
Abstract
With the development of mobile communication technology, persuasive technology is widely used in mobile health. Using personalized persuasive strategies in mobile health education (MHE) apps can effectively improve users’ health literacy and health behaviors. The transtheoretical model explains the process of user behavior change. Different usage frequency of the app reflects changes in user behavior. However, few studies have examined how the perceived importance of persuasive strategies among older adults changes with increasing use frequency. In this study, we analyzed the sensitivity of 111 older adults in China to persuasive strategies in MHE apps. Thirteen persuasive strategies were selected for this study. A repeated measure analysis of variance (RM-ANOVA) was used to demonstrate the influence of gender, health information attention and frequency of use on the sensitivity of perceived persuasive strategies among older adults. The results revealed older adults with a high usage frequency of health apps were more receptive to persuasive strategies, especially in social comparison strategy. This result may help developers consider factors such as the frequency of use by older users when designing personalized persuasive strategies for MHE apps.
Keywords
Introduction
The increasing ageing has made the health of older adults a hot topic. As technology evolves, e-health and mobile health tools are increasingly being used in health promotion and primary prevention among older adults. 1 Mobile health devices can manage and motivate older adults’ health behaviors, assess health abnormalities and detect certain early diseases by monitoring relevant physical data from users. 2 Besides, mobile-based health education apps help reduce the workload of healthcare providers, improve the efficiency of care, reduce healthcare costs, and help older adults maintain their health and independence. 3
Health education is an essential tool to promote health in older adults because it provides knowledge to prevent and reduce disease, enables active participation in life transitions, and encourages self-care and the search for autonomy. 4 Mobile phone-based health education helps to promote health behaviors. Health education programs can be effective in improving health promotion knowledge and behaviors among older adults. 5 Studies have shown that mobile app-based interventions may help to improve various health promotion behaviors.6,7 Changizi and Kaveh 8 suggested that appropriate educational programs using smartphones can significantly change behaviors related to healthy lifestyle quality and reduce health problems in old age. Consistent use of mobile health education (MHE) apps can be effective in improving users’ health literacy and health behaviors.7,9 In addition, habits directly influence users’ willingness to continue using mHealth apps. The stronger the habit of using mHealth apps, the stronger the probability to continue using mHealth apps. 10 It has been demonstrated that the usage frequency of health technologies affects sustained usage behavior. 11 The critical driver of reduced usage frequency or abandonment of mHealth apps is a loss of motivation and interest. 12 Maintaining a high level of user motivation and interest tends to be more likely to increase the frequency of use of mHealth app. Therefore, app developers need to consider effective strategies to engage users in the habit of using mHealth apps and to maintain user motivation and interest to enhance health behaviors.
The persuasive technology proposed by professor Fogg is mainly defined as intervening in the user’s behavior through information and computer technology with persuasive strategies rather than coercion. 13 Kaptein et al. 14 demonstrated the importance of personalization strategies for system design by sending personalized text messages to users to help reduce snack intake. The mechanisms that cause changes in people’s attitudes and behaviors may arise from many different theoretical and psychological processes. In this regard, Oinas et al. 15 proposed a persuasive system design (PSD) model and 28 persuasive strategies for designing and evaluating influencing user attitudes or behaviors. These strategies are divided into four categories according to system characteristics: task support, dialogue support, credibility support, and social support. Persuasive techniques (PT) are used to engage users and promote healthy behaviors through a variety of persuasive strategies. PT facilitate the process of health behavior change in people with chronic diseases. 16 Persuasion and motivation help people improve their health status. 17 A review examined the effectiveness of PT in health, and the results demonstrated that PT can be used to promote desirable behaviors within the context of health and wellness. 18 The use of persuasive technology can also help promote the acceptance of mHealth applications. Demonstrating the usefulness and usability of mHealth apps in a more persuasive manner can increase the acceptance of these new technologies among older adults. 19
Studies have shown that individuals differ in their susceptibility to different persuasive strategies. 20 A particular persuasive strategy may motivate one group of individuals to change their behavior while discouraging another. 21 Therefore, the cognitive characteristics and individual differences of older adults need to be considered when selecting individualized persuasive strategies. Studies have found that older adults’ susceptibility to persuasive strategies is influenced by personal motivation, education level, and life situation. 22 According to the transtheoretical model (TTM) of change proposed by Prochaska et al., 23 behavior change is a gradual process. We assume that users prefer different persuasive strategies at different use stages. However, existing studies on persuasive strategies for mobile health rarely consider the influence of users’ attention to health information and the use frequency on the susceptibility of persuasive strategies. Therefore, we conducted a study on personalized persuasive strategies based on Chinese older adults. This study aims to analyze whether age, gender, health information attention and frequency of use affect older adults’ susceptibility to persuasive strategies in MHE apps. The findings of this study will help to tailor MHE apps for older adults and make their health interventions more effective.4–9,16–19
This paper is structured as follows. In the next section, we reviewed the related work and present our research questions. In the section “Methods,” we described our research method and progress. In the section “Results,” we presented the results and analysis of the study. In the section “Discussion,” the implications and conclusions of personalized persuasive strategies were discussed for the design and development of MHE apps for older adults. The research framework of this paper is shown in Figure 1.

