
Abstract
Implementation of artificial intelligence (AI) in medical decision-making is still in early development. We developed an AI robot intervention prototype with a health literacy-friendly interface that uses interactive voice response (IVR) surveying to assist in decision-making for weight loss. The weight-specific health literacy instrument (WSHLI) and Shared Decision-Making Questionnaire (SDMQ) were used to measure factors influencing weight-loss decisions. Factors associated with participants choosing to lose weight were analyzed using logistic regression, and factors influencing the selection of specific weight-loss plans were examined with one-way analysis of variance. Our study recruited 144 overweight or obese adults (69.4% women, 58.3% with body mass index (BMI) ≥ 24). After interacting with the AI robot, 78% of the study population made the decision to lose weight. SDMQ score was a significant factor positively influencing the decision for weight-loss (odds ratio [OR]: 2.16, 95% confidence interval [CI]: 1.09–4.29, p = 0.027). Individuals who selected self-monitored lifestyle modification (mean ± SD: 11.52 ± 1.95) had significantly higher health literacy than those who selected dietician-assisted plan (9.92 ± 2.30) and physician-guided treatment (9.60 ± 1.52) (both p = 0.001). The study results demonstrated that our prototype AI robot can effectively encourage individuals to make decisions regarding weight management and that both WSHLI and SDMQ scores affect the choice of weight-loss plans.
Background
Obesity is a major health problem worldwide. In 2016, the World Health Organization estimated that globally more than 1.9 billion adults were overweight (body mass index [BMI]: 25–29.9 kg/m2) and that 650 million adults were obese (BMI ≥ 30 kg/m2). 1 Obesity is associated with an increased risk of cardiovascular morbidity, diabetes, musculoskeletal disorders, and cancer. 1 From 1999 to 2018, the prevalence of obesity in the United States increased from 30.5% to 42.4%, and the prevalence of severe obesity increased from 4.7% to 9.2%. 2 Obesity was also associated with 4 million deaths and 120 million disability-adjusted life-years globally in 2015 and caused more than 320,000 deaths in the United States alone in 2014. 3 Obesity accounts for approximately US$149.4 billion per year and an annual average of US$1901 per obese person in the United States. 4 The Nutrition and Health Survey in Taiwan (NAHSIT, 2013–2016) found that one in five people in Taiwan is obese. 5 Thus, it is paramount to focus on weight loss and management to reduce morbidity and mortality worldwide. Weight-loss methods include self-monitored lifestyle modification, specific programs that promote an energy-restricted diet, physical activity, pharmacological therapy, and bariatric surgery.
Two potential factors associated with an individual's weight management plan are health literacy and shared decision-making (SDM).6–8 Specifically, health literacy is a growing concern in public health policy and health promotion across the globe. Healthy People 2030, an initiative by the U.S. Department of Health and Human Services designed to improve the health and well-being of Americans, defined personal health literacy as “the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others.” 9 Many countries have addressed health literacy as a critical component in healthcare policies to improve population health. 10 Lower health literacy levels have been consistently associated with increased hospitalization, inability to take medications appropriately, and poor ability to interpret labels and health messages. 11 However, empirical evidence regarding the association between health literacy and preference for weight-loss intervention has rarely been reported. 11
SDM is an approach where clinicians educate patients on the best available evidence and patients are encouraged to make informed choices according to their preferences during the clinical decision-making process. 12 SDM empowers patients to choose the medical treatment plan most suitable for them and is a critical component of patient-centered care. 13 One study suggests that SDM is an effective strategy for improving patient satisfaction with the medical care they choose. 14 Shared decision-making applications in medicine, including weight management facilitates patient involvement in complex clinical problems and leads to improved patient-perceived quality of care. 14 The Health Information National Trends Survey in the United States found that SDM was done more than two times more often among adults who sought and consumed health information more frequently, 15 thus indicating that patients with higher health literacy skills may have higher involvement in SDM. 15
Innovations in artificial intelligence (AI) and robotics have offered new methods for medical care. AI applications have been developed to solve some of the problems that health organizations currently face, for example, insufficient manpower and health information to empower patients’ health literacy. AI technologies can be used to improve the efficiency of the process of shared decision-making, and access to health services, thus achieving a better institutional health literacy environment. AI-associated technologies include machine learning, natural language processing, and AI voice assistants, 16 as well as speech recognition, image recognition, and text-to-speech functions. Medical institutions have used AI in the contexts of medical education, preoperative instructions, and question-and-answer interactions after medical education. 17 Through observing patient interactions with AI, we can measure and improve patients’ health literacy and ability to perform SDM. This intervention can be a time-efficient way to perform SDM with patients and help them make weight-loss decisions that adhere to current guidelines. However, previous studies suggested that we were still in the infancy stage of applying AI to assist in weight loss–related behaviors. 18 Although several studies had developed a robot-assisted system to improve health literacy or designed technology-assisted tools for weight loss, there were some limitations with these studies, that is, small sample size, lack of health literacy level data from participants, and questionnaires without verified validity.19–23
In order to fill up the literature gap regarding how AI can be implemented with health literacy and SDM in making weight-loss plans, we aimed to develop an AI prototype intervention to evaluate the percentage of participants deciding on weight loss afterward. This study further examines the factors influencing the selection of specific weight-loss plans. Moreover, how health literacy and SDM associated with weight management decisions were assessed.
