
Abstract
Objective
Combining continuous positive airway pressure with physical activity (PA) might be a promising strategy to treat obstructive sleep apnea (OSA). This article describes how intervention mapping (IM) can guide the development, content, and mechanisms of action of a mobile application to promote PA in adults with OSA.
Methods
To develop the program, the IM approach was followed. This article presents the first three steps of IM to develop a mixed intervention (with interventionists and a digital application) aiming to: (1) assess patients’ health problems and needs in a literature review to determine their expectations and perceived facilitators and barriers to PA behavior change and thus select the determinants of behavior; (2) formulate the expected intervention outcomes and objectives to be met to achieve the overall program goals; and (3) select and implement the behavior change techniques (BCTs) to achieve the change objectives.
Results
The literature review identified the relevant determinants (e.g., self-efficacy, coping, planning, and habit) of PA behavior using the health action process approach and multiprocess action control. These results were used to specify the program outcomes for PA adapted to physical, psychological, and social parameters. Overall, 11 performance objectives and 30 change objectives were defined. Lastly, BCTs and practical applications were identified.
Conclusions
The study provides a theoretical and methodological basis for researchers and practitioners given the current paucity of evidence-based PA interventions for adults with OSA. It addresses the lack of BCTs (framing and prompts/cue techniques) and meaningful behavioral determinants (identity and habit) in most interventions.
Keywords
Background
Obstructive sleep apnea (OSA) is the repeated complete or partial obstruction of the upper airway during sleep, with brief arousals leading to significant sleep fragmentation. OSA is quite prevalent, 1 showing regional disparities (i.e. 9–38% in Europe and North America and 8.8–24.2% in China)2,3 and affecting 4% of middle-aged men and 2% of middle-aged women, 4 with prevalence increasing with age. 5 The 5-year incidence of OSA was estimated at 7% to 11% in middle-aged adults. 2 The consequences of OSA include cognitive and behavioral deficits such as excessive daytime sleepiness that can affect daily life (e.g. work performance) as well as cardiovascular and metabolic dysfunction. 6 Moreover, overweight is the most important risk factor for OSA, and around 70% of individuals with OSA are obese. 7
First-line treatment for OSA is continuous positive airway pressure (CPAP), which has a beneficial effect on breathing during sleep and thus contributes to reducing the OSA severity index (i.e. apnea-hypopnea index or AHI) and excessive daytime sleepiness as well as improving sleep quality. However, long-term CPAP effectiveness remains limited due to low adherence, 8 while an absence of protective effects against secondary problems such as cardiovascular disease and stroke has been demonstrated. 9
Previous evidence supports the value of exploring other potential strategies such as introducing physical activity (PA) in complement to CPAP. Indeed, the efficacy of lifestyle changes for OSA has been reported in several meta-analyses.10,11 For example, PA has positive effects on AHI in terms of rapid eye movement (REM) and non-REM sleep, subjective sleepiness, cardiometabolic risk factors associated with OSA, and VO2peak, which is associated with a significant survival benefit.11–14 However, individuals with OSA report low levels of PA and have low aerobic capacity. 11 Their symptoms may hamper daily life activities in several ways, and PA appears to decrease with increasing AHI. 15 Hence, there is a strong need to combine CPAP and PA for patients with OSA in order to optimize risk factor control and reduce long-term morbimortality. 11
Among the systematic reviews and meta-analyses examining the effect of PA in the context of OSA,10,11,13,16–23 only one focused on an outcome associated with PA behavior (i.e. number of steps). In this meta-analysis, three randomized controlled trials (RCTs) investigated the effects of physical exercise24,25 or a lifestyle intervention 26 on PA levels. Only one trial observed increased PA levels after the intervention in patients with OSA and coronary artery disease. 25 Since the publication of this meta-analysis, three studies have measured PA levels,27–29 but only Black et al. 28 and Berger et al. 29 evaluated this outcome (i.e. PA questionnaire and accelerometer: unit in counts) before and after the intervention. Both studies showed an increase in PA following the intervention, which then decreased after 12 months. 29 Many studies have focused on the effects of PA interventions on the parameters associated with OSA.12,24,25,27,28,30–41 By contrast, few have explicitly investigated the effect of a PA intervention on PA behavior itself using objective 26 or subjective measurements. 29 This limited number of studies integrating the outcome of PA is surprising insofar as CPAP, as the first-line treatment of OSA, has a limited impact on cardiometabolic risk factors, whereas exercise training has a well-documented effect on numerous cardiometabolic risk factors. 11
In individuals with chronic disease, several prospective studies have shown a positive association between motivation and PA behavior.42–44 Thus, increasing patients’ motivation for PA seems pertinent in order to increase their PA level. Studies have also demonstrated that the intention to perform a behavior is necessary45–47 but insufficient to initiate the new behavior,48,49 thus suggesting that the psychological processes associated with behavior change are manifold. Indeed, many factors contribute to the initiation of PA50–56 and its maintenance.57–61 In the literature, these constructs have been associated with small to large effect sizes to explain behavior change. Therefore, focusing on the determinants of behavior seems paramount to understanding how to develop more effective PA interventions.52,62 In the context of OSA, however, only one study measuring the effect of a PA intervention also assessed a variable associated with motivation 27 prior to the intervention. To date, no study has integrated these factors as an outcome both before and after the intervention. These results point to the need for RCTs to investigate the effects of PA interventions on PA behavior itself and its determinants in order to develop more effective interventions.
