
Abstract
Objective/Background
Telepathology has been widely adopted to allow intraoperative pathology examinations to be performed remotely and for obtaining second opinion teleconsultation. In the Italian northern region of South Tyrol, the widespread geographical distances and consequent cost for the health system of having a travelling pathologist cover intraoperative consultations in peripheral hospitals was a key driver for the implementation of a telepathology system.
Methods
In 2010, four Menarini D-Sight whole slide scanners to digitize entire pathology slides were placed in the peripheral hospitals of Merano, Bressanone, Brunico, and in the hub hospital of Bolzano. Digital workstations were also installed to allow pathologists to remotely perform intraoperative consultations with digital slides. This study reviews the outcome after 12 years of telepathology for this intended clinical use.
Results
After an initial validation phase with 100 cases which yielded a sensitivity of 65% (CI 43–84%) and specificity of 100% (CI 95–100%), there were 2058 intraoperative consultations handled by telepathology. The cases evaluated were mainly breast sentinel lymph nodes, followed by urological, gynecological and general surgical pathology frozen section specimens. There were no false-positive cases and 165 (8%) false-negative cases, yielding an overall sensitivity and specificity of 65% (CI 61–69%) and 100% (CI 99–100%), respectively.
Conclusion
Telepathology is reliable for remote intraoperative diagnosis and, despite technical issues and initial acquaintance issues, proved beneficial for patient care in satellite hospitals, improved standardization, promoted innovation, and resulted in cost savings for the health system.
Introduction
The original definition of telepathology was ‘the practice of pathology at a long distance’, with ‘long distance’ meaning any distance bridged by a telecommunication system 1 which may range from a few meters separating nearby two rooms in the same building to thousands of kilometers between geographically separated institutions. In the last two decades, many experiences regarding telepathology services have been published,2–4 with increasing utilization of whole-slide imaging (WSI) technology for intraoperative consultations by remotely performing frozen sections (FS). The deployment of digital pathology with WSI for telepathology has allowed pathology practices to overcome the constraints of geographical distance among different hospitals within the same health system, or to even connect with collaborators in different countries. Digital pathology was particularly helpful during the COVID-19 pandemic as it remotely permitted continuity of diagnostic anatomical pathology services. 5 Moreover, digital pathology has proven to be beneficial for non-clinical uses such as education and research.6–8
Deployment of digital pathology systems has resulted in cost-savings, 9 despite the expense of acquiring and maintaining this technology. 7 The safety and reliability of digital pathology for clinical diagnostic use has been reported in many published validation studies dealing with different practice settings ranging from general surgical pathology,10–13 to intraoperative services,14–17 and highly specialized fields of pathology including neuropathology,18–20 transplantation pathology,14,21,22 and cytopathology.23–26
More than a decade ago, in the Italian province of South Tyrol, the geographically widespread intraoperative consultation service was reorganized by introducing a digital pathology system to digitally connect different hospitals within the region. This allowed the provincial health system to leverage telepathology in order to provide cost-effective, expert-level service to patients at all local hospitals. Herein, we present the outcome of over 12 years of telepathology use in South Tyrol. This article also discusses the challenges of implementing and sustaining this frozen section telepathology service.
Materials and methods
Background
South Tyrol is the far north province of Italy, with an area of 7398.38 square kilometers, mostly covered by mountains and inhabited by a population of about 535,0000 people. The region is historically at the crossroads between north and south Europe. Most people speak both German and Italian. There is an uneven distribution of the population, with some medium-sized urban centers and a myriad of small settlements in the various valleys. The main hospital of the region is located in the chief town of Bolzano (hub hospital). There are another six community (spoke) hospitals servicing the mountain communities within the districts of Merano, Bressanone, and Brunico (Figure 1, map credit to Ref. 27 ). The main pathology department, located in the hub hospital of Bolzano, gathers all specimens coming from the smaller spoke hospitals so that they can be processed for surgical pathology and cytopathology examination. The hub pathology service employs pathologists with expertise in various subspecialties.

Geographical map of South Tyrol (credits for the map to Ref. 27 ).
