
Abstract
Objective
Childhood cancer patients need to have good treatment adherence. Unfortunately, treatment non-adherence often occurs due to high side-effect burdens of treatment and the lack of knowledge of one's illness and treatment. Therefore, a serious game intervention based on the Protection Motivation Theory (PMT) was designed and developed to motivate childhood cancer patients to undergo treatment, perform daily self-care and educate them about their illness.
Methods
Childhood cancer patients (6–17 years old) and their caregivers were recruited in a multi-centre, single-arm intervention in Malaysia. A total of 24 child-caregiver dyads have completed the study. This study used PMT-based surveys to collect quantitative data regarding children's motivation to adhere to treatment and perform daily self-care. Additionally, a 20-question multiple-choice quiz was used to determine children's knowledge levels. These surveys were conducted pre-test and post-test. Children's and caregivers' feedback were also gathered post-test as qualitative data.
Results
The results showed that overall, the children's intention to undergo cancer treatment had increased significantly. A significant increase in the intention to perform daily self-care was found among younger children, while older children showed significant improvement in their cancer knowledge levels. The post-test feedback suggested that the game was liked by both children and caregivers and it provided various benefits to children with cancer.
Conclusions
Findings suggest that the intervention has the potential to improve childhood cancer patients’ motivation for treatment adherence and daily self-care, in addition to educating them about cancer and treatment.
Introduction
Deaths from childhood cancer globally continue to outnumber those from infectious diseases such as tuberculosis, malaria and HIV infection. 1 Luckily, most childhood cancer fatalities can be prevented through early and timely diagnosis and treatment. 2 In Malaysia, where the incidence of childhood cancer is about 77.4 cases per 1 million children under 15 years old, 3 the local childhood cancer survival rate is reported to be at 70%. 4
However, undergoing cancer treatment has many challenges, including high side effects burdens. 5 Additionally, childhood cancer patients are often required to be hospitalized for treatment, which can be emotionally, physically and psychologically taxing. 6
Cancer patients' fears regarding treatment include symptoms of pain, nausea and fatigue, loss of independence, loss of control, not knowing what to expect, and changes to one's appearance, such as hair loss and scars. 7
The side effects and fears faced by cancer patients may discourage patients from keeping up with their treatment to fight cancer, which can lead to treatment non-adherence.
Treatment non-adherence can occur at any age, with very young children and very old adults being the least adherent. 8 Children with chronic illnesses can also be resistant to undergoing treatment, especially if the treatment was unpleasant, had bad side effects or was time-consuming.9,10
Additionally, a study 11 on the use of pain medication among children and adolescents reported that they tend to lack awareness, self-discipline and knowledge of medicines used. This lack of knowledge about their illness and treatment can cause children to develop unnecessary fears about their medication, affecting treatment compliance. 12
Children with chronic illnesses such as cancer do not like feeling different from other ‘normal’ children and do not like others knowing about their condition. 13 Similarly, adolescents also experienced difficulties accepting their chronic illnesses. Their need to look ‘normal’, and be more like their peers may cause poor treatment adherence. 14
Besides the factors above, poor treatment adherence can also be caused by forgetfulness, the lack of support and the lack of motivation of the patient. 15 For childhood cancer patients, treatment non-adherence or treatment abandonment can significantly decrease their chances of survival from the disease.
As treatment side effects are one of the main contributors to treatment non-adherence, childhood cancer patients should learn to manage them by practising proper daily self-care. They can do this by maintaining a balanced diet,16,17 drinking enough fluids daily,18,19 maintaining good personal hygiene,20,21 being well-rested, 22 and sharing their thoughts and worries with loved ones. 23 A positive outlook on the cancer experience can also help children with cancer improve their psychological well-being. 24
In addition, age-appropriate information about cancer and treatment should be taught to childhood cancer patients to help them cope with having cancer,25,26 and encourage them to be more compliant and understanding towards their treatment. 27 Lower complication rates and better long-term results in patients have been linked to good treatment compliance. 27 Furthermore, it was found that diabetic patients with a good understanding of diabetes had better medication adherence. 28 Therefore, it is important to consider the practice of good daily self-care, medical knowledge and motivation towards childhood cancer treatment, as these factors can affect treatment adherence.
Consequently, we have proposed a health intervention for children with cancer that can encourage them to adhere to their treatment, encourage daily self-care and educate them about cancer and treatment would be beneficial. We have conducted a literature review to determine the form of the intervention for children with cancer. The findings of this review are as follows.
It was observed that young children are adept at using mobile devices and often entertain themselves with mobile games.29,30 Digital play, such as video games, was also of therapeutic benefit to children with chronic illness in place of real-life physical play. 31 This shows that a mobile game intervention would suit childhood cancer patients.
Following this, a review 32 was performed on 11 existing game-based digital health interventions for cancer patients. The review suggested limitations to existing interventions, as games for children often have simple aims, seldom involve treatment adherence and lack focus on the importance of daily self-care in general. Existing interventions for children with cancer, such as Empower Stars!, 33 Ben's Game 34 and Pain Buddy 35 only focus on a limited number of game aims. The same review 32 also proposed that future interventions for childhood cancer patients should include multiple game aims supported by well-designed game mechanics to provide better overall care for childhood cancer patients.
