
Abstract
Background
The growing use of digital primary care consultations has led to concerns about resource use, equity and quality. One of these is how it affects antibiotic prescription. Differences in ease of access for patients and available diagnostic information for the prescribing physicians are reasons to believe prescription rates may be affected.
Objectives
We estimated differences in antibiotic prescription between traditional office-based and digital contacts, if these differences varied between groups of diagnoses depending on the availability of information for the prescribing physician, and if differences were associated with socio-demographic patient characteristics.
Methods
Using individual level register data for a sample of patients diagnosed with an infection over a two-year period, we estimated differences in prescription between the two types of contacts and applied propensity score techniques to mitigate possible problems with treatment selection bias.
Results
The share of antibiotic prescription was 28 (95% CI 27–30, p < 0.001) to 33 (95% CI 29–36, p < 0.001) percentage points lower among digital contacts as compared to office-based contacts. For urinary tract infections, the differences in prescription rates between the two contact types were smaller (34 to 41 percentage points difference) than for throat and skin infections (50 to 60 percentage points difference). For women, rural, older, and people born outside Sweden, digital contacts were associated with higher prescription rates.
Conclusions
Antibiotic prescription rates were significantly lower for digital contacts compared with office-based contacts. The findings suggest that digital primary care may be an effective alternative to in-person visits without undue consequences for antibiotic prescription levels, although to varying degree depending on diagnosis.
Introduction
Digitally provided services in primary health care have increased sharply over the past decade and provide both opportunities and challenges to health care systems. A key quality concern is the effect that digital primary care services may have on antibiotic prescription rates. In digital contacts patients cannot necessarily be examined in the same way as in office-based visits. Lower barriers to a prescribing physician attributed to easier patient access online and a more anonymous patient–physician relationship could lead to higher rates of antibiotic prescription, if they are given on less strict medical indications.1,2
In Sweden, digital primary care has developed rapidly over the past six to seven years. It is likely that the low access to traditional primary care services has contributed to the development, 3 but also a strong innovative digital sector and the generally high digital literacy among the population. It has been shown that antibiotic prescription is higher in Swedish municipalities with shorter waiting time to primary care. 4 Improved access to care through digital means could negatively affect recent years’ gains in lower antibiotic consumption in Sweden. 5 In Swedish primary health care, large focus is given to prudent prescription, which is encouraged financially and through strict treatment protocols.5,6
The current evidence on the effects of digital primary care on antibiotic prescription rates is still relatively limited. Furthermore, contextual differences are likely to impact prescription behaviour and thereby the relevance of the emerging evidence, which largely consists of studies from the US. 7 We found one systematic review on the impact of consultation on antibiotic prescribing in primary health care, which showed a mixed picture regarding the effect on prescribing. 8 Beyond the review, one study found higher level of prescription among digital contacts for urinary tract infections. 9 However, a study on antibiotic prescription for sinusitis found lower prescribing in the group of digital contacts. 10 A study of acute respiratory infections found no significant difference in prescription levels. 11
In the Swedish context, three studies with similar aims but adopting different approaches have been published.12–14 One study selected patient cases from an electronic records system at a local private group of clinics, providing both in-office and digital contacts in the form of asynchronous text-based messages. 13 Prescription rates were compared for sore throat, dysuria (indicating urinary tract infection), and respiratory symptoms, and findings showed that asynchronous digital contacts were not associated with higher prescription rates compared with office visits. Another study compared nation-wide contacts from private digital providers in Sweden with traditional office-based visits in primary care in one region (population 300,000) over a two-month period. They found almost five times higher odds of an antibiotic prescription during office-based visits, although with large variation between diagnoses. 14 Both studies applied descriptive logistic regression with basic patient characteristics such as age and sex. Applying a differences-in-discontinuity estimation, making use of data from before digital contacts were available and the difference in user fees at the age of 20, one study found that digital meetings were at least as restrictive on antibiotic prescriptions as traditional care. 12 In addition, a recent working paper (preprint) on utilization of digital primary care documented generally lower levels of prescriptions among digital contacts. 15
Evidence for possible differences in antibiotic prescriptions between traditional office-based contacts and digital contacts is inconclusive. We also found that few studies have applied more than descriptive regression analyses, only using data on crucial differences in the patient mix as controlling covariates. Further, we note the differences in barriers to access between the two types of contact and that these differences may vary between different infection diagnoses. The fact that a single diagnosis can include a spectrum of severity (heterogeneity) that is not observable in quantitative data and include a possible self-selection in care seeking behaviour has not been assessed. With its early adoption of digital primary care services and emphasis on restrictive antibiotic use, Sweden provides a case for assessing prescribing effects of new forms of primary care services. 16 We define a digital contact in this study as an online consultation, remotely provided either by video or chat function.
