
Abstract
Objective
The shortage of pathologists is a worldwide problem that is more severe in Africa. One of the solutions is the use of telepathology (TP); however, most of the TP systems are expensive and unaffordable in many developing countries. At the University Teaching Hospital of Kigali, Rwanda, we assessed the possibility of combining commonly available laboratory tools into a system that can be used for diagnostic TP using Vsee videoconferencing.
Methodology
Using an Olympus microscope (with a camera) operated by a laboratory technologist, histologic images were transmitted to a computer whose screen was shared, using Vsee, with a remotely located pathologist who made the diagnoses. Sixty consecutive small biopsies (≤6 glass slides) from different tissues were examined to make a diagnosis using live Vsee-based videoconferencing TP. Vsee-based diagnoses were compared to pre-existing light microscopy-based diagnoses. Percent agreement and unweighted Cohen’s kappa coefficient of the agreement were calculated.
Results
For agreement between conventional microscopy-based and Vsee-based diagnoses, we found an unweighted Cohen’s kappa of 0.77 ± 0.07SE with a 95% CI of 0.62–0.91. The perfect percent agreement was 76.6% (46 of 60). Agreement with minor discrepancy was 15% (9 of 60). There were 2 cases of major discrepancy (3.30%). We were unable to make a diagnosis in 3 cases (5%) because of poor image quality related to the instantaneous internet connectivity problems.
Conclusion
This system provided promising results. However, additional studies to assess other parameters which can affect its performance are needed before this system can be considered an alternative method of providing TP services in resource-limited settings.
Introduction
Telepathology (TP) can be defined as an act of providing pathology services at a distance using any form of telecommunication system. 1 Despite that shortage of pathologists is a worldwide issue, Rwanda like many African countries suffers more from a lack of sufficient pathologists and pathology services compared to the rest of the world.2–5 One of the solutions to that shortage is the use of TP.2,6,7 Particularly in developed countries, the TP system has enabled improvement of not only pathology services but also pathology education, research, quality improvement, improved cancer care, improved tumor board discussion, improved surgical care by access to pathology intraoperative consultation in remote areas without pathologists, access to a second opinion in a short time and continuous medical education.7–9
With the continued evolution of telecommunication techniques, recently pathology informatics and digital pathology recognized tremendous applicability and development. 10 Hence, TP services can be offered in different forms using a mobile phone, web, internet-based technology, and other means of information transmission. Different platforms in current use are classified as static TP, dynamic TP, hybrid (static and dynamic) TP, whole slide imaging (WSI), and dual dynamic-WSI TP.6,7
The basic requirements for TP are either a microscope (motorized for dynamic TP) with an attached high-resolution camera or a WSI system. Additional requirements are internet access or a video/image transmission system, and a TP workstation with a screen or monitor to remotely display/project the image captured by the camera or WSI system.11,12 But, depending on the type of the TP system, some of these components may not be needed.12,13 Consequently, the cost, as well as the effectiveness of TP systems, have a wide range of variability.7,12 The capital expenditure can be as high as USD 100,000 to USD 130,00013,14 in the case of TP using WSI or robotic microscopy. The cost may amount to USD 6500 if only a modular hardware platform with integrated digital pathology software applications is needed. 15 On the other hand, using equipment already present in most pathology laboratories (microscope, image acquisition software, and transmission hardware), the capital expenditure can be as low as less than USD 1000–4000 if only a microscope camera is needed.13,16
Above the capital cost, the maintenance and running costs will depend on the system in use. For the WSI, the service contract was reported to be USD 4500 in Malawi. 13 The robotic dynamic TP will require a broadband internet connection of up to 2000 kilobits per second (kbps) or higher which cost more than low bandwidth. 12 On the other hand, some videoconferencing TP-based systems have been reported to be effective for an internet connection of 384 kbps. 17
The comparability of different platforms or different studies is very difficult since the available literature has evaluated different variables or used different methodologies. Bushshur et al. 7 provided an extensive list of literature related to TP. The holistic evaluation of the TP system can be challenging. This may be due to the complexity of its components and different parameters (hardware, software, accuracy in the diagnosis, quality of images and sound, acceptability of the system by the end users, etc.) to be assessed. Most importantly, the acceptability of any TP system will depend on the user-friendliness of the system, quality and speed (of both sound and images), and the accuracy in the diagnosis compared to conventional light microscopy.