Next, as children prefer animal game characters, 36 we look into virtual pets, which are electronic toys or games that simulate real pets that can be interacted with. 37 The virtual pet genre can motivate children to learn. 38 Besides that, these games have been used as health interventions, such as teaching children about asthma management 39 and encouraging healthy habits such as exercising and eating nutritious food.40,41 This aligns with the Social Learning Theory, 42 which states that people can learn new behaviours through observation, including from game characters. 43
Besides that, the Protection Motivation Theory (PMT) 44 was explored. This theory is used to understand why and how various individuals respond to potential health threats by picking up good health behaviours. According to the PMT, 44 a person's intention to utilize a health behaviour is influenced by seven factors which are separated into two categories. The first category, threat appraisal, is made up of perceived threat severity, perceived threat vulnerability, intrinsic and extrinsic rewards and fear arousal. The coping appraisal, which is the second category, includes perceived response-efficacy, perceived self-efficacy and response cost. For childhood cancer patients, threats they face include cancer itself, and treatment-related side effects. These children can adopt protective behaviours to cope with these health threats by adhering to cancer treatment to fight cancer and practising good daily self-care to manage treatment side effects.
To address these problems and incorporate the findings of the review, we have developed a virtual pet serious game called Pets vs Onco. In this paper, we aim to understand if the serious game can improve the intentions of children and adolescents with cancer (ages 6–17) in adhering to their treatment plans and performing daily self-care, as well as educate them about their illness and treatment.
This led to the following hypotheses:
H1: After playing a PMT-based virtual pet serious game, childhood cancer patients will have more intention to adhere to their treatment plans to fight cancer. H2: After playing a PMT-based virtual pet serious game, childhood cancer patients will have more intention to perform daily self-care to manage treatment side effects. H3: After playing a PMT-based virtual pet serious game, childhood cancer patients will become more knowledgeable about childhood cancer and cancer treatment.
We additionally aim to determine how much childhood cancer patients enjoy the serious game intervention. We intend to identify where the serious game does well and where it requires improvement for future work through the feedback from children and caregivers post-intervention.
Development of Pets vs Onco: a virtual pet serious game
According to our literature review findings, the prototype intervention for this study, Pets vs Onco, was conceptualized 45 and developed for Android mobile devices. In this game, players take care of a virtual pet's daily self-care and cancer treatment needs.
The development of this game was based on the two theories reviewed. The first theory was the Social Learning Theory, 42 which depicts that it is possible for a virtual pet game character to convey healthy habits to children. The virtual pet genre was chosen for this study's intervention as the pet can be used as a role model for undergoing cancer treatment and daily self-care. The second theory employed to guide the intervention's design and development was the PMT. 44 As the player learns about their illness and treatment, takes care of the pet and sees the good effects daily self-care and treatment can have on the pet; they can become more confident and motivated to take care of their own needs as well.
The previously mentioned review 32 identified that the game mechanics that can help motivate children to fight cancer through treatment are fighting virtual enemies and role-modelling good health behaviours. Continuous gameplay can be encouraged with game mechanics such as virtual rewards, custom avatars and randomly generated stages.
Pets vs Onco consists of multiple game modules,46,47 designed to support the intervention's aims. The game is also designed to boost the children's PMT coping appraisal by improving their response efficacy and self-efficacy for cancer treatment and daily self-care, and reducing the response costs of treatment side effects.
The following are the main game modules of Pets vs Onco:

Screenshots of Pets vs Onco mobile game. (a) Home screen, players can access care actions and other menus. (b) Mini-games selection screen. (c) Quiz mini-game, part of educational module. (d) Alarm screen. (e) Diary screen. (f) Pet customization screen, for a custom avatar incentive.
The Pets vs Onco prototype was tested and improved with voluntary adult playtesters until a final prototype was produced to be used as the intervention.
Methods
We followed a mixed-methods research approach in this study. Qualitative and quantitative data were collected to triangulate the research findings.
The evaluation of the game was conducted in three phases: pre-intervention preparation, the conduct of the intervention and post-intervention data analysis. Figure 2 depicts the overview of the methodology used.

Overview of the evaluation methodology.
Pre-intervention preparation
Before the intervention was carried out, we obtained the agreement from two cancer societies in Malaysia to collaborate, the Sarawak Children's Cancer Society (SCCS) and the National Cancer Society Malaysia (NCSM). Next, ethical approval for the study was obtained. Following that, the prototyping of the mobile game intervention (i.e. Pets vs Onco) was carried out.
After the preparation phase, eligible participants were recruited for the study to evaluate the intervention. Procedures that have been established were then used to carry out the pre-test and post-test surveys with the children and caregivers.
Participant selection: inclusion and exclusion criteria
Unless stated otherwise, the term ‘participant’ in this article refers to the children who participated in this study and does not include their caregivers.
To be eligible to take part in this study, participants needed to meet all of the following requirements:
Have a formal diagnosis of cancer Be between the ages of 6 and 17 Able to communicate basically in at least English/Bahasa Melayu/Chinese Have an Android device to install the game on Able to play the game for 1-month
This study excluded patients who were receiving palliative care. Participants were considered to have dropped out if they or their caregivers decided to discontinue the intervention for any reason before completing the post-test surveys, if the individual had passed away, or if they were no longer able to participate in the study due to changes in their circumstances.
