
Abstract
Background
Artificial intelligence (AI) Healthcare applications are listed in the national visions of some Gulf Cooperation Council countries. A successful use of AI depends on the attitude and perception of medical experts of its applications.
Objective
To evaluate physicians and medical students’ attitude and perception on AI applications in healthcare.
Method
A web-based survey was disseminated by email to physicians and medical students.
Results
A total of 293 (82 physicians and 211 medical students) individuals have participated (response rate is 27%). Seven participants (9%) reported knowing nothing about AI, while 208 (69%) were aware that it is an emerging field and would like to learn about it. Concerns about AI impact on physicians’ employability were not prominent. Instead, the majority (n=159) agreed that new positions will be created and the job market for those who embrace AI will increase. They reported willingness to adapt AI in practice if it was incorporated in international guidelines (30.5%), published in respected scientific journals (17.1%), or included in formal training (12.2%). Almost two of the three participants agreed that dedicated courses will help them to implement AI. The most commonly reported problem of AI is its inability to provide opinions in unexpected scenarios. Half of the participants think that both the manufacturer and physicians should be legally liable for medical errors occur due to AI-based decision support tools while more than one-third (36.77%) think that physicians who make the final decision should be legally liable. Senior physicians were found to be less familiar with AI and more concerned about physicians’ legal liability in case of a medical error.
Conclusion
Physicians and medical students showed positive attitudes and willingness to learn about AI applications in healthcare. Introducing AI learning objectives or short courses in medical curriculum would help to equip physicians with the needed skills for AI-augmented healthcare system.
Introduction
Artificial intelligence (AI) is “the ability of computer systems to perform tasks that would usually require human levels of intelligence.” 1 AI applications recently witnessed substantial growth across many industries including healthcare. Machine learning is thought to transform healthcare systems profoundly in the coming years. 2 A plethora applications have been developed that aim to improve different aspects of clinical work such as improving medication compliance, 3 reducing waiting time at outpatient clinics, 4 providing fast reporting for medical imaging, 5 and other reported benefits. 2 Machine learning has been reported to outperform physicians in some such as detecting breast cancer in mammogram images. 6 It was implemented at higher scale during the COVID-19 pandemic to improve disease diagnosis, trace tracking, and intensive care unit admission prediction. 7 Some of these AI-based algorithms have been approved by the American Food and Drug Administration for clinical use. 2
Despite the rapid global progress in research and development in innovative medical AI technologies, there are several barriers that hinder its clinical use at a wider scale. 8 Resistance to adopt AI among physicians has been reported frequently.9,10 On the other hand, other studies have reported an optimistic view that medical AI technologies will augment physicians’ work and allow them to direct their time toward more cognitive and higher-order skills. 11
Future healthcare professionals will directly use software, applications, and machines that are AI powered. To be able to implement such applications with ease, future doctors should be equipped with the needed knowledge and basic skills to understand and deal with such machines and softwares. They should be aware of the advantages and disadvantages of AI-powered medical technologies and acquire the needed skills to work in the upcoming AI medical ecosystem. 12 It is even expected that AI will be a main element in the medical curriculum in the future. 13 There is no agreement on how much and where AI should be introduced in medical education. Experts agree that medical curriculum should not introduce sophisticated technical tools; instead, an understanding of the topic, its uses, applications, disadvantages, limitations, and data management are the main areas to be highlighted. 14 There is a growing movement to include such topics in both undergraduate and postgraduate formal medical curricula.
In Oman, the healthcare system at the primary, secondary, and tertiary levels had undergone a digital transformation a long time ago and become fully digitized by the years 2008 to 2009. Since then, all patients’ records are available online through password-encrypted hospital access. The aim was to improve clinical care delivery, and patients’ experience and enhance the care operational efficiencies. With time the amount of digital data available that needs to be studied and mined to improve care necessitates enhancing digital literacy among current and future physicians. Physicians are usually not equipped with digital skills or are even unaware of the benefits of such big data and the applicability of AI techniques in their field. There is an ongoing discussion to introduce an AI-oriented learning objective in the medical curriculum at both the undergraduate and postgraduate levels in Oman. Therefore, the objective of this study is to evaluate and analyze familiarity, attitudes, and perceptions of physicians, trainees, and medical students about medical AI applications. This is a preliminary step to evaluate the baseline knowledge and readiness before introducing AI into the medical curriculum in our institute. To the best of our knowledge, this is the first study that evaluates the perceptions and attitudes of physicians, trainees, and medical students toward medical AI applications in the same setting. Previous studies have analyzed the views of either medical students or physicians in different settings.15–17
Method
Study population
This study was approved by the ethical committee from Sultan Qaboos University (reference no. 2078). Google Form was used to construct the questionnaire which was disseminated among physicians working at tertiary hospitals, interns, and residents from the Oman Medical Specialty Board, and medical students from the College of Medicine at Sultan Qaboos University through institutional emails. Participation was voluntary and all participants were consented and informed about the goal of the survey in the preface of the questionnaire. The IBM definition of “Artificial Intelligence in Medicine” was introduced in the preface of the survey which stated that: “Artificial intelligence (AI) in medicine is the use of machine learning models to search medical data and uncover insights to help improve health outcomes and patient experiences.”