To contribute to an improved understanding of the effect of digital primary care, the aim of this study was to evaluate differences in the probability of antibiotic prescription between digital and office-based primary care. Specifically, we analyse differences in the probability of prescription by sub-groups of infections, as differences in prescription rates between digital contacts and traditional primary care may vary with differences in what clinical information is available. We also investigate if single socio-demographic patient characteristics were associated with differences in prescribing between digital and office-based contacts.
Conceptual framework and context
Patient characteristics as factors for antibiotic prescription
A primary care contact for an acute but mild infection is typically initiated by the patient and can lead to a prescription of antibiotics. With the introduction of digital services, the barriers to seeking and accessing a medical provider who can prescribe an antibiotic were reduced for many patients. With lower barriers to seeking care, it is likely that for any given diagnosis, there is a self-selection among patients which correlates with the severity of the infection. With the new lower barrier alternative that was previously not available, patients with less severe infections may be more prone to contact health care. Early evidence from England supports this possibility. 17 If patients have the same probability of antibiotic prescription for any same condition regardless of whether they contact an office-based or a digital provider, it would lead to proportionally lower levels of prescription in the more easily accessible contact form since more patients with less severe infections would present themselves to that health care provider, given the lower barrier for contacting health care. By means of register data, a possible patient self-selection in play relative to the severity of each diagnosis is not possible to observe. However, data on socio-demographic factors that can impact the response to the potentially lower care seeking and access barriers to providers, such as age, sex, income, and education level, are available. These factors are all related to various aspects of digital literacy, including health care seeking behaviour 18 and often vary between traditional and digital contacts. 19 It is also well documented in Swedish official statistics that age and sex are associated with the level of antibiotic prescription, which is generally lower among men and increase with age. 20 It has not been studied if these factors can explain possible differences in prescription between office-based and digital contacts, even though evidence unambiguously shows that both access to services and quality of care are dependent on patients’ socioeconomic characteristics. 21
Differences in required information to prescribe antibiotics
After initial contact by the patient, there are factors on the provider side, which can affect the probability of prescription depending on type of contact. A digital contact includes fewer investigative tools and hence less information on which to base the treatment decision. However, according to Swedish guidelines for some diagnoses, most prominently lower urinary tract infections in non-pregnant women, the decision can often be taken solely based on patients’ self-declared health status. 22 This implies that the same information is available to the physician in either model of care and any differences in prescribing between the two types of contacts are due to factors of access barriers and guideline adherence. For some infection diagnoses, data available to make a decision about prescription are lacking in digital types of contacts. This situation limits the advantageous effect of low barriers to digital care and requires that patients contacting a digital physician have an additional care contact apart from meeting the physician. An example is tonsillitis, for which a streptococcal antigen test is recommended for decision making according to Swedish guidelines. In a third group of diagnoses, which includes several skin conditions, the patients’ self-declared health status in combination with a visual aid can in theory, but not necessarily in clinical practice, adequately inform the decision about whether to prescribe antibiotics.
The above implies that the share of contacts leading to a prescription in office and digital types of contacts differ between diagnoses that require only patient-reported health status compared with diagnoses that require either a visual investigation, a physical meeting, or a laboratory test. More restrictive prescriptions in digital contacts relative to office-based contacts for diagnoses that require clinical data beyond what the patient's anamnesis can provide would then be expected.
The Swedish primary care context
Funding and provision of health care in Sweden is the responsibility of 21 independent regional administrations. In primary care, all regions apply a predominantly capitation-based payment and a broad service package requirement, but contracts and reimbursement rules vary considerably. Sweden's primary care is characterised by a mix of public and private clinics with multi-professional teams. The free provider choice for patients was strengthened with new legislation in 2010 by liberalising the rules for establishing new clinics. 23 The intention to support a more patient responsive primary health care system was partly met, although effects on waiting times and geographical access were not large. 24 In addition, primary care visits outside the patient's home region are reimbursed by the home region on a per-visit-bases. This inter-regional billing system works in parallel with the capitation system and has been important for the evolvement of publicly funded digital primary care services, as digital providers operating nationwide have used it to charge for contacts.
Methods
Sampling and data collection
We used a purposive Swedish consultation level dataset for 1 January 2017 to 31 December 2018. The data were collected for an ongoing project of the effects on the Swedish health system following the fast-growing use of digital primary care. The dataset combines detailed clinical data on traditional office-based and digital contacts by residents in five Swedish regions spread across the country, including both mid-sized cities and rural areas. Only adult patients (from age 18 and older) were included, as prescription data on children were not captured in the same way across regions.