Pre-test and post-test surveys
A single-arm pre-test–post-test design was used to evaluate the intervention. The surveys were conducted before the intervention and once again after the 1-month intervention to identify any improvements.
Two PMT-based surveys were developed for the study based on other studies which have utilized and created their own PMT-based surveys.49–56 The first PMT-based Survey (PMT Survey 1) is based on the PMT factors and the intention of participants to adhere to their cancer treatment to fight cancer. The second PMT-based Survey (PMT Survey 2) is based on the PMT factors and the intention of participants to use daily self-care to manage treatment side effects. Each of these PMT-based surveys were to be filled out by the children and their caregivers, as obtaining responses from both children and caregivers can allow for a clearer understanding of the child's views. 57
These PMT-based surveys utilize a Likert scale of 1–5, with 1 being ‘strongly disagree’ and 5 being ‘strongly agree’. This means that the higher the value, the stronger the belief for that PMT factor-based statement (Table 1).
Example of Protection Motivation Theory Survey Likert scale statement items.

The third survey is the Cancer Knowledge Survey. This is a 20-question multiple-choice quiz, developed to test children's knowledge levels of cancer and cancer treatment facts. This survey was produced by adapting the information from sources that educate children about cancer58,59 (Table 2).
Example of Cancer Knowledge Survey multiple choice question items.

Procedures for the conduct of intervention
All contact methods and forms for this study were conducted virtually due to the social distancing restrictions of the COVID-19 pandemic. The procedures used to conduct the intervention for each child/caregiver dyad are as follows:
The staff of SCCS, NCSM Kuala Lumpur branch and NCSM Melaka branch helped to facilitate the recruitment process by identifying children and adolescents that met the selection criteria and advertising the recruitment posters. During the recruitment process, parental consent was obtained from the caregiver of each eligible participant who was interested in participating. Basic demographic information on the participant, such as gender and age, was collected.
Post-intervention analysis
After the data had been collected, two types of data analysis were conducted. Quantitative analysis was used to analyse the pre-test and post-test surveys consisting of the PMT-based Surveys and the Cancer Knowledge Surveys. Qualitative analysis was conducted to identify themes from the feedback and follow-up responses.
As the data collected from both the PMT-based surveys and the Cancer Knowledge Survey were ordinal, non-parametric tests were used for the quantitative analysis.
For the analysis of the two PMT Surveys, three tests were conducted. The first test was the Spearman's rank order correlation coefficient, which was used to conduct a correlation analysis to determine the correlation of each PMT factor to the intention. Prior to the correlation analysis, the summary median values of all questions under each PMT factor were calculated. The next test was the Kruskal–Wallis H-test, which was used to determine if there were any differences between the children's responses and their caregivers. The final test was the Wilcoxon signed-rank test, which was used for hypothesis testing. The tests compared the pre-test and post-test scores to determine if there were any significant changes to the participants’ intention to use cancer treatment to fight cancer and their intention to use daily self-care to manage treatment side effects. This test was performed on all participants’ responses, and by dividing the children into two age groups, younger children (ages 6–12) and older children (ages 13–17).
The next part of the data analysis involved the quantitative analysis of the Cancer Knowledge Survey. Firstly, descriptive statistics were used to compare the pre-test and post-test minimum, maximum and median scores for the results. Next, the Wilcoxon signed-rank test, which was used for hypothesis testing, was carried out. The test compares the pre-test and post-test scores to determine if there are any significant changes. This test was also performed for all participants and then for younger children and older children.
Finally, data analysis was conducted for the feedback and follow-up responses. First, descriptive statistics were used to analyse the close-ended questions. Next, the mean and standard deviation (SD) were calculated to determine the overall game ratings. Finally, thematic analysis 62 was used to review, code and identify themes from the responses obtained. We analysed the qualitative data collected in this study according to the categories from our earlier study 47 where we identified the seven main themes. Therefore, this analysis was primarily deductive, and the sub-themes under each category were adjusted according to new findings from this dataset.
Results
The results of this study are presented based on data collected from three components: (1) the PMT Surveys, (2) the Cancer Knowledge Survey and (3) the feedback and follow-up responses.
A total of 24 child/caregiver dyads have completed this study. From this total, 10 child-caregiver dyads were recruited from SCCS, while 14 were from NCSM. Figure 3 depicts the recruitment flow from both cancer societies.

Recruitment flow of participants.
In total, there were 15 male and 9 female participants, with the ratio being 3:2 male to female participants. The participants’ ages at the time of recruitment averaged 11.75 ± 3.22, where the youngest was 6 years old, and the eldest was 17 years old.
PMT Surveys
The results from the PMT Surveys consist of the correlation analysis of the PMT factors, whether there is a difference between children and caregivers’ survey scores, and hypothesis testing.
Correlation analysis of PMT factors
Spearman's correlation coefficients were calculated to determine the relationships between the PMT factors and the intention for both PMT Surveys.
Correlation analysis results for PMT Survey 1 (cancer treatment).