The questionnaire
An anonymized survey was adapted and modified with permission from Goh and Sandars 13 and Masters. 12 The survey is composed of 25 closed-ended questions (Supplemental Appendix A) distributed among 5 sections as follows: demographics section (6 items), familiarity section (2 items), attitude section (14 items), expected application in medicine section (3 items), and possible risks section (1 item). Five of the questions used a 5-point ordinal Likert scale (1=strongly disagree to 5=strongly agree). The remaining 20 questions were constructed as multiple-choice questions. The survey was piloted and the reliability scores of the different sections of the survey were computed and all the sections have been modified accordingly. The calculated Cronbach’s scores for the sections were all >0.78, which indicates good inter-item reliability.
Statistical analysis
Basic statistics were computed for all covariates where continuous variables are expressed as mean, standard deviation, median, minimum, and maximum values, and categorical variables as frequency (n) and percentages (%). Pearson analysis was done to evaluate the effect of different demographic factors such as age, gender, and years of experience, on the participants’ responses to different items. For all tests, the level of significance was set at a p-value of ≤ 0.05.
Results
Respondent demographics
The survey was disseminated to 300 physicians and trainees and 750 registered medical students. A total of 293 (82 physicians and 211 medical students) have responded to the survey with a response rate of 27% and 28%, respectively. The sociodemographic and professional characteristics of the participants are shown in Table 1.
Demographic and professional descriptions of survey participants.

ENT: ear, nose, and throat.
About 177 (60.4%) of the total participants were females. Almost half (57.31%) of the physicians reported 10 or fewer years of medical practice and the other half has practiced for more than 10 years. The participating students were mainly from preclinical years (77.73%).
Familiarity
Both physicians and medical students reported being familiar that AI as a new and emerging tool in medicine (21%, and 48%, respectively) and they would like to learn more about its applications in medicine (16% and 33%, respectively; Table 2). More than half (165, 56%) of all participants have not attended a talk or read papers that focus on using AI to make interpretations, diagnostic or prognostic within the past 1 year. Only 7 (8.5%) physicians reported reading or attending 5 or more articles/talks about AI in the last year. The remaining participants reported reading or attending less than five articles/talks. Age and year of experience of the participants were found to be statically negatively associated with familiarity with AI applications in healthcare. The older physicians with more years of experience were found to be less familiar with AI and its application in medicine (p-value <0.05; Table 3). There was no association between gender and familiarity level (p-value >0.5).
Familiarity of the participants with AI applications in healthcare.

AI: artificial intelligence.
The association of different sections with the participants’ demographics.

The bold values indicates significance P value.
Analysis of the five Likert scale questions from different subscales is shown in Table 4. The most perceived concerns regarding AI application in medicine are that it “Cannot be used to provide opinions in unexpected situations” and is “Difficult to apply to controversial issues.” The most perceived advantage was the AI's ability to “Speed up the management process in health care” and “can deliver clinically relevant and high-quality data in real-time.” The majority of the participant reported being neither agree nor disagree with the questions related to the item about AI replacing medical doctors. Almost half of the participants (n=159) reported that “AI will create new positions and increase the job market for those who embrace it.” Overall, the concerns about physicians’ replacement and the impact on physicians’ employability were not prominent. Almost 35% (n=105) of participants reported that “fewer doctors will be trained in some profession” and 20% (n=60) think that “currently trained doctors in some medical profession will lose their positions.” Most of the participants neither agree nor disagree that the integration of AI in their profession will affect efficiency. More than half of the participants agree that with the appropriate training, AI could increase the efficiency of their practice. When asked about their readiness—from a training perspective—to implement AI in their work, 82% (n=249) of the participants agreed that with dedicated courses and workshops, they can start implementing AI in their practice.