Rwanda with a population estimated at 12.7 million in the year 2020 18 has <20 general pathologists distributed in five hospitals. Based on our personal experience, sometimes difficult cases from all around the country that require sub-specialization consultation are referred to Butaro Cancer Center of Excellence (BCCOE) where using static or WSI TP19,20 a teleconsultation from abroad is performed. The aim of this study was to evaluate the feasibility of establishing a low-cost TP system for diagnostic pathology with the possibility of serving in low-resource settings communities.
Materials and method
Study site
Our study site was the University Teaching Hospital of Kigali (CHUK, a French acronym), the largest teaching and tertiary level hospital in Rwanda, with a 519-bed capacity, located in Nyarugenge District, City of Kigali, the capital of the Republic of Rwanda. 21 The pathology department at this hospital has five anatomic pathologists and processes around 3500 biopsies and 1000 cytology specimens per year. Contrary to some developed countries with a considerable number of pathologists, the practice of pathology is not based on subspecialty. Therefore, the pathologists will be required to examine any type of issue brought to their attention.
Experiment settings
Onsite (hospital) hardware and software for TP diagnosis
Histologic glass slides were examined using a trinocular microscope (Olympus, Japan) with an attached DP74 microscope camera (Olympus). Images from the microscope were transmitted to a desktop computer using CellSens (Olympus corporation) imaging software. The desktop screen (displaying the image from the microscope) was shared with the pathologist located abroad (Japan) using the free-of-charge version of the Vsee application (Vsee Lab Inc., Sunnyvale, CA). This application is a low bandwidth videoconferencing application that allows free video calls of up to 10 people/partners (computers or videoconferencing sites) and is Health Insurance Portability and Accountability Act compliant. 22
Hardware and software used by the pathologist for Vsee-based TP
Personal computer laptop (Toshiba/Dynabook, Intel core i7, central processing unit 1.80 GHz, 16.0 GB Random Access Memory, 64-bit Operating System) and internet connection using Wi-Fi, and free-of-charge version of Vsee videoconferencing application.
Histologic cases analyzed
Consecutive sixty small biopsies (≤6 glass slides) from different tissues, with pre-existing light microscopy-based acceptable image quality and diagnosis made in 2019, were retrieved and examined in June–August 2020 using Vsee videoconferencing-based TP. The pathologist was blinded to the pre-existing diagnosis.
Procedure for evaluation of glass slides using Vsee videoconferencing-based TP
A former CHUK pathologist with 3-year of experience in pathology practice was located in Japan during this experiment and served as the Vsee-based TP diagnostician pathologist.
An experienced histotechnologist (with 8 years of histotechnology practice) was located at CHUK, Rwanda, and participated in this experiment. Eight live videoconference sessions of Vsee-based diagnostic TP were done between June and August 2020. The duration for each session was 45 to 60 min. During each session, six to nine cases were examined.
The technologist presented clinical information for each case to be analyzed and put the corresponding glass slide on the stage of the microscope with a digital microscope camera connected to a desktop computer. The technologist was moving the stage holding the glass slide as needed and/or guided by the pathologist. The image was transmitted and displayed on the computer screen. The computer screen was shared with the pathologist using Vsee, and finally, the pathologist made a diagnosis. At the time of the image quality problem due to image transmission over the internet, the pathologist waited for a moment <10 min to see if the problem was resolved. In case the issue persisted for more than 10 min, the session was terminated, and the case was reported as “non-diagnostic” due to poor image quality. The next session started with the next case.
