
Abstract
Objective
Due to the growing complexity in monitoring and treatment of many disorders, disease-specific care and research networks offer patients certified healthcare. However, the networks’ ability to provide health services close to patients’ homes usually remains vague. Digital Health Technologies (DHTs) help to provide better care, especially if implemented in a targeted manner in regions undersupplied by specialised networks. Therefore, we used a car travel time-based isochrone approach to identify care gaps using the example of the neuroinflammation-focused German healthcare and research networks for multiple sclerosis (MS), myasthenia gravis (MG), myositis and immune-mediated neuropathy.
Methods
Excellence centres were mapped, and isochrones for 30, 60, 90 and 120 minutes were calculated. The resulting geometric figures were aggregated and used to mask the global human settlement population grid 2019 to estimate German inhabitants that can reach centres within the given periods.
Results
While 96.48% of Germans can drive to an MS-focused centre within one hour, coverage is lower for the rare disease networks for MG (48.3%), myositis (43.1%) and immune-mediated neuropathy (56.7%). Within 120 minutes, more than 80% of Germans can reach a centre of any network. Besides the generally worse covered rural regions such as North-Eastern Germany, the rare disease networks also show network-specific regional underrepresentation.
Conclusion
An isochrone-based approach helps identify regions where specialised care is hard to reach, which might be especially troublesome in the case of an often disabled patient collective. Patient care could be improved by focusing deployments of disease-specific DHTs on these areas.
Keywords
Introduction
Neurological diseases are often challenging to diagnose and treat,1–3 but decades of intensive research have led to a better understanding of neuroinflammatory diseases such as multiple sclerosis (MS), myasthenia gravis (MG), or myositis.4–6 A broader therapeutic landscape combined with more elaborated diagnostic criteria allows for a more personalised approach to disease management in such disorders. Due to the growing complexity of disease monitoring and treatment,6,7 physicians increasingly need to specialise within their respective fields and engage in interprofessional communication. Especially when diagnosing or treating rare diseases, novel procedures are usually only carried out in specialised centres, adding to the often unnecessarily prolonged time to diagnosis.3,8 Due to the limited number of experts in rare neurological disorders, accessibility to excellent care remains a challenge even in a country as densely populated and developed as Germany. 1
To foster excellent care, research and care networks have been established for many diseases or disease groups in Germany.9,10 By orchestrating research activities as well as offering communication and education channels, such networks aim to standardise disease management for their respective diseases. 11 Even though the number of specialised centres is increasing, these networks are still limited, resulting in considerable patient travel distances. Such travel can significantly increase the social burden for patients and caregivers, especially in often highly disabling neuroinflammatory diseases.3,12 Digital Health Technologies (DHTs) 13 are increasingly being applied to support remote disease management and comprehensive research efforts, which often used to be impaired by geographic inaccessibility.14,15 Well-directed deployment of DHTs in areas where currently specialised care is not available could help to reduce the overall travel time, patient burden and health outcomes significantly. With a larger number of DHTs available,16,17 the digital support can increasingly be tailored to the patient's and clinician's needs and provide assistance regardless of the respective location.
Thus, this study aims to identify such areas by using a new travel time-based technical approach on the example of coverage of excellence centres for different neuroinflammatory diseases in Germany.
Materials and methods
Overview
For the analysis, we used open-source software to calculate isochrones, areas that can be reached within a defined driving time given a particular start location. Consequently, we estimated the population living in the isochrone-covered areas.
Data
Neuroinflammation-focused excellence networks analysed include the research-focused networks ‘Kompetenznetz Multiple Sklerose’ (KKNMS) for MS; the integrated myasthenia centres (iMZ) for MG, the ‘Myositisnetz’ centres for myositis, and ‘Kompetenznetz Peripherer Nerv’ (KKPNS) for immune-mediated neuropathies. Additionally, the ‘Deutsche Multiple Sklerose Gesellschaft’ (DMSG) care-focused network was analysed for MS. Lists of centres of the respective networks were obtained from their public websites or by contacting the respective organisation. For DMSG centres, only clinical in- or outpatient centres were included, with rehabilitation and care centres not included in the analysis. Last centre data were collected on 30 April 2022 (for an overview, see Supplemental Table 1).