Analysis of Likert scale of the survey sections.
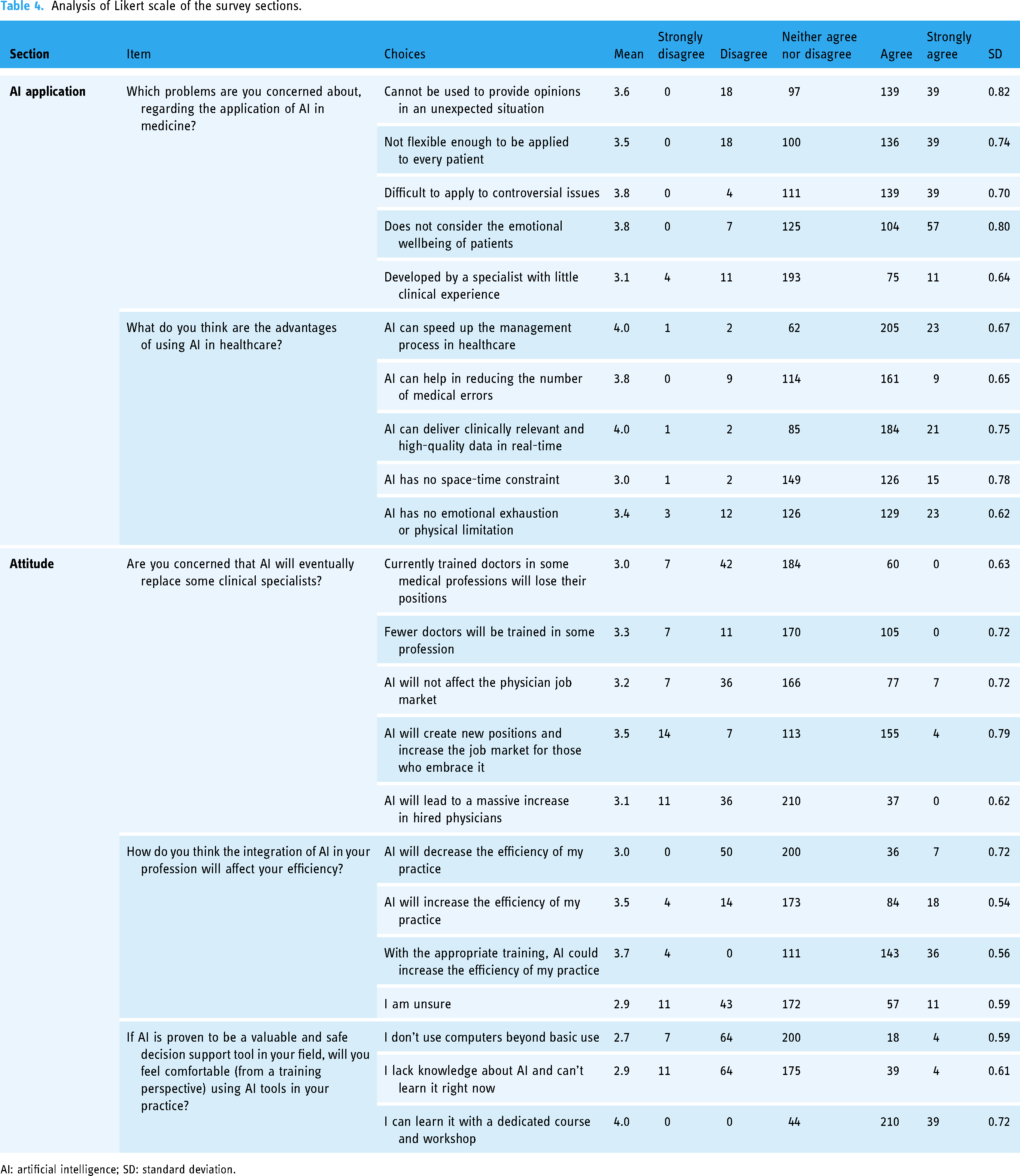
AI: artificial intelligence; SD: standard deviation.