Given the geographical setting, there are logistical difficulties for patients to travel to Bolzano to undergo specific surgeries that may need a frozen section performed by a subspecialist pathologist to accurately guide intraoperative surgical management. Prior to deploying a digital pathology solution to overcome this hindrance, the intraoperative service was handled by having pathologists from the hub hospital physically travel with a laboratory technician to the spoke hospital whenever surgery was planned that may need an intraoperative examination. This legacy situation was very time and resource consuming. Travel costs (where an estimated round trip travel time ranged from 50 min to 2.5 h) were covered by the public health system. Moreover, pathologists who traveled to cover the frozen section service could not sign out any other patient cases at these spoke hospital, nor were they available for additional activities in the hub hospital such as participating in tumor boards or helping their colleagues who needed consultation with difficult cases. Notably, the lab technicians who had to also travel to assist with the frozen section procedure were underutilized in this setting. The first attempt to deploy a telepathology system dates back to 2003, with a single spoke hospital using a robotic telepathology system with no slide scanning capabilities. This early robotic microscope was controlled remotely by a pathologist in the hub hospital. Over time, the number of required intraoperative consultations greatly increased. Additionally, as changes were made to the information technology (IT) infrastructure this early deployed system became obsolete. Therefore, in 2010 it was decided to adopt a newer digital telepathology system with whole slide scanning capabilities.
Telepathology system
Workstations (digital cockpit with computer monitor) for pathologists to examine digital slides, as well as a small footprint whole slide scanner to digitize entire glass slides, were located and connected via the Internet in the hub hospital and spoke hospitals of the district towns of Merano, Bressanone, and Brunico (Figure 2). The scanners were D-Sight instruments (Menarini) with five slide capacity and 4×, 10×, 20× and 40× scanning magnifications. The scanner weight was less than 30 kg and only 60 cm in width (dimensions 60 × 40 × 40 cm). Scanning resolution was 0.5 μm/pixel at 20× and 0.25 μm/pixel at 40×. Scanning times was only a few minutes for image acquisition at 20×. Digital slides were in JPEG 2000 format. The workstations included monitors with a 30″ with 2560 × 1600 resolution. For each workstation, a mid-range computer equipped with Microsoft Windows operating system (e.g. Windows XP, updated to Windows 7), there was a 1 Gbps optical fiber internet connection among the hub and spoke hospitals. D-Sight software was installed on the desktop workstation to control the scanner and navigate the image viewer. For data storage and retrieval of images, along with corresponding metadata (e.g. case notes, diagnostic text, technical details of image), a Microsoft SQL server database was installed.
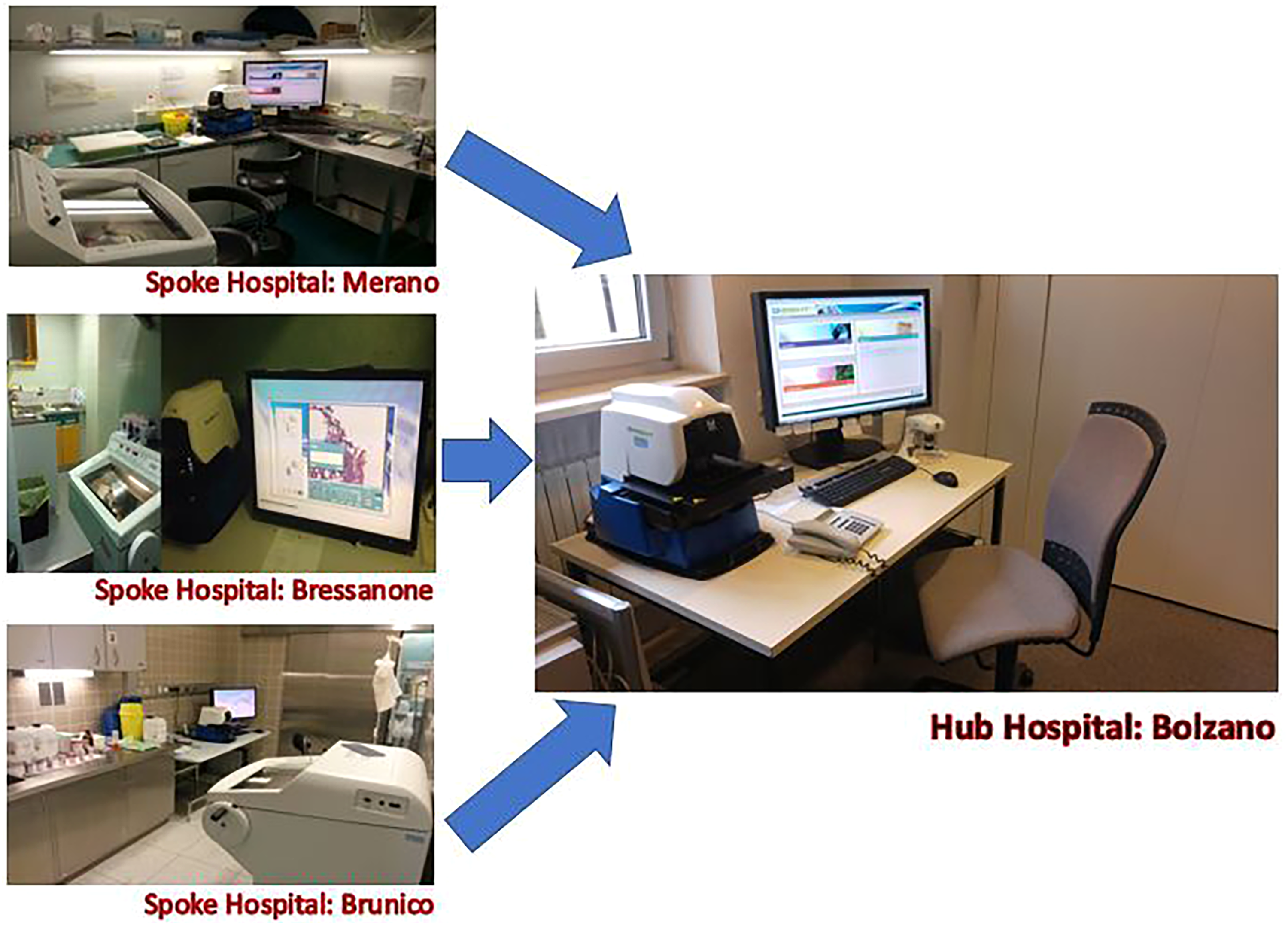
The workstations at the hub hospital of Bolzano (right) and each of the spoke hospitals at Merano, Bressanone, and Brunico. The arrows indicate the direction of image transmission during intraoperative teleconsultation.