Bearing this aim in mind, the first critical step is to identify the effective and efficient intervention components to change the behavioral determinants 63 : for example, a behavior change theory to underpin the intervention and operational constructs to be targeted, 64 behavior change techniques (BCTs), 65 and modes of intervention delivery (e.g. frequency and duration of contact, individual/group delivery). All these components make it possible to build the necessary links between BCTs (i.e. observable, replicable, and irreducible components of an intervention designed to alter or redirect the causal processes that regulate behavior 65 ) and the factors associated with motivation (e.g. instrumental attitude representing the expected long-term utility of performing PA), as well as between these factors and PA behavior.52,66–71 For instance, if the BCT “information about health consequences” is used to provide scenario-based risk information, it is assumed that this will influence risk perception, 72 which will in turn prompt people to formulate an intention to engage in PA to reduce the risk. 73 Indeed, theoretical knowledge might facilitate the greater inclusion and precision of BCTs in PA interventions, thereby targeting behavior more effectively compared to no-stated-theory interventions. This may even be necessary to derive significant effects. 74 Theory-based interventions are significantly effective in promoting PA, 75 and indeed, behavioral theory-based interventions have been recommended in the guidelines for PA interventions in the general population. 76 These include social cognitive approaches such as the theory of planned behavior, 77 social cognitive theory,78,79 transtheoretical model, 80 and health action process approach (HAPA) 73 in addition to dual process frameworks. 81 To structure the description of content, the v1 taxonomy of BCTs 65 is known to improve the ability of researchers, practitioners, and policymakers to interpret and replicate effective interventions. 82 This taxonomy comprises an extensive hierarchical classification of clearly, distinctly (i.e. no overlap, no redundancy), and precisely labeled BCTs. Among the techniques identified as effective in positively impacting the determinants of PA are “feedback on behavior”52,66,68 and “self-monitoring of behavior.”52,66,68,69,83,84 In practice, however, the duration of self-monitoring with diaries and feedback may be limited by cost and time constraints. Moreover, common traditional interventions include advice from professionals, educational materials, and face-to-face approaches, but these have high resource requirements and are impractical for widespread implementation. 85 To overcome these limitations, mobile health (mHealth) interventions may be a promising mode of delivery. 86 mHealth interventions refer to “medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants, and other wireless devices.” 87 mHealth applications (apps) have unique advantages, as they allow for continuous monitoring that provides the basis for individualized feedback and goal setting. 88
Even though behavior change interventions are not in their infancy, many evidence gaps remain. Thus, more evidence-based studies are needed to improve the significance of the results. These should describe the intervention content (e.g. BCTs) and application functionalities in sufficient detail to allow for the reproduction of the study and the advancement of this research area.62,85,86,89,90 To respond to these needs, the intervention mapping (IM) framework 91 seems relevant. Indeed, this theory-based and evidence-based approach enables interventionists and developers to plan, develop, implement, and evaluate health promotion programs in a systematic way. Moreover, IM ensures that the intervention development deals with the three aspects associated with the dynamics of behavior change.92,93 First, the behavior change methods should be chosen by matching them with the determinants that they are likely to impact; second, a precursor to the intervention development should ensure that these determinants predict the relevant behavior; and third, when change methods are applied, the parameters evaluating the effectiveness of the method must be satisfied. Lastly, the IM framework should include evidence-based techniques and behavior change theories.
To promote regular PA behavior in adults with OSA undergoing CPAP treatment, we developed a mixed intervention delivered to patients with OSA in an everyday setting by both health professionals in a healthcare organization and an mHealth app. For 6 months, multifaceted content is provided either face-to-face or remotely (phone or video) in individual or group sessions. Moreover, patients stay in regular contact with a care manager who can ensure continuous follow-up and refer them to specific professionals (e.g. physician, specialist in adapted PA) if necessary.
This article aims to describe how the IM framework was used to develop a theory-based and evidence-based mHealth intervention to promote regular PA in patients with OSA.