Attitude
Overall, participants expressed a positive attitude toward AI applications in healthcare. They reported willingness to adapt AI tools in clinical practice if it was incorporated in the international guideline (30.5%), published in highly respected scientific journals (17.1%), included in formal training (12.2%) or if adopted by leaders in their filed (8.5%; Figure 1). Twenty percent of the participants reported actively seeking new technologies and 11% are ready to adapt new technologies regardless of where they are published.

Willingness to incorporate new technological advances in clinical practice among the participants.
All 69 (23.55%) participants showed interest to learn more about AI if dedicated courses and training are offered. Two-third (78%) of the participants expressed their willingness to adopt an AI-based decision support tool in their practice if it could help to devote more time to other clinical, academic, and/or research activities.
The vast majority of participants (55% physicians and 62.5% students) strongly believe that AI use in image analysis in radiology, pathology, and dermatology will be cost-effective. The remaining participants think it will not be cost-effective or don’t know if it will be cost-effective which could be due to a lack of understanding and knowledge about AI and its use.
Nearly half of the participants reported that image-based specialties such as pathology, dermatology, and radiology will be the first to adopt AI tools followed by surgical procedures and public primary care (Figure 2). Overall, many respondents predicted the integration of AI into diagnostic workflow within the next 5 years (28%) or 10 years (31.7%). The remaining (39%) predicted that it will need more than 15 years for such implementation (Figure 3). Furthermore, participants believed that AI tools application in healthcare would improve the quality of care (51.2%), research productivity (78%), and improve teaching responsibilities (45%).

Healthcare sectors to adopt artificial intelligence at a higher scale.

Respondent perception of the period needed for artificial intelligence to be a major routine tool in medical practice.
When asked about how their colleagues and patients would perceive AI tools if applied in clinical practice, most of the participants (84%) agreed that they would perceive AI tools very well if they are offered proper education and awareness.
The attitude of the participants was not found to be statistically associated with age, gender, or year of experience (p-value >0.5; Table 3).
Risk
Among all participants, more than one-third (36.77%) think that the physicians who make the final decision should be legally liable for any medical error occurred when a physician uses an AI-based decision support tool while (6.19%) think it is the manufacturer of the AI tool who should be liable and (48.45%) believed that both the manufacturer of the AI technology and the physician are legally liable (Figure 4).

Who should be held legally liable for medical errors caused by artificial intelligence-based medical software?
The majority (63.5%) of the participants reported that they will follow the physician's opinion in case of conflict between an AI tool and the treating physician’s decision, 24.2% will go by patient's choice, 6.49% will consult a colleague, and 17% will follow AI opinion.
This was significantly and negatively associated with the age and year of experience of the participants (p-value <0.05; Table 4). Older age physicians and those with more years of experience reported that the physicians who took the decision are to be legally liable for any medical errors resulting from the AI-based decision support tool. On the other hand, younger physicians with fewer years of experience and medical students reported that both the manufacturer and the physician should be legally liable for such medical errors.
Discussion
The current healthcare systems in the Arab countries in general and the Gulf Cooperation Council (GCC) specifically is complex due to the challenge to reach an equilibrium between the quality and cost of care, technology, and maintaining humanity.18,19 Some GCC states have AI in healthcare applications as a core objective of the country's national vision.20,21 These strategies put AI at the core of the corresponding country’s development and growth. The successful use of AI in healthcare depends on the awareness and perception of medical experts of its applications. 22 To the best of our knowledge, this is one of the few studies in the GCC countries 23 to evaluate the opinions and attitudes of physicians and medical students on AI medical applications. Overall, we found that both physicians and medical students across all specialties and years of experience have a positive perspective about the future use of AI in healthcare which is similar to the previously reported attitude.11,24 There is a generally low familiarity with AI, especially among older and senior physicians. However, the majority have reported eagerness to learn and apply AI tools if dedicated courses and workshops are offered and if included in international guidelines and formal training.25–27 AI replacing physicians was not a concern of physicians and medical students in Oman which is consistent with findings from other studies10,28–30 but not consistent with a recent study from Saudi Arabia. 23 Some participants did report a fear that some medical professions might be largely impacted and the training in these professions will be modified to adapt to working with machines especially image-based and laboratory-based specialties. This fear was mainly reported by young physicians and medical students.