The sample included all patients who had been diagnosed with at least one of three different types of infections during the study period: urinary tract infections, upper respiratory tract infections and skin and soft tissue infections. A national identification number enabled linking of data from different sources on the level of each individual. Data on the socio-demographic variables sex, age, income, education, residency and place of birth of these individuals were collected from Statistics Sweden. Data on diagnoses from specialised care (outpatient and inpatient) were collected from the National Board of Health and Welfare and used to construct a Charlson comorbidity index value for each patient. 25
We selected the infection diagnoses which have recommendations on antibiotic use by the Swedish strategic programme against antibiotic resistance (STRAMA) 26 to focus the study on conditions that are specifically sensitive to careful antibiotic prescription. The specification of diagnoses captures both coding by the International Classification of Diseases 10th edition and the International Classification of Primary Care used by many physicians. 27 Supplement 1 provides a table with the exact diagnosis codes. The final sample is described in Table 1.
Descriptive statistics of sample.

Source: Digital primary care study; consultation level data for sampling period.
Only the three largest Swedish cities are classified urban, where no patient in the sample is resident.
* We conducted statistical analysis for differences between the groups. The tests (chi2-test for the categorical variables and t-test for the continuous variables) show statistical differences between the two groups (p-value < 0.001).
Statistical analysis
We first tabulated the crude differences in prescription between office-based and digital contacts (results in Table 3). We then estimated the difference in probability to receive a prescription of antibiotics (the outcome) between office-based and digital contacts (treatment choices) by applying three different regression models (results in Table 4). First, a logistic regression model was applied, in which the patient characteristics are used as controlling factors to adjust for case-mix. The estimated coefficients were used to predict the differences in levels of prescription between the two types of contact. With the intention to mitigate the potential bias in the first regression model's treatment estimate due to self-selection of contact type, two propensity score models were applied. These two models make use of the patient characteristics to estimate the propensity to choose one or the other type of contact.
Propensity score models
Because the assignment to one of the contact types (digital or office-based) was not random in our material, there are most likely unobserved mechanisms influencing the choice of contact that correlate with the outcome, prescription of antibiotics. We applied modelling based on the potential outcomes framework, which attempts to mitigate the selection problem. 28 As the potential outcome of choosing the other contact than the de facto chosen is not known, the potential outcomes framework is a set of estimation techniques that attempts to estimate the unobserved potential outcome in the data and compare the two intervention groups.
Specifically, we modelled the relationship between antibiotic prescription and type of contact using propensity score matching and inverse probability weights models. Both approaches estimate what would be the effect if everybody in the sample had the same type of contact. They both reflect the probability of contact assignment conditional on the observed characteristics of the sample, hence the name ‘propensity’. 29 However, they differ as to how the differences in the characteristics of observations are used. In propensity score matching, observations are matched by finding patients with the same probability of selecting one or the other type of contact. In our sample, the matching was based on the equal propensity to choose an office-based or digital contact. In the inverse probability weighting model, each contact groups’ observations are weighted so they become the inverse of their probability to have selected the other type of contact. 30 The two approaches complement each other to strengthen the analysis of the effect of digital care on the identified outcomes. As both techniques use covariates of the observations to obtain comparable treatment and control groups and meet the assumption of independence between the outcome and treatment choice, the observations in the matched samples should be balanced in their characteristics, that is, the mean and covariance of variables should be close between treatment levels. 31
For these models we used Stata's treatment effect commands teffect psmatch and teffect ipw, 32 to estimate the difference between the two types of contacts with respect to prescription. We specified each model using the variables available (Table 1) to achieve the highest possible balance between covariates after the propensity estimates. The main result for each model and sample group (Table 4) is the average treatment effect, that is, the difference between two mean outcomes in the hypothetical situation when all patients had chosen one or the other contact. This can also be seen as the estimated average casual effect in the population.33,34
Diagnose groups to reflect differences in available information for prescribing antibiotics
We identified three groups of diagnoses to analyse the effect that information availability may have in the probability of antibiotic prescription across the two treatment alternatives. We specified a first group of diagnoses for which no additional information than the patient's description is needed to prescribe as lower urinary tract infections in women. A second group was defined by the throat infection diagnoses pharyngitis and tonsillitis, which typically require laboratory data to prescribe. A third group was defined by three skin infections that may be assessable over video: borrelia (Lyme disease); impetigo; and erysipelas (Table 2). Supplement 1 provides a table with the exact diagnosis codes per group.
Information needs for prescribing by diagnoses group.

Socio-demographic factors and prescription
To meet the objective to investigate each socio-demographic factors’ association with differences in prescribing between the two types of contacts, we tested if the share of prescription by type of contact differed depending on the level of each patient characteristics age, sex, co-morbidity status, income, education, place of residence, and country of birth (see Table 1 for the list of covariates). Equation 1 describes our general model.
Results
Differences in prescription between types of contact
The share of contacts leading to an antibiotic prescription was significantly lower in digital contacts as compared with office-based contacts, regardless of estimation model or diagnosis grouping. When no adjustments for case-mix or modelling of the data were made, including the entire sample, the difference was 31.5 percentage points (Table 3). Of the three groups of infection diagnoses defined by differences in information need for prescription, the difference in prescription was smallest (41.2 percentage points) among lower urinary tract infection diagnosis (group 1). In group 2, with diagnoses which typically require a physical meeting or laboratory test to prescribe antibiotics, the difference was larger (52.3 percentage points). Skin infections, requiring a visual or image assessment, had the largest difference in prescription between the two types of contact (59.4 percentage points).