Validation and training
All laboratory personnel involved in the on-call intraoperative telepathology service received training. After technical testing and before use in routine activity, the system was validated. The validation study utilized a mixed population of 100 cases chosen to represent the average type of cases likely to be encountered with routine clinical activity. Most of the intraoperative consultations were comprised of breast sentinel lymph nodes (n = 60 cases), followed by urological specimens for margin assessment (n = 17 cases), and a lesser number of other organs (gynecopathology, eight cases; gastrointestinal system, seven cases, peritoneal biopsy, three cases; lung, two cases; thyroid two cases; testis, one case). These cases were collected retrospectively for the purpose of validation and there was a single pathologist involved in validation. Glass slides for the selected cases were digitized and those digital slides were diagnosed first at the hub hospital to test the system, then they were later reviewed (washout time range 2–21 days) using glass slides and a traditional light microscope by the same pathologist, so in this phase a direct comparison between diagnosis on telepathology and diagnosis on glass slide was assessed. Technical problems occurred twice, which were related to inferior internet connectivity. It should be noted that at time of deployment of this telepathology service, no official guidelines on validation had been published, given that the most referenced guideline from the College of American Pathologists (CAP) dates to 2013 28 and newer updated have come further.29,30 Nevertheless, when such recommendations became available in 2013 the system was re-validated on the same case set by another pathologist accordingly to the CAP guidelines, similar to other projects started in the same years. 31
Telepathology workflow
The frozen section rooms in the spoke hospitals are located near the operating rooms. During an intraoperative consultation, in one of these rooms, the surgeon prepares the gross specimen and chooses where to sample, and a lab technician processes the sample to provide FS slides. The technician subsequently loads the slides into an on-site D-Sight instrument to scan them and when scanning is complete calls the on-call pathologist in the hub hospital via a dedicated telephone line. The technician can decide independently to cut a new FS slide if warranted (e.g. deeper tissue levels are needed for microscopic interpretation) or to rescan a slide if the scanned slide is perceived to be out of focus or of low quality. At the hub hospital, the on-call pathologist accesses the dedicated digital cockpit and connects to the spoke hospitals’ D-Sight console to remotely visualize the digitized slide. The pathologist can remotely navigate around the slide (x and y axis) and zoom up to 400× magnification. When the pathologist has established their diagnosis, a full screen image at low magnification of the case is acquired and archived as a small-sized digital file, along with the diagnosis in a repository. The pathologist communicates the FS diagnosis by phone with the surgeon waiting in the spoke hospital. Thereafter, the lab technician in the spoke hospital regains control of the workstation, records the result of the examination, and prepares all the material (e.g. specimen, glass slides) for subsequent delivery to the hub hospital. The FS slide and the cassette with the specimen are sent to the hub hospital, where normal processing to obtain a permanent section is done. The pathologist (in most of cases the same who did the telepathology diagnosis) receives both the original FS glass slide and the new permanent section, together with deeper sections and immunohistochemistry slides in case of sentinel lymph node.