Methods
In the present pilot study, we recruited healthy adults from a single medical center and used an AI prototype to intervene and evaluate their decisions on weight loss along with its influencing factors, health literacy level, and SDM score.
Study population
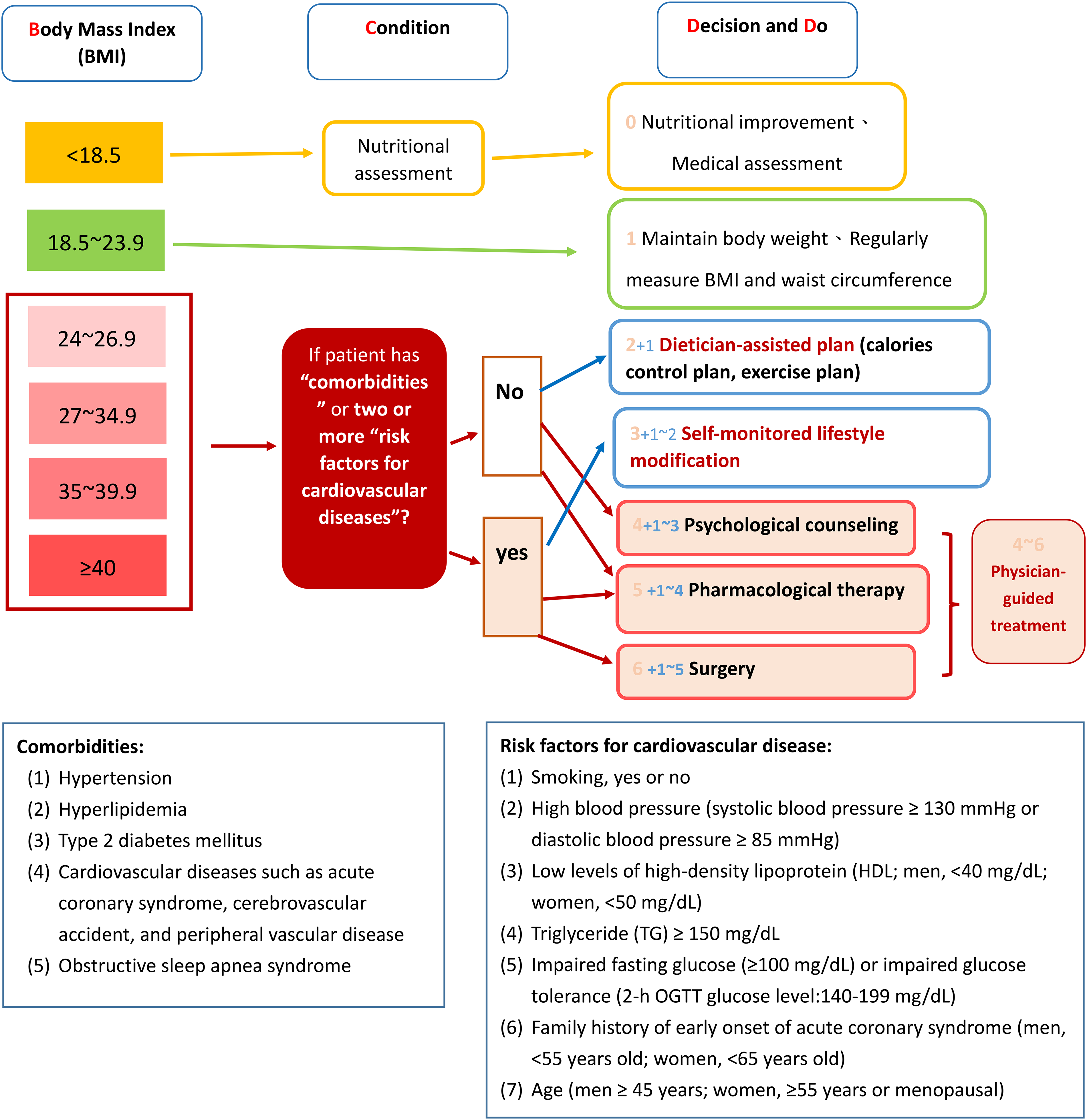
Patients were recruited in the waiting area of the department of Family Medicine and the health examination center at E-Da Hospital in Kaohsiung, Taiwan, from September to November 2019. Inclusion criteria were Taiwanese patients aged 18–65 years. We excluded pregnant women. Patients were stratified by BMI following the Taiwan Ministry of Health and Welfare (MOHW) Guidelines: normal weight (18.5 ≤ BMI < 24), overweight (24 ≤ BMI < 27), mild obesity (27 ≤ BMI < 30), moderate obesity (30 ≤ BMI < 35), and severe obesity (35 ≤ BMI < 40). We used questionnaires to ask patients whether they had the following clinical characteristics at baseline: obesity-related comorbidities (hypertension; hyperlipidemia; type 2 diabetes mellitus; cardiovascular diseases such as acute coronary syndrome, cerebrovascular accident, and peripheral vascular disease; and obstructive sleep apnea syndrome) and risk factors for cardiovascular disease: (1) smoking (yes or no) (2) high blood pressure (systolic blood pressure ≥ 130 mmHg or diastolic blood pressure ≥ 85 mmHg), (3) low levels of high-density lipoprotein (HDL; men, <40 mg/dL; women, <50 mg/dL), (4) triglyceride (TG) ≥ 150 mg/dL, (5) impaired fasting glucose (≥100 mg/dL) or impaired glucose tolerance (2-h OGTT glucose level:140–199 mg/dL), (6) family history of early onset of acute coronary syndrome (men, <55 years old; women, <65 years old), and (7) age (men ≥ 45 years; women, ≥55 years or menopausal).