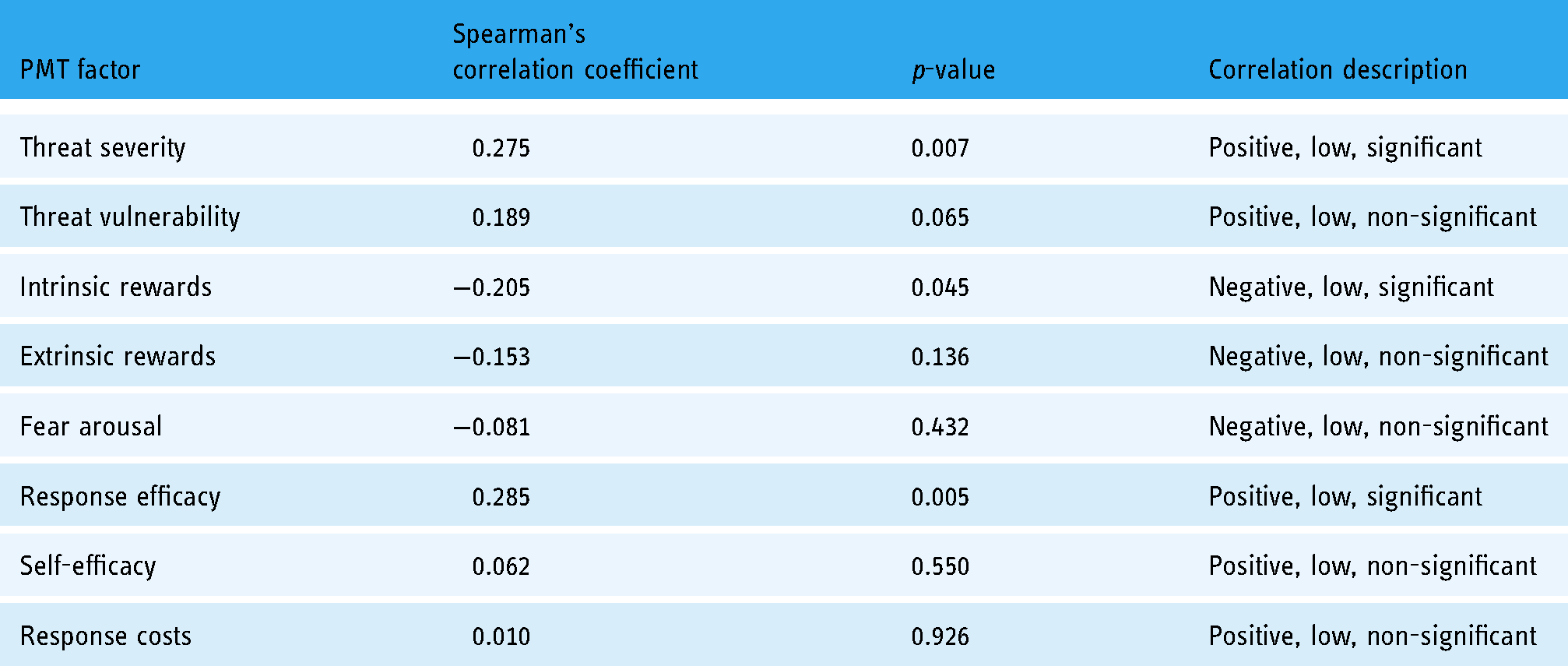
For PMT Survey 1 on using cancer treatment to fight cancer, PMT factors with significant levels (p < 0.05) of correlation with the intention were threat severity, intrinsic rewards and response efficacy (Table 3).
Correlation analysis results for PMT Survey 2 (daily self-care).

For PMT Survey 2 on using daily self-care to manage treatment side effects, PMT factors with significant levels (p < 0.05) of correlation with the intention were threat vulnerability, response efficacy and self-efficacy (Table 4).
Hypothesis testing
As no significant differences were found between the responses for the intention values between the children and caregivers for both the pre-test and post-test results of PMT Survey 1 and PMT Survey 2; the Wilcoxon signed-rank test was performed to compare the pre-test and post-test results of both PMT Surveys using the responses from each child/caregiver dyad (Table 5).
Wilcoxon signed-rank test results for pre-intervention and post-intervention intention.

*if p-value <0.05, it would indicate a significant difference in responses for the pre-intervention and post-intervention.
For the PMT Survey 1 to determine the participants’ intention to adhere to their cancer treatment to fight cancer, there was an increase in the scores for the pre-test results (Median = 4.0), and the post-test results (Median = 5.0); p = 0.0003, p < 0.05.
Next, for the PMT Survey 2 to determine the participants’ intention to use daily self-care to manage treatment side effects, there was an increase in the scores for the pre-test results (Median = 4.0) and the post-test results (Median = 4.5); p = 0.006, p < 0.05. As a result, the evidence proved that after playing the serious game, participants became more motivated to adhere to their cancer treatment and perform daily self-care.
Wilcoxon signed-rank test results for pre-intervention and post-intervention intention for younger and older age groups.
