
Abstract
Objective
Older adults are at high risk of falls and this problem calls for efficient and scalable interventions. This study investigated whether a motion capture system paired with balance training exergaming software is a feasible strategy to deliver therapeutic exercise to older adults in an aged care facility.
Methods
This study analyzed data from a quality improvement rehabilitation initiative. Two convenience samples of older adults were included: a usual care group (n = 12), admitted to a rehabilitation hospital and receiving standard in-patient therapy 5×/week and the Evolv group (n = 12), admitted to an aged care facility, prescribed exergaming 3×/week. All participants performed 30-minute exercise sessions based on a fall prevention program over 3 months. The Short Physical Performance Battery (SPPB) and Tinetti Performance Oriented Mobility Assessment test were administered pre- and post-treatment.
Results
No adverse events were recorded during the interventions. Mean SPPB increase for Evolv participants was 2.25 ± 1.35 (p < .001, CI for mean = 1.39 to 3.11, d = 1.66), compared with a non-significant change in the usual care group (mean increase = 2.25 ± 3.82, p = .066, CI for mean = −0.18 to 4.68, d = 0.59). Tinetti improvement was significant for the individuals receiving usual care (3.83 ± 2.82, p = .012, CI for mean = 1.01 to 6.66, d = 0.86) but there were no significant between-group differences in outcomes.
Conclusions
Exergaming with the Evolv system for balance and strength training may be a feasible strategy to improve physical function for older adults recovering in an aged care facility.
Introduction
The number of adults 65 or older in the United States is predicted to increase from 49 million in 2016 (15% of the population) to 71 million by 2030 and 98 million by 2060 (25% of the population). 1 Due to declining physical capacity along with reduced functional status, aging is associated with frailty and greater susceptibility to adverse health outcomes. 2 A quarter of all adults in America over age 65 fall every year, 3 with one out of five incidents causing serious injury. For older adults, falls are the leading cause of injury-related fatalities and nonfatal traumatic hospital admissions,4,5 which, in 2015, resulted in medical costs of $754 million and $50 billion, respectively. 6 With the rapidly aging population and ever-growing health care expenses, it is critical to develop efficient methods to maintain health and prevent falls.
In vulnerable individuals, safe mobility is a necessary component of fall prevention, with home or group-based exercise consistently emerging as an effective intervention that also has the potential for significant cost-savings.7–9 Guidelines recommend screening for performance deficits followed by a multifactorial assessment to determine the appropriate mitigation strategy; however, implementation of this approach remains a challenge for policy makers and health professionals. 10 For example, the Vivifrail project aims to promote physical activity in various settings for the prevention of frailty and falls among older adults through a multicomponent protocol.11,12 Following a battery of tests, appropriate exercises are prescribed for balance, endurance, resistance, and coordination training. Recently, this intervention was found to significantly improve gait and strength while decreasing fall risk after 3 months. 13 Unfortunately, comprehensive programs such as Vivifrail are resource-intensive and adherence may be challenging due to fatigue or lack of motivation. 14 Fall prevention interventions often have low long-term adherence rates. 15 Potential barriers are insufficient encouragement, low social support, complexity of instructions, and poor availability of transportation. 16 Another major obstacle is the shortage of funding for staff, facilities, and equipment.
Exergaming is a technology-based exercise intervention, where the user's physical movements interact with motion capture software. Exergaming delivers high-intensity, goal-oriented movement repetitions in an engaging and motivational format. Compared to standard care, exergaming has been found to have greater adherence rates and enjoyment. 17 Notably, exergaming has been suggested as a sustainable fall prevention strategy18,19 with efficacy for improving both balance 20 and postural control. 21 These interventions have been found to be safe across a wide variety of health applications and gaming systems in a recent review. 22 However, most of the consoles covered by this review have been discontinued from commercial sale, creating a need for additional consumer products to be explored in order to expand this promising area of health technology.
Other low-cost, commercially available optical motion capture cameras could feasibly substitute for the more popular Microsoft Kinect but have not been studied in the context of fall prevention and exergaming. The goal of this retrospective study was to investigate (a) the feasibility of using a novel exergaming system that utilizes the Orbbec Astra sensor to deliver a balance and fall prevention program to older adults in an aged care facility; and (b) short-term outcome differences compared with a similar population receiving conventional physical therapy.
Materials and methods
Study design
The present study is a retrospective review of a convenience sample of data collected as part of a quality improvement initiative at IMQ Igurco in Bilbao, Spain. De-identified data analysis activities were deemed exempt by The Mount Sinai Program for Protection of Human Subjects (STUDY-21-01425).