Prototype intervention
The prototype program was delivered through the touchscreen surface of an AI robot. The program included (1) interactive voice response (IVR) survey method for collecting participant health data, (2) the weight-specific health literacy instrument (WSHLI) (Table S3), 24 and (3) the shared decision-making questionnaire (SDMQ) (Table S2). 25 Informed consent was obtained prior to participation in this study. Participants interacted with the robot to learn about the differences between weight-loss plans so as to make their final choices (Figure 1). Trained personnel who have been taught by the principal investigator through instruction and practice assisted the participants in completing the robotic intervention. To improve the quality of reporting, we used the Template for Intervention Description and Replication (TIDieR) checklist (Table S1). 26

Prototype artificial intelligence robot.
Interactive voice response (IVR) survey method
The IVR survey method was used to assess obesity levels and general health conditions in the study population (Figure 2). The AI robot used facial recognition or National Health Insurance card number to identify the patient and activate the IVR system to record patient data. After completing the initial assessment, a 3-min health literacy video about weight loss (developed by the Health Promotion Administration, MOHW) was played. The content of the 3-min health literacy video introduces the definition and basic concepts of obesity. It also reminded patients of chronic diseases and complications related to obesity, as well as its impact on Taiwan and the world.

The development of interactive voice response (IVR) methods from AI robots.