Data analysis
Analyses were performed using Python 3.8.8 (Python Software Foundation, Delaware, USA) with pandas package version 1.3.4. 18 All used services rely on data from the OpenStreetMap (OSM) project, 19 which is the basis for all shown maps. Geospatial analysis and manipulation of geometric objects were carried out using Rasterio package version 1.1.1 20 and Shapely package version 1.7.1. 21 Address geocoding was obtained using the geopy package version 2.2.0 22 with Nominatim geocoder for OSM data. Isochrones for geocoded excellence centres were calculated for 30, 60, 90, and 120 minutes using a local installation of openrouteservice23,24 to circumvent capacity constraints of the online interface. Isochrones of each care network for a given time were summed up via a urinary union to obtain complete coverage for the specific care network and driving time. The resulting geometric figure was then used to mask the publicly available global human settlement population grid 2019 (GHS-POP) 25 to approximate the population that lived in the covered area in 2015 (the most recent year included in the dataset). The relative population was calculated in reference to isochrones for MS data enlarged to the maximal size. Visualisation of results was accomplished by using plotly version 5.4.0. 26
Data availability
The data assessed in this study are available from the corresponding author on reasonable request. An interactive Figure of the main results that contains much of the data is available in a GitHub repository.
Results
The isochrones created from the respective medical networks showed a different coverage of Germany for the different timeframes. While differences between the networks were comparably large in isochrones focusing on shorter driving times such as 30 and 60 minutes, the analysis for 120 minutes revealed fewer differences as some care networks were already present throughout the landscape (see Figures 1 and 2). A link to an interactive version of the map is available in the footnote or Supplemental Material. 1

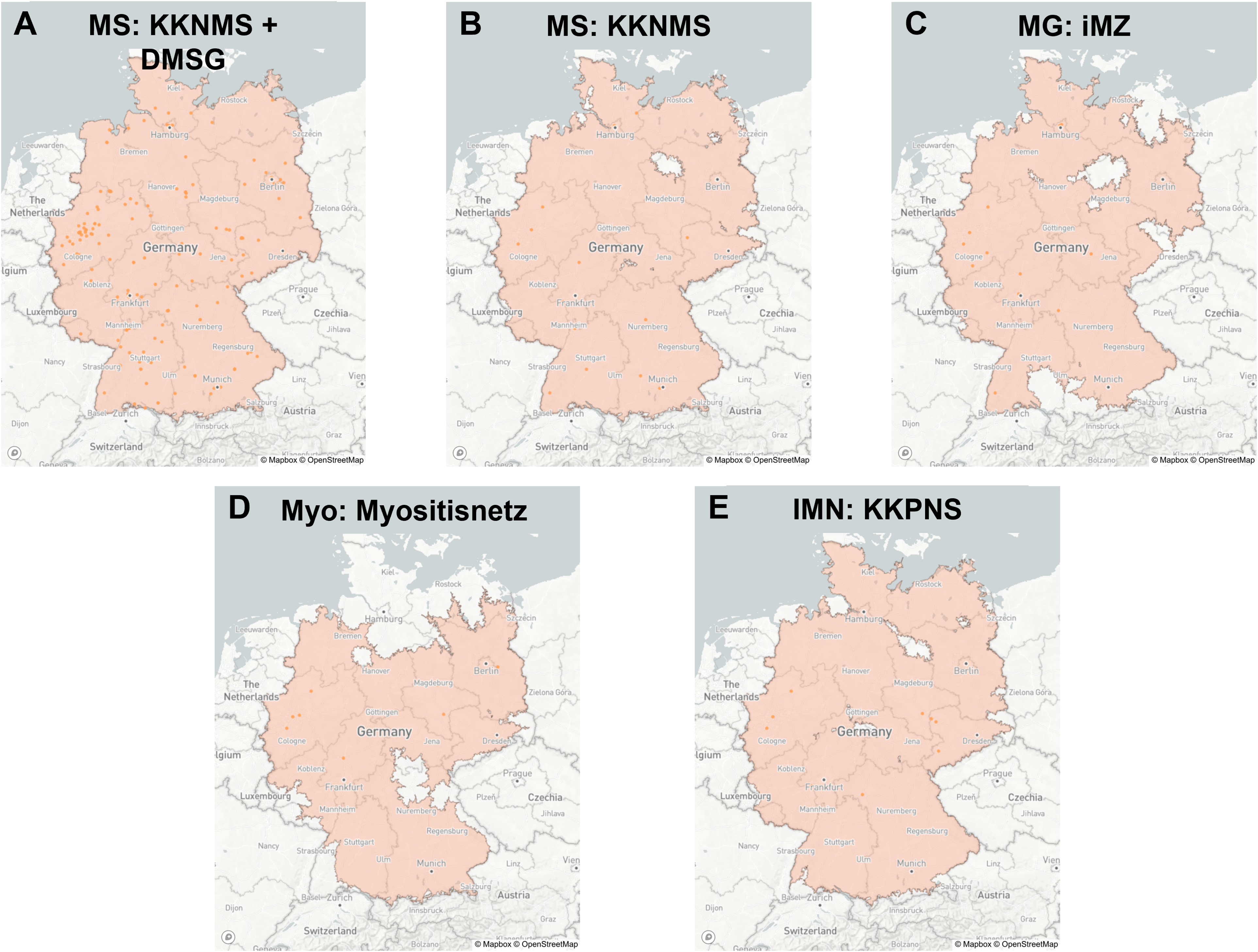
Isochrones for care networks with 60 minutes driving time from centres. The graphics (A–E) depict static images created from an interactive visualisation of the areas covered by the care networks (red) within 60 minutes of driving time. Networks analysed are focused on the different disorders MS (A and B), MG (C), myositis (D) and immune-mediated neuropathies (E). DMSG, Deutsche Multiple Sklerose Gesellschaft; IMN, immune-mediated neuropathies; iMZ, integrated myasthenia centres; KKNMS, Kompetenznetz Multiple Sklerose; KKPNS, Kompetenznetz Peripherer Nerv; MG, myasthenia gravis; MS, multiple sclerosis; Myo, myositis.