Research framework.
Related work
The transtheoretical model
The TTM proposed by Prochaska et al. 23 is a useful tool for understanding behavior change. It explains the motivation and stages of behavior change in people. 24 The model has been shown to have a significant impact on promoting health behavior change. 25 The model divides individuals’ health behavior- change in five stages according to the temporal dimension: precontemplation, contemplation, preparation, action and maintenance. 24 People in the precontemplation stage do not consider behavior. In the contemplation stage, they begin to recognize their needs and consider solutions. In the preparation stage, people gradually adopt some solutions. Over the next 6 months, people in the action stage commit to change and take action but have more difficulty sticking with it than people in the maintenance stage. People in the maintenance stage have established behaviors for 6 months or longer. 23
Currently, TTM has been used in a variety of health behavior studies in older adults. A study by Jiménez-Zazo et al. 26 demonstrated that TTM is a useful tool for creating, developing, and evaluating tailored interventions to promote physical activity behaviors in older adults. A study by Chang et al. 27 demonstrated that increasing dairy intake at different stages of change can benefit older adults in terms of dietary health. In addition, TTM-based treatment programs are effective in alleviating common joint diseases and improving joint function in older adults. 28 Although TTM has been widely used in studies related to health behavior change, it has been less used in studies on persuasive strategies to promote the use of MHE apps in older adults. The use of the TTM to categorize the user behavior changing process helps to understand the user characteristics at each stage. In this paper, we hypothesize that applying personalized persuasive strategies at each behavioral stage can help people to better improve their health behaviors.
Personalized persuasive strategies for older adults
Persuasion techniques, as a technique aimed at changing attitudes or behaviors, 15 can contribute to the long and difficult process of health behavior change. Today mobile health apps are playing an increasingly important role in accessing health information for older adults, because mobile health apps have great potential to help older adults access health information. First, older adults are considered most likely to benefit from online health information due to the large number of older adults with health problems. 29 Second, the way older adults access and share health knowledge is changing. 30 Smartphones are rapidly penetrating into people’s daily lives, and more and more seniors will use these new technologies to maintain their health and well-being. 31 Third, mobile health applications can help older adults access health information more conveniently. With the development of the COVID-19 pandemic, offline health education is gradually beginning to shift to an online education approach. Due to physical limitations and restrictions on attending face-to-face educational sessions, older adults may benefit from e-health, which in turn may have a positive impact on their health status. 32 This provides an opportunity for PT in managing the healthy lives of older adults.
There has been much research on the persuasive strategies used in health behavior interventions for older adults. For example, self-monitoring has long been proven to be the basis for many health interventions. 33 Mohadis et al. 34 revealed that similarity is essential for designing fitness apps for older adults. Persuasive strategies are associated with maintenance of use. When older users can set, monitor, and evaluate their health goals and behaviors more easily and conveniently through the use of mHealth apps, they are more likely to maintain their use of mHealth apps and engage in health behaviors. 35 Given the physical and cognitive abilities of older adults, mHealth user interfaces designed for them are often simplified for easy identification and use. Kim and Han 35 suggested using social comparison and similarity strategies to display the health behaviors of others similar to older users or to provide an opportunity to interact with others so that older users feel socially validated. In addition, praise and rewards that emphasize older users’ achievements and self-worth can maintain or improve their health behaviors. The intrinsic motivational effect of rewards is particularly evident. 36 Some of the literature has also researched individualized persuasion strategies for older adults. Using demographic variables to segment populations can help to provide targeted persuasive strategies for users. Age and gender affect the sensitivity to persuasive strategies in learners, which has been demonstrated in many researches.37,38 Abdullahi et al. 39 also noted that personalized persuasive strategies in health interventions needed to consider factors such as mental health, emotional well-being, and life satisfaction of the elderly. van Velsen et al. 22 noted that older adults’ preferences for health-related persuasive strategies are also related to personal motivation, education level and life situation.
Although these studies have analyzed several factors that influence the susceptibility to persuasive strategies, few studies have combined TTM to explore personalized persuasive strategies for older adults. Since health information attention responds to users’ health awareness and intrinsic motivation, usage frequency represents users’ usage behavior change stage. Therefore, the purpose of this paper is to analyze the effect of the health information attention status of older adults and the frequency of MHE apps use on the sensitivity of persuasive strategies. We planned to investigate four factors influencing the susceptibility of older adults to persuasive strategies: gender, age, attention to health information and frequency of using MHE apps. We also measured the susceptibility of 13 persuasive strategies. We expanded our research questions (RQ) on the following issues:
RQ1: Whether factors such as gender, age, health information attention and usage frequency affect older adults’ attitudes toward 13 persuasive strategies?
RQ2: Which persuasive strategies are more sensitive to older adults with different usage frequencies and health information attention in MHE apps?