Next, the AI robot inquired about the patient's height, weight, and medical history (comorbidities and risk factors for cardiovascular disease). Then the robot displayed different weight-loss plans based on current evidence-based guidelines (Figure 3) on adult obesity management developed by the Health Promotion Administration and includes home-based obesity management resources. 27 The weight-loss intervention plans include (1) self-monitored lifestyle modification (2) dietician-assisted plan (3) physician-guided treatment.
Evidence-based guidelines on adult weight management.
After being shown the available options, patients chose an initially preferred weight-loss plan. Then, the AI robot provided information about the advantages and disadvantages of different weight-loss plans. Next, patients answered questions on the personal factors affecting choice of weight-loss plan, such as expected weight loss in one year, difficulty of maintenance, convenience, degree of starvation, exercise requirement, cost, side effects, health professionals’ advice, and self-determination. Then, they answered the six questions of the Shared Decision-Making Questionnaire (SDMQ) to test knowledge of weight-loss management. After the intervention, participants decided on a final weight-loss plan.
Shared decision-making questionnaire (SDMQ)
The SDMQ (provided by the MOHW) (Table S2) was used to measure the patient's knowledge of weight management. 25 Using the IVR method, the AI robot explained the advantages and disadvantages of each weight-loss plan and then allowed patients to choose an appropriate plan. The SDMQ, used to assess patient knowledge during the shared decision-making process, has been widely used in clinics, health centers, and hospitals in Taiwan.
Weight-specific health literacy instrument (WSHLI)
The WSHLI (Table S3) measures functional health literacy levels using 13 questions. The first part of the instrument requires patients to read a health education summary and answer five-related questions. The second part includes eight situational questions associated with diet, physical activity, and weight management. All questions are in a multiple-choice format (score range: 0–13). 24
The construct validity of the WSHLI is supported by high correlation between WSHLI and short-form Mandarin Health Literacy Scale(s-MHLS). Both health literacy screening questionnaires assess comprehension and writing. The WSHLI is significantly correlated with s-MHLS (γ = 0.71, p < 0.001; γ = 0.22, p < 0.001), comprehension (γ = 0.32, p < 0.001: γ = 0.10, p < 0.05), and writing (γ = 0.44, p < 0.001: γ = 0.11, p < 0.05). 24 The WSHLI's Cronbach's α coefficient, an indicator of reliability, measured 0.81. Thus, the WSHLI is a valid and reliable instrument for evaluating weight-specific health literacy in the Mandarin Chinese–speaking population. 24
Statistical analysis
Chi-square test and t-test were used to compare differences in baseline sex, BMI, comorbidities, and risk factors for cardiovascular diseases. The aforementioned AI robot runs an interactive program that collects patient information such as general characteristics, personal factors (i.e. expected weight loss in one year, difficulty of maintenance, convenience, degree of starvation, exercise requirement, cost, side effects, health professionals’ advice, and self-determination). We built the model based on stepwise logistic regression, selected variables with p < 0.05, and excluded those with p > 0.10. 28 The explanatory variables were comorbidities associated with hyperlipidemia, risk factors associated with triglyceride (TG) ≥ 150 mg/dL, and risk factors associated with low HDL level. The variable derived from the literature review was health professionals’ advice.
The outcome variable was whether the participant chose to lose weight after the AI prototype intervention. We analyzed the associations between making the decision for weight loss and its influential factors, for example, scores derived from the WSHLI and SDMQ and the personal factors affecting the choice of weight-loss plan, such as expected weight loss in one year, difficulty of maintenance, convenience, degree of starvation, exercise requirement, cost, side effects, health professionals’ advice, and self-determination. We further stratified these associations by participants’ baseline BMI (normal/overweight/obese). The subgroup analyses of the associations between choosing different weight-loss plans (self-monitored lifestyle modification/dietician-assisted plan/physician-guided treatment) and influential factors were done. One-way analysis of variance was used to examine the association of BMI, WSHLI, and SDM and different weight management decisions.
All statistical analyses were performed with SPSS v19 (IBM, Armonk, NY, USA). This study was sponsored by E-Da Hospital Intelligent Medical Center and the National Health Agency and was approved by the Human Experiment Committee of E-Da Hospital (IRB number: EMRP-108-011).