Quantitative analysis
The total number and type of diagnostic intraoperative examinations performed during the 12 years utilizing telepathology were extracted from the pathology information system, together with discordances identified between the FS and final (definitive) diagnosis. A major discordance is defined as a discrepancy that would have changed the patient’s management, while a minor discordance is a discrepancy in diagnosis not resulting in any significant consequence for patient management. A descriptive synthesis of the data is provided highlighting any difficulties encountered, benefits achieved, and the cost-savings of employing digital pathology for this purpose. Concerning the economic issues, we considered in the analysis of cost-benefit on one side the costs of the instrumentations (scanners, workstations, maintenance and assistance); and on the other side, an estimate of the costs of travelling for pathologists and technicians and the indirect costs of pathologists not being able to sign out other diagnosis in the day of intraoperative service in a spoke hospital.
Results
Pilot phase
The overall diagnostic concordance rate (digital vs. glass) was 85% and the Cohen’s Kappa was 0.794 (CI 95% 0.660–0.928). Of the concordant cases, 52 out of 85 (61%) were sentinel lymph node specimens. The deferral rate (to glass slides during final signout) was 5% and deferred cases included two testicular biopsies for malignancy, an ovarian lesion, a lung nodule, and questionable capsular invasion of a thyroid nodule. There were no false-positive cases; no specimens negative for cancer were erroneously diagnosed as positive for cancer by telepathology. There were eight false-negative cases and all were concerned with sentinel lymph nodes with either micrometastases or macrometastases up to 4 mm in size. Altogether, the validation phase yielded a sensitivity when using the telepathology system of 65% (CI 43–84%) and specificity of 100% (CI 95–100%).
Routine service
During the time span of 2010–2021, there were a total of 2058 intraoperative pathology consultations at the three spoke hospitals, all using the telepathology system. This comprised a total of 3078 frozen sections (mean number of sections cut per case was 1.5). The population of cases was as follows: 55% (N = 1129) of these intraoperative consultations involved examination of breast sentinel lymph nodes, 20% (N = 406) concerned evaluation of urological specimens, 9% (N = 190) were gynecological specimens, 9% (N = 191) were gastrointestinal specimens and 3% (N = 51) concerned endocrine organs, while the rest was represented by a miscellaneous quota of other requests to assess for adequacy of tissue material, evaluation of resection margins, diagnose breast or thoracic lesions and examine peritoneal biopsies for carcinomatosis. A graph of case types is reported in Figure 3.