Method
Intervention mapping approach
IM is composed of six steps 94 : (1) problem analysis, (2) identification of program outcomes and objectives, (3) selecting theoretical methods and practical strategies for program design, (4) program production, (5) program implementation planning, and (6) evaluation planning. This article presents the first three steps of IM using as an example of our development of a mixed intervention for individuals with OSA (with interventionists and a digital app). Indeed, the first version of the app will be tested in a multicenter clinical RCT to evaluate its acceptability, usability, organizational barriers, and effectiveness. To guide the development process of this intervention, a development group was established consisting of two researchers in psychology and behavior sciences (CL and JB) and an expert in adapted PA with professional experience in respiratory rehabilitation (BC).
Step 1: Problem analysis
This first step of IM is to fully describe the health problem, assess the needs (qualitative or quantitative modalities) of stakeholders, and identify the determinants of the behaviors to be modified individually in the targeted population. In the IM protocol, these determinants are combined with key concepts from social and health psychology (e.g. knowledge, skills, self-efficacy, outcome expectations, perceived social norms) to identify the best theories to explain the problem.
The relevant literature on OSA was systematically reviewed in the PubMed database to identify the studies exploring patient expectations about PA behavior change and the perceived facilitators and barriers for PA engagement. The titles, keywords, and abstracts of papers were screened with terms referring to (1) barrier or facilitator, (2) obstructive sleep apnea, and (3) physical activity. Studies about adults with OSA that explored barriers or facilitators to PA were thus included.
Next, the development group selected the important and modifiable determinants of PA behavior. According to the IM approach, the importance of the determinants relates to their relationship with the current behavior of participants. The development group established the determinants that could be impacted by an intervention, and the importance of these determinants was determined based on group consensus and the available scientific literature.52,55,56,62,63,65,66,68–71,82,83,95–98
Step 2: Identification of program outcomes and objectives
The second step consists of formulating the expected intervention outcomes and the objectives that need to change in order to achieve the overall goal of the program—that is, for adults with OSA to adopt healthy PA behavior in order to prevent health complications. The performance objectives (PO) formalized the behavior changes that patients with OSA need to implement to achieve the behavioral goals of the program (program outcomes). For each program outcome, one researcher (CL) defined what, in concrete terms, the participants would need to do in the program to reach the desired behavior (POs). Next, the same researcher identified the useful behavioral determinants to effect change with regard to each PO. For example, for the PO “patients learn to perform the physical activity behavior,” the appropriate determinants are “self-efficacy,” “knowledge,” and “skills.” Next, change objectives that state the expected program effects on the determinants were formulated by combining the POs with the changeable determinants of PA behavior. Thus, for “self-efficacy,” which is included in the PO“patients learn to perform the physical activity behavior,” the change objective is to “feel confident in their ability to perform the physical activity behavior without support.” Finally, an IM matrix was built. The matrix specifies the POs, behavioral determinants, and change objectives, which were subsequently validated by the group.
Step 3: Selecting theoretical methods and practical strategies for program design
The third step involves selecting the techniques (or theoretical methods) and determining how to implement them to achieve the formulated change objectives. A BCT is an observable, replicable, and irreducible component of an intervention designed to alter or redirect the causal processes that regulate behavior. For example, “problem-solving” involves analyzing the factors that influence the behavior and selecting the strategies that include overcoming barriers.62,65
For each behavioral determinant and in conjunction with the change objective, one researcher (CL) selected the techniques based on the literature of currently used PA promotion interventions52,56,58,66,68–70,83,84,99–118 and the tools to understand them.62,65,97,119 For example, to reach the change objective “feel confident in their ability to perform the physical activity behavior without support,” we selected the techniques “instructions about how to perform a behavior,” “demonstration of the behavior,” and “behavioral practice/rehearsal” to change the determinant “self-efficacy.”
The development group chose the conditions under which the methods were shown to be effective and then translated the selected methods into practical strategies. A practical strategy is “a specific application of a theoretical method, adjusted to the intervention setting, tailored to the target population, and applied considering parameters for effective use of the methods.” 94 For example, the selected method “self-monitoring of behavior” was translated into the practical strategy “every week, data associated with self-monitoring are interpreted and provided to the patient via visual and understandable feedback (text messages).”