Crude differences in shares of prescription between office-based and digital contacts, by type of diagnosis groups.

* p < 0.001.
All three regression models showed a lower share of prescription for digital contacts. By the first model, in which we predicted the differences in levels of prescription based on the coefficients from a logistic regression model, the probability of a prescription at a digital contact was 28 percentage points lower than at an in-office visit. The respective propensity score models both showed 33 percentage points lower prescription for digital contacts in the total sample (Table 4). For lower urinary tract infections, the estimated difference in prescription between digital and office-based contacts was smaller (34 to 41 percentage points depending on model) than for skin infections (48 to 58 percentage points difference) and throat infections (52 to 53 percentage points difference) in all regression models. The lower difference to skin infections were significant in all models, but undecisive relative to throat infections due to the matching model's large confidence intervals.
Difference in prescribing probability between in-office and digital contacts, by groups of diagnoses and by estimation model [95% confidence interval]*.

* p-value for all differences is <0.001.
Supplement 2 provides each models’ specification, as well as mean and variance differences for each covariate.
The estimated differences in prescription between types of contact were larger in the two propensity models. In particular, the inverse probability weighting model showed significantly larger prescription differences in all groups except for throat infections. The results indicated that when we compared individuals with the same propensity to choose one or the other care contact based on socio-demographic characteristics, the differences in prescription were higher.