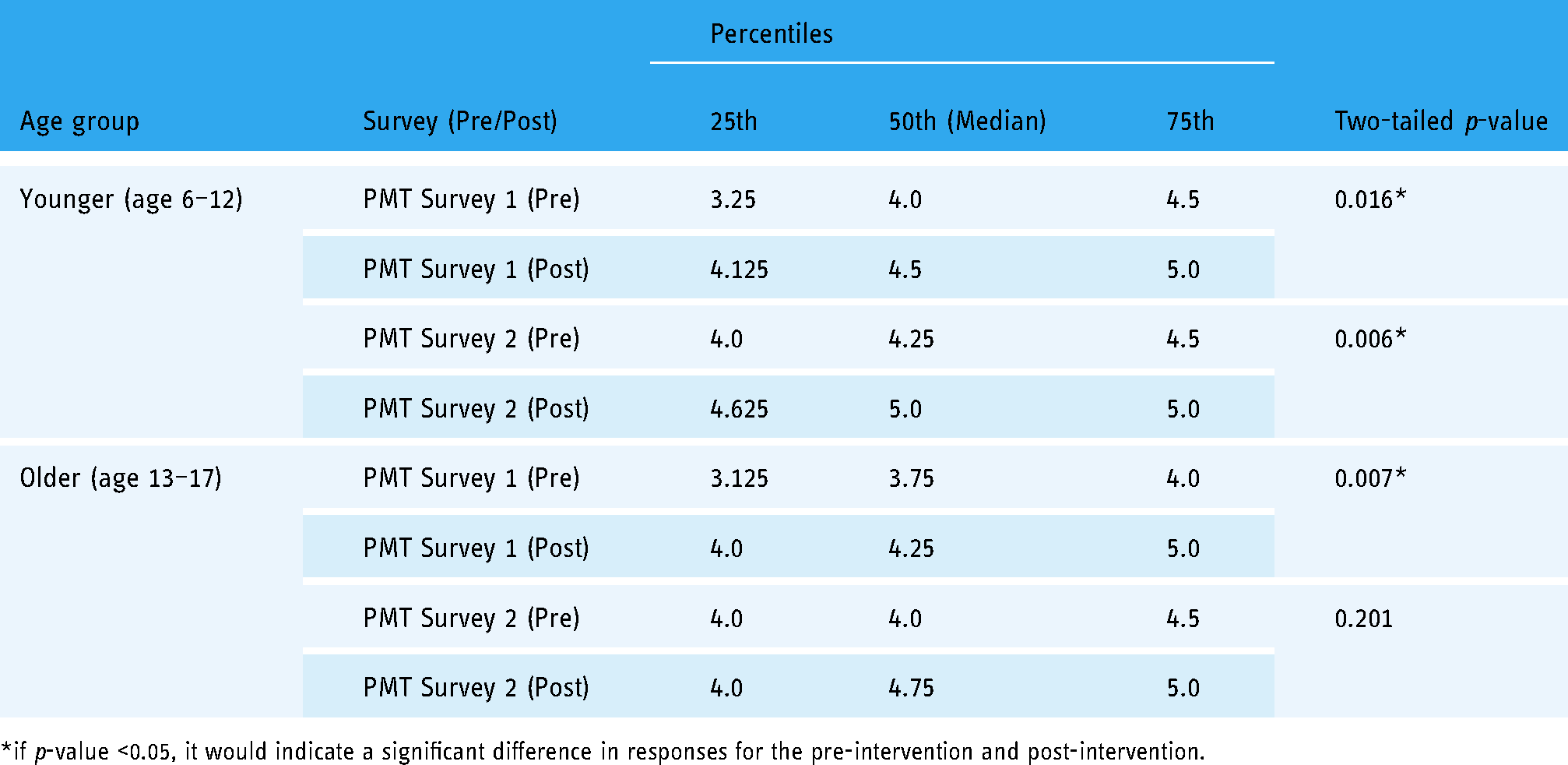
*if p-value <0.05, it would indicate a significant difference in responses for the pre-intervention and post-intervention.
The tests were repeated with the participants divided into two age groups, younger children (age 6–12) and older children (age 13–17) (Table 6). In PMT Survey 1, both the younger (p = 0.016) and older (p = 0.006) children groups had a significant increase in the intention scores to use cancer treatment to fight cancer. This indicated that the evidence is strong enough (p < 0.05) to suggest that for both younger and older age groups, the game had an effect on the participants’ motivation to keep up with their cancer treatment.
In PMT Survey 2, the younger children group showed a significant increase in intention scores for using daily self-care to manage treatment side effects (p = 0.007). For the older children group, there was a non-significant increase in the scores (p = 0.201).
This indicated that the evidence is strong enough (p < 0.05) to suggest that for the younger children, the game had an effect on the participants’ motivation to perform daily self-care to manage their cancer treatment side effects. However, although there was an overall increase in the results for the older children, the evidence was not strong enough (p > 0.05) to suggest that the game had an effect on improving their motivation to perform daily self-care.
Cancer Knowledge Survey
The results from the Cancer Knowledge Survey consist of descriptive statistics and hypothesis testing.
