
Abstract
Background
The digital transformation of healthcare enables new ways of working in cancer care directing attention on the digital skills of healthcare professionals. This systematic review aims to identify existing evidence about digital skills among health care professionals in cancer care to identify the needs for future education and research.
Methods
Database searches were conducted in PubMed, CINAHL, Web of Science, Scopus, Cochrane and ERIC to identify studies until March 2023. The inclusion criteria were digital skills of health care professionals in cancer care as described by themselves, other health care professionals, patients or significant others. The CASP tool was used for quality assessment of the studies. Data was analysed following inductive content analysis.
Results
The search produced 4563 records, of which 24 studies were included (12 qualitative, 10 quantitative, 1 mixed methods design and 1 strategy paper). Four main categories were identified describing HCPs’ required skills, existing skills and development areas of digital skills in cancer care: Skills for information technology, Skills for ethical practice, Skills for creating a human-oriented relationship and Skills for digital education and support. In development areas, one more main category, Skills for implementing digital health, was identified.
Conclusion
The digital skills of health care professionals in cancer care are multifaceted and fundamental for quality cancer care. The skills need to be assessed to provide education based on actual learning needs. The review findings can be used for education and research in this field.
Introduction
In recent years, cancer care has been increasingly complemented by digital technology,1,2 including monitoring symptoms and facilitating adherence to treatment and care, promoting healthy lifestyles and user engagement with digital cancer services. 3 The evidence supports the comparability of cancer care services produced digitally and in person in terms of patient satisfaction and effectiveness. 1 Although the research evidence on digitally produced supportive cancer care is limited, improvements have been achieved in health-related outcomes. 2 Successful implementation of digital technologies can significantly improve healthcare delivery in the European Region, 4 but full exploitation of the potential of digital cancer care services requires advanced digital skills.5–7
There are few definitions of digital skills, and skills can be seen as an attribute to digital competence.8,9 The overlap of the two concept definitions makes it challenging to describe digital skills. Skills in general means the ability to apply and use knowledge to complete tasks and solve problems. 10 Digital skills refer to the ability to access, manage, understand, integrate, communicate, evaluate and create information safely and appropriately. Furthermore, domains such as device and software operation, problem-solving and career-related competencies have been recognised in digital skills framework. 11 This review focuses on digital skills defined as actions that HCPs take to support the health and resources of people with cancer to provide quality digital cancer care services. Competence is a broader concept encompassing skills and referring to the proven ability to use knowledge and skills as well as to personal, social and methodological abilities in professional development. 10 It comprises (a) information and data literacy, communication and collaboration, digital content creation, and safety and problem-solving, 9 (b) knowledge of digital technology, social and communication skills, and ethical considerations, 12 and (c) self-assessed competence, knowledge and attitudes towards the use of digital technologies. 13
Several recommendations related to digital skills have been reported. The emphasis has been on enhancing opportunities for digitalisation in cancer care 7 and providing education, information and support digitally for people with cancer while maintaining confidentiality. 14 Furthermore, HCPs need digital literacy, that is, abilities to use digital technologies to find, evaluate, create and communicate information, 12 as well as apply the knowledge gained from electronic sources to address health problems. 15 In their work, HCPs also collect, utilise and make decisions about digital health data. This requires skills for secure data handling and sharing whilst respecting the rights of individuals. 16 The Code of Conduct for mobile health apps focusing on privacy and consent aims to increase trust in mobile health apps. 17
The challenges in digital skills in cancer care have focused especially on developing a trusting relationship and providing person-centred care in a humane way. 18 Person-centred care requires identifying patients’ willingness to use digital technology, evaluating patients’ digital capabilities and incorporating patients’ needs into digital cancer care services. However, how to conduct patient education in digital environments needs clarification. 19 Challenges have also been related to physical examination and assessment of patients via digital tools 1 as well as ethical practice, such as respecting patients’ privacy and confidentiality during the digital appointment. 20 Recent studies assessing HCPs’ digital skills indicated that majority of participants (n = 803) demonstrated basic level of digital competence, 8 whereas in low-income countries (n = 167) the level was relatively low. 21 There is a research gap in assessing HCPs’ current digital skills in cancer care, and no previous literature review has been reported on the subject so far.
The purpose of this literature review is to identify existing evidence of digital skills among HCPs in cancer care to identify needs for future education and research. The review was guided by the following research questions:
What are the digital skills of HCPs in cancer care? How should the digital skills of HCPs be developed in cancer care?
