolic equivalents (METs) pre-RCRP and post-RCRP intervention compared to traditional CCRP. CCRP: center-based cardiac rehabilitation program; METs: metabolic equivalents; RCRP: Remote Cardiac Rehabilitation Program.
RCRP exercise goals and patient performance
Overall, the total weekly minutes of aerobic training for 24 weeks was 183 min (median) for the entire population. Upon further analysis, the elderly group (age ≥ 65) achieved 208 min whereas the younger group achieved 186 min (p < 0.01). The median number of minutes of total aerobic minutes for 6 months was 183 min per week, which was 122% of the goal set by the physiologists. Additionally, time spent at the target HR was 101 min per week, which was only 84% of the 120 min exercise goal, usually divided into 4 exercise sessions. Figure 2 presents the median weekly aerobic activity of RCRP participants.

The weekly aerobic exercise activity at target heart rate and below the target zone.
Exercise at the target HR was 55% of the total exercise time, which was less than our predefined goal of 70%, representing an intensity of 75% of the patient's personalized maximum aerobic capacity (all median values). The subjective perception of effort (Borg scale) was 11.7 and the daily step count was 7700. Participants used the program's mobile application 3.8 times per week.
Patients’ baseline characteristics and exercise goals attained
We evaluated the characteristics of those patients achieving the exercise goals set by the RCRP compared to those who did. Patients who achieved the exercise goals in the third month, were more likely to be older and have greater exercise activity during the first program month. Comparisons are summarized in Table 2.
Observed differences between the baseline characteristics according to the RCRP “exercise goals.”

BP: blood pressure; HR: heart rate; MET: maximal metabolic equivalent; RCRP: Remote Cardiac Rehabilitation Program; SD: standard deviation.
Predicting exercise goals achievement during the third month of the program
Two main exercise goals were assessed using multivariate analysis: (1) would the patient achieve 600 min of monthly physical aerobic exercise and (2) would the patient achieve 400 min of monthly aerobic exercise at the target HR. Both outcomes were assessed during the third month of RCRP.
For every 100 min of training there was a 10% higher likelihood of achieving the 600 min aerobic goal during the third month. Similarly, for every 1000 steps the likelihood increased by 4% for the same outcome. Table 3 presents the results of the regression model.
Predictive models for achieving “exercise goals” during the third month of RCRP.
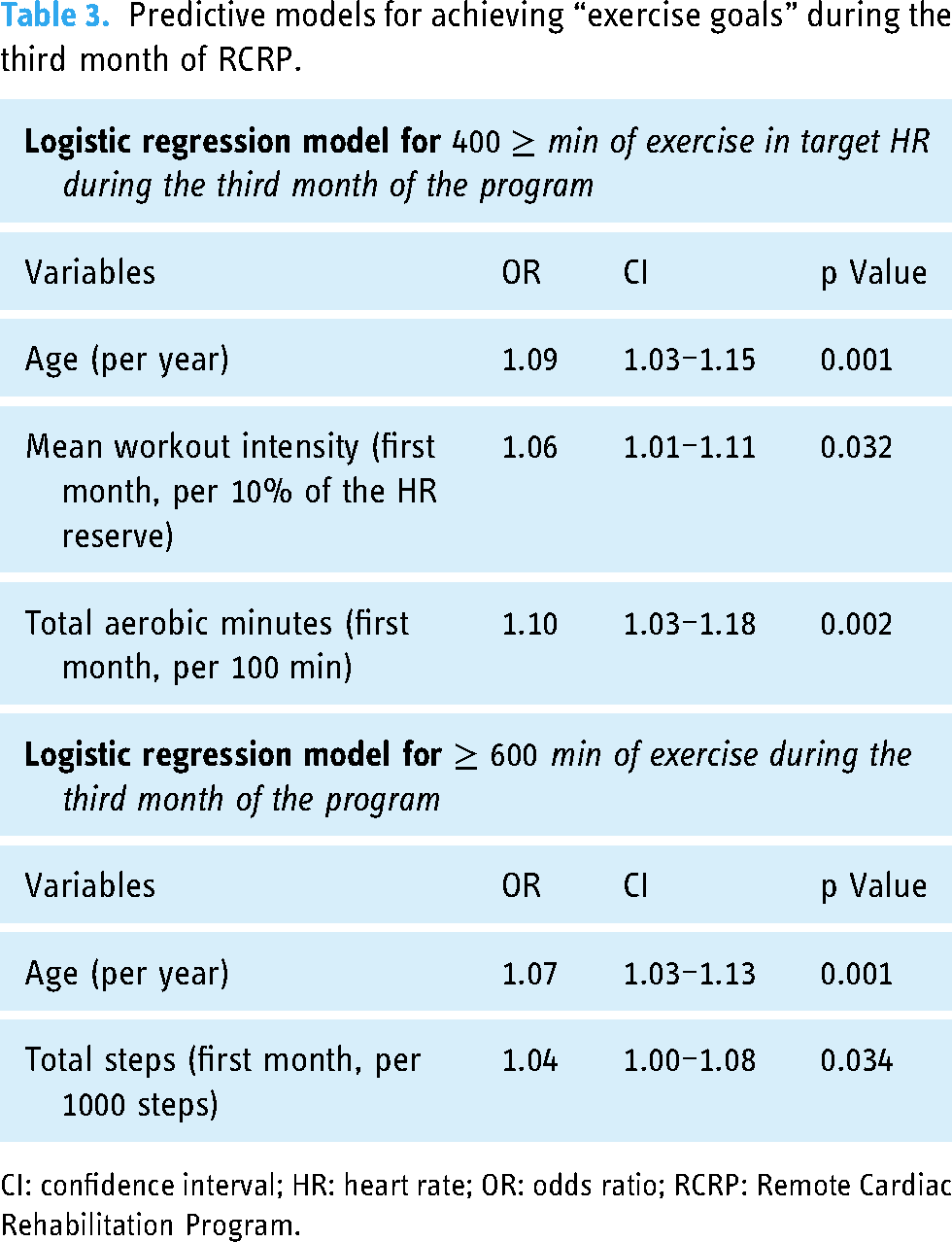
CI: confidence interval; HR: heart rate; OR: odds ratio; RCRP: Remote Cardiac Rehabilitation Program.
Among all the variables included in the multivariate model, only age and aerobic performance in the first weeks of RCRP were significant predictors, while variables such as gender, pre-rehabilitation METs, mobile phone application usage or workouts’ average HR were not significant.
Discussion
The main findings of our study show that patients participating in RCRP can reach the programs’ multiple exercise targets and improve their aerobic capacity. We also found that the patient's age and aerobic exercise volume during the program's first month are independently correlated with the program's goal achievement rate.
CR has been proved to be an underutilized service. It reduces cardiovascular mortality, hospital readmissions, and associated healthcare costs, while simultaneously improving health-related quality of life. 12 RCRP has also been demonstrated to be an effective and cost-efficient alternative to the traditional CR delivery model. It facilitates individualized support in almost any location. 8