Results
Step 1: Problem analysis
Out of 64 papers, the systematic literature review revealed only one study that had conducted semistructured individual interviews with 15 patients with OSA. 120 This study aimed to explore the aspects of engagement (i.e. expectations, perceived facilitators, and barriers) in PA in overweight adults with OSA. The transcribed data were analyzed according to qualitative content analysis. Two themes reflected the influences on PA engagement: (1) strong enough incentives and (2) facilitators for success and challenges to overcome. Moreover, the conception of the intervention was based on previous work carried out by our team in obese patients, many of whom had OSA. 98 In this qualitative study, a self-administered questionnaire was completed by 151 patients with chronic diseases (chronic obstructive pulmonary disease, cardiovascular disease, obesity, diabetes, or OSA) to determine the barriers and facilitators of patient adhesion to a mobile digital telerehabilitation solution that proposes personalized interventions for patients. The analyses of both qualitative studies revealed that the psychosocial factors that emerged were “risk perception,” “outcome expectancies,” “self-efficacy,” “social support,” “action planning,” and “coping planning.” These factors are part of the HAPA theory. 73 Although HAPA has not been used in the context of OSA, it is a promising framework that constitutes a relevant theoretical backdrop for intervention designs to improve PA levels in adults with obesity. 42 HAPA is a social-cognitive dual-phase model that identifies the determinants for the initiation and maintenance of health behavior (Figure 1). Behavioral intention is a pivotal construct in this model. The model differentiates two distinct phases, each comprising different sets of constructs that determine behavioral enactment. Thus, the motivational phase encompasses outcome expectancies, action self-efficacy, and risk perceptions, whereas the volitional phase includes maintenance and recovery self-efficacy as well as action and coping planning. Furthermore, social support seems to be related to both intention and PA. A meta-analysis that identified the effects of HAPA constructs on PA 121 showed significant effect sizes ranging from 0.13 to 0.43 depending on the construct. These results provide evidence that all HAPA variables are useful to predict PA. Moreover, after applying structural equation modeling, the fit of the HAPA model was deemed satisfactory, explaining 30% of the variance for intention and 18% of the variance for PA in obese adults. 42 Thus, to develop a PA intervention, the HAPA theory seems relevant.

Health action process approach schema (adapted from Parschau, 2014).
Finally, several studies have sought to improve our understanding of the translation of intention into PA, particularly its maintenance. Recent studies showed that identity, as an underlying factor of automatic processes, is a moderator of the intention–PA relationship, 122 and this finding reinforces the need for integrative models that include habit formation and the development of an active identity. 123 These factors are part of the multiprocess action control (M-PAC) model. 97
M-PAC, 97 which is a recent integrative model used to understand PA, includes findings from several streams of contemporary research in PA, thus bringing together the relevant operational constructs (Figure 2). Schematically, the M-PAC framework is composed of three articulated and interlinked levels. The first level concerns the different phases of behavior and includes intention formation, adoption of action control, and maintenance of action control. The second relates to initiating reflective processes, ongoing reflective processes, regulation processes, and reflexive processes. Lastly, the third level concerns operational constructs that include, for instance, perceived capacity, behavioral regulation, and habit. Thus, at the top of the M-PAC model, the antecedents of the formation of an intention constitute the initiating reflective processes and correspond to instrumental attitude and perceived capability. M-PAC may serve as an appropriate behavior change theory for the development of interventions aimed at the adoption and maintenance of regular PA in patients with OSA. Indeed, this represents an attempt to integrate research advances regarding PA behavior within a cohesive framework in order to provide a pragmatic structure for practitioners. The M-PAC approach identifies links between BCTs, operational constructs, and phases of behavior change, from the initiation to continuation stages. This model is thus in line with the IM approach: the theory explains how the mechanism of action works, thereby providing insights into why a causal link between the method and behavior change can thus be expected. 62 Thus, in addition to IM, we used HAPA and M-PAC as theoretical bases to design the intervention.

Multiprocess action control schema (adapted from Rhodes, 2017).
Step 2: Identification of program outcomes and objectives
The results of the problem analysis were used to specify the program outcomes, POs, and change objectives, which are described below. First, the program outcomes were specified as follows: (1) patients increase their PA level by incorporating aerobic and/or strength-building exercises, 3 to 5 times per week, for a total of at least 150 min, and maintain this practice while performing other daily activities and (2) patients engage in PA in a way that is adapted to their capacities by considering the intensity of the effort with regard to shortness of breath, muscular sensations, and exhaustion.
Second, the performance and change objectives for each of the specific program outcomes were defined. In combination with the HAPA 73 and M-PAC 97 frameworks, the results of the semistructured individual interviews 120 were used to define the POs. After specifying these POs, we created a matrix of change objectives by linking the POs to the constructs. To design the program, 11 POs and 30 change objectives were defined (Table 1).
Performance objectives, change objectives, and determinants.

CO: change objectives; PO: performance objectives.
Step 3: Selecting theoretical methods and practical strategies for program design
After identifying the program outcomes, POs, change objectives, and constructs, the theoretical methods and practical strategies were selected. Indeed, the theoretical methods and their translation into practical strategies are the constructs needed to achieve the change objectives. The following paragraphs present this structuration for the 11 POs.