Isochrones for care networks with 120 minutes driving time from centres. The graphics (A–E) depict static images created from an interactive visualisation of the areas covered by the care networks (red) within 120 minutes of driving time. Networks analysed are focused on the different disorders MS (A and B), MG (C), myositis (d) and immune-mediated neuropathies (E). DMSG, Deutsche Multiple Sklerose Gesellschaft; IMN, immune-mediated neuropathies; iMZ, integrated myasthenia centres; KKNMS, Kompetenznetz Multiple Sklerose; KKPNS, Kompetenznetz Peripherer Nerv; MG, myasthenia gravis; MS, multiple sclerosis; Myo, myositis.
Taking into account the distribution of the population, the geospatial isochrone coverage can further yield valuable information on healthcare access for the German population. In this context, 64.2% of Germans can reach an MS-centre (KKNMS or DMSG) within 30 minutes of driving time, 96.5% within 60 minutes, and 99.9% within 120 minutes. For the rare diseases, the MG iMZ centres cover 21.3% of the population within 30 minutes of driving time. For myositis and the immune-mediated neuropathies focused KKPNS, the respective numbers are 16.2% and 20.5%. These numbers increased at 60 minutes of driving time to 48.3% for MG iMZ, 56.7% for KKPNS, and 43.1% for myositis and reached 93.0% (MG), 97.4% (KKPNS), and 83.8% (myositis) at 120 minutes (see Table 1).
Overview of the German population covered by the respective isochrone areas for different care networks.

Of note, all three analysed networks for rare diseases additionally showed some specific regional underrepresentation: Northern Germany for the myositis centres, Eastern and Southern Germany for the MG iMZ centres and central Germany for the peripheral nerve inflammation focusing KKPNS network. The region of North-Eastern Germany showed a less complete coverage across all analysed networks.
Discussion
Even in countries with a well-developed healthcare system, such as Germany, the healthcare and disease burden remains high for patients suffering from rare neurological diseases. As specialised care is needed for the state-of-the-art treatment of neuroinflammatory diseases, new approaches to healthcare are urgently needed to overcome the limited accessibility to specialised centres. Here, we used a new technique to detect the regional healthcare coverage gap for neuroinflammatory diseases. Our method easily identifies underserved regions and highlights the burden of patients and caregivers due to the real-world driving time.