Prescription and socio-demographic factors’ interaction with type of contact
Four socio-demographic factors had a significant interaction with type of contact in the regressions, that is, the share of antibiotic prescriptions by type of contact differed depending on the level of the factor (Table 5). Figures 1 to 4 show the predicted rates of antibiotic prescription for these factors. For men, the effect of contacting primary care in a digital format was associated with less probability to receive a prescription as compared to women making the same choice of contact (urinary tract infections excluded, Figure 1). With increasing age, there was a considerable increase in prescriptions for digital contacts, especially for the oldest group, but only small differences for the office-based contacts (Figure 2). This age pattern was consistent across groups of diagnoses (not shown). For people living in sub-urban areas, contacting digital services was associated with a lower rate of prescription than for people living in rural areas (Figure 3) and for people born in Sweden, digital contacts were not associated with higher prescription than for foreign-born, which was the case for in-office contacts (Figure 4).
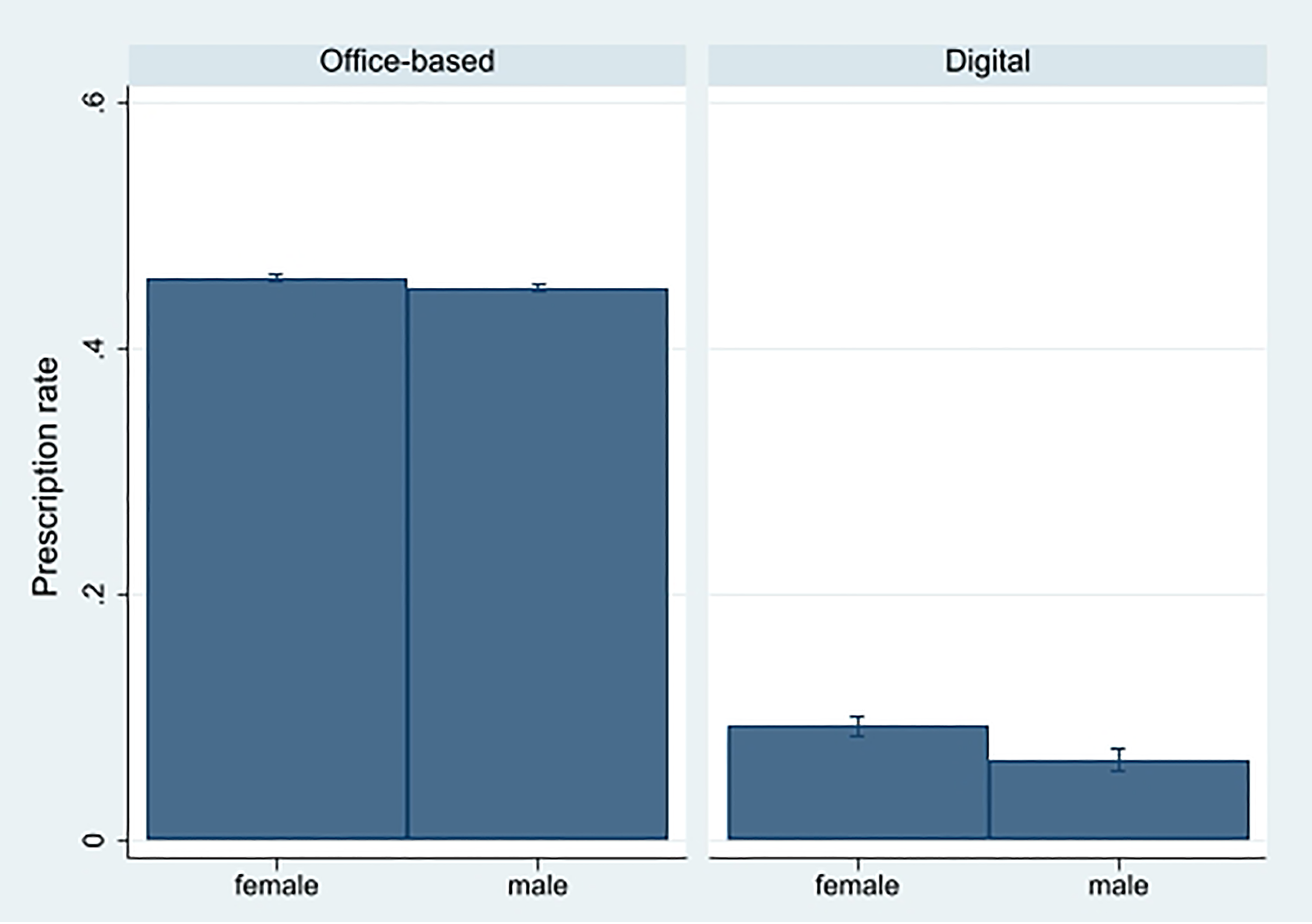
Predicted rates of antibiotic prescription by sex and type of contact (95% confidence intervals).
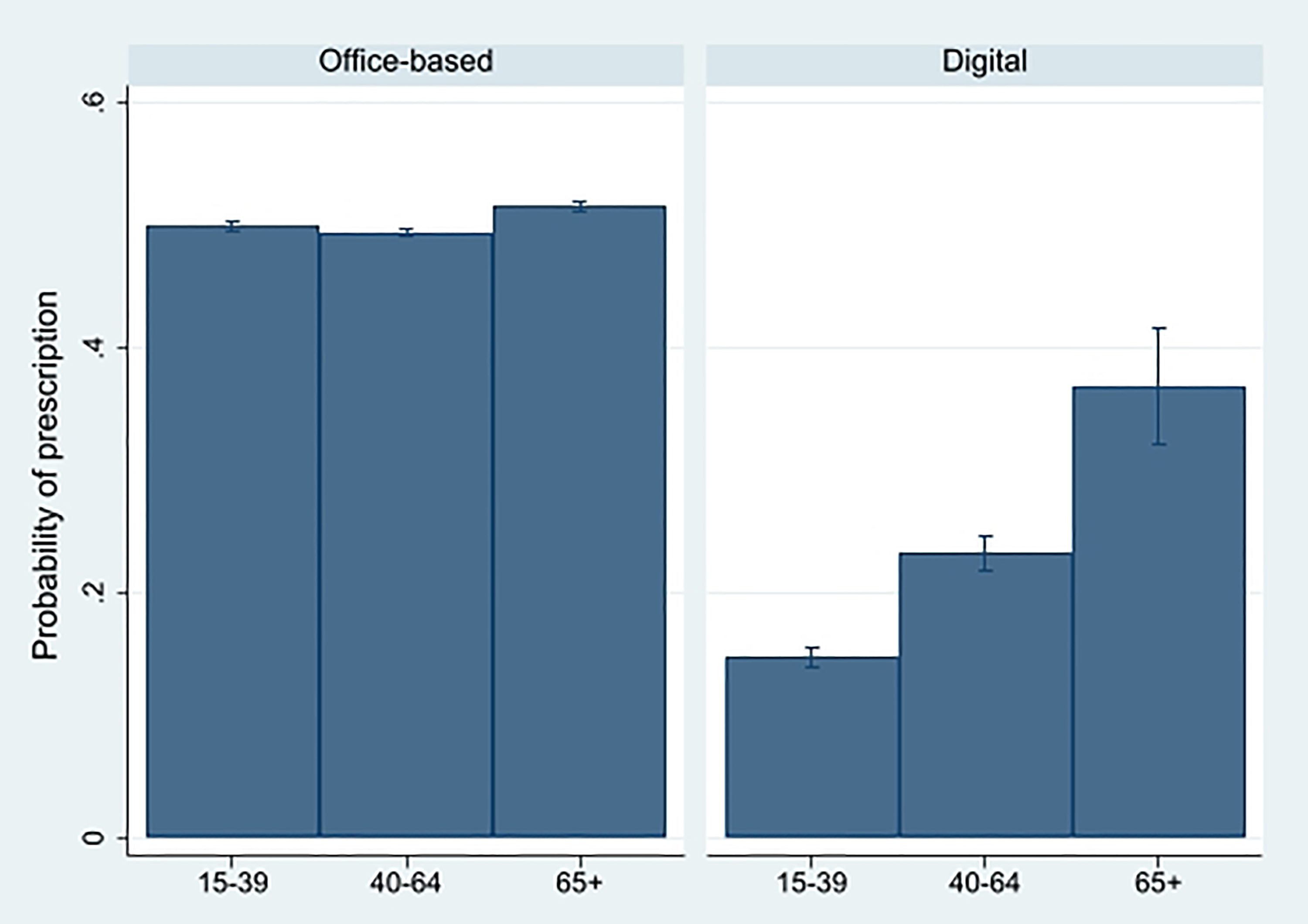
Predicted rates of antibiotic prescription by age and type of contact (95% confidence intervals).