Performance objective 1: Providing health risk and benefit information and recognizing pros and cons
A recent meta-analysis has highlighted the positive effect of patient education on knowledge, skills, and health behavior. 100 Education interventions usually consist of providing health information about risks/benefits and comparing the advantages and disadvantages of behavior change. The targeted constructs are “risk perception,” “knowledge,” “outcome expectancies,” and “attitude.” Brief messages delivered via mobile device technologies such as short message services have been shown to contribute to behavior change.99,101 Furthermore, interventions based on unidirectional messages produce positive effects on behavior change. 102 As research on message frequency and quantity has not yet identified an optimal level, 103 we chose to send one daily unidirectional message at a time when the user would be available to read the text message (i.e. at 8 am in the morning). The content of the message concerned the health risks of not performing the PA, the health (bio-psycho-social) benefits of PA behavior, and the links between health and PA. In addition, one 60-min group session (session 1) provided users with the opportunity to learn the “pros and cons” technique to identify the advantages and disadvantages of PA behavior change, hear other points of view, and develop their own representations.
Performance objective 2: Providing personal advice and instructions on how to perform the physical activity
The BCTs related to exercise class attendance and hands-on experiences (i.e. instructions on how to perform the PA, demonstration of the PA, and behavioral practice) to make the new PA behavior achievable. Moreover, prompting preparation for behavior during the intervention may be a good means to positively impact the behavioral determinants. 52 The targeted constructs are “self-efficacy,” “knowledge,” and “skills.” For this purpose, patients have access to adapted exercise videos on the app. These videos are sorted according to the different parts of the body, the type of exercise (strengthening, aerobic, and/or stretching), and the task difficulty. Thus, depending on their choices and goals (associated with a type of exercise), patients can benefit from specific exercises. A group session (session 2) is carried out with a health professional to suggest personalized adaptations of the exercises not anticipated by the app in terms of users’ desires and resources (environmental). At the same time, when patients indicate that they are on a treatment that should be adapted to PA, they are regularly reminded about the instructions for this treatment (e.g. pharmacological support).
Performance objective 3: Providing instructions on how to adapt effort and monitor sensations
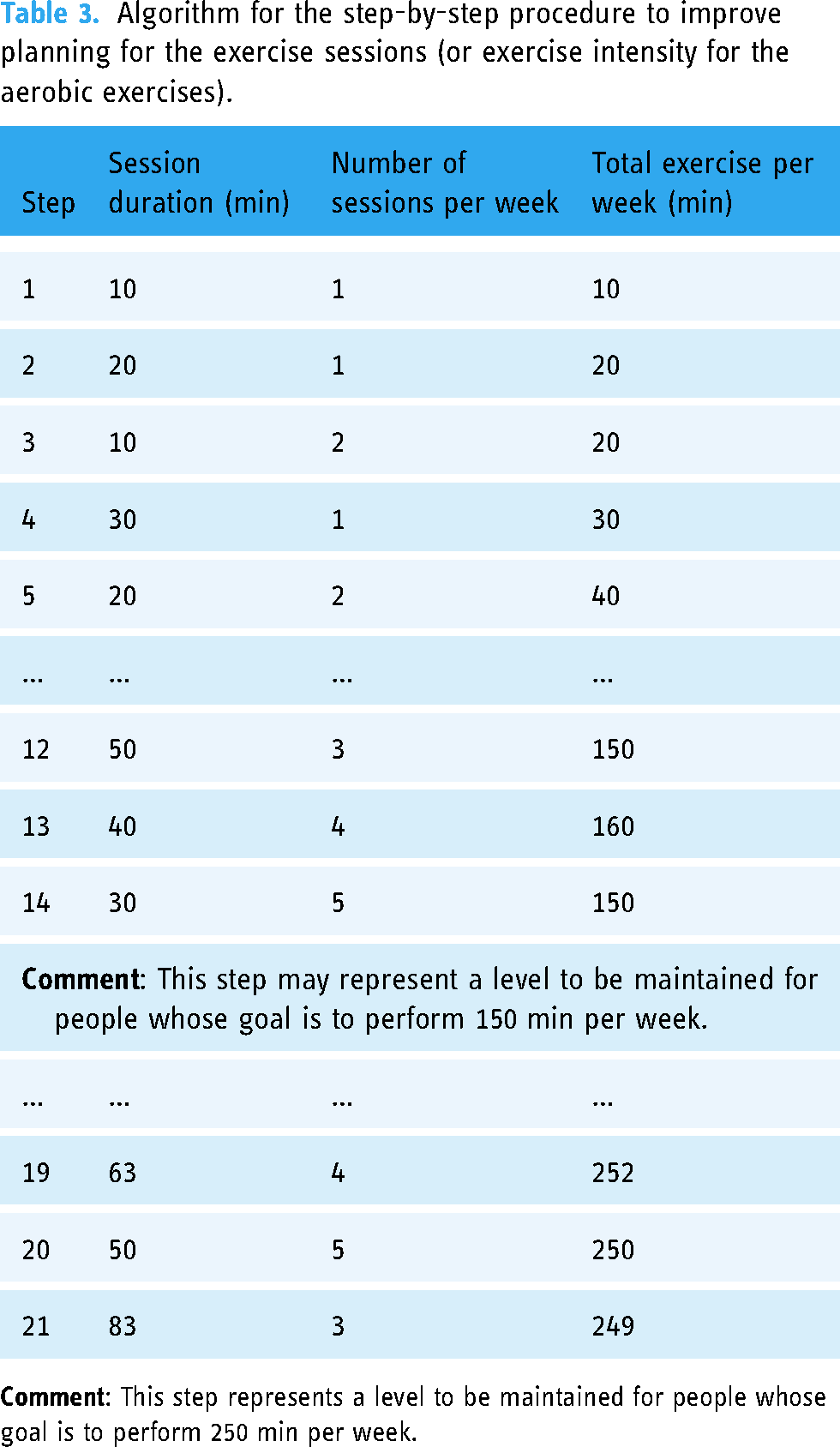
There is evidence that providing graded tasks leads to significant improvements in PA behavior change.52,68,83,104 In practice, this technique, alongside the use of sensation rating scales, is linked to more positive affective states during the performance of PA. 105 These can also predict future PA. 124 The targeted constructs are “self-efficacy” and “skills.” To help patients adapt their efforts in a nonpainful way, the app offers two accompaniments. The first is a step-by-step organized procedure to improve exercise intensity (Table 2) for strengthening exercises, with graded steps defined by the number of exercises, repetitions, and sets. The objective of this support is for patients to perform the recommended 10 exercises with 20 repetitions and 3 sets per exercise. The second accompaniment is a step-by-step organized procedure to improve planning for the aerobic exercise sessions (Table 3), with stages defined by the number of weekly