Descriptive statistics
The Cancer Knowledge Survey was treated as a test to indicate the level of participants’ knowledge. The results for the pre-intervention surveys and the post-intervention survey scores for all participants (n = 24), the younger children (age 6–12) age group (n = 12) and the older children (age 13–17) age group (n = 12) are summarised in Table 7.
Summary of Cancer Knowledge Survey pre-test and post-test results for all, younger, and older age groups.

During the pre-intervention Cancer Knowledge Survey, the minimum score was 7/20 (35%), while the maximum score was 18/20 (90%). Additionally, the median score was 14/20 (70%).
For the post-intervention Cancer Knowledge Survey, the minimum score was 8/20 (40%), while the maximum score was 20/20 (100%). The median score was 15.5/20 (77.5%).
The results indicated an improvement in overall scores for participants during the post-test for the majority of the participants.
Hypothesis testing
Before conducting the hypothesis testing, the data was first observed for outliers. It was decided that the Wilcoxon signed-rank test would be conducted on the dataset, excluding the data from Participant 4 (pre-test taken in Bahasa Melayu, post-test taken in English) and Participant 18 (completed post-test in 1 min, with the average time being 5 min). The Wilcoxon signed-rank tests were carried out with all participants (n = 22) and also for the younger children (age 6–12) age group (n = 11) and the older children (age 13–17) age group (n = 11) (Table 8).
Wilcoxon signed-rank test results for pre-intervention and post-intervention Cancer Knowledge Survey scores for all, younger, and older age groups.

*if p-value <0.05, it would indicate a significant difference in responses for the pre-intervention and post-intervention.
There was no significant increase in the scores for the pre-intervention results for all participants (Median = 14.0) and the post-intervention results (Median = 16.0); p = 0.081.
There was also no significant increase in the scores for the younger children with the pre-intervention results (Median = 15.0) and the post-intervention results (Median = 16.0); p = 0.751.
However, for the older children, there was a significant increase in the scores for the pre-intervention results (Median = 12.0) and the post-intervention results (Median = 16.0); p = 0.024.
Based on the scores, these results indicated that after playing the serious game, there was an overall improvement in participants’ knowledge of childhood cancer and cancer treatment. Although this increase in score was more evident for the older children age group, indicating that they were more likely to benefit from this game in terms of education.
Feedback and follow-up responses
All 24 pairs of child/caregiver dyads provided their feedback on the game intervention. For the voluntary feedback follow-up sessions, only 16 (66.67%) caregivers agreed to answer the follow-up questions.
According to all 24 caregivers (100%) who responded to the feedback survey, Pets vs Onco was useful and helpful for children with cancer and beneficial to their children.
Additionally, all of the caregivers who agreed to the feedback follow-up (n = 16) said they detected positive changes in their children after they had played the game. All caregivers (n = 16) agreed that the game motivated their children to keep up with therapy and practise daily self-care. All caregivers (n = 16) also agreed that the game had improved their children's knowledge of cancer and treatment. Lastly, the majority (n = 15) of caregivers agreed that the game had encouraged them and their children to talk about cancer. One caregiver who disagreed with this statement deemed her child (aged 6) too young to engage in conversations about cancer.
Caregivers’ qualitative feedback from the follow-up responses are in line with the feedback survey.
Benefits of Pets vs Onco
According to most caregivers, the game had taught their children to better understand their illness and treatment. Caregivers commented that they liked the game as it is educational; this may indicate that children enjoy the game as it is a fun way to learn more about cancer and treatment, especially through the quiz mini-game. The game was also found to be educational for caregivers who played it with their children. My son is diligent in reading information related to cancer in the game, so he follows the advice from the information there, and uses it in daily life. P9's (Age 14, Male / 14M) Caregiver
Besides educating about cancer treatment, the game was also said to be motivational. Caregivers have reported that their children were more enthusiastic about following their cancer treatment after playing the game. As the children become more motivated about their cancer treatment, some have even become more interested in their treatment progress. When he's done all the chemo… he asked the doctor about progress, about how he is doing now. The doctor said it's ok, all is well. P16's (13M) Caregiver
From the caregivers’ responses, the game helped open up conversations about cancer as the children became more willing to share their experiences with others. He does share about treatment and what he felt during the treatment… Previously, he didn't tell me anything. P17's (10M) Caregiver
Caregivers also mentioned that the pet serves as a good role model for daily self-care, especially for younger children. Additional benefits highlighted include the alarm module being used as reminders for treatment and daily self-care and that the game teaches problem-solving skills. If the child takes the pet as a role model together with the different scenes, it will increase his confidence and help him understand (the importance of daily self-care). P24's (6M) Caregiver
Children were found to be more motivated to perform daily self-care and more punctual and self-disciplined for activities such as taking medication and other daily self-care. Several caregivers have shared that their children, who usually needed to be told when to perform daily self-care activities, became more independent about it after playing the game. He is more receptive to the idea of “taking care of one's health” and is less resistant when I remind him to take medicine and drink water… P24's (6M) Caregiver
Additionally, children have shared that they liked the game as it reminded them about the importance of taking care of their health. …she can remember when she needs to eat, drink milk and take medicine. P2's (11F) Caregiver
As the pet serves as a role model for the effects of selecting healthy food and drinks. The game's educational value was evident in the better food and beverage choices that the children make. He used to want to bring sweet drinks to school. But now he prefers to bring plain water… He prefers to eat healthy food now. (He understands that) if he eats unhealthy food, his cancer may recur. P14's (12M) Caregiver
We found that children with cancer were curious to learn more about their sickness, and some children miss their pet, which the virtual pet reminded them of. Furthermore, one participant was so engrossed in playing the game that she had difficulty putting it down, another participant began to want to dress better after playing the game, one caregiver stated that the game was full of love, and another caregiver stated that their child was already proactive about daily self-care even before being diagnosed with cancer. The game was found to be fun and able to cheer up children with cancer. The game was also found to help in improving children's outlook, attitude or behaviour. Children had become more proactive, positive and understanding about the importance of taking care of one's health. (The game) taught my child the meaning of a better life despite having cancer and to work harder to heal and become stronger. P5's (16M) Caregiver
Children also used the game as entertainment to pass the time, for example, during treatment. Additionally, the game provided stress relief for the children and also taught them about basic pet care. This game can relieve the feeling of stress for me. P10 (10M)
Game rating
To determine how much the children enjoyed Pets vs Onco, they were asked to assign the game a rating from 1 to 5 stars, where 1-star indicates ‘strongly dislike’, 2-stars indicate ‘dislike’, 3-stars indicate ‘feeling neutral’, 4-stars indicate ‘like’ and 5-stars indicate ‘strongly like’.