Participants and interventions
Older adults (≥60 years old, Mini-Mental State Examination (MMSE) score ≥20 points) were engaged in balance and strength training exercises. Subjects were convenience-sampled from two different sites, with separate modes of intervention delivery. De-identified data from participants who completed at least 3 months of therapy were independently analyzed. Baseline characteristics included age, gender, illness severity, comorbidity burden, and activities of daily living (ADL)/functional independence.
Usual care group
The usual care group was composed of individuals admitted to a rehabilitation hospital where supervised sessions of standard in-patient therapy consistent with the Vivifrail program were provided by a physical therapist 5 days per week for 30 minutes.
Evolv group
The exergaming (Evolv) group consisted of individuals living in a nursing home who were engaged in gamified rehabilitation based on the Vivifrail program, which consisted of exercises, such as squats, single leg balance, arm raises, leg raises, vertical arm stretches, heel lifting exercises, and other exercises of this nature that are designed to improve balance while remaining true to the parameters of the Vivifrail program. Each patient was prescribed their own set of exercises in the Evolv system by their treating therapist depending on clinical assessment and judgment, and they were encouraged to participate at least three times per week for 30 minutes each session. The exercises were customizable by an on-site physiotherapist involved with the study who administered the first session. Subsequent sessions were supervised by staff members of the nursing home. Good clinical practice stipulated that all of these residents had Functional Ambulation Category (FAC) score ≥3 for safety to engage in lightly supervised physical activity. 23 A score of 3 is defined as the participant being able to ambulate on level surfaces without manual contact of another person, but for safety, still requiring standby guarding of one person. As shown in Figure 1, the exercises were delivered via the EvolvRehab® (Evolv Rehabilitation Technologies; Bilbao, Spain) virtual therapy platform, which ran on an Intel NUC Mini PC connected to an Orbbec Astra camera sensor, and a widescreen television to instruct and monitor users. On-screen visual instructions were provided to direct subjects' movements. These movements were captured and analyzed to generate feedback, including positive motivational messages, on the subject's performance.

Nursing home residents performing exercises guided by the EvolvRehab system.
Outcome measures
The primary outcome of this retrospective study was feasibility, defined by levels of adherence, compliance, and adverse events including falls during the intervention. Falls were defined as unexpected events which result in a person coming to rest inadvertently on the ground or at other lower level. 24 Any fall experienced by a participant was recorded during the study period to determine the safety and ability to avoid loss of balance.
The secondary outcomes were physical function and balance ability, evaluated by the Short Physical Performance Battery (SPPB) Protocol and Tinetti Performance Oriented Mobility Assessment (Tinetti), respectively, at baseline and after 3 months for all subjects.
SPPB assesses lower extremity function and is based on three timed tasks: standing in three different positions (feet together, semi-tandem, and heel–toe), gait speed (3- or 4-m walk), and chair rise test. 25 Each of the components is scored from 0 to 4 to obtain a total ranging from 0 to 12, with higher scores indicating better performance. 26 Research has shown the SPPB to be valid, 27 reliable, 28 and responsive 29 in older adults.
Tinetti measures balance through nine tasks, such as sit-to-stand and turning as well as gait ability by assessment of seven specific variables, including step length, height, symmetry, and continuity. Each item is scored on a 2- or 3-point scale for a maximum total of 28 at the highest level of performance. 30 The test has excellent reliability and is used to predict fall risk in older adults. 31
Data analysis
The Shapiro–Wilk test was performed to determine the normality of data. Within-group comparisons of baseline and endpoint SPPB and Tinetti were analyzed using paired t-tests. For the nonparametric data, within-group comparisons were analyzed with the Wilcoxon signed rank test. The 3-month change in outcome measures was compared between Evolv and usual care groups with independent t-tests. All testing was two-tailed, with a significance level of .05. Statistical analyses were performed using SPSS software, version 27 (IBM Corp.).
Results
Of the 24 participants (12 in each of the Evolv and usual care groups) included in this study, 13 were women (54.2%) and the mean age was 81.2 (Table 1). The usual care group had higher comorbidity (p = .033) as assessed using the Cumulative Illness Rating Scale-Geriatric (CIRS-G) and lower functional independence (p = .004) as assessed using the Barthel Index, and worse walking ability (p = .001) as assessed using the FAC test. The FAC is a clinician-completed walking evaluation with participants scored on level of assistance, from least to most independent. 32 Baseline scores were not significantly different for SPPB (p = .14) or Tinetti (p = .07).
Demographic, clinical, and functional data at baseline by group.