sessions and the duration of the session. The objective of this support is to help patients achieve the recommended 150 min—up to 250 min—of PA per week with at least three sessions. The progression within the procedures depends on the level of sensations (shortness of breath, pain, muscle difficulty, and/or tiredness) declared (10-point scale) throughout the effort (during and/or at the end). Thus, based on their declarations, patients receive feedback that invites them to progress to the next step, return to the previous step, or stay at the current step. The video exercises offered by the app also depend on the users’ perceived sensations. Following their declarations, the patients receive feedback that may suggest more suitable exercises. In session 2, the goal is complementary to that of PO2: to check that patients are performing exercises adapted to their physical capacities and to confirm that they know how to monitor and evaluate their sensations.
Algorithm for the step-by-step procedure to improve exercise intensity for strengthening exercises.

Algorithm for the step-by-step procedure to improve planning for the exercise sessions (or exercise intensity for the aerobic exercises).
Performance objective 4: Providing positive reinforcement
Positive reinforcement (i.e. nonspecific reward, social reward, and nonspecific incentive 65 ) has been identified as a suitable method to change PA.66,68,70 Moreover, in combination with mastery experiences and persuasion techniques, this strengthens patients’ beliefs in their ability to change.62,97 The targeted constructs are “outcome expectancies,” “self-efficacy,” and “social support.” The app provides incentives and rewards patients’ effort and progress through a digital badge system. Once every 2 weeks, feedback reminding users about their last badges prompts them to acknowledge their past success. Mastery experiences (challenging tasks with feedback to indicate capability) are stimulated with “challenges.” This enables them to experiment with PA and encourages the practice or rehearsal of the behavior performance. Finally, an individual session (session 3) is carried out with a health professional to commend their progress and persuade them that they can successfully perform the desired PA.
Performance objective 5: Providing opportunities and environmental facilities
Restructuring the physical environment is one of the promising BCTs. 106 Adding objects to one's environment has been identified as an effective method to change PA behavior.52,83 These techniques are integrated into the opportunity determinant.90,97 This construct has been shown to contribute to PA behavior change.107,108 Thus, the construct targeted in this PO is “opportunity.” In the intervention, physical opportunity is implemented in relation to the home environment and material resources by providing tips (short digital messages) to help patients restructure their physical environment and by giving them free PA materials.
Performance objective 6: Prompting goal setting
Health coaching by healthcare professionals along with goal setting brings about positive changes in self-efficacy62,109 and PA.109–111 The targeted construct is “skills.” To ensure their commitment, patients are asked to choose a PA goal in line with their preferences and capacities. The app asks questions to guide them in identifying what motivates them to increase their PA level. For each motive, proximal (i.e. over 7 consecutive days) and distal (i.e. in 6 months) goals are defined as incentives for immediate action that evolves over time. The goals are defined in terms of PA frequency and duration per week. An individual session (session 4) is carried out with a healthcare professional to improve the patients’ ability to define relevant goals.