Methods
Persuasive strategies selected
In this section, we discuss 13 persuasive strategies that are frequently found in MHE apps. The specific meanings of the selected strategies are shown in Table 1.
The example requirements of the 13 persuasive strategies category. 6

Persuasive strategy cards
To improve the comprehensibility and accuracy of the test, we created 13 persuasive strategy cards 40 as a supporting tool. The design of the persuasive strategy card was based on the Prswedo card 41 developed by Ren et al. which explains the persuasive strategies extracted from the PSD model. 15 The persuasive strategy card consists of three parts: an explanation of the persuasive strategy, a use case and an example of the interface in the smartphone app. Each card introduces one persuasive strategy. Figure 2 shows an example of a “personalization” strategy card. The cards were validated before the study by conducting two rounds of internal evaluation and adjustment to ensure that the strategy cards accurately conveyed the intent of each persuasive strategy. Experts were invited to optimize and determine the final persuasive strategy cards.

Persuasive strategies card (take personalization as an example).
User research
In this study, we mainly considered the target group of older adults who use smartphones in China, and selected the group of older adults aged 50 to 80 years old with experience in using mobile health apps to participate in the experiment. This is because older people with medical conditions gradually develop health problems starting at age 50. 42 Studies have shown that e-Health literacy of older adults decreases with age, 43 and those over 80 years of age are less familiar with mobile applications, so this group was not addressed in this study. Due to the impact of the epidemic, this study was conducted using a combination of offline and online research, and the same questionnaire and process were used for both research methods. This study was approved by the Ethics Review Committee of East China University of Science and Technology (approval number: ECUST-2022-071). The participants’ personal information was not disclosed in the paper, and the privacy of the participants was protected. Subject selection criteria were that participating older adults had mobile devices and sufficient skills to use health apps. For the offline research, team members randomly invited seniors at a public activity space. For the online research, we recruited from several WeChat groups composed of retired elderly people. The research procedures were as follows: the group members explained the purpose and methods of the study to the participants and obtained their informed consent before conducting the questionnaire. We sent the questionnaire to the participants via the WeChat version of “Questionnaire Star.” After the questionnaire was completed, we interviewed some of the offline participants and distributed small gifts to those who completed the survey and interview. A total of 111 participants over 50 years old (41 offline and 70 online) completed the survey.
The details of the research are as follows. At the beginning of the research, the subjects were asked about the frequency that they paid attention to health information and whether they used MHE apps. The frequency of health information attention is divided into four parts: barely pay attention (less than once a month), occasionally pay attention (monthly or when needed), frequently pay attention (weekly or regularly active) and daily pay attention. This study classifies the frequency of MHE app use among older adults according to the stage of behavioral transition. According to our study, older adults in the pre-contemplation and contemplation stage usually never used MHE apps. Those in the preparation and action stage reported that they occasionally used MHE apps, but had difficulty maintaining long-term use. And those in the maintenance stage were used to using MHE apps and used MHE apps regularly within 6 months.
The subjects were then invited to view all the persuasive strategy cards. Researchers explained the meaning and function of the 13 persuasive strategies and showed examples from apps so that the subjects clearly understood the meaning of each strategy. Then the subjects were asked to rate the strategy based on the questions in Table 2. This score was used to measure the susceptibility of each persuasive strategy.
Study structure and content.

Our research questions were selected from an adapted version of the susceptibility scale. 44,46 What’s more, the study has shown that usage intention can further validate user ratings. 45 Therefore, we included the subjects’ intention to use as the fifth question. We used a 5-point Likert scale to measure subjects’ ratings of susceptibility to the persuasion strategy (“1” for totally disagree; “5” for strongly agree). 47
This study conducted a descriptive statistical analysis of the basic information of the participants. The basic information of the participants mainly included age, gender, degree of attention to health information and usage frequency of the MHE app. The sample information obtained is shown in Table 3.
Socio-demographic data of the participants.

A total of 120 questionnaires were collected, with a valid sample size of 111. The gender ratio of the participants was more even, with 59 women (53%) and 52 men (47%). The statistics of participants’ attention to health information are: never pay attention to health information (7%), occasionally pay attention (23%), often pay attention (50%), and pay attention every day (20%). The frequency of participants using MHE apps was: never (27%), occasionally (38%), and frequently (35%).
Results
This section presents the results of our data analysis, including the mean rating and repeated measure analysis of variance (RM-ANOVA) for the 13 persuasive strategies.
Measurement reliability analysis
Before conducting the data analysis, the reliability and validity tests of the questionnaire were first conducted with SPSS 27. The Cronbach alpha coefficient is 0.915, indicating that the questionnaire has high reliability. 48 The validity of the questionnaire was tested by Bartlett’s spherical test. The KMO was 0.894, and the p-value was less than 0.05. The results of the analysis showed that all data met the reliability requirements.