Overall, our program achieved its goals in terms of exercise adherence and was shown to significantly improve the functional capacity of its participants. These results are comparable with previous reports. 13
In our study, we aimed to explore the differences in baseline characteristics between patients who managed to achieve the main goals of the RCRP and those who did not. We found that individuals who were deemed to be more successful by the end of the third month of the program tended to achieve greater aerobic performance in the first month. The main predictors of achieving the RCRP goals during the third month include the age, and the number of aerobic minutes in the first month as well as steps. Accordingly, we can cautiously conclude that increased commitment to the program goals at the beginning of the rehabilitation is associated with better program goal completion. Importantly, this permits early identification of patients less likely to attain goals.
Despite ongoing research in this field, many studies have not documented a similar association between early aerobic minutes and RCRP goal completion. Initial active engagement in RCRP could be a significant predictor for future goal completion as well as attaining desired level of cardiovascular health. Several studies have shown that the timeous start of rehabilitation after a cardiovascular event leads to better health outcomes for patients. 14 Furthermore, other studies have even gone as far to say that delays in starting CR can cause avoidable harm in the long-term health of patients. 15 This shows the already well documented importance of the timely start of CR programs.
However, just informing patients to join CR early after their cardiovascular event is insufficient on the part of the physician. Our results indicate that patients who demonstrated early active participation in the program (those who achieved greater aerobic minutes) better achieved the program's adherence goals. These results indicate that physicians should motivate patients early on in their remote-CR progress, as we found that the first few weeks are a crucial period for determining their future success in completing program goals. Younger patients could require special consideration since apparently it appears to be more difficult for them than for the elderly to fulfill all the requirements of the RCRP.16,17 This can be explained both by the lack of time and by a less serious perception of their illness. We speculate that motivation was an important factor for early active participation in the program. Patients who achieved greater total aerobic minutes early on in the program could have had certain motivation that resulted in their better completing program goals. Another relevant CR study demonstrated that motivational programs appear helpful in increasing participation in early outpatient cardiac rehabilitation. 18 Whether patients in our study who achieved greater total aerobic minutes early on in the program were or were not motivated intrinsically or extrinsically is debatable, but further studies need to be performed in the future to determine which plays a bigger role in CR program completion.
However, it should be noted that, despite a good indicator of the total number of aerobic minutes, their aerobic exercise intensity was lower than desired: the percentage of time that patients spent in the target HR during the training was significantly lower than we expected. Also, the subjectivity when assessing training intensity was questionable.