According to Bodenheimer, 31 only 27% of physicians’ time is spent on direct clinical face-to-face duties with their patients and about 49.2% of their time is spent on electronic hospital records and desk work. In this study, 78% of participants expressed their willingness to adopt AI tools if they can direct their time toward more focused clinical-oriented tasks. The major advantage of AI as perceived by all participants in this study is AI can speed up the process of healthcare followed by providing high-quality care in real-time and reduce medical errors which are similar to perceived advantages in earlier studies.10,11,23,25–27 On the other hand, there are major concerns reported for AI in healthcare such as its inability to provide an opinion in an unexpected situation, lack of empathy, and concerns about the feasibility of AI use in controversial issues are similar to what was reported earlier.10,24
Senior physicians reported that it is both the manufacturer and the physicians who implemented the AI decision support tool to be held legally liable for any resulting medical errors. This was explained earlier as one of the causes for physicians’ resistance to the innovative technology in healthcare 32 since they evaluate such technologies by their abilities to provide secure and reliable care. Generally, it is both the physician's and patient's acceptance of the new technologies that determine the successful implementation. Reports showed that patients are more excited about innovative technologies in healthcare than physicians because it gives them greater autonomy in their healthcare plans. 33
The reported resistance especially among senior physicians could be explained by the lack of awareness and competencies. In a systematic review to study the major barriers to successful digital health applications in developing countries in general and Arab countries specifically, a lack of technical competencies and knowledge among healthcare workers was reported as one of the main barriers. 34 Furthermore, the professional identity of physicians was claimed to be a barrier to innovative technologies implementation in the GCC countries. 35 Despite all of these reported barriers, physicians who participated in this study showed an overall willingness to learn about AI applications and are ready to implement them once introduced in clinical guidelines.
Therefore, to improve knowledge and acceptance, efforts should be directed toward constructing learning sessions and a medical curriculum that exposes healthcare workers and medical students to AI and its applications to prepare future doctors to work along with AI machines and software. This was clearly stated in the 2018 American Medical Association report that proposed the use of the term “augmented intelligence” instead of AI as the physician job is far from full automation. 36 AI will augment and facilitate the job of physicians where the future healthcare system will be a teamwork between physicians and machines instead of a competitive environment.37–39 This would be of great impact in places with expert shortages and high-demand institutes, especially in image-based specialties. It was very obvious during the COVID-19 pandemic, that AI has been very powerful to speed up the vaccine and drug discovery process instead of the usual laborious, costly, and time-consuming clinical trials and laboratory studies. 7 It is not meant to provide a final diagnosis but is found to assist human physicians in detecting suspicious images and filtering them from normal ones. This would be very helpful to devote physicians’ time to evaluating suspicious cases deeply.
Conclusion
The united triple aim of healthcare has been largely impacted by the increased incidence of different chronic and acute illnesses that needs prolonged management plans and the availability of huge medical data. Therefore, technological solutions have proven their abilities to handle such big data and offer smart and fast solutions. According to a Forbes report in 2019, AI applications in healthcare would serve the triple aim of healthcare as it will cut the cost of care, improve accessibility, and improve treatment. Physicians and medical students are showing curiosity and a positive attitude toward future applications of AI in healthcare. It is well known that healthcare providers have typical resistance to change unless the change has been tried and tested thoroughly. Therefore, there is an unmet need to include AI in healthcare training, and construct dedicated courses/workshops for physicians and medical students. There is a need as well for a regulatory and multidimensional framework that lists the detailed responsibilities of stakeholders, legislations, and logistics for future AI applications.
Limitations
The relatively small size of physician participants is one of the limitations of our study which impacted the possibility of detecting statistical significance between different professions. Furthermore, since the survey was disseminated online, selection bias could impact the results as physicians and students who are interested in AI are more likely to participate and provide a positive perception.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231152167 - Supplemental material for Are physicians and medical students ready for artificial intelligence applications in healthcare?
Supplemental material, sj-docx-1-dhj-10.1177_20552076231152167 for Are physicians and medical students ready for artificial intelligence applications in healthcare? by Adhari AlZaabi, Saleh AlMaskari and Abdulrahman AalAbdulsalam in Digital Health
Footnotes
Acknowledgment
Author contributions
The study conception and design were by AALZ. All authors contributed to the manuscript write-up. The compilation of all sections and the construction of headings and figures were done by AALZ and AAA. The first draft of the manuscript was written by all authors. The manuscript was proofread by AAA and SA. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The project has been approved by the Ethical committee of the College of Medicine and health sciences.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AA.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.