Overall average ratings of persuasive strategies
The mean values of the overall ratings of the older participants’ susceptibility to health persuasive strategies are shown in Table 4. The means for all 13 persuasive strategies were above the median, indicating that older adults had positive evaluations of these persuasive strategies. The three strategies “reduction” (M = 4.05), “simulation” (M = 4.02) and “suggestions and reminders” (M = 3.90) had a greater impact on older adults. In contrast, “social role” (M = 3.34) and “reward” (M = 3.06) had lower mean scores, indicating that older adults are less likely to be influenced by these two strategies.
Means and standard deviations of susceptibility for the 13 strategies.

M = means, SE = standard error mean, SD = standard deviation.
Influences and susceptibility analysis of persuasive strategies
Research showed that different individuals respond differently to persuasive strategies. 20 A persuasive strategy that positively motivates one type of person may also be counterproductive for another type. 21 To analyze the sensitivity of elderly subjects to persuasive strategies in terms of four elements (age, gender, health information attention, and frequency of MHE app use), this paper performed a RM-ANOVA on the data using SPSS. Gender, age, health consciousness, and usage frequency of MHE apps were used as between-subject factors, and 13 persuasive strategies were used as within-subject factors. The results of the analysis are as follows.
Effect of gender on susceptibility to persuasive strategies
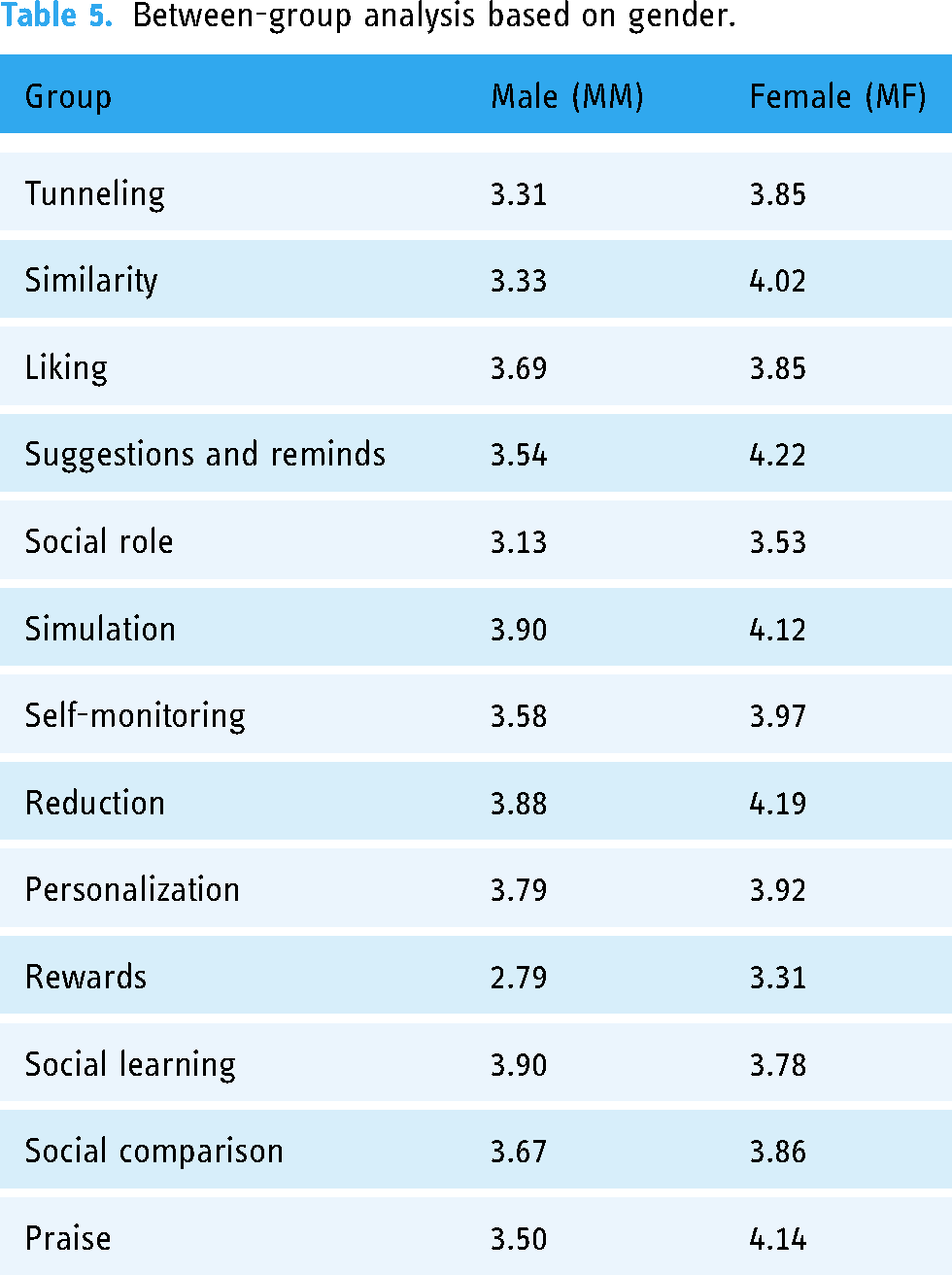
Figure 3 shows the mean rating for persuasive strategies based on gender, while Table 5 shows the result of the RM-ANOVA. The findings indicate that gender has a significant effect on susceptibility to persuasive strategies (Pillai’s trace = 0.221, F (1, 111) = 2.115, p = 0.020 < 0.05), and that females are more susceptible to most persuasive strategies. In the 13 strategies tested, the three persuasive strategies of “similarity,” “suggestion and reminder,” and “praise” have the greatest differences in susceptibility between male and female subjects, and the means were greater for females than for males. Only “social learning” is a strategy that affects males more than females.