Performance objective 7: Prompting behavior planning
The BCT known as action planning (as well as implementation intention) has been shown to contribute to significant PA behavior change.56,69,112 The constructs targeted in this PO are “self-efficacy” and “action planning.” In the app, patients answer questions to guide them in the development of their action plans. One action plan is created per goal. The action planning process consists of specifying a goal in terms of context (i.e. when, where, and with whom), frequency, duration, and intensity. In individual session 4, the goal is also complementary to that of PO6: helping patients improve their ability to create action plans.
Performance objective 8: Prompting self-monitoring
Self-monitoring has been identified as a suitable method to change PA behavior.83,84,113–115 The targeted constructs are “skills (self-regulatory)” and “action planning.” At the beginning of the intervention, patients synchronize the app with a connected watch. They are asked to wear it throughout the intervention period in their everyday life. Graphs built into the app let them track their daily, weekly, and monthly step counts. In addition, they are also invited to plan the sessions for the coming week (agenda) and then validate what was done in reality (training log). This information is then used to provide automatic feedback on the gap between their goals and actions. In addition to this self-monitoring, patients are invited to monitor their outcomes. To do this, one message is sent to each patient on a monthly basis. A healthcare professional discusses the self-monitoring results with patients and provides feedback. Group session 5 is carried out with a professional to look at any discrepancies between patients’ current behavior and goals. Moreover, during an individual session (session 6), a review of the behavioral goals and action plans is proposed. These sessions aim to teach patients how to use self-monitoring to enrich their reflections and strengthen their decision making.
Performance objective 9: Prompting coping planning
Coping planning contributes to PA behavior change.56,62,68,97,116,117 The targeted constructs are “self-efficacy,” “social support,” and “action coping.” Using the app, patients are asked to respond to questions once a month about the barriers that they encountered and then to develop a coping plan (i.e. if/then plan). To help them identify solutions, information about antecedents is provided by text messages. In group session 5, the goal is to help them consider solutions through discussions with other patients and feel able to deal with barriers.
Performance objective 10: Developing a physical self-identity
Self-identity may contribute to behavior change maintenance.58,97 The constructs targeted in this PO are “awareness” and “identity.” Therefore, the app provides text messages with content to inform patients about the qualities (values or personal strengths) that enable them to assert their identity as part of a behavior change strategy. An individual session (session 7) is carried out with a healthcare professional to draw the patients’ attention to discrepancies between their current behavior and self-image, to elicit the perceived causes of behavior and suggest alternative explanations, and to help them reinterpret any unhelpful or demoralizing thoughts, feelings, and opinions.
Performance objective 11: Developing a physical activity habit
Habit may also contribute to behavior change maintenance.58,97,118 The constructs targeted in this PO are “self-efficacy” and “habit.” Cues are provided by the app in the form of reminders about the PA sessions planned in the agenda. An individual session (session 8) is carried out with a professional to define more relevant stimuli (environmental or social) to prompt or cue the PA behavior at a specific time or place as well as to prompt the rehearsal and repetition of the PA behavior in the same context repeatedly so that the context elicits the behavior.
Discussion
Main findings
This article uses a detailed systematic process to develop a theory-based and evidence-based intervention targeting the adoption and maintenance of PA in patients with OSA. We used the IM framework, which made the process of intervention development and content transparent.
Despite the benefit of PA in the context of OSA,10–13,16–41,125 few studies have incorporated an outcome associated with PA level to measure the effect of interventions on the PA behavior itself.24–29,40,41 The results are nevertheless heterogeneous, and more RCTs that integrate behavioral outcomes are needed. 11 The analysis of PA interventions from 20 experimental studies targeting patients with OSA12,24–41,125 indicate that only 2 (10%) studies provided educational content12,32 and 3 (15%) included motivational content26,27,40 in addition to the PA practice. The only intervention26 to have precisely described its content based on BCTs formed the basis of the latter three studies. This was also the only intervention to have developed its content on the basis of behavior change theories (i.e. social cognitive theory, self-determination theory, and self-regulation constructs). Finally, only one study measuring the effect of a PA intervention also measured a variable associated with motivation prior to the intervention. 27 To date, no study has integrated PA-associated variables as an outcome both before and after the intervention.