Methods
This study adheres to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 22 and is registered with PROSPERO (CRD42023413979).
Eligibility criteria
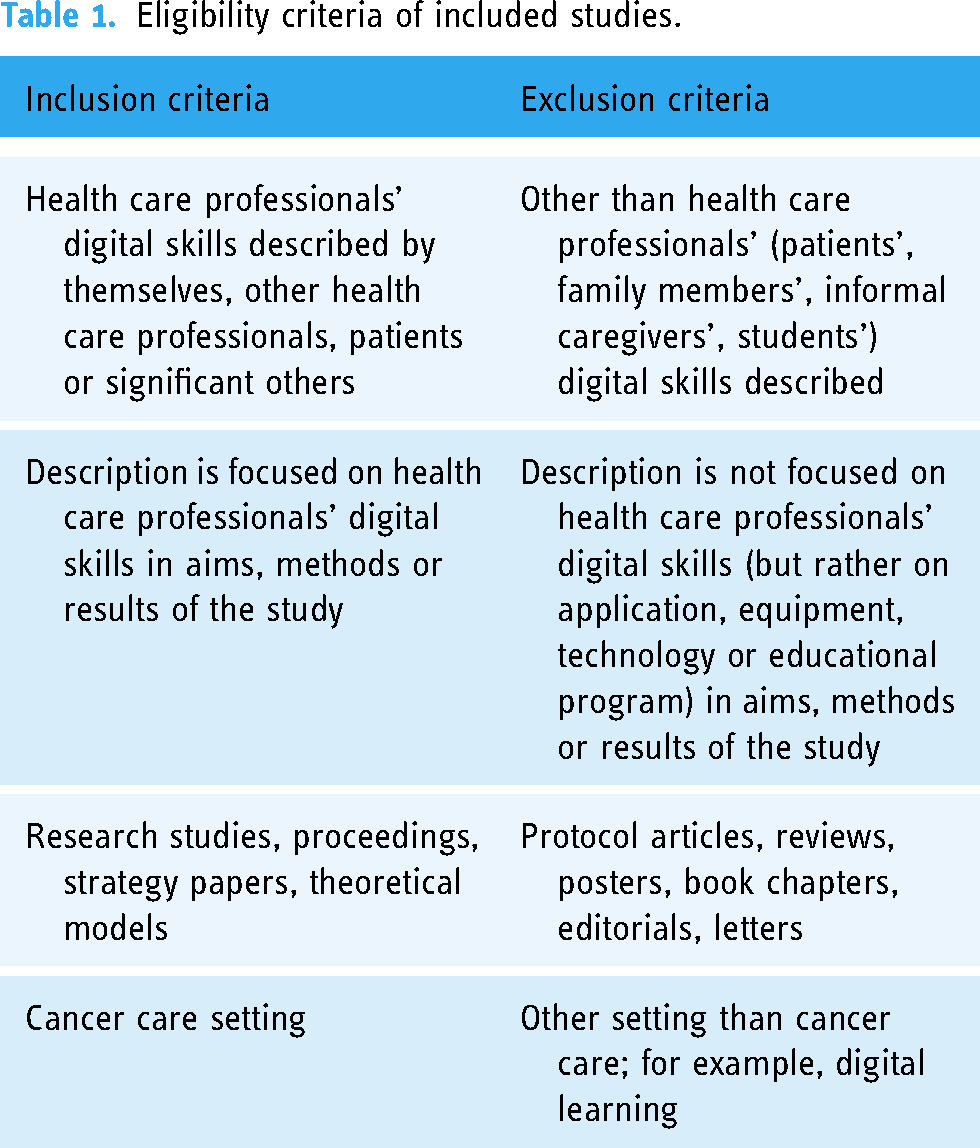
Inclusion and exclusion criteria for the review are described in Table 1. We accepted studies published from the establishment of the databases until March 2023.
Eligibility criteria of included studies.
Information sources
A systematic literature search was conducted in collaboration with the researchers and Information Specialist to six databases to identify eligible studies: PubMed, CINAHL, Web of Science, Scopus, Cochrane and ERIC. Additionally, references cited in the study reports included in the systematic review were screened to identify additional studies.
Search strategy
The literature search was conducted with three main concepts and their synonyms: digitalisation, skills and search were limited to peer reviewed journals and English language (Supplementary File 1). The search strategy was validated by test searches and discussion in the research group.