The effect of gender on susceptibility to persuasive strategies.
Between-group analysis based on gender.
Effect of age on susceptibility to persuasive strategies
Subjects were divided into three groups according to age: 51 to 60 years, 61 to 70 years, and 71 to 80 years. Figure 4 shows the mean values of persuasive strategies based on the three age groups, and the results of the RM-ANOVA are shown in Table 6. The results of the multivariate test indicate that the age of older adults did not have a significant effect on the susceptibility to persuasive strategies (Pillai's trace = 0.198, F (1, 111) = 1.249, p > 0.05). This may be since the age distribution of the subjects was concentrated in the older age groups and the age difference in the population was too small. However, the persuasive strategy mean ranking (Figure 4) shows that those aged 71 to 80 years were less susceptible to most persuasive strategies than those aged 51 to 60 years and 61 to 70 years. The influence of the “tunneling” strategy was significantly lower than the central value for those aged 71 to 80. The susceptibility to the “liking” strategy is much higher among 51 to 60 years and 61 to 70 years than among 71 to 80 years.

The effect of age on susceptibility to persuasive strategies.
Between-group analysis based on age.

Effect of health information attentions on susceptibility to persuasive strategies
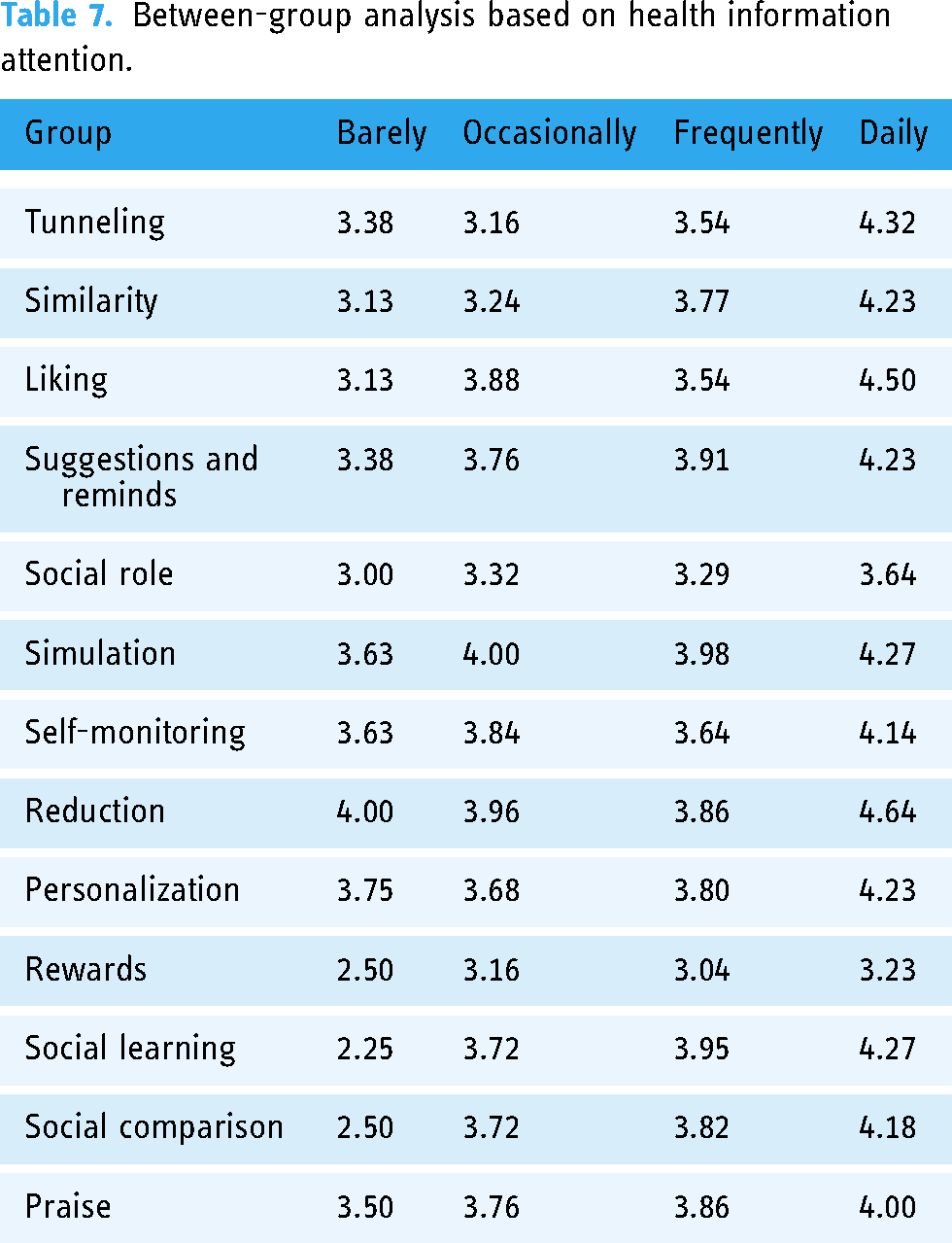
Figure 5 shows the mean scores of the persuasive strategies based on health information attention. The results of the RM-ANOVA in Table 7 indicate that concern for health information has a significant effect on susceptibility to persuasive strategies (Pillai’s trace = 0.518, F (1, 111) = 1.557, p = 0.023 < 0.05). The analysis revealed that those who paid little attention to health information were generally significantly less susceptible to persuasive strategies than those who paid daily attention to health information, while those who paid regular attention to health information did not differ significantly from those who paid occasional attention to health information. The greatest differences in susceptibility to the three persuasive strategies of “social learning,” “liking,” and “social comparison” were found among the four groups of subjects. Figure 5 shows that the “social learning” strategy has the greatest variation in susceptibility for different groups of people. Those who paid attention to health information every day had a much higher susceptibility to the “social learning,” “liking” and “social comparison” strategies than those who paid little or no attention to health information. This suggests that these three persuasive strategies have a greater impact on people who are strongly health conscious.

The effect of different health information attentions on susceptibility to persuasive strategies.
Between-group analysis based on health information attention.
Effect of usage frequency of MHE app on susceptibility to persuasive strategies
Figure 6 shows the mean scores of persuasive strategies based on the usage frequency of MHE apps. The results of the RM-ANOVA in Table 8 showed that the use frequency had a significant effect on the susceptibility to persuasion strategies (Pillai’s trace = 0.418, F (1, 111) = 1.974, p = 0.005 < 0.05). The three persuasive strategies of “social learning,” “social comparison,” and “tunneling” showed the greatest differences in sensitivity among those who used the MHE app with varying frequency. Those who used MHE apps regularly had a much higher susceptibility to the “social learning,” “tunneling,” and “social comparison” strategies than those who never used them. However, occasional users were more sensitive to the “tunneling” and “social role” strategies than never-users and frequent users.