Recording for histologic images
To record the image received on the telepathologist computer screen, the Snipping Tool of Microsoft Windows was used. The obtained images were saved in a word document.
Data analysis
The diagnoses made using a Vsee videoconference-based system were compared to the diagnoses made using light microscopy. As suggested by McHugh, 23 we calculated both percent agreement and Cohen's kappa. For percent agreement, our diagnoses were classified into one of four categories: perfect concordance, concordance with minor discrepancy, major discrepancy, and no diagnosis. A minor discrepancy was defined as a difference in further qualification or grading of the diagnosis and has no or little effect on the management of the patients. The major discrepancy was defined as totally different diagnoses (which may lead or not to different management of the patient). The percentage was calculated by multiplying the number of cases in each category by 100 divided by the total number of cases examined. To calculate Cohen’s kappa, each diagnosis was classified into one of five diagnostic categories (see Table 1). After categorization unweighted Cohen's kappa was calculated using VassarStats 24 an online website for statistical computation.
Diagnostic categories for classification of diagnoses for Cohen's kappa statistics.

Ethical approval
This study has been approved by the Institutional Review Board (IRB) of the College of Medicine and Health Sciences (CMHS), University of Rwanda (Approval Notice No. 006/CMHS IRB/2020) and the Ethics Committee of the University Teaching Hospital of Kigali (Review Approval Notice No. Ref.:EC/CHUK/062/2020).
Results
Agreement between conventional microscopy- and Vsee TP-based diagnoses
The 60 cases examined using Vsee-based TP together with their corresponding diagnostic categories are provided in Table 2.
List of light microscopy-based and Vsee-based diagnoses and their diagnostic categories.

*Each code is made by two digits: the first digit is for the light microscopy diagnostic category and the second is for the Vsee-based diagnostic category.
We found substantial agreement between light microscopy-based and Vsee-based diagnoses with an unweighted Cohen’s kappa of 0.77 ± 0.07 and 95% CI [0.62–0.91]. The results for percent agreement are presented in Table 3
Percent agreement between microscopy-based and videoconference-based diagnoses.

n: number of cases.
The quality of histologic images received by a remotely located pathologist using our Vsee-based TP system
For all cases for which the pathologist was able to make a diagnosis using Vsee-based TP, their images had good to high quality as shown in representative examples in Figure 1. In contrast, Figure 2 shows microscopic images with different quality issues. In the case of the poorest image quality (which was infrequently occurring), the pathologist could not be able neither to recognize the tissue organ nor make the diagnosis for that case.

Good quality hematoxylin and eosin-stained microscopic images capture at a distance using our telepathology system: (A) breast fibro adenoma, (B) lipoma, (C) benign nasal inflammatory polyp, (D) invasive breast ductal carcinoma, high grade, (E) invasive squamous cell carcinoma of the cervix, and (F) breast tissue with inflammation.