Selection process
Records were imported to Covidence software that assisted with the screening process and duplicates were removed. First, the records were screened independently by two researchers of the research team (CC, HLK, HV, JP, LT, TF or VS) based on title and abstract according to the eligibility criteria (Table 1) and conflicts were resolved by a third reviewer. Second, full texts were screened independently by two researchers according to the eligibility criteria and conflicts were resolved by a third reviewer of the research team (AB, CC, FSR, HLK, HV, JP, LT or SM).
Data collection process
Data was collected as follows: (a) reference, year, country, (b) purpose, (c) method, (d) theoretical approach, variables or focus of the research, (e) participants, (f) data collection, (g) analysis method, (h) findings related to digital skills and (j) conclusions related to digital skills. Data extraction was conducted independently by two researchers (LT and JP) and disagreements were resolved in consultation with a third person of the research team (HV or HLK). 23
Data analysis
Purpose of the analysis was to describe HCPs’ digital skills. Data comprised both qualitative and quantitative studies, and based on that, inductive content analysis was used.24,25 The coding of the content focused mainly on describing the manifest content of the literature. Since the studies did not actually assess HCP's digital skills, the analysis focused on the descriptions of digital skills in the results, discussion or conclusion sections of the studies. The analysis included five steps for each research question. 25 First, the researchers familiarised themselves with the data by reading the texts. Second, data was divided into meaning units and abstracted into codes related to digital skills. Third, the content and context of the codes were compared with each other, and corresponding codes were grouped into sub-categories. Fourth, the sub-categories were compared with each other, and based on similarities and differences, main categories were formed. Main categories were named according to their content.24,25 Finally, the main categories were compared with each other, and their names were refined. During the whole abstraction process, construction of sub- and main categories and decisions was made in consensus among the research team (LT, JP, HV and HLK). In reporting, study characteristics and findings were tabulated, and representative quotes were used for supporting the credibility of the findings. 24
Quality appraisal of the studies
Articles were assessed independently by two researchers (SM and CC). Disagreements were discussed until consensus was reached. For qualitative studies, a 10-item CASP scale (0–10) for qualitative studies was used 26 focusing on (a) validity of the study, (b) accuracy of the results and (c) transferability. For quantitative studies, a 12-item CASP scale (0–12) for cohort studies was used 27 focusing on (a) validity of the study, (b) internal validity of the results and (c) external validity. Items 6A, 6B, 7 and 8 were not applicable for included cross-sectional studies, they were thus omitted. When there was a ‘No’ for questions 1 and/or 2, the quality assessment was not completed with follow-up questions. 31 Quality appraisal was used to demonstrate the methodological quality of the studies as it affects the validity of the findings of the review. 27
Results
Of the 4563 records identified a total of 24 studies met the inclusion criteria (Figure 1).

PRISMA flow chart for the study search and selection process. 22
Study characteristics
The included studies were published during the last 18 years (2005–2023). Of those, 67% were published during the last five years. The studies were conducted in USA,28–36 Canada,37–40 Australia,41–44 England,45,46 Netherlands,47,48 Denmark, 49 Rwanda 50 and Turkey. 51 Designs of the studies were qualitative (n = 12, 50%),28,31,32,34,35,38,40,41,43,48–50 quantitative (n = 10, 42%),29,30,33,36,39,42,44,46,47,51 mixed method (n = 1, 4%) 41 and a strategy paper (n = 1, 4%). 45 Data was collected primarily by interviews (n = 10, 42%),31,32,34,35,37,38,41,43,49,50 or by surveys (n = 7, 30%).29,30,33,36,42,47,51 The participants were HCPs in different cancer care settings: nurses (n = 4, 8%),31,33,37,39 medical oncology providers (n = 1, 4%), 32 radiation oncology nurses (n = 1, 4%), 28 radiation oncologists (n = 2, 8%),30,51 surgical learners (n = 1, 4%), 29 psychosocial cancer care providers (n = 2, 8%)36,40 and trainees and fellows in radiology/radiation oncology (n = 1, 4%). 42 In six studies (25%), the participants represented several professions.32,46–48,50 In two studies, the participants were people with cancer (n = 2, 8%),38,49 and in two studies, both nurses and people with cancer (n = 2, 8%).35,44 In two studies, care givers were included with people with cancer and/or HCPs (n = 2, 8%).34,41 One study had a broad sample of consumers and other stakeholders (n = 1, 4%) 43 (Table 2). Skills were most often reported in connection with using digital technology or as HCPs’ concerns related to the skills. None of the studies assessed the level of these skills.