The effect of different usage frequencies on susceptibility to persuasive strategies.
Between-group analysis based on usage frequency.

Discussion
The findings reflect the effects of gender, age, health information attention, and frequency of MHE app use on the sensitivity of 13 persuasive strategies. In this section, we discuss these results in detail.
Effect of gender on susceptibility to persuasive strategies
Abdullahi et al. 37 concluded that there are differences between male and female responses to persuasive strategies, revealing the relative effectiveness of persuasive strategies. 38 As shown in Figure 3, females typically rated the persuasive strategy higher than males. Female older adults rated reward (FM = 3.31, MM = 2.79) and praise (FM = 4.14, MM = 3.50) strategies with much higher values than males. Our study is consistent with the findings of existing studies.49,50 It is also similar to the results of Abdullahi et al.’s study. 39 They noted that women’s high sensitivity to reward strategies may be influenced by ideology and socio-culture. Females have been found to be more sensitive to reward strategies.37,51 Possible reasons for this are that females have more emotional mechanisms in their brains than males, 52 which may also lead to a greater tendency for females to resort to emotional strategies. 49 In a study promoting physical activity, Busch et al. 53 showed that both the gender of the target audience and the degree to which they described themselves as feminine influenced the effectiveness of persuasive strategies; those with femininity found praise and reward strategies more persuasive. Through a literature review analysis, Li et al. 54 concluded that reward sensitivity is related to cultural differences in social and personal environments. Therefore, we suggest the appropriate use of praise and reward strategies in designs for older Chinese women.
Furthermore, we found that male older adults (MM = 3.90) were more likely to be influenced by social learning strategies than female older adults (FM = 3.78). Existing research has confirmed that men are more likely to learn through interaction with each other. 37 Similar conclusions apply to the elderly. This implies that social learning strategies are more helpful for male older adult health education. Therefore, we suggest that more social learning strategies can be provided for male seniors when designing MHE apps.
Effect of age on susceptibility to persuasive strategies
As shown in Figure 4, the susceptibility of older adults to most persuasive strategies decreased significantly with age. This finding was supported by Johnson’s study, which indicated that the younger the age, the more susceptible they were to persuasive strategies. 55 The highest susceptibility scores for reduction strategies (M = 4.05) were found in the 71- to 80-year- olds. This may be due to the declining physical fitness, cognitive level, and energy of senior citizens resulting in their decreased receptivity to information. According to a study, seniors in the age range 65 or older, each additional year is 8% less likely to use the Internet. 56 By using the reduction strategy to reduce complex information and present the main information directly to the elderly, it is beneficial for the elderly to receive health information. Therefore, we believe that reduction is the most appropriate strategy for older adults aged 71 to 80 years to achieve their goals.