Results
Our study population included 144 adults (44 men and 100 women). Of them, 84 (58.33%) were overweight (11 men and 25 women) or obese (22 men and 26 women). The mean BMI of those making the decision for weight loss (BMI = 25 ± 5.02) was lower than those deciding against it (BMI = 27 ± 4.50), but the difference was not significant (p = 0.087; Table 1). The SDMQ scores and the perceived importance of health professionals’ advice were significantly higher in the group making the decision for weight loss. Among those who chose to lose weight, 27% of patients were overweight and 28% of patients were obese. Of those who did not want to lose weight, 13% were overweight and 56% were obese.
Descriptive analysis of patient characteristics by the weight management decision.

Statistically significance at p < 0.05.
BMI: body mass index; SDMQ scores: Shared Decision-Making (SDM) Questionnaire scores; WSHLI: Weight-Specific-Health-Literacy-Instrument.
We compared the relationship between comorbidities and risk factors for cardiovascular disease on weight-loss decision (Table 2). Comorbidities were not significantly different between the groups of making the decision for or against weight-loss. A significantly smaller proportion of patients making the decision for weight loss had low high-density lipoprotein (HDL) compared to those who did not choose weight loss (3.5% vs. 5.6%; p = 0.002). The weight-loss group also had a significantly higher percentage of people with hypertriglyceridemia (7.6% vs. 6.3%; p = 0.044).
Descriptive analysis of comorbidities, risk factors for cardiovascular disease, by participants’ weight management decisions.

High blood pressure: systolic blood pressure≥ 130 mmHg or diastolic pressure ≥ 85 mmHg).
Low high-density lipoprotein (HDL): male < 40 mg/dL, female < 50 mg/dL.
Statistically significant at p < 0.05.
High Triglyceride(TG) ≥ 150 mg/dL.
Impaired fasting glucose: fasting glucose: 100–125 mg/dL or impaired glucose tolerance: 2-h OGTT glucose level :140–199 mg/dL.
Family history of early onset of acute coronary syndrome: male < 55 years old, female < 65 years old.
Overall, 112 of 144 patients (77.78%) were willing to adopt a weight-loss plan after the AI prototype intervention. Of these, 80 were women (80%) and 32 were men (72.73%). The proportion of women was slightly but not significantly higher than that of men. At the end of the process, patients had to choose a weight-loss plan and 90.36% of patients made their final decision based on the evidence-based guidelines on adult weight management, 16 and no significant difference was seen between men and women.
Univariate analysis of factors influencing patients’ decisions for weight loss revealed SDMQ scores (p = 0.037) and health provider advice (p = 0.032) to be significant factors. Multivariate regression revealed only SDMQ scores (p = 0.027) as a significant factor leading to patients making the decision for weight loss (adjusted OR: 2.16, 95% CI: 1.09–4.29; Table 3).
Factors influencing patients’ making the decision for weight loss.

Adjusted for hyperlipidemia, triglyceride (TG) ≥ 150 mg/dL, and low high-density lipoprotein (HDL): male < 40 mg/dL, female <50 mg/dL.
Statistically significant at P < 0.05.
SDMQ scores: Shared Decision-Making (SDM) Questionnaire scores; WSHLI: Weight-Specific Health Literacy Instrument Scale.
After stratification of the study population by BMI, we found that influential factors for choosing weight-loss plans were different among obese patients (BMI ≥ 27; Table 4). In the obese group, the decision for weight loss was significantly influenced by SDMQ score (p = 0.042).
Influential factors for making weight-loss decisions according to BMI stratification.

BMI: body mass index; SDMQ scores: Shared Decision-Making (SDM) Questionnaire scores; WSHLI: Weight-Specific-Health-Literacy-Instrument.
Statistically significant at p < 0.05.
There were no significant differences in SDMQ scores between participants who selected different weight-loss plans (including self-monitored lifestyle modification; dietician-assisted plan; and physician-guided treatment). However, we found that the group that chose self-monitored lifestyle modification (mean ± SD: 11.52 ± 1.95) had significantly higher WSHLI scores than groups choosing dietician-assisted plan (9.92 ± 2.30) or physician-guided treatment (9.60 ± 1.52; both p = 0.001; Table 5). This finding indicates that patients with higher health literacy for weight-loss management were more likely to choose self-monitored lifestyle modification than healthcare professional-assisted options.