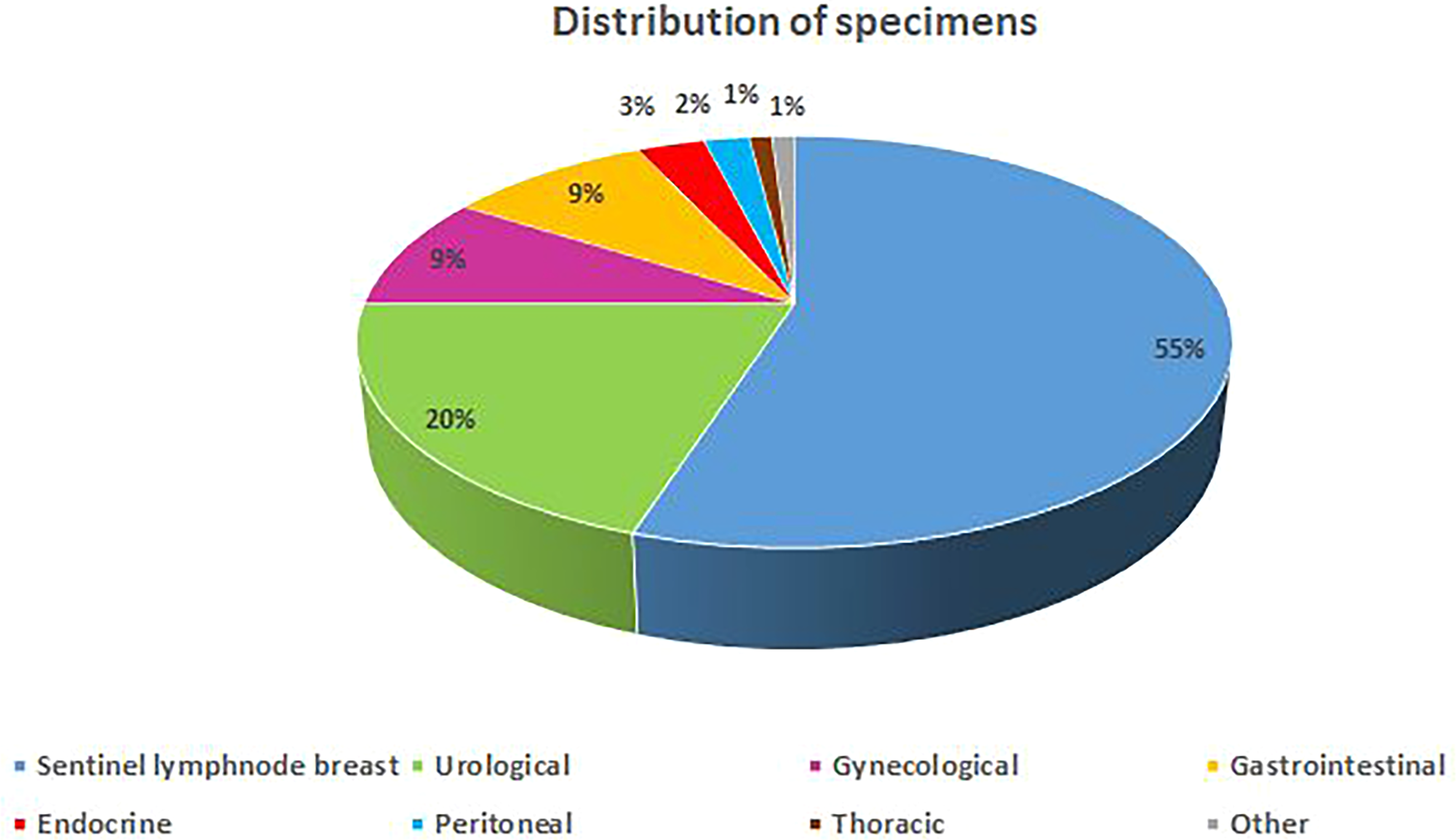
Graphical distribution of case population.