In addition, our findings also indicated that the susceptibility scores to social roles (M = 3.34) and reward strategies (M = 3.06) were generally lower in the elderly of all ages. Some elderly people mentioned “distrust” many times when talking about social roles and reward strategies. This evaluation is confirmed by the research of Poulin et al. 57 They proposed that elderly adults are more sensitive to credibility. Due to a high level of defensiveness, it is difficult for older adults to be impressed by social roles in MHE apps or by common reward strategies. Therefore, we suggest that personalized reward strategies could be used appropriately to meet the different needs of older adults.
Effect of health information attentions on susceptibility to persuasive strategies
As shown in Figure 5, older adults who paid little attention to health information generally had lower rating values for the 13 persuasive strategies, and even lower than median values for the reward (M = 2.50), social learning (M = 2.25), and social comparison (M = 2.50) strategies. However, the rating values for the reduction (M = 4.00) and personalization (M = 3.75) strategies were relatively high. Since these elderly people rarely pay active attention to health information, the two strategies can reduce the complicated information and present the important content to the users. Therefore, the reduction and personalization strategies should be used for older adults who pay little attention to health information.
In addition, we found that older adults who occasionally paid attention to health information had higher susceptibility scores for the simulation (M = 4.00), reduction (M = 3.96), like (M = 3.88), and self-monitoring (M = 3.84) strategies. Possible reasons are because older people who occasionally follow health information rarely have their own regular health information search platform, they are more likely to be attracted to concise and engaging content. In addition, because they have not yet developed the habit of following health information, they need to rely on external motivation to motivate their behavior and typically tend to accept strategies such as self-monitoring and simulation. Therefore, the use of these persuasive strategies can attract older adults at the beginning of use (liking, reduction, simulation) and motivate continued use (self-monitoring). In contrast, older adults who paid attention to health information frequently had lower susceptibility scores for liking (M = 3.54), reduction (M = 3.86), self-monitoring (M = 3.64), reward (M = 3.04) and simulation (M = 3.98) strategies than those who followed occasionally. The possible reason is that frequent followers have formed personal health information search and browsing habits. The need for these persuasive strategies to attract or stimulate use has decreased. For this reason, we suggest that for older adults who follow health information occasionally, liking, reduction, and simulation strategies can be used to attract them to follow health information. For those who follow health information frequently, more targeted persuasive strategies such as simulation, suggestion and reminder, social learning, and praise can be used to help them achieve their goals.
Finally, we also found that older adults who paid attention to health information every day generally had higher rating values for the 13 persuasive strategies. This implies that the frequency of paying attention to health information largely influences older adults’ susceptibility to persuasive strategies. Those who paid attention to health information every day have stronger health awareness and were more receptive to health information. Thus, they were more willing to receive health education. This result suggests that the frequency of health information attention among older adults has a positive effect on the susceptibility to persuasive strategies. We suggest that reduction, liking, and tunneling can be used to further enhance the user experience of older adults who pay attention to health information every day.
Effect of usage frequency of MHE app on susceptibility to persuasive strategies
The usage frequency of MHE apps among the elderly is divided into three stages: never use, occasional use and frequent use. The frequency of use reflects the process of change in older people’s behavior towards MHE app use. As shown in Figure 6, since no consideration will be given to starting healthy behaviors, the susceptibility to 13 persuasive strategies among the older adults who never used MHE apps was generally lower than those who used the MHE app frequently and occasionally. 58 According to interviews, older adults feel some concern and fear about learning to use new health apps. Older adults are often considered to be the most difficult population to use digital technology. 59 Due to physical limitations, older adults have four ageing process barriers (cognition, motivation, physical ability, and perception). They are often afraid to experiment with mobile devices and applications, thus potentially limiting their effective and satisfactory use of mHealth.60,61 Nevertheless, older adults who never used MHE apps had relatively higher susceptibility ratings for the reduction (M = 3.73) and simulation (M = 3.67) strategies. Reduction strategies can reduce the difficulty of use for older adults through rationalization of visual presentation and enhanced feedback.61,62 Simulation strategies can demonstrate behaviors and possible outcomes to older adults in advance and enhance their sense of control when using MHE apps. Therefore, we recommend that reduction and simulation should be used for older adults who have never used a MHE app.
Older adults who occasionally used MHE apps had higher susceptibility scores for suggestions and reminders (M = 4.14), social learning (M = 4.10), and reduction (M = 4.10) strategies. Since this group of older adults is in the preparation and action stage, they have not yet formed long-term habits of use. 63 Therefore, there is a need to provide triggered strategies for older adults who occasionally use health apps. The above persuasive strategies are suggested to be used in the design to promote users’ motivation to use the MHE app.