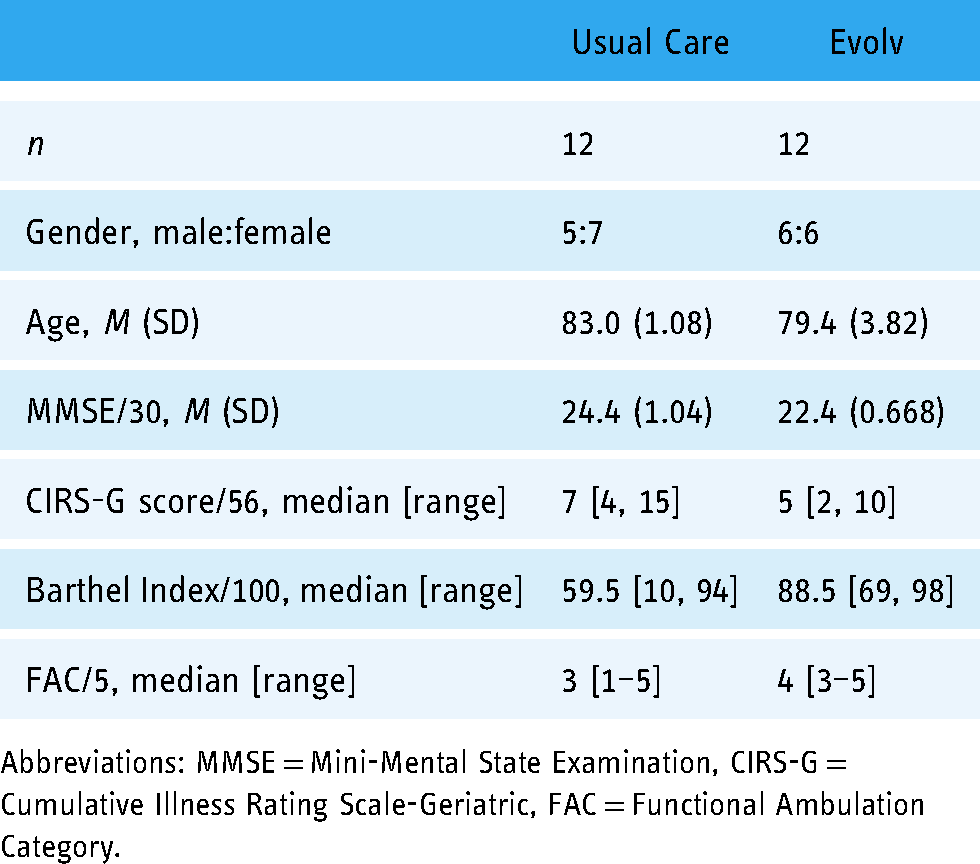
Abbreviations: MMSE = Mini-Mental State Examination, CIRS-G = Cumulative Illness Rating Scale-Geriatric, FAC = Functional Ambulation Category.
Primary outcomes
In the Evolv group, there were originally 17 participants with 12 completing a total of 3 months of therapy. Two participants dropped out during the first month, one dropped out during the second month, and two dropped out during the third month (dropout reasons include: early discharge from the facility, or simply stopping the sessions). Of the 12 Evolv participants who completed therapy, the number of sessions completed ranged from 31 to 44 with a mean and SD of 38.9 ± 3.94.
In both groups, there were four participants who fell for a total of five falls in the usual care group and 14 falls in the Evolv group during the treatment period. No falls occurred during Evolv therapy and all recorded falls occurred outside of therapy.
Secondary outcomes
The baseline and study endpoint results for secondary outcomes are shown in Table 2 and Figure 2. Effect sizes are listed for parametric data. Over 3 months, there was a significant improvement in SPPB scores for the Evolv group (p < .001, 95% CI [1.39 to 3.11], effect size 1.66). The usual care group significantly improved on the Tinetti (p = .012, 95% CI [1.01 to 6.66], effect size 0.50). When analyzing the individual SPPB components, Evolv participants overall experienced significant improvement in each, while the usual care group only significantly improved for gait (Table 2). Figure 3 shows each individual data point before therapy and after 3 months of therapy.

Change in primary outcomes from baseline to endpoint. The top whisker indicates the maximum value; the bottom whisker, the minimum value; the top of the box, 75th percentile; the bottom of the box, 25th percentile; horizontal line inside the box, median.

Participant scores at baseline before intervention and after 3 months of intervention. The maximum possible SPPB score is 12 and the Tinetti score is 28.
Baseline and endpoint results for primary outcomes by group.

Abbreviations: SPPB = Short Physical Performance Battery Protocol, Tinetti = Tinetti Performance Oriented Mobility Assessment.
Bold indicates significance at p<.05.