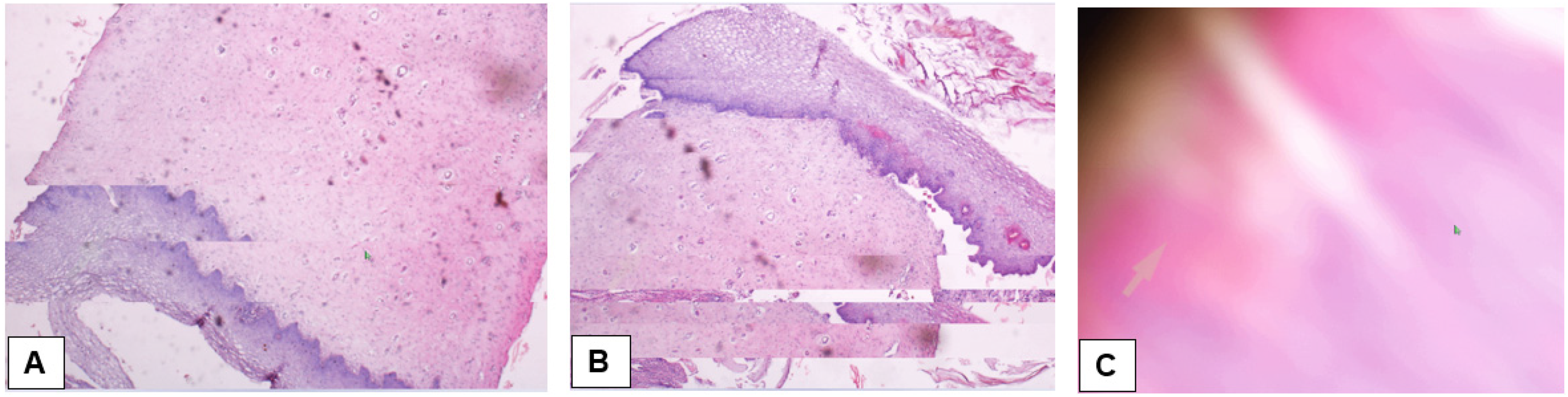
Illustrative examples of images with quality issues: (A) Image with subtle defect well seen at the left side, the middle part of the image; (B) image with defects in the entire lower one-third part of the image; and (C) image of poorest quality due to more severe poor internet connectivity.
Discussion
Different authors recorded different rates of concordance between conventional light microscopy-based and TP-based diagnoses. 7 We found a kappa of 0.77 which is comparable to kappa values reported in different studies. For example, Thrall et al. 25 reported a K = 0.8, Papathomas et al. 26 a K = 0.73 in two tiers and K = 0.65 in three tiers, and Gage et al. 27 a K = 0.6–0.7. Our overall diagnostic concordance rate of 91.6% (perfect concordance of 76.6% plus concordance with minor discrepancy of 15.0%) was comparable to findings of other studies.16,19,28,29
Das et al. 30 using WhatsApp® for TP reported that the telepathologist was able to make a diagnosis in 70% of cases for which 13% was a confirmed diagnosis while 57.7% was a probable diagnosis. In contrast, our Vsee-based TP system was able to provide a diagnosis in 91.6% of cases, whereby perfect diagnosis was rendered in 76% of cases compared to conventional light microscopy. In only 3 cases (5%), we were unable to make a diagnosis due to the poor quality of the images received by the telepathologists.
The poor image quality in our system was of two types. The first type consisted of stationary or freeze images on the telepathologist’s side, where the images did not move while the glass slide was moved under the microscope. The second type consisted of blurred images (as in Figure 2C), where the pathologist considered that the best option was not to make a diagnosis for the concerned case. In fact, the poor quality of the images may be attributed to internet connectivity problems, which we were not able to investigate further in this study. Jones et al. 31 explained that different internet connection parameters, such as bandwidth, latency, and packet loss, influence the quality of video conferencing experience, and that long delays and degradation in video quality could be attributed more to latency than to other parameters.
In our study, the perfect concordance rate—without any discrepancy—was 76.6%. Thrall et al. 25 during the validation of WSI found an interobserver agreement of 79%. The high rate of discordance was attributable to a minor discrepancy (15.0%) which was mostly noted within the non-neoplastic conditions, similar findings were reported elsewhere.29,32 We reported a 3.3% rate of major discrepancy. This is comparable to a major discrepancy rate of 5.4% reported by Jones et al. 33 in their study assessing inter-institutional teleconsultation using WSI. Sirintrapun Cimic 16 have argued that “not having a skilled driving pathologist providing context and showing critical regions of the slide would theoretically lower the concordance rates.” From their point of view, we have to mention that in our study, the laboratory technologist rather than a pathologist, was driving the microscope. Hence, we can argue that the concordance rate in our study could have been different if the driver of the microscope was a pathologist who can assist in choosing a more representative diagnostic area.