The older adults who frequently used MHE apps rated higher on the susceptibility of social comparison (M = 4.33) and social learning (M = 4.23) strategies. Possible reasons for this are, first, those older adults in the maintenance phase have developed the habit of using MHE apps. This behavior has been translated into the subconscious and no longer requires excessive external reminders. Secondly, since they are already familiar with the basic functions of the app, they do not need much operational prompting or guidance. Third, the social interaction strategy of the MHE app can meet the social needs of the elderly. Social comparison and social learning strategies help to increase the engagement of older adults through collective communication and learning. Effective user engagement can increase loyalty to mobile apps and thus consolidate health behaviors of older adults. 64
This study found significant differences in the persuasion strategies preferred by older adults at different stages of use. Therefore, to improve the effectiveness of persuasion strategies, we suggest using different persuasive strategies at different usage stages according to the usage frequency of MHE apps. There is a huge gap between the wide availability of e-health resources and the skills of older adults to use them effectively due to the digital divide. 65 The lack of technological knowledge and the “fear” of adverse effects of misuse among older adults often makes them hesitant to use mobile technology. 66 For older adults who never use MHE apps, reduction and simulation strategies are recommended to reduce the difficulty of using and help them overcome their fear of technology.59,60,65,66 For older adults who occasionally use MHE apps, suggestion and reminder, social learning and reduction strategies are recommended to encourage them to participate in activities on MHE apps. And for older adults who use frequently, social comparison and social learning strategies are recommended to increase their interest in the product, which leads to long-term usage behavior.
Conclusion
In this paper, we analyze the sensitivity of older adults to 13 persuasive strategies using RM-ANOVA and propose personalized persuasive strategies for the design of MHE apps for older adults. The innovation of this paper is to analyze the effects of gender, age, health information attention and frequency of use of older adults on the sensitivity of persuasive strategies by combining the TTM. The main contributions of this paper are as follows. (1) When designing MHE applications for older adults, we should consider the influence of gender, user health information concerns, and frequency of use when selecting persuasive strategies. (2) For seniors who rarely pay attention to health information, reduction strategies and personalization strategies are recommended. For older adults who occasionally pay attention to health information, liking, reduction and simulation strategies are suggested to attract them to pay attention to health information. While for those who pay attention to health information frequently, persuasive strategies such as simulation, social learning, suggestion and reminder, and praise are more beneficial for them to maintain their usage habits. For seniors who are concerned about health information on a daily routine, strategies such as reduction, liking and tunneling strategy are recommended. (3) When older adults are at different usage frequencies of MHE apps, their preferred persuasive strategies also differ. For those who have not used MHE apps before, reduction and simulation may quickly teach them how to use them. For those who are familiar with the basic operation of MHE apps but use them occasionally, suggestions and reminders, social learning, and reduction strategies will attract them to increase the frequency of use. For older adults who use the MHE app frequently, the use of social comparison and social learning strategies can further increase user engagement and maintain their long-term usage behavior.
We conclude that older adults have different sensitivities to persuasive strategies in different contexts of using MHE applications. The results of this study can be applied to other health apps designed for older adults to promote their usage behavior. With the ageing population and the global pandemic of COVID-19, the Internet has become the primary channel of connection for all aspects of life, and eHealth literacy among older adults has become more important than ever. 67 Mobile health and health apps have been effective in improving patient health literacy. 68 This paper suggests that the persuasive strategies used to design health apps should refer to the sensitivity of older adults to persuasive strategies in different use situations. Designing more persuasive MHE applications will provide a useful addition to health education for older adults and make the dissemination of health information more efficient. The results of this study will likely have a positive impact on improving health literacy and expanding the reach of digital health education for older adults.
There are three limitations in our study. First, the older adults’ ratings of persuasive strategies in this study were based on their personal app user experience and persuasive strategy cards. This is somewhat different from the experience of using real mobile devices. Secondly, the subjects in this study were all older adults from coastal cities in China. This factor does not guarantee that the results of our study will remain generalizable to other regions of the elderly population. Third, the target group of this study mainly considers the situation in China, and only older people aged 50 to 80 years with experience in using mobile apps were selected to participate in the experiment. Because seniors over the age of 80 may respond differently to persuasive strategies, we will do more research on this group in our future work. We will do further validation in future studies by expanding the number of study participants and simulating their use in real applications to expand the applicability of this study.
Footnotes
Acknowledgement
The authors are grateful to the interviewees for their willingness to participate in the study.
Contributorship
YG conceptualized the study design. TW, SY, XZ and KH recruited and enrolled participants during the study. TW and SY conducted the data analysis. YG, TW, SY, and XZ wrote the first draft of the manuscript. YG and TW edited and reviewed the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained by East China University of Science and Technology (approval number: ECUST-2022-071).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education Humanities and Social Sciences Foundation of China. (Grant number 17YJCZH055).
Guarantor
YG.