The majority of participants enjoyed the game (Mean = 4.125, SD = 0.958). When divided by age, younger children (age 6–12, n = 12), (M = 4.357, SD = 0.644) had rated the game a little higher than the older children (age 13–17, n = 12), (M = 3.875, SD = 1.170). Male participants (n = 15) rated the game 4.100(±1.039), while female participants (n = 9) rated it 4.167(±0.866). This indicates that in this sample, gender has little impact on the game's rating in this sample.
Likes and dislikes
When children and caregivers were asked what they liked about Pets vs Onco, we received the following reasons. Many caregivers listed that they liked the game as it was beneficial to their children. This game is very beneficial for children with cancer because they can learn a lot from this game, they can take care of their health, take care of nutrition and learn more about cancer. P9's (14M) Caregiver
For some children, they liked the game's graphics and the pet character. Additionally, whether in the form of a virtual playmate or a pet to take care of, it can be seen that children and caregivers liked the virtual pet game as it was able to provide a sense of company to children with cancer who were undergoing treatment at the hospital. This game can make my son happy. (He is) able to give attention to pets even if they are just digital animals. P14's (12M) Caregiver
Other likes include using the game to fight cancer virtually by fighting the enemy cancer cells within the game. I love this game to treat cancer and to fight cancer. P3 (13M)
Additionally, other children commented that they liked the game as it was easy to play, that it reminded them of a popular mobile game, and that the diary module gave them a place to express themselves.
On the other hand, feedback was also gathered on what was disliked about the game. Although the game can be fun at first, some caregivers and children found that the game would lose appeal later. This was especially true in the case of older children. Similarly, some children, especially older children found the game to be not interesting or challenging enough due to lack of content. Since he's in his teens, this game was not challenging for him… The children over 12 years old may be less interested in playing this game because there are other games that are more challenging. P11's (12M) Caregiver
Feedback showed that the content of the game can be difficult to understand for younger children. Caregivers had to guide those who were not fluent in reading while they play.
Additionally, one participant found the waiting time to restore the pet's energy by sleeping to keep playing to be too long. However, no other children have commented on the long waiting time for restoring energy. This resting period was also added to encourage moderation in playing the game, which the child could use to rest themselves between playtimes.
Lastly, there was one complaint about lag while playing the game; this may be due to the participant's phone being too low on memory to play the game smoothly.
Caregivers have agreed that Pets vs Onco still has room for improvement. To address the game's losing appeal over time, more content should be added. Children who played consistently each day would be close to completing all the game content by one month. Just need to improve (the selections) for accessories, eating, drinking… Add more activities that can be done with the pet… P10's (10M) Caregiver
On the other hand, the inclusion of more mini-games was also a popular suggestion by both children and caregivers. It was suggested that mind-challenging mini-games would attract the interest of older children.
Other suggestions include reducing the use of difficult words to aid younger children's understanding and including sounds for the pet.
Appendix 1 lists the main themes, sub-themes, frequencies in which they were mentioned and example quotes.
Discussion
The study's main aim was to evaluate a PMT-based digital health intervention, Pets vs Onco, designed for children with cancer, which can encourage them to adhere to their treatment, encourage daily self-care and educate them about cancer and treatment.
The survey data collected from this study was evaluated via quantitative analysis, while the caregiver and children's feedback was analysed thematically.
The maximum score for intentions is five, as the surveys utilize a Likert scale of 1 to 5. Results from the quantitative analysis of PMT Survey 1 indicated a significant rise in the intention scores of participants to use cancer treatment to fight cancer during the post-test (pre-test Median = 4.00, post-test Median = 5.0, p-value = 0.0003, p < 0.05). This supports the first hypothesis of this study (H1) that after playing the PMT-based virtual pet serious game, childhood cancer patients will have more intention to adhere to their treatment plans to fight cancer.