Study characteristics (n = 24).

Quality appraisal results
In the CASP checklist for 13 qualitative studies (Supplementary File 2), most of the studies showed a clear statement of the aims of the research, the qualitative study design was adequate, the findings were clearly defined, data collection and analysis were adequately rigorous in nine of the studies, and nine of them were designed in an appropriate way to achieve the aims of the research. However, recruitment strategy was considered appropriate in only three studies, and study results were likewise defined as being transferred to different settings in only three studies.
In the CASP checklist for 11 cohort studies (Supplementary File 3), most of the studies clearly stated their research objective, but only four of the 11 studies recruited the study population according to the aims of the research, and most of them used a convenience sampling strategy. Due to a cross-sectional study design, none of the studies measured exposure prior to the outcome, considered potential cofounding variables nor had a long enough follow-up. All studies have good internal validity but none of them has enough external validity to implement the results into different settings.
Digital skills of health care professionals in cancer care
The digital skills are analysed based on descriptions in the Results, Discussion and Conclusion sections of the studies. In the analysis, we identified three themes: required and existing skills and development areas in digital skills of HCPs. The required skills were those that were identified as skills that HCPs need to have to provide digital services. Existing skills were those that studies found HCPs to already have. Development areas were digital skills that, according to studies, still need improvement. In each of these themes, the following four main content categories were identified:
Skills for information technology Skills for ethical practice Skills for creating a human-oriented relationship Skills for digital education and support
In addition, one main category, ‘Skills for implementing digital health’, was identified as development area of HCPs’ digital skills. (Table 3). Of the main categories, ‘Skills for information technology’ consists of four sub-categories, ‘Skills for ethical practice’ of three sub-categories, ‘Skills for Creating a human oriented relationship’ of four sub-categories and ‘Skills for digital patient education and support’ of six sub-categories. However, not all the above sub-categories appear in every question considered. In addition, ‘Skills for implementing digital health’ comprises two sub-categories. Next, digital skills identified as required, existing and development areas are presented in more details.
Study findings related to digital skills.

Required digital skills of health care professionals in cancer care
The required skills are based on descriptions by HCPs themselves,28,29,31–33,41,50 patients, 49 or both HCPs and patients34,35 and as strategy outlines. 45 The digital skills required of HCPs formed four main categories: skills for (a) information technology,28,29,31,35,38,45,49 (b) ethical practice,32,41,45,50 (c) human-oriented relationship34,35,45 and (d) digital patient education and support45,49 (Table 3).
Required skills for information technology comprise two sub-categories: using digital technologies28,31 and technological preparing of digital appointments.29,35,38,45,49 Using digital technologies includes skills to find alternative ways to assess patients and operating various digital platforms.
28
It also includes skills to integrate digital technologies into clinical practice, access the Internet and search and filter online information. In addition, it includes developing the content, functionality and design of online sources.
31
The following quotation expresses the requirements for using digital technologies: The nurses need to know how to access the Web and how to search and separate good and bad sites.
31
For FTF encounters, seating arrangements, chair height, and eye level can impact the dynamics of the interaction, while on video the emphasis should be on camera position, appropriate front lighting, and minimizing technical issues with plans for trouble-shooting.
29
Required skills for ethical practice comprise two sub-categories: protecting patients’ privacy
45
and ensuring confidentiality
50
and patients’ consent.
41
Protecting patients’ privacy includes ensuring the setting is appropriate for health information discussion.
45
Confidentiality includes protecting patients’ passwords during digital appointment
50
: To maintain patient confidentiality, which may be compromised using personal mobile phones, most participants suggested that the mobile applications should be password protected.
50
Required skills for creating a human-oriented relationship comprise two sub-categories: adopting a person-centred approach32,35,41,43,45 and building rapport.34,35,45 Adopting a person-centred approach includes working with patients to create person-centred options and knowing patients as persons
35
: They (patients) appreciated being asked questions about their families, occupation, and things that brought them joy and appreciated the nurses remembering these.
35
Required skills for digital patient education and support comprise three sub-categories: providing information,31,45 ensuring understanding and providing support.
45
Providing information includes setting a common agenda for the appointment, delivering the key information and ending the appointment by summarising the main points and reviewing the next steps.