The GHS-POP19 dataset used as population approximation method in this study has shown remarkable accuracy in other European countries. 27 Additionally, data generated by our method using GHS-POP19 align with published data from the German Federal Statistical Office, 28 with both sources relying on German 2011 census data. As isochrones rely on car access, a few areas that cannot be reached by car directly, such as certain maritime islands, and their population, were not included in the analysis. However, this should not influence relative population size as we estimate that less than 0.15% of the German population are not included in the analyses. The role of longer journeys for patients with rare neuroinflammatory diseases to their treating physicians were also investigated in a representative study involving 1634 German MG patients. 3 Of these, 17.6% had to drive more than 50 km, with patients treated in a specialised iMZ centre driving longer distances on average (unpublished data). In our study, all analysed networks enable more than 80% of the German population to reach one of the specialised centres within 120 minutes by car under normal traffic conditions. However, there are considerable differences between the well-established MS-focused networks, which cover almost the entire population, and rare-disease networks such as the ‘Myositisnetz’ for myositis, which only two-thirds of the population can reach within 90 minutes of driving. In particular, we also identified regional differences in healthcare coverage. Especially in the North-Eastern part of Germany, we observed inadequate coverage across all rare disease entities. Similar to the finding that rural areas are generally less well covered, this finding is consistent with data from a report analysing medical access across Germany in 2017. 29
Long driving times to medical facilities are associated with worse health outcomes in many studies, 30 and driving time is a more patient-centred and accurate proxy for access than mere distance. 31 As the number of neurologists is limited and modern demands make it impossible to specialise in many indications, it appears unlikely to establish proper patient-care coverage for the often severely impaired patients in more remote regions. Our analyses easily and rapidly demask such regional differences in healthcare coverage and could thus serve as a foundation to deploy DHT in a disease- and region-specific manner. Specialised care networks could expand their reach by applying remote monitoring and care solutions combined with telemedicine approaches for local doctors to consult with rare disease specialists.32,33 Similarly, action plans for rare diseases, such as the German National Plan of Action for People with Rare Diseases, explicitly call for integrating digital solutions into outpatient care to distribute knowledge to the point of care.34,35 Such approaches could reduce the patient and caregiver burden, increase access to healthcare in rural regions, and reduce the ecological footprint of medical care by reducing the often necessary long car rides.
Overall, future studies could investigate the real-world accessibility of many other healthcare entities for different diseases using the here advocated isochrone-based methodology.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231152989 - Supplemental material for Driving time-based identification of gaps in specialised care coverage: An example of neuroinflammatory diseases in Germany
Supplemental material, sj-docx-1-dhj-10.1177_20552076231152989 for Driving time-based identification of gaps in specialised care coverage: An example of neuroinflammatory diseases in Germany by Lars Masanneck, Saskia Räuber, Christina B Schroeter, Sophie Lehnerer, Tjalf Ziemssen, Tobias Ruck, Sven G. Meuth and Marc Pawlitzki in Digital Health
Footnotes
Acknowledgements
The authors would like to thank the open-source community for providing powerful research tools.
Author contributions
LM and MP researched the literature and conceived the study. LM wrote the code and conducted the first data analysis. SR, CB and SL gathered relevant data and assisted in the analysis as well as critically reviewed and edited the manuscript. LM and MP wrote the first draft of the manuscript. TZ, TR and SGM helped to clarify the research question, reviewed the data and provided feedback and funding. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LM received personal fees from Biogen and Merck. SR declares no conflict of interest, CBS declares no conflict of interest. SL has received speakeŕs honoraria and honoraria for attendance at advisory boards from Alexion and Argenx. TZ personal compensation and project support from Alexion, Almirall, Biogen, Bristol Myers Squibb, Janssen, Novartis, Roche, Sanofi, and Teva. TR reports grants from German Ministry of Education, Science, Research and Technology, grants and personal fees from Sanofi-Aventis and Alexion; personal fees from Biogen Idec, Roche and Teva; personal fees and nonfinancial support from Merck Serono, outside the submitted work. SGM received honoraria for lecturing and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer HealthCare, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS, and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Bundesinstitut für Risikobewertung (BfR), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, Gemeinsamer Bundesausschuss (G-BA), German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and by Alexion, Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, HERZ Burgdorf, Merck Serono, Novartis, ONO Pharma, Roche, and Teva. MP received honoraria for lecturing from Argenx, Biogen and Merck. He received research funding from Novartis. His research is funded by the German Multiple Sclerosis Society North Rhine-Westphalia (DMSG) and the programme ‘Innovative Medizinische Forschung’ (IMF) of the Medical Faculty of the University of Muenster.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
No ethical approval was necessary as this study worked with publicly available anonymous data.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.