There was no significant between-group difference in SPPB nor Tinetti change from baseline to endpoint (p = 1.00 [−2.51 to 2.51] and .093 [−0.47, 5.64], respectively).
Discussion
This work found that a multicomponent strength and balance program resulted in physical function improvements for older adults whether delivered via exergaming technology (three times weekly) or standard supervised therapy (five sessions per week). The absence of falls across a few hundred successfully completed Evolv therapy sessions indicates that it can be safely administered in a community care setting, which is an important consideration for a population at high risk of falling. Additionally, the high number of sessions completed by the participants who adhered to treatment is promising. While the Vivifrail protocol is currently being studied in the outpatient setting, this is the first investigation of its implementation as gamified rehabilitation using the Orbbec Astra motion capture system.33,34 Exergaming-based balance training has previously been shown to provide positive benefits as a potential alternative or complementary therapeutic approach.35–38
The mean change in total SPPB score was 2.25 for both groups, but only significant in the Evolv participants due to a tighter spread of the data (1.35 vs. 3.82 SDs). Based on prior effect size and standard error of measurement determinations for the SPPB, the observed improvement corresponds to a clinically important difference. 28 Notably, a potential ceiling effect did not obscure the Evolv group's gains despite a relatively high baseline score, which was likely due to the requirement of FAC ≥3. 39 A quarter of the usual care subjects (3/12) worsened on the SPPB while all from the Evolv group had greater endpoint totals. Across subscales, the highest overall change was in gait and chair stand for the usual care and Evolv groups, respectively, suggesting different functional implications of each intervention.
Improvement on the Tinetti POMA was only significant in the usual care group, with five of these participants exceeding the minimal detectable change compared to two who received therapy via Evolv. 30 Since this assessment tool emphasizes dynamic as opposed to static balance (as in SPPB), the results seen may reflect a specificity of outcomes depending on how treatment is delivered. Due to the nature of the Evolv system and necessary safety precautions, only a certain amount of exercises that target dynamic balance are feasible in an unsupervised or lightly supervised paradigm. However, in the future, it is possible that therapists (such as those working with the usual care group) can spontaneously facilitate the flexible practice of mobility tasks with hands-on assistance, while utilizing the Evolv system for unsupervised practice of static balance tasks. In addition, there is a possibility that the ambulatory activities were more emphasized in the usual care group, which could justify why these participants showed greater improvements in the higher-level balance items on the Tinetti.
Given these considerations, clinical decision making is important when appropriately providing individualized care to a diverse population with various degrees of physical impairment such as older adults. Perhaps individuals who have already achieved a minimum level of functioning may further improve through exergaming such that professional expertise can be directed toward specialized training for optimal patient benefits. In the context of limited resources, leveraging technology to reduce staff burden may allow rehabilitation to be performed more efficiently as quality standards are maintained. In fact, the outcomes of each group were comparable even though Evolv participants received 40% less therapy supervised by nursing home staff without a greater risk of falls. The results are particularly promising when taking into consideration that the average age of subjects was very high (80+), comprising a cohort that is often underrepresented in studies on exergaming.40,41 In addition, these patients were of high complexity, reflected by overall CIRS-G.
Although these results are encouraging for the implementation of similar programs in a community setting, this study had a number of limitations that limit further conclusions. Mainly, the groups were small and unmatched, which precludes direct comparison of effectiveness. The short length of study, lack of follow-up, and no access to data collected on falling or functional status prior to the intervention period limit any interpretation of fall prevention that Vivifrail aims to address. Additionally, despite knowledge of the standard hospital protocol, a lack of specific adherence data for the “usual care” cohort limits comparisons between the two groups. Cost efficacy was not assessed, but is a promising area for future research. As a retrospective analysis, we could not control for differences in how the separate locations implemented the treatment program. Although the outcome measures chosen are well-validated and not overly time-consuming for good clinical utility, there were no self-reported or comprehensive physiological assessments, which may have provided additional valuable information. Evolv participants were not asked about their experience so no conclusions about usability or satisfaction can be drawn; however, the supervision provided likely contributed to good adherence.
Conclusion
Our study indicates that physical function improvements can be feasibly obtained through exergaming. This type of intervention may benefit older adults in rehabilitation settings, where human resources are limited, to receive effective balance and strength training. Future research should include randomized clinical trials designed to confirm these findings and investigate the effects of combined treatment approaches as well as individual characteristics that determine optimal response to therapy.
Footnotes
Acknowledgements
The authors would like to thank the staff and patients at IMQ Igurco who enabled this work.
Contributorship
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Mount Sinai Program for Protection of Human Subjects deemed the de-identified data analysis activities exempt (STUDY-21-01425).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
DP.