One benefit of our system is that it does not require the acquisition of new hardware or a working platform. We just operated it as a plug-in-and-play model as the required hardware was already available at our facility and this can be available in many of the existing histopathological facilities. This modality does not require any additional contract maintenance fees from a third party. Therefore, the use of Vsee for teleconsultation would be a good alternative for a WSI system or dynamic TP system using a robotic motorized microscope which is expensive and cannot be affordable for many developing countries. 2 Our system requires a microscope, a microscope camera, an internet connection, a pathologist, and a lab technologist/pathologist. In regard to instruments' capital cost, if the three elements (microscope, camera, and internet access) are already available at the facility, this capital cost would be very low. If none of those materials is available, the initial cost can range between USD 5000 and USD 25,000. 34 Of note is that the cost for WSI or static or dynamic robotic motorized TP system would cost several thousands of USD as more than USD 100, plus monthly or yearly service contract fees of around USD 5000.2,13,14 Additionally, this system can allow a quick consultation by pathologists even if they are out of their work site in the case a situation demands as long as they are near a computer with internet access. That is a solution for hospitals that have only one pathologist or in case a second opinion is required from another pathologist located at a different site. This teleconsultation can offer instant discussion and coaching of less experienced pathologists or pathologists without a particular sub-specialization to be able to use the system to consult peer pathologists.
Despite that most TPs that use a camera coupled to the microscopy are classified among static TP systems, 12 we argue that our system should be viewed as a real-time dynamic system as Sirintrapun and Cimic 16 and Orah and Rotimi 2 have considered TP system using desktop sharing videoconference application among a live dynamic model of non-robotic TP. Nevertheless, our TP system is totally different from both robotic TP- and WSI-based TP. The most important downside of this system is that the telepathologist will depend on the second person to drive the microscope. This dependency may limit the area of the glass slide examined by the pathologist, with a possibility of missing the diagnosis in case the diagnostic area is not shown to the pathologist. We expect that with proper training, these drawbacks can be minimized.
Limitations
Cases under investigation in this study were reviewed by only one pathologist using our proposed TP system. Additionally, the fact that the Vsee pathologist had only 3-year of pathology practice, might affect the accuracy of diagnosis compared to a more experienced pathologist. Our study did not evaluate the cost that can be associated with increased use of internet and electricity nor has evaluated the capital expenditure of establishing a new TP system in case none or some of the basic requirements for this TP system are not available. Furthermore, we did not investigate internet connectivity factors that caused problems in cases for which we did not provide a diagnosis. We expect that further studies will explore these problems. Moreover, we did not include cases stained with immunofluorescence, immunohistochemical and histochemical (special) stains.
Conclusion
Our TP model based on the Vsee application provided promising results. The ability to use already existing infrastructures with the addition of less costly material could help many healthcare organizations with limited financial and qualified health personnel to have access to pathology services using an affordable, real-time model of TP. However, further studies are needed to evaluate other factors that can affect the effectiveness of this system before it can be considered an alternative method of providing TP services in resource-limited settings. The factors for further evaluation may include internet quality and cost and the efficacy of this system for use in particular circumstances such as special stain and immunofluorescence staining.
Footnotes
Acknowledgements
We would like to thank Kellen Kyomugisha for her administrative assistance and Marceline Uwase for her technical assistance.
Contributorship
FM and JPN contributed to conceptualization, methodology, formal analysis, and project administration. FM wrote the first draft of this manuscript and obtained ethical approval. TH and JBS contributed to data acquisition and critical review of the manuscript. BR and EN contributed to data analysis and critical reviewing of the manuscript. All authors reviewed, edited, and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study has been approved by the IRB of CMHS, University of Rwanda (Approval Notice No:006/CMHS IRB/2020) and the Ethics Committee of University Teaching Hospital Kigali (Review Approval Notice No. Ref.:EC/CHUK/062/2020).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
FM.
Informed consent for participation
Not applicable.
Consent for publication
Not applicable.
Trial registration
Not applicable.
Availability of data and materials
All raw data that support the findings of this study are available from the corresponding author upon reasonable request.