45
It also includes information consulting for patients.
31
Ensuring patients’ understanding includes providing information in a structured way
45
and encouraging patients to participate.45,49 Furthermore, it includes using silence to help patients process information and checking patients’ understanding
45
: Checking a patient's current understanding of the reason for the visit can help the clinician structure the conversation and fill in knowledge gaps when appropriate.
45
Pay attention to emotional cues from the patient during your visit, such as fidgeting, tuning out, crying, or looking very worried. Verbally acknowledge these cues during the visit.
45
Existing digital skills of health care professionals in cancer care
Existing digital skills of HCPs are based on descriptions by HCPs themselves,31,33 patients, 38 or both HCPs and patients.34,35 Existing digital skills of HCPs comprise three main categories: skills for (a) information technology,31,33 (b) creating a human-oriented relationship34,35,38 and (c) digital patient education and support29–31,34,38,40 (Table 3).
Existing skills for information technology comprise two sub-categories: using digital technologies31,33 and assessing digital health information. 31 Using digital technologies includes work-based computer skills, such as to access online clinical sources and patient outcomes. 33 It also includes actively searching information from databases for both HCPs and patients. 31 Assessing digital health information includes assessing information sources and website quality. In addition, it includes filtering relevant information from databases. 31
Existing skills for creating a human-oriented relationship comprise one sub-category, skills for building rapport,34,35,38 which includes skills to adapt a bedside manner during VC,
35
being patient
38
and using a caring tone of voice and guidance
34
: Most (patients) felt that providers were very patient during the call, never rushed through questions, and were respectful of scheduled appointment times.
38
From individual statements (n = 28), 19 learners (68%) felt comfortable communicating using telehealth, and 21 learners (75%) indicated that they could express their emotional responses via VMC.
29
The development areas of digital skills of health care professionals
The development areas of HCPs’ digital skills are based on descriptions by researchers,28,31,37,39,41,43,44,48 HCPs themselves,29,30,32–35,42,46,47,50,51 or patients.38,49 The development areas for digital skills formed five main categories: improving skills for (a) information technology,33,37,41–43,46,47,51 (b) ethical practice,28,30,41,50 (c) creating a human-oriented relationship,29,34,38,44,49 (d) digital patient education and support28–32,35,36,38,39,41,43,44,48–50 and (e) implementing digital health (Table 3).28,34,35,42,49,51
Developing skills for information technology comprises three sub-categories: improving HCPs’ skills for using digital technologies,33,41 accessing digital resources37,42,43,46,51 and assessing digital health information.43,47 Using digital technologies includes learning basic operational skills for digital equipment, such as video-conferencing,
41
as well as assessing and developing computer skills
33
: All physicians and health staff participating in VC and the tele oncology service should undergo formal competency training in communication skills, basic operational skills for VC equipment and cultural awareness.
41
Developing skills for ethical practice comprises two sub-categories: protecting patients’ privacy28,30 and ensuring confidentiality.28,30,41,50 Protecting privacy was a concern in only 6% (n = 13) of the HCPs.
30
Ensuring confidentiality includes accessing patients’ information with their consent,
50
participation of a third person in a digital appointment
41
and the confidentiality of conversations
28
: It was often difficult to have confidential conversations on a telehealth visit conducted in a shared, tight clinic space. Nurses described colleagues’ talking in the background … team members continuously entering and leaving the clinic space while they were trying to focus during a telehealth encounter.
28
… many providers reported difficulties connecting with patients or concerns regarding their ability to forge or maintain a robust provider-patient relationship.
32
Future communication skills training programs for telephone-based supportive care needs to focus on responding verbally to patient emotional cues and verballing expressing empathy by health professionals.
44
Digital interaction includes using different digital media in communication.
29
It also includes having necessary communication skills29,41,49 and keeping nuances during digital communication, as digital appointments are often more factual, shorter and with fewer nuances compared to in-person appointments.
49
In addition, it includes preserving the human component in interaction,
38
showing facial expressions,29,44,49 and being present with a caring tone of voice and guidance
34
: Given the significance of empathy and support that patient experience in the cancer centers, attention to preserving the humanistic aspects of cancer care should be at the forefront of this virtual endeavour.
38
The low number of utterances… and checking patient understanding… confirms the need for skills training to specifically assess clarification of patient understanding.