One-way analysis of variance results for BMI, WSHLI, SDMQ scores and health professionals’ advice among participants choosing different weight-loss plans.
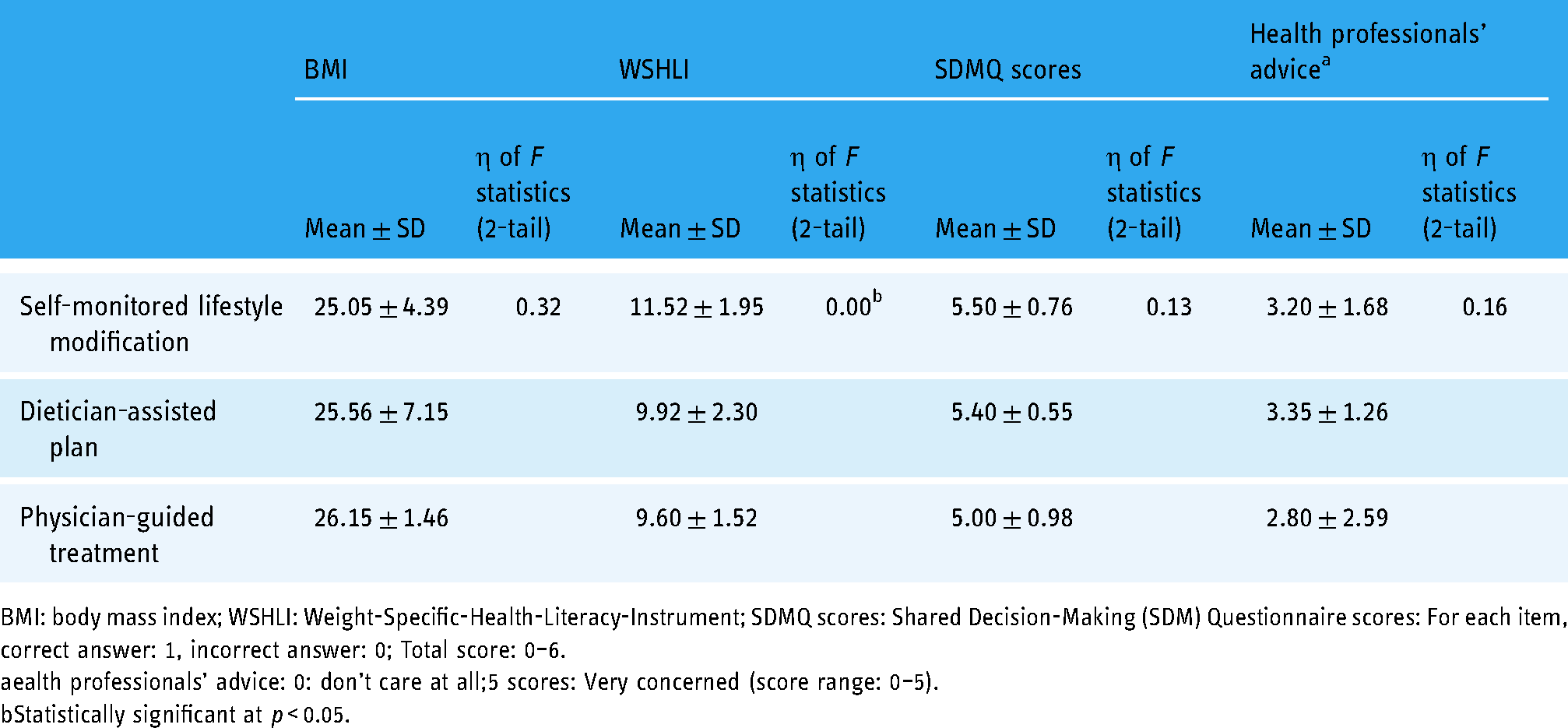
BMI: body mass index; WSHLI: Weight-Specific-Health-Literacy-Instrument; SDMQ scores: Shared Decision-Making (SDM) Questionnaire scores: For each item, correct answer: 1, incorrect answer: 0; Total score: 0–6.
ealth professionals’ advice: 0: don't care at all;5 scores: Very concerned (score range: 0–5).