Scanning times ranged from 3 min 57 s to 7 min 45 s (average time to scan a case was 4 min 52 s). The total time for an intraoperative examination ranged from 10 min to 30 min. The time span between diagnosis on FS and definitive diagnosis depended upon organization of routine activity (e.g. subsequent rotation on grossing of case, time for technicians to deliver permanent sections) and ranged between 2 and 10 days. The overall concordance rate was 92% after review of glass slides with a light microscope for a final definitive diagnosis. There were no false-positive cases, but there were 165 (8%) false-negative cases in which cancer was later detected. Therefore, telepathology for overall intraoperative examinations showed a sensitivity of 65% (CI 61–69%) and specificity of 100% (CI 99–10%) with a general accuracy of 92% (CI 91–93%), with Cohen’s Kappa of 0.742 (CI 95% 0.705–0.778). Major discordances for the false-negative cases included misdiagnosis of metastasis in a sentinel lymph node, cancer infiltration in a margin specimen, and presence of high-grade dysplasia. For the assessment of breast sentinel lymph node specimens, the concordance rate was 92% with Cohen’s Kappa of 0.731 (CI 95% 0.679–0.782). Subsequent review of glass slides with light microscope for a final definitive diagnosis revealed no false-positive cases for submitted sentinel lymph nodes, but there were 90 (8%) false-negative cases in which a metastasis was later detected. Therefore, telepathology for sentinel lymph node evaluation showed a sensitivity of 63% (CI 57–69%) and a specificity of 100% (CI 99–100%) with a general accuracy of 92% (CI 90–94%). A representative imagine of paired FS, permanent section and deep stepwise section of a breast lymph node with micrometastasis is shown in Figure 4.
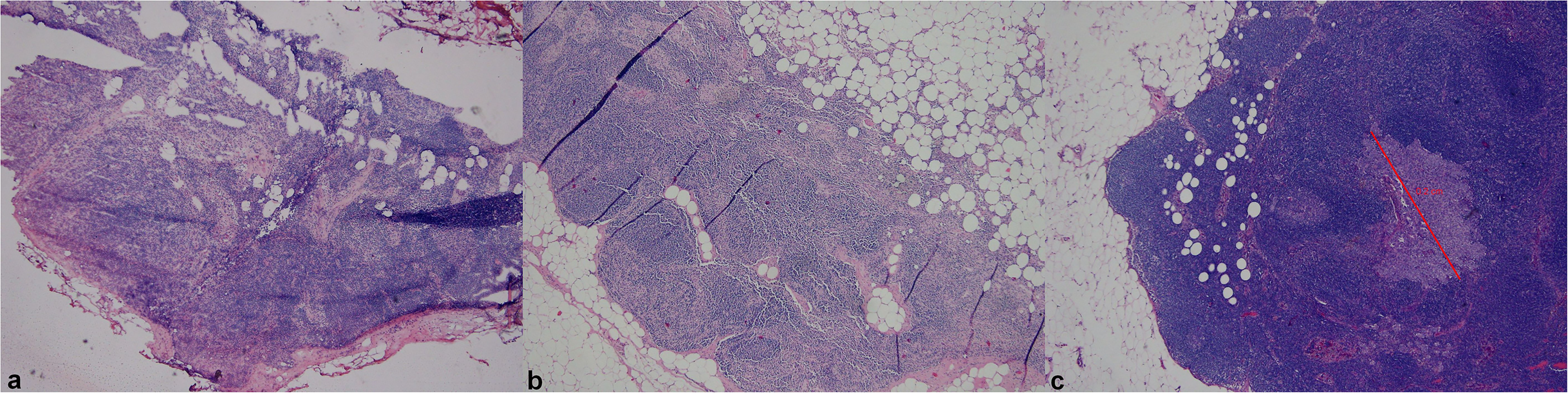
Paired images of a representative case of sentinel lymph node where FS was negative (a), permanent section showed more adipose tissue and histiocytes (b), while a micrometastasis appeared only in a deeper section cut according to sentinel lymph node protocol examination (c).