44
Discussion
This systematic review produced a synthesis of digital skills of HCPs in cancer care divided into three areas, that is, the required and existing digital skills and the development areas of these skills. Existing and required digital skills of HCPs working in cancer care are a broad skillset covering skills for information technology, ethical practice, creating a human-oriented relationship and digital education and support. The studies were mainly conducted in recent five years, which is understandable considering the topic. According to the findings, the level of HCPs’ existing digital skills was not systematically assessed by the professionals themselves or others involved. Due to the digital transformation in cancer care, there is an emerging need for research on HCPs’ digital skills. Most of the studies showed good internal validity and decent quality. However, they were not specifically designed to study HCPś digital skills but rather, HCPs’ experiences related to digitalisation and its effects on care delivery. Only four studies addressed the digital skills in more detail33,36,42,46; however, one of them was designed to evaluate HCPs’ knowledge of institutional e-resources 46 with fair study quality. Three other studies designed to explore HCPs’ needs to improve their information technology skills, 33 its current use, perceptions of AI 42 or training needs for conducting e-counselling 36 showed lower methodological quality and the results should thus be viewed with caution.
Required and existing digital skills of HCPs in cancer care
In previous literature, digital skills of HCPs in cancer care were looked at from the perspective of requirements or existing skills. None of the previous studies had compared the required and existing skills or assessed the level of these skills. Both the required and the existing skills had the same main categories that were related to information technology, ethical practice, human-oriented relationship and patient education and support. Some of the content in the main and sub-categories may seem overlapping because we have tried to express their core content in the areas of related content. Next, we discuss their correspondence with earlier studies and digital skills frameworks.9–11,13
In information technology, a study related to the required skills for information technology, that is, finding and assessing information from the Internet, was published almost 20 years ago, 31 and the requirements are likely to be different today. In recent years, requirements in skills related to digital technology have focused on preparing digital appointments, perhaps due to their strong increase in cancer care. HCPs have been required to have basic technical skills to produce digital cancer care services, as also reported in previous studies12,15,19 and digital skills frameworks. 11 In terms of existing skills, HCPs in cancer care perceived having skills to use computers and search and assess online information more than ten years ago.31,33 However, a recent study by Jarva et al. (2022) from various healthcare settings reported lack of technical skills related to software or technical equipment. 19 Since the use of digital technology has increased rapidly in cancer care, technical skills need to be updated accordingly to deliver quality healthcare, as outlined by WHO. 4 Skills and educational needs can vary considerably between HCPs, 20 which is why assessment of actual skills and focusing education on deficiencies of these skills is needed.
In ethical practice, the required skills focused on consent to and privacy during digital appointment. This is in line with digital skills’ frameworks related to safe and appropriate information delivery. 12 Privacy concern is relevant since digital appointments are often held in patients’ home environment, which may compromise privacy. In previous studies, privacy has been related to digital health data within services, such as whom the health information is shared. 52 Previously, patient consent has been related to users’ right to determine whether or how their personal data is collected, used or shared. 53 In terms of existing skills, HCPs in cancer care were not concerned with confidentiality and privacy during digital appointments, although the result does not tell us about real skills to protect patients’ privacy. Research on HCPs’ existing digital skills for ethical practice in cancer care is lacking, although ethical values are essential for HCPs. 54 Therefore, the skills need to be explored further from the perspectives of privacy, confidentiality and consent.
In human-oriented relationship, the required skills were related to a person-centred approach, rapport and including patients’ preference in recently published studies.32,34,35,43,45 This is in line with digital skills framework emphasising communication and collaboration in digital skills. 11 The fear of the patient–HCP relationship deteriorating due to digital technology has been addressed in previous studies,18,19,52 indicating that the relationship is seen as uniquely important in cancer care. In individualised care, HCPs need to evaluate whether digital health services are appropriate for the patient's situation 19 ; thus, knowing the patient well when making decisions about a digital appointment could enhance individualised cancer care. In terms of existing skills, the only skill reported within human-oriented relationship was building rapport. Some nurses felt that bedside manner can easily be adapted in the digital environment. 35 It means active listening, connecting with the patients’ story and exploring emotional cues. 55 Furthermore, patients felt that HCPs had skills to establish a good relationship and communicate in a respectful and supportive way digitally. 34 Due to lack of physical presence, non-verbal communication through camera may enhance digital communication. 20 Identifying non-verbal communication and training these skills in the digital environment could support a deeper connection with the patient. In the included studies, skills for individualised, person-centred care were not assessed, although they are essential aspects in the care of people with cancer.