Following our needs assessment, we identified only one qualitative study that explored the barriers and facilitators to engaging in PA. 120 However, engaging in PA is a complex and dynamic process involving behavior change. In the context of chronic disease, although PA interventions like practice and/or educational sessions are usually effective in terms of increasing the PA level, highly heterogeneous effects have been observed. 75 Interestingly, strategies based on cognitive-behavioral learning and social principles may facilitate engagement. 126 To understand why not all interventions lead to an increase in PA, it seems crucial to explore the role played by the determinants of behavior change and to ascertain which intervention characteristics are associated with more significant results. 63 Factors that vary among interventions include the presence and type of behavioral theories underpinning their content, 64 the BCTs implemented, 65 and their mode of delivery. 83 To better understand the effect of interventions on behavior change in patients with OSA, future RCTs should include interventions based on behavior change theories with their content tailored to the explicit objective of promoting behavior change. They should also evaluate the determinants of behavior before and after the intervention. In addition, more qualitative studies that explore the barriers and facilitators to PA engagement in patients with OSA are needed.
In the field of behavior change, the quality of reporting on intervention content should be improved. 127 Studies should describe the intervention content (e.g. BCTs) and app features with sufficient detail to enable other researchers to reproduce the study and thereby advance this field of research.62,85,86,89,90 Indeed, the results of previous meta-analyses examining the effects of various techniques on the determinants of behavior and/or health-related behavior are limited by the amount of information available regarding both the intervention (i.e. it is often difficult to identify all the techniques implemented) and its level of application. 62 Thus, the IM protocol, which ensures that all important program objectives are addressed in the intervention and are based on theoretical insights and taxonomies of techniques, offers a relevant method to address this issue.
The type of PA behavior that is beneficial for patients with OSA was shown to be regular PA that is maintained over time. 128 However, the only study that measured the effect of an intervention on the PA level over the long term (i.e. 12 months) showed that the increase obtained following a 9-month intervention was not maintained in the following months. 29 This result was also found in contexts other than OSA.129,130 It is therefore important to focus on the processes associated with the maintenance of PA behavior. The M-PAC framework indicates that habit and identity are key factors influencing the long-term uptake of PA. Despite their usefulness for maintaining behavior,97,118,131 these two factors have received little attention to date in the context of PA. 97 Techniques associated with identity and habit formation, framing,132,133 and prompts/cues have been seldom used in the context of PA,52,134 although they were implemented in our intervention.
To our knowledge, this is the first study to have developed an mHealth PA intervention for patients with OSA. This intervention uses mHealth technology to support the translation of evidence-based methods into practical applications. Indeed, most techniques seem to be supported by these interventions, which enable, for instance, the automatic and continuous monitoring of real-life outcomes. 88 This offers the possibility of creating individualized and interactive feedback, thus ensuring that PA interventions are better adjusted to the context of everyday life. For example, mHealth could provide good support for habit formation. Indeed, to help people develop exercise habits, intervention efforts should focus on encouraging them to frequently and reliably prepare for and initiate exercise in the same context. 118 Furthermore, mHealth interventions 96 like video counseling 135 and personalized feedback136,137 seem to offer promising perspectives for improving the effect of the interventions.
The app that we created here includes multiple proven techniques that focus on the initiation and maintenance of PA behavior change. We believe that this makes it a unique and promising mHealth intervention to promote PA.
Limitations
The study has several limitations. First, the effectiveness of the intervention has not yet been evaluated by an RCT. Second, PubMed was the only database used in the systematic literature review. Although it is one of the largest available databases, we acknowledge that some useful interventions may have been overlooked. Third, due to time constraints, no focus group was organized during the problem analysis step. Indeed, other researchers who have used the IM protocol have described this as very time-consuming,138–140 and the time schedule of the project prevented us from carrying out a focus group. However, the development of this mHealth intervention was based on previous research carried out by our team in a population of obese patients, many of whom had OSA. 98 This first experience allowed us to identify levers and understand the needs of these patients regarding the different aspects of a telerehabilitation program. Lastly, we only focused on PA as opposed to including other factors like diet. Further studies are needed to explore more comprehensive interventions for multiple lifestyle changes such as sedentary and diet behaviors.
Conclusions
This article describes the development of an intervention to promote the adoption and maintenance of PA in patients with OSA. The results of the study provide a theoretical and methodological basis for researchers and practitioners. This is especially important given the current paucity of evidence-based PA interventions and their limited content regarding important BCTs (framing and prompts/cues techniques) that address meaningful behavioral determinants (identity and habit). A future paper will report on steps 4, 5, and 6 of the IM framework along with an RCT to indicate whether the intervention is acceptable, usable, well-implemented, and effective in improving PA in this population.
Footnotes
Acknowledgments
We thank the members of the scientific committee of the m-Rehab consortium for their feedback during the follow-up presentations of this project.
Contributorship
CL, BC, and JB participated in the intervention development group discussions, created the program functionalities, and developed the intervention map. CL collected the needs assessment data from all described sources and wrote the manuscript. All authors read and critically reviewed the manuscript and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was funded by the European Regional Development Fund and the Occitanie Region, France.
Guarantor
JB.