Estimate of cost-savings
The total cost for the instrumentation (4 scanner, the complete workstations, maintenance, assistance and the time spent on training) was quantified in about 250,000 Euros, with the scanners representing the main expensive part with a little less than 50,000 Euros each. There were expenses for travelling, comprising taxation for autoroutes, fuel, insurance costs for the vehicles property of the hospital trust and their maintenance, and injury and accident insurance of the personnel travelling among hub and spoke hospital on work hours. There was variability in the loans of pathologists and technicians in the time span, but an indirect expense was considered the fact that the pathologist and the technician on the day of intraoperative service were not available to sign out other cases nor preparing other slides, so on a rotation scheme of ten pathologists and technician on a monthly base (weekends excluded) every day they were deployed for less than ten cases. Moreover, if there was a need for intraoperative service at the same time in two spoke hospitals, other pathologist and technician must move from the hub hospital, with doubled costs. Taking these issues into account, a projected saving of about 40,000 Euros per year was estimated, with the offset of the costs after six years of use of the system.
Discussion
The implementation of a telepathology service for intraoperative consultation was a turning point for the delivery of pathology services in the public healthcare network in South Tyrol. This system demonstrated similar results in terms of feasibility, safety and reliability compared with other published experiences around the world, where the barrier of geographical distance was the main stimulus for implementing such a system.4,32–36 Overall, the diagnostic performance of the telepathology system showed a specificity of 100% and sensitivity of 65%, with an overall accuracy of 92%. A major limitation was the limited adherence to evidence-based guidelines for validation,28–30 given that during the initial validation phase the cases were not chosen in a consecutive manner and the washout period (time between digital vs. glass reads) was lower than the two weeks prescribed in the CAP guideline. Nevertheless, the system was since validated according to published CAP guidelines in 2013. We also have to acknowledge that another limitation could be represented by the presence of a comparison of telepathology FS with definitive diagnosis on permanent section, and not with FS on conventional glass slide. Indeed, the instances of discrepancy between FS on telepathology and glass slide were very few, required always the confirmation with permanent section and serial sectioning, and were not collected formally in final reports. This is relevant, as the proportion of errors due to telepathology and not to sampling error could not be assessed, but such an analysis was formally done only during the validation phase, then the system was used routinely without formal reporting of this issue. However, an indirect comparison could be derived from literature specifically analyzing concordance of FS telepathology. 37 Studies with large mixed case populations reported a very high concordance rate (98–99.8%) between digital FS with WSI and FS with glass slide,4,34,38 and this could indirectly indicate that in studies where the telepathology FS is compared with definitive diagnosis like ours the major quota of errors could be due to sampling error of the FS itself. The sampling of specimens is done by the surgeons and not the technicians, and in the majority of cases the specimen was frozen and examined entirely (single lymph nodes, margins, small biopsies); therefore, the quota of sampling error is difficult to quantify and potentially remove. During the study period, several external factors impacted the intraoperative activity. In recent years, the absolute number of intraoperative consultations requested decreased slightly due to a diminished clinical need to examine breast sentinel lymph nodes. Telepathology activity also decreased in the last two years because of the COVID-19 pandemic, during which time major surgeries were delayed or cancelled.