In digital education and support, the required skills entailed ensuring patients’ understanding45,49 whereas individual approach in education was not reported as required skills of HCPs. In terms of existing skills, ensuring patients’ understanding was not reported; instead, the skills focused on digital interaction and support. HCPs in cancer care perceived digital interaction to be as easy and effective as in-person interaction, and some of them were able to express themselves emotionally as well.29,30 Assessing these skills could benefit the identifying of possible gaps in existing skills in providing support digitally.
Development areas on digital skills of HCPs in cancer care
Several development areas in HCPs digital skills were identified. Studies on development areas in the skills for information technology were published about ten years ago in Australia and USA,33,41,47 meaning that the data need to be updated. The need for skills development continues to focus on technical competence, but the emphasis is more on assessing the reliability of information sources and accessing digital sources such as artificial intelligence globally.42,51 Jarva et al. 19 have stated that using digital health requires skills for finding the correct information but also media literacy to critically evaluate the available information. The need of developing HCPs’ information technology skills has been addressed in previous studies19,56 and digital skills framework, 11 as well.
In ethical practice, the development area was related to privacy and confidentiality during digital appointments. These studies were mostly conducted during the last few years in the USA, Australia and the United Kingdom.28,30,41,50 Further research is needed on ethical skills in digital cancer care to ensure its continued use in the future. In creating a human-oriented relationship, the development areas focused on building rapport and expressing empathy. Today, HCPs may lack skills to establish an emotional connection with patients and to maintain rapport digitally.30,32 Previously, this has been a challenge from both patients’ and HCPs’ perspective.19,20,52 Offering continuing education and opportunities to practice skills for human-oriented relationship digitally could enhance the skills for building rapport in cancer care. In delivering difficult news, the development area was focused on responding patients’ emotions and providing comfort without touching.29,44,48 Careful preparation of such a delicate situation and training these skills in clinical settings is needed. HCPs’ skills for delivering difficult news digitally for people with cancer have not been reported in previous studies. This may be connected to HCPs’ preference to deliver difficult news in-person. Continuing education and careful preparation are needed to further develop these skills digitally as in-person appointments are not always possible.
In patient education and support, there were many development areas, the focus being on digital communication skills, which have been studied globally over the years,41,49,50 and especially on non-verbal communication skills,29,44,49 maybe due to the increasing number of digital appointments in cancer care. In this area, a study reporting lack of skills to conduct e-counselling was topical ten years ago, 36 which means that findings need to be considered with caution. Studies addressing ensuring patients’ understanding and encouraging patient participation have also been published during the last decade,29,38,44,49 indicating global interest in the matter. In digital education and support, the development areas focused on digital interaction and obtaining necessary information. Skills for providing e-counselling was a current area of skills about ten years ago 36 and it is necessary to update the level of these skills. Studies addressing patients’ understanding and encouraging patient participation have also been published during the last decade, which indicates global interest in the issue.29,38,44,49 One development area was assessing patients’ condition remotely, which has been reported in recent years.28,30,32,38 Inability to perform a hands-on physical examination digitally requires new skills of HCPs.18,19 It could be useful to innovate, together with the patients, how to replace a physical examination at a digital appointment. An important development area is checking patients’ understanding of the information provided during the digital appointment. Given that misunderstandings occur in the digital environment, 50 practising skills to ensure patients’ understanding could enhance patients’ understanding of the information provided.
In implementing digital health, research conducted in Europe and Australia42,51 demonstrates that HCPs can play a significant role in implementing digital services to cancer care practice. Creating a standard policy and introducing guidelines for digital cancer care services were the main development areas in implementing digital health. Those delivering digital cancer care need to be aware of state laws and regulations that govern digital health practice, 18 especially when implementing new technologies such as artificial intelligence. Legal concerns related to the use of artificial intelligence in cancer care include governance, liability and accuracy. 57 Digital health ethic codes, on the other hand, focus on the establishment of the principles such as quality, privacy and informed consent among digital services.17,53 These recommendations and guidelines are important to implement in cancer care to enhance HCPs’ digital skills.