Predicted rates of antibiotic prescription by geographic region and type of contact (95% confidence intervals).

Predicted rates of antibiotic prescription by country of birth (quantiles) and type of contact (95% confidence intervals).
Log odds interaction coefficients between type of contact and patient characteristics with regard to level of antibiotics prescriptions.
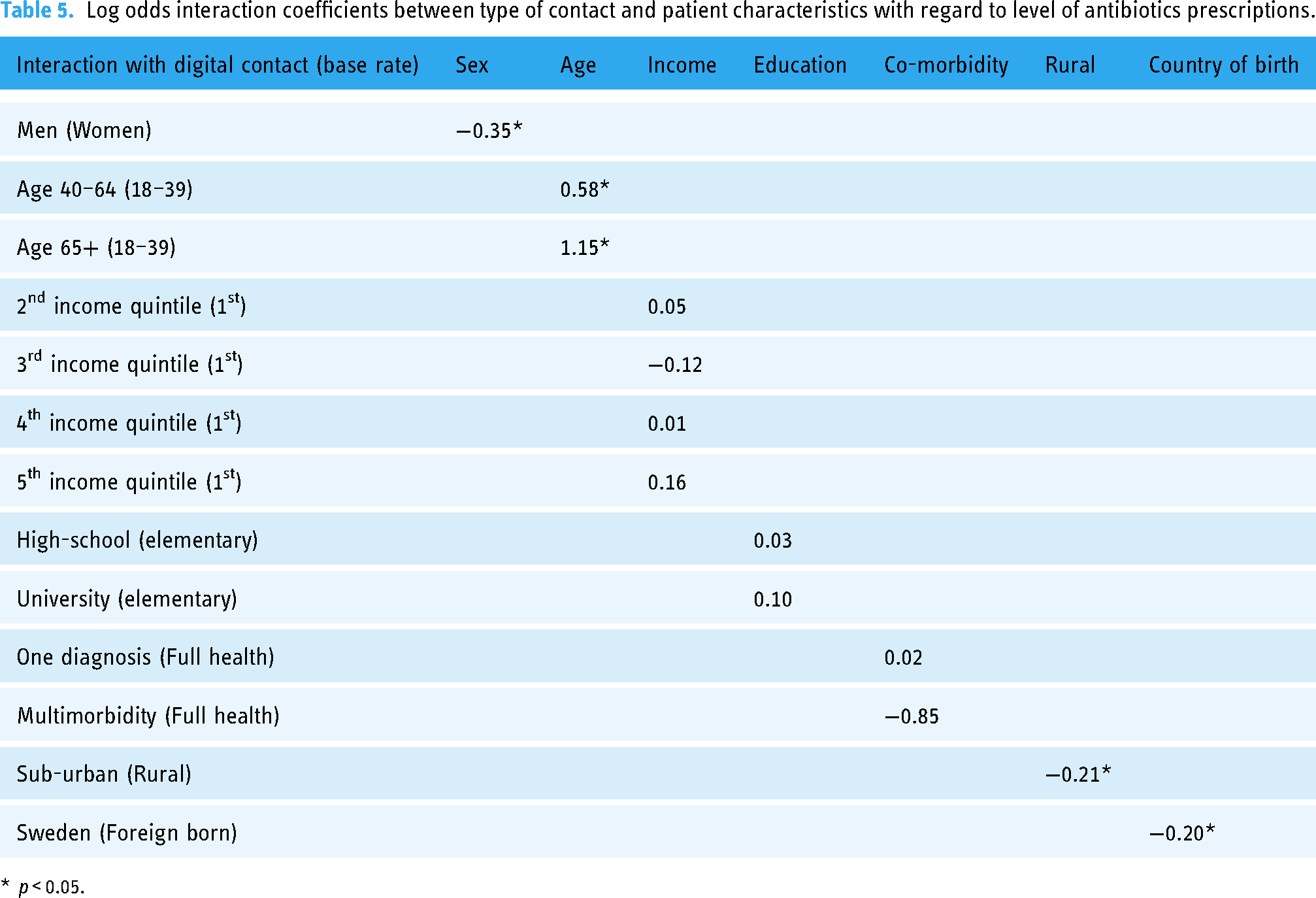
* p < 0.05.