Statistically significant at p < 0.05.
Discussion
Our study used a novel AI prototype intervention to assist participants in making weight management decisions through shared decision-making. Approximately four in five patients decided to lose weight after the intervention. Moreover, >90% of patients chose the weight-loss plan according to evidence-based guidelines on adult weight management. SDMQ scores were positively associated with making the decision for weight loss. Furthermore, this association remained significant among obese patients in our cohort after the stratification of the study population by BMI. To the best of our knowledge, this is the first study to find that patients who have higher health literacy are more likely to choose self-monitored lifestyle modification over healthcare professional-assisted options to lose weight.
The application of AI robots in medical care is burgeoning.19–21 Wei et al. developed a robot-assisted learning system to improve health literacy and learning perception for the elderly. 20 Other studies have designed technology-assisted tools for weight loss.7,22,23 For example, Watson et al. used a digital tool called the Web-Based Behavior Change Program for weight-loss intervention. 23 Their retention rate for the first three months was 78%, which was similar to that in our study. 23 Moore et al. 7 developed a patient decision aid to support SDM for making weight management decisions. They offered two major treatment options for severe obesity: intensive lifestyle management and bariatric surgery plus lifestyle management. Most (93%) participants reported having enough support/advice to make a choice, and 89% felt their decision was the best choice. 7 In contrast to our study, their population focused on adolescents (12–17 years old) with severe obesity (defined as BMI ≥ 120% of the 95th percentile for age and sex or ≥35 kg/m2) 29 ; therefore, it is possible that adolescents or more obese patients might be more willing to make the final choice for weight loss after technology-assisted intervention. Although AI technology can facilitate decision-making for weight loss, our study results point out that the health information presented should be adjusted based on the patient's level of health literacy. Therefore, future studies should include a personalized interface on AI robot based on health literacy level, so as to help patients choose plans most suitable for themselves according to current weight-loss guidelines.
Examining the association between influential factors and making the decision for weight loss, we found that the SDMQ scores positively influenced patients to decide on weight loss.
SDM in healthcare is positively associated with improvement in patients’ health outcomes 30 and is affected by patients’ health literacy.30–32 Ousseinea et al. found that adequate patient participation in SDM requires high levels of health literacy, particularly in the functional and communicative domains. 31 Health literacy can be improved by public health campaigns or professional education. 33 Thus, raising patient's health literacy can facilitate SDM and improve patient-centered medical care.
Evidence-based guidelines on adult weight management recommend three weight-loss plans: (1) self-monitored lifestyle modification, (2) dietician-assisted plan (including calorie control, exercise, or behavior therapy), and (3) physician-guided treatment. Patients who have higher weight-specific health literacy levels chose self-monitored lifestyle modification over other options in our study. Robert et al. used a stepped-care approach to weight-loss management and found regular self-monitoring and high health literacy proved to be significant correlates of success. 34 One systematic review had evidence for the effectiveness of interventions that focused on improving knowledge and skills (health literacy) for weight loss. 35 Von Wagner and colleagues found that health literacy might affect a range of health actions. They proposed a framework from psychology perspective to depict the associations between health literacy and health outcomes that could be mediated by patients’ actions such as self-management of health and other motivational determinants. 36 Lower health literacy level was associated with increased hospitalization, poorer ability to take medications appropriately, poorer health outcomes, and higher rates of chronic disease.11,37 Health professionals can enhance patients’ health literacy to improve weight management and chronic disease control.