Conclusion
This systematic review provides a novel synthesis of the required and existing digital skills of HCPs in cancer care, as well as the development areas of these skills. Both requirements and existing skills were identified in the literature. There are no, however, studies comparing the required and existing skills which could give also future development areas. Therefore, numerous development areas exist, with emphasis on using digital health technology in communication and education and creating an emotional connection with the patient. These skills are needed to ensure successful deployment of digital technologies in cancer care. In clinical practice, continuing education, considering both existing skills of HCPs and clinical requirements, is needed for the further development of these skills. The findings of this review can be used in development activities and research in this field. The required digital skills need clarification related to digital patient education and delivering difficult news. Studies assessing HCPs’ existing digital skills in cancer care are scarce, especially related to ethical practice and patient education. Therefore, quality studies assessing these skills with valid instruments are needed.
Strengths and limitations
The strength of this review is that it provides a comprehensive synthesis of HCPs’ digital skills in cancer care, identifying both skills that are required, skills that already exist and skills that need to be developed. We also used several databases without time limit, applying along historical perspective. Another strength is that good scientific practice was followed during the research process. The data selection, extraction and analysis process were conducted independently by the authors and confirmed by the research group. 58
There are also limitations in the review. The first one has to do with the focus of the studies analysed: in the studies, digital skills were mainly described, not assessed. Moreover, in some cases, data was analysed relying on interpretation of the researchers, which might pose a risk to the validity of the results. 25 No valid tools for assessing the digital skills were identifiable in the literature. The second limitation has to do with the concept of skill, which was described as an independent concept or as part of digital competence, with overlapping between these two concepts. In most of the earlier studies, skill is part of competence, but also an independent concept. Thus, in future studies it would be relevant to clarify this conceptual discrepancy; the problem is, however, that these concepts are not clearly defined in the literature. The third limitation has to do with the nature of the studies included: their methodological quality was not very high, and this clearly limits the generalisation of the results. Thus, the results of this review can be seen as indicating thoughts for future developments.
Implications for practice, policy and research
The results of the review have several implications. In practice, these implications have to do with existing digital skills. These are skills that professionals can be assumed to have, and practice can rely on them. There are, however, many skills still that require development, which must be considered in clinical practice and in new service fields for patients with cancer, for example, by creating a human-oriented relationship and ensuring patient understanding digitally. To secure high-level ethical practice, issues such as patients’ privacy and confidentiality need to be considered during digital appointments in cancer care. This review indicates the implementation of ethical and practical guidelines to support digital cancer care. Assessment of HCPs’ actual skills and educational needs could further enhance the use of digital technologies in cancer care; thus, development and validation of instruments to assess digital skills of HCPs in cancer care are also implications for future research.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241240907 - Supplemental material for Digital skills of health care professionals in cancer care: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241240907 for Digital skills of health care professionals in cancer care: A systematic review by Tuominen Leena, Poraharju Jenna, Carrion Carme, Lehtiö Leeni, Leino-Kilpi Helena, Moretó Sònia, Stolt Minna, Sulosaari Virpi and Virtanen Heli in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241240907 - Supplemental material for Digital skills of health care professionals in cancer care: A systematic review
Supplemental material, sj-docx-2-dhj-10.1177_20552076241240907 for Digital skills of health care professionals in cancer care: A systematic review by Tuominen Leena, Poraharju Jenna, Carrion Carme, Lehtiö Leeni, Leino-Kilpi Helena, Moretó Sònia, Stolt Minna, Sulosaari Virpi and Virtanen Heli in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241240907 - Supplemental material for Digital skills of health care professionals in cancer care: A systematic review
Supplemental material, sj-docx-3-dhj-10.1177_20552076241240907 for Digital skills of health care professionals in cancer care: A systematic review by Tuominen Leena, Poraharju Jenna, Carrion Carme, Lehtiö Leeni, Leino-Kilpi Helena, Moretó Sònia, Stolt Minna, Sulosaari Virpi and Virtanen Heli in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Antoni Baena, Francesc SaigÍ, Heli Kokkinen, Tanja Vienonen and Teija Franck for their assistance and guidance in this research.
Contributorship
CC, HLK, SM, HV, JP, VS, LT and MS were responsible for the study’s conception and design, with assistance of LL designing and conducting literature search. CC and SM assessed quality of studies. JP and LT extracted and analysed the data, with assistance of HLK, HV and MS. JP and LT wrote the original draft of the manuscript, with assistance of CC and LL. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This is a systematic review of published literature and does not require ethical approval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the European Union [2023,101101253]. Views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union or the Health and Digital Executive Agency (HaDEA). Neither the European Union nor the granting authority can be held responsible for them.
Guarantor
HLK.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.