The accuracy or concordance rate appears to be slightly lower than what has been reported in other recent systematic reviews. 37 However, the system in South Tyrol was in use since 2010. Since then, the system software had been updated, but no updates were made to the scanner hardware device or monitors. Newer imaging systems have better cameras and optics to generate high resolution images. This may explain why more recently published studies reported better diagnostic performance. 37 Nonetheless, there are some recently published studies with a similar design as ours with telepathology FS compared to definitive diagnosis on permanent section, showing similar results in terms of overall concordance rate. Interestingly, these studies focus on other specific pathology setting such as pancreatobiliary and liver pathology 39 or lung and thoracic pathology40,41 and show concordance rates ranging 92.9–96.7%. Other recent studies are focused specifically on lymph nodes assessment and show slightly higher concordance rate, but with all the issues of discrepancy concerning indeed micrometastases of breast cancer. 42 Taken together, these comparisons with recent experiences with a similar study design and comparable achievements indicate that our system has shown a non-inferior performance. Most importantly, no false-positive cases were recorded in our study; in other words, no diagnosis of cancer was made via telepathology that was later changed after reviewing the permanent glass slides with a traditional microscope. Thus, there were no instances of overtreatment of patients. Conversely, there were some false-negative cases where metastases in breast sentinel lymph nodes were missed. Most of these false negatives were attributed to micrometastases that were subsequently discovered only after serial sectioning of these nodes and performing immunohistochemical studies. Since these metastases were not identified on the FS slides, the reason for the false negative is the result of sampling error. This is in line with literature on the topic, highlighting that FS itself has very good diagnostic performance concerning detection of macrometastases, but inferior sensitivity in detection of micrometastases and isolated tumor cells.43,44 False-negative rates range in international studies between 5% to 43% and also in large centers is comparable to ours. 45 The potential negative consequence of a false-negative FS diagnosis of a sentinel node should be evaluated is not that severe, considering that the indications for axillary dissection have changed over time. Indeed, in patients with breast cancer of low stage I–II with no clinical and radiological suspicion of lymph node involvement, even 1–2 positive sentinel nodes would not necessarily be an indication for a complete axillary dissection if radiotherapy and systemic therapy are offered.46–49
Following deployment of the aforementioned digital pathology network feedback was provided by surgeons, lab technicians, and pathologists. The main challenges for surgeons were the necessity to schedule an FS and provide details ahead of time of the exact specimen to be analyzed intraoperatively, as well as slight prolongation of surgery times. However, these drawbacks were counterbalanced by the increased control surgeons had with handling specimens themselves, closer interaction with expert pathologists based at the hub hospital, and the convenience for their patients to be able to undergo oncological surgery at a district spoke hospital instead of travelling to the chief hub hospital. The main challenge reported by technicians was the need to better reorganize their routine work at spoke hospitals, in order to accommodate additional on-call intraoperative consultation duties. Nevertheless, technical personnel showed a general positive attitude towards adopting this technology.
The principal challenge encountered by pathologists was their initial unfamiliarity and skepticism towards using the digital pathology solution for telepathology. However, their hesitancy decreased over time and today remotely reading an FS at one of the spoke hospitals via telepathology has become routine practice and the digitized FS slides are perceived as routine as the FS provided traditionally at the hub hospital. Deploying the telepathology system also forced standardization of how FS cases were handled at all locations (e.g. same instruments, cryoembedding medium, 50 stain protocols). This also improved the quality of slides, making them easier to scan and view on a monitor. The biggest advantage for pathologists, and the technician on-call for this intraoperative service, was that they no longer had to waste time travelling to the spoke hospitals. As a result, there were cost-savings related to the recovered time of the medical and technical workforce. It is difficult to precisely quantify this cost saving due to the variation of diverse factors (e.g. loss of productivity, salaries, travel expenses). Nonetheless, after the initial cost of 250,000 euros to set-up of the entire digital pathology system (four scanners, computers with monitors, and time spent on training), a projected savings of more than 40,000 euros/year was estimated calculated secondary to better rationalization of personnel activities and ceasing expenses for travel. However, we clearly acknowledge that this study is not intended as a health economics evaluation study, 51 and the projections reported are to be considered in the overall benefits of the telepathology system.
Conclusion and future directions
In conclusion, the results of using telepathology for remote intraoperative consultations in South Tyrol for greater than 10 years demonstrate not only the feasibility and safety of utilizing such a system in a geographically complex territory, but also benefits related to quality of clinical diagnoses, convenient patient access to expert care, and cost savings. Moreover, the use of telepathology in a public health setting showcases the role of digital pathology to drive innovation and standardization in diagnostic pathology practice.
Footnotes
Acknowledgments
The authors are thankful to all the pathologists, surgeons and the technicians who participated in the intraoperative frozen section telepathology service.
Conflict of interest
The authors have no conflicts of interest to declare.
Contributorship
IG, SN, AE, MB and GM conceived the study. SN, EH and GM collected and analyzed data. IG wrote the first draft of the manuscript. MH and LP critically reviewed and edited the manuscript. All authors reviewed the manuscript and approved the final version of the manuscript.
Ethical approval
No approval needed for archival studies with no intervention on patients.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
IG.