For level of income, education and multi-morbidity, there was no significant interaction effect with type of contact regarding prescription level, that is, shares of prescriptions did not change with these factors in combination with office-based and digital contacts (Table 5).
Sensitivity analysis
The results may be sensitive to data collection differences across regions, due to differences in health information systems such as electronic medical records and database management. To check if results held across regions, we estimated the differences in prescription between contact types also per region (results not shown). The results remain largely robust to these adjustments in the samples. The share of prescriptions in digital contacts was significantly lower and the differences were smaller in lower urinary tract infections than for the other specified diagnosis groups across all regions, consistent with the full sample analysis.
As Table 1 shows, there are differences between the types of contact with regard to which profession the patient meets. In the digital contacts the staff category is almost exclusively a physician, which is not the case for in-office contacts. There are also observations with missing data for in-office contacts. To ensure our results hold, regardless of which profession provides the service, we conducted sub-analyses with comparisons of physicians only. The differences to our main results are small in all estimation models, with a slightly smaller difference in prescriptions overall when we compare physicians only. Table 6 replicates crude percentage differences in prescriptions from Table 3, with differences for only physicians as a comparison. Other results are not shown but in line with these comparisons.
Comparison of crude differences in prescription for all providers and physicians only.

* p < 0.001.
Discussion
This study evaluated the differences in antibiotic prescription between traditional office-based and digital contacts in the early phase of the digital primary care development in Sweden. Antibiotic prescription rates were significantly lower in digital contacts compared with office-based contacts and this held true for all defined sub-groups of diagnoses. Differences in antibiotics prescriptions between the two types of contacts vary by diagnoses. We found smaller difference in antibiotics prescriptions for lower urinary tract infections in women than for the groups of diagnoses requiring image or visual data (skin infections) and indication of the same for diagnoses requiring laboratory testing (throat infections). Other studies comparing digital contacts with physical contacts have also found differences between groups of diagnoses.13,14 Although we cannot conclude what leads to these differences, the findings are in line with our conceptual framework that differences in prescription rates between types of contact can be related to differences between conditions in how much patient information the prescribing doctor has. In contrast, an earlier US study found double the number of antibiotics prescriptions for urinary tract infection during digital contacts than office visits, hypothesizing that inability to examine the patient could instead lead the physicians to a more ‘generous’ prescription. 9 This does however not seem plausible from more recent evidence, which in line with our results show lower prescription rates for digital contacts.
The propensity score modelling approach from the potential outcomes framework, making use of patient characteristics to make assumptions about choice of contact type, produced somewhat higher estimated differences in prescription, as compared to the descriptive regression model. Hence, when we attempted to mitigate the problem of a possible selection bias in the register data by applying the propensity models, we observed larger differences than in purely descriptive comparisons. The differences between the models were not conclusive but illustrate the problems with the almost exclusively observational studies in the literature, as the differences in prescription are possibly larger than we observe in descriptive statistics. The only earlier study evaluating the effect of digital primary care on antibiotic prescription that applied both a descriptive model and a matching technique did not observe any differences between the modelling techniques, but that study applied direct matching on observations and not a propensity score technique, and was conducted in a different context. 11
This is the first study that has assessed which socio-demographic factors may drive antibiotic prescription in digital primary care. It has been repeatedly documented in public official statistics that antibiotic consumption increases with age and is lower among men than women, measured as share of population size. 20 A Swedish study on traditional primary care with data from 2016-2017 indeed showed that women and patients in the highest age groups had significantly higher levels of dispensed antibiotics. 35 It also found higher levels among high-income groups. Our study indicates that the choice of contact interacts with age and sex with regards to antibiotics prescriptions. Male patients had lower and older patients higher probabilities of prescription if they made a digital contact than an office-based contact. Furthermore, the uptake of digital services in Sweden has been faster in urban than in rural areas. 36 The significantly lower level of antibiotic prescription in digital contacts among patients residing in sub-urban areas relative to rural that we found, suggests that the effect of generally lower prescription rates for digital contacts were strengthened among patients in sub-urban areas.
Whilst it has been shown that high co-morbidity was associated with higher rates of antibiotic prescriptions in traditional, office-based care, 4 we saw no significant multi-morbidity interaction effect with type of contact, as variation in digital contacts were large and we only had 43 patients in the multi-morbidity group. The same study found that patients born in Sweden received antibiotic prescriptions at a higher rate in traditional primary care, although another study found the opposite result for dispensations.4,35 Our results show that higher antibiotic prescription for people born in Sweden may only be true in traditional in-office care (Figure 4). But we also note that there may be other aspects of ethnicity than country of birth, that we cannot capture in Swedish register data. We could also not observe any significant interaction between educational level and digital contacts with regard to antibiotic prescriptions.