A patient-centered approach to illness, particularly for chronic pain conditions, may be more effective than the traditional approach. 38 It increases patient satisfaction with care and improves treatment adherence. 39 The key features of patient-centered communication are exploring the patient's experience of illness and working in partnership to define problems and choose a course of action. 39 SDM uses similar principles to emphasize the importance of exploring a patient's background and developing a strong patient–health provider relationship, 38 leading patients to feel comfortable with sharing their opinions and participating in SDM. 38 Our AI robot used patient-centered and SDM methods to interact with participants and help them select an appropriate plan for weight loss according to evidence-based guidelines. 27
This pilot study has limitations. A major limitation is the lack of a comparison group, so these results were not directly compared to that of a human provider. To analyze patient characteristics, we collected data on comorbidities and cardiovascular risk factors, but we lacked age and socioeconomic status data. We used health literacy as a substitute for patients’ socioeconomic variables. However, patients’ health literacy may be better evaluated with the addition of parameters related to education level and income. Patients who agreed to fill out health-related questionnaires may have healthier behaviors and also be more willing to receive medical therapy. This healthy user effect may have introduced a healthy participant bias in our recruitment. 40 Moreover, our participants answered the questionnaires through an AI robot, so they may have better digital literacy. The IVR survey is a new interface requiring verbal commands and touching the screen, so a lack of familiarity with the technology could have affected responses. Lastly, the size of screen was approximately 5.5 inches, requiring participants to slide the screen if the texts were too long. Lack of interface user-friendliness may have also influenced results.
Conclusions
Our findings indicated that our prototype AI Robot can encourage individuals to adopt a healthier lifestyle. The patients’ SDMQ scores were significantly associated with making the decision for weight loss. Participants with higher health literacy tended to prefer self-monitored lifestyle modification over professional-assisted treatment plans. In a clinical setting, our AI robot can be used to assist healthcare professionals in patient health education and involve patients in SDM. Further studies to measure weight changes after AI robot intervention are needed to validate and quantify the impact of our findings.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076221136372 - Supplemental material for Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions
Supplemental material, sj-doc-1-dhj-10.1177_20552076221136372 for Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions by Yi-Tang Chu, Ru-Yi Huang, Tara Tai-Wen Chen, Wei-Hsuan Lin, James TaoQian Tang, Chi-Wei Lin, Chi-Hsien Huang, Chung-Ying Lin, Jung-Sheng Chen, Sabrina Kurtz-Rossi and Kristine Sørensen in Digital Health
Supplemental Material
sj-doc-2-dhj-10.1177_20552076221136372 - Supplemental material for Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions
Supplemental material, sj-doc-2-dhj-10.1177_20552076221136372 for Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions by Yi-Tang Chu, Ru-Yi Huang, Tara Tai-Wen Chen, Wei-Hsuan Lin, James TaoQian Tang, Chi-Wei Lin, Chi-Hsien Huang, Chung-Ying Lin, Jung-Sheng Chen, Sabrina Kurtz-Rossi and Kristine Sørensen in Digital Health
Supplemental Material
sj-doc-3-dhj-10.1177_20552076221136372 - Supplemental material for Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions
Supplemental material, sj-doc-3-dhj-10.1177_20552076221136372 for Effect of health literacy and shared decision-making on choice of weight-loss plan among overweight or obese participants receiving a prototype artificial intelligence robot intervention facilitating weight-loss management decisions by Yi-Tang Chu, Ru-Yi Huang, Tara Tai-Wen Chen, Wei-Hsuan Lin, James TaoQian Tang, Chi-Wei Lin, Chi-Hsien Huang, Chung-Ying Lin, Jung-Sheng Chen, Sabrina Kurtz-Rossi and Kristine Sørensen in Digital Health
Footnotes
Acknowledgments
The authors would like to thank Dr Jian-Han Chen, chief of the E-Da Hospital Metabolism and Diabetes Surgery Center for assistance in implementing this project; Yi-Chen Lee, chief of E-Da Hospital Department of Clinical Nutrition Therapy for offering nutrition recommendations; Chia-Wei Liu, family medicine physician for proofreading. The authors would also like to thank all the colleagues of E-Da Center of Medical Artificial Intelligence who provided the funding for this project.
Contributorship
Yi-Tang Chu and Ru-Yi Huang researched literature and conceived the study. Ru-Yi Huang was involved in protocol development, gaining ethical approval, patient recruitment and data analysis. Yi-Tang Chu wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript. Yi-Tang Chu is the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Human Experiment Committee of E-Da Hospital (IRB number: EMRP-108-011).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the EDA Center of Medical Artificial Intelligence (grant number EDAH-AI-107-013) and E-Da Healthcare Group (EDAHM109006).
Guarantor
RYH.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.