In other words, patients who trained a lot, did not always do so effectively. Although the overall increase in functional capacity (METs) was good, it seems that patients were capable of more.
In addition, we found that older age was also associated with better achievement in all RCRP goals and was a predictor of adherence to these goals refuting the generally accepted opinion that digital programs are less suitable for the elderly.19,20
The applicability of the research findings and limitations
The results of a study can have significant applicability in the healthcare industry. RCRP utilizes telemedicine and digital health technologies to provide patients with cardiovascular disease rehabilitation services in their homes, without the need for in-person visits to healthcare facilities.
The study results can be used to inform the development of new remote cardio-rehabilitation programs, as well as the refinement of existing ones. Healthcare providers and policymakers can use the study's findings to design and implement effective remote cardio-rehabilitation programs to improve patient outcomes and reduce healthcare costs. In particular, we propose to focus efforts on better engagement with younger patients, as well as on better compliance with the program in the first weeks.
Additionally, the results can help clinicians to optimize their use of digital health technologies and telemedicine platforms to provide high-quality care to patients with cardiovascular disease and manage expectations regarding activity levels and change in functional capacity. Overall, the study results can contribute to the development of more patient-centered, accessible, and cost-effective models of care delivery that can improve health outcomes of individuals with cardiovascular disease.
Our study is not without limitations. This research is based on a single center experience and thus variations are to be expected. The study population enrolled was defined as low risk per national guidelines thus results cannot be extrapolated to all patients with cardiovascular conditions. Additionally, patients in our study did not work out as intensely as the program indicated (the average Borg was less than 12–14). Patients generally coped well with goals, however, we would have liked to see more intense training, such as more time spent in the target HR and a higher Borg scale. Furthermore, patients did not achieve goals that were related to their strength exercises (resistance training). This is partly due to a lack of time, patient preferences, and the instructions of medical staff who emphasized the value of aerobic exercise for cardiovascular health. This aspect has been identified in other similar RCRPs. An additional limitation worth mentioning is that patients in the study were mostly male (81.5%), making it difficult to extrapolate our results. In addition, the patients who participated in this study represent a low-risk group, which means that at baseline they already had good functional capacity and risk factors of cardiovascular disease were mostly within guideline recommended ranges. Because this is an observational study we can report associations and not address causations. It is also important to note that subtle differences in the execution of the stress tests, and other less definable variables may have impacted the observed change (e.g., higher confidence of the patient and the care team itself in the second stress test).
Conclusion
To the best of our knowledge, there have been no previous attempts to understand how the patient's behavior at the beginning of the RCRP could serve as a predictor of future program success. Understanding this information is instrumental in building more accurate, patient-oriented intervention programs in the future. Additionally, availability of this information at the outset will help us recognize certain characteristics which could contribute to or hinder their success in the program. The RCRP care team should pay special attention to the adherence and performance of physical activity in the first weeks of RCRP, because it is correlated with subsequent successful completion of the program.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180762 - Supplemental material for Israel's first national remote cardiac rehabilitation program: A retrospective analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180762 for Israel's first national remote cardiac rehabilitation program: A retrospective analysis by Irene Nabutovsky, Daniel Breitner, Alexis Heller, Merav Moreno, Yoav Levine, Yarin Klempfner, Mickey Scheinowitz and Robert Klempfner in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231180762 - Supplemental material for Israel's first national remote cardiac rehabilitation program: A retrospective analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076231180762 for Israel's first national remote cardiac rehabilitation program: A retrospective analysis by Irene Nabutovsky, Daniel Breitner, Alexis Heller, Merav Moreno, Yoav Levine, Yarin Klempfner, Mickey Scheinowitz and Robert Klempfner in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231180762 - Supplemental material for Israel's first national remote cardiac rehabilitation program: A retrospective analysis
Supplemental material, sj-docx-3-dhj-10.1177_20552076231180762 for Israel's first national remote cardiac rehabilitation program: A retrospective analysis by Irene Nabutovsky, Daniel Breitner, Alexis Heller, Merav Moreno, Yoav Levine, Yarin Klempfner, Mickey Scheinowitz and Robert Klempfner in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the ARC Innovation Center and Medical Center beyond for their support.
Author contributions
IN led, designed, and conducted the study. DB, AH, and YL drafted and reviewed the manuscript. MM and YK collected and prepared the data alongside its statistical analysis. MS and IN interpreted the study results. RK oversaw the study and was involved in the study design, drafting, and reviewing. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The present retrospective study was conducted according to the IRB approval instructions and GCP principles. Sheba Medical Center, approval ID: 1553-14-SMC.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
IN.
Patient consent
Our study was conducted on de-identified data files extracted from the Sheba Medical Center data lake by hospitals approved personnel, according to the IRB approval granted (IRB approval number SMC 15-2699).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.