We note that the study is limited to a geographical selection of Sweden and does not include the three main urban areas, where digital services grew fastest in the beginning. Antibiotic prescribing for mild infections indeed varies across Swedish regions. 37 The strength of using data from several regions in the analysis carries risks that differences in coding practice between physicians, clinics and regions, and data administration systems, affect the results. We observed large differences in the crude prescription rates for in-office contacts (33–76% for all diagnoses) across the five regions while differences were considerably smaller in digital contacts (17–21%).
There are several factors that may affect prescription patterns, which would need further studies. Some are related to the care process and could affect rates of prescription in both directions, depending on how they influence the decision process of patients and prescribing medical staff.
When the patient contacts the care facility, the triage functions are different in the two forms of care. In Swedish office-based primary care, the first contact is often with a nurse. When there are symptoms of a mild infection some of these contacts may not lead to an infection diagnosis, but instead lead to advice on self-care and expectance (watchful waiting). In contrast, the digital providers offer a more direct contact with a physician and this higher probability to see a physician directly could lead to a smaller share of prescriptions in our study. It has also been suggested that built-in clinical support tools available to physicians working on digital platforms could enable more prudent prescription.38,39 Notably, phone contacts are not included in this study. Differences in opportunity to contact the provider over phone by types of contact may impact both choice of contact and the diagnostic process. Also, digital tools develop both technically and in their practical applications, and medical staff and patients become more used to them, which will affect the care process and calls for updated studies on this topic. Finally, when the physician meets the patient, there might be individual factors that affect prescription rates and explain the observed lower prescription rates in digital contacts. One of these is if younger physicians are more attracted to working digitally, as it has been shown that younger physicians can be more prone to follow guidelines than older colleagues. 40
In addition to care process factors, there are several structural aspects in the Swedish primary care system that could affect the differences we have observed. Digital providers in Sweden work on a fee-per-visit basis while office-based providers largely operate on a capitation rate. As the digital service is only reimbursed when a physician contact takes place, the incentive is to meet patients also on less severe indications. These contacts may not have taken place if the payment system had been based on capitation. Again, more contacts based on less severe indication (but with the same diagnosis) would lead to a proportionally lower prescription rate among diagnosed digital contacts. If on the other hand prescription rates had been on the same level in the same situation, it would imply that digital contacts follow guidelines less strictly. Further, growth of digital contacts was in Sweden initially driven by private for-profit providers. This difference in market conditions could also affect prescriptions. With the market reforms approximately ten years earlier, there were signs of an increase in antibiotic prescriptions among private office-based providers.41,42 Generally, a shift to more patient demand-driven health care have raised concerns about providers’ ability to base their decisions strictly on medical grounds. 43
Conclusions
We conclude that digital services do not generally imply higher antibiotic prescription levels among their contacts than traditional primary care, but rather the opposite. The results are relevant for continued development of service provision and can support further policy development with regards to digital primary care. Continued studies of antibiotic prescription will be important in the context of growing digital primary care services. These services evolve fast and potential patients will be increasingly used to contact them, and new forms of hybrid contact forms are likely to develop. As such, the results presented in this article can also be seen as a base-line study of the effects of increasing digital primary care.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231156213 - Supplemental material for Evaluating the effect of digital primary care on antibiotic prescription: Evidence using Swedish register data
Supplemental material, sj-docx-1-dhj-10.1177_20552076231156213 for Evaluating the effect of digital primary care on antibiotic prescription: Evidence using Swedish register data by Jens Wilkens, Hans Thulesius, Eva Arvidsson and Björn Ekman in Digital Health
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231156213 - Supplemental material for Evaluating the effect of digital primary care on antibiotic prescription: Evidence using Swedish register data
Supplemental material, sj-docx-2-dhj-10.1177_20552076231156213 for Evaluating the effect of digital primary care on antibiotic prescription: Evidence using Swedish register data by Jens Wilkens, Hans Thulesius, Eva Arvidsson and Björn Ekman in Digital Health
Footnotes
Contributorship
JW formulated research questions, defined methods, conducted the statistical analyses and drafted the manuscript. HT ensured clinical relevance in the design of the study, guided the selection of variables, interpreted results and contributed to writing the manuscript. EA led the diagnoses selection, advised on clinical relevance and critically revised the manuscript. BE was the Principle Investigator of the project, conducted the acquisition of the data, guided model design and statistical analyses and edited the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval has been provided by the Swedish Ethical Review Authority (reference number 2019-01500). This is a registry-based study. As such, use of data follows the Swedish legislation and practice with regards to consent. For more information about ethical aspects and consent in registry-based studies in Nordic countries, see Ludvigsson et al. 44
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was mainly funded by the Swedish Research Council for Health, Working Life and Welfare (grant number 2018-00093). The overall aim of the study was included in the funding proposal, but not the specific design and statistical methods. Additional resources for the study represented a minor part of funding and were not raised externally.
Guarantor
JW
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.