This result aligns with the results of Re-Mission 63 where the game had improved treatment adherence in adolescent and young adult cancer patients. Re-Mission and Pets vs Onco allowed the players to virtually fight cancer, empowering them to fight the disease. This improvement in treatment adherence can be explained by the PMT, 44 which indicates when a person's belief in the efficacy of a health behaviour increases, they will become more likely to use it against a health threat.
Similarly, based on PMT Survey 2, the participants’ intention to use daily self-care to manage treatment side effects had also improved (pre-test Median = 4.0, post-test Median = 4.5), p-value = 0.006, p < 0.05). The result supports the second hypothesis of this study (H2) that after playing a PMT-based virtual pet serious game, childhood cancer patients will have a greater intention to perform daily self-care to manage treatment side effects.
This result matches that of Wizdy Pets 39 where children with asthma became more aware of their own needs and how to take care of them. Both Wizdy Pets and Pets vs Onco showed the importance of certain health behaviours to their players through taking care of a virtual pet, and demonstrating the effects good health care would have on the pet. This corresponds to the Social Learning Theory 42 which hypothesizes that people can learn good health behaviours through role models in a game. Additionally, taking care of virtual pets can boost the players’ confidence in taking care of themselves.
The improvement in the motivation of children to perform daily self-care can be explained by the PMT 44 as well. As a person's belief in the effectiveness or response efficacy of a health behaviour increases, so will their intention to use it to improve their health. Also, as a person's belief in their self-efficacy or confidence in their ability to carry out a health behaviour increases, their intention to do so will also increase.
Additional tests were conducted to test the hypotheses for participants based on their age group. It was found that the game improved the motivation of younger children (age 6–12) to undergo cancer treatment and perform daily self-care. However, for older children (age 13–17), a significant increase in motivation was found only for using cancer treatment to fight cancer, but not for performing daily self-care. This may be because younger children are more likely to see the pet as a role model for daily self-care, as depicted in the caregiver feedback.
The participants’ knowledge levels of basic cancer and treatment-related facts were also evaluated pre-test and post-test. As two participants did not properly fill the 20-question multiple-choice quiz, their data were excluded from the analysis. Results showed that there was a non-significant improvement in scores for the majority of the participants post-test (pre-test Median = 14.0, post-test Median = 16.0, p-value = 0.0081, p > 0.05). When the tests were repeated for the results of younger children (age 6–12), there was also no strong evidence for improvements. However, for the older children (age 13–17), significant improvements in scores were found (pre-test Median = 12.0, post-test Median = 16.0, p-value = 0.024, p < 0.05). The findings support the third and final hypothesis of this study (H3), which states that after playing a PMT-based virtual pet serious game, childhood cancer patients will become more knowledgeable about childhood cancer and cancer treatment. However, older children showed more improvement. This could be because some younger children may find the educational content of the game difficult to understand, as shared in the children's and caregivers’ feedback.
These findings also show that as the knowledge levels of the children regarding their illness and treatment methods improve, so does their treatment adherence. This aligns with the finding that age-appropriate information can help children and adolescent cancer patients to cope with the cancer experience,25,26 and also with the findings that patients who were more knowledgeable about their illness were more compliant with their treatment.27,28 Furthermore, results from some games for cancer patients showed that it is possible to learn about cancer and treatment through games, such as in Re-Mission, 63 FightHPV, 64 and ILOVEBREAST 65 .
From the analysis, we found all PMT factors had low degrees of correlation toward the intention to use cancer treatment. Out of the seven factors, the three factors with significant levels of correlation with intention are threat severity (positive), intrinsic rewards (negative) and response efficacy (positive). This indicates that the higher the threat severity of cancer, the lower the intrinsic rewards such as believing that they would feel happier for not undergoing cancer treatment, or the higher the response efficacy of using cancer treatment, the higher the participants’ intentions of using cancer treatment.
This matches with the PMT, 44 which theorizes that when a person's perceived threat severity and response efficacy are high, along with low intrinsic rewards, it would increase their intention to take up a health behaviour to combat a health threat. For this sample, the children viewed cancer as a strong threat, had low intrinsic that would have encouraged them to not use cancer treatment and viewed the response efficacy of using cancer treatment as high and effective. This indicates that both the threat appraisal, which includes the PMT factors of threat severity, intrinsic rewards and extrinsic rewards and the coping appraisal which includes the PMT factor of response efficacy play a role in encouraging the use of cancer treatment.
Besides that, the correlation analysis results suggest significant, moderate degrees of correlation between response efficacy (positive), self-efficacy (positive) and intention on utilizing daily self-care to control treatment side effects. An additional PMT factor that had significant levels of correlation with the intention is the threat vulnerability (low, positive). This means that if the response efficacy of the positive effects of using daily self-care is high, or the self-efficacy or belief in one's ability to perform daily self-care is high, or the threat vulnerability of having treatment-related side effects is high, the intention to perform daily self-care to manage the side effects is likely to be high as well.
This corresponds with the PMT, 44 which theorizes that when a person's perceived threat vulnerability, perceived response efficacy and self-efficacy are high, it would increase their intention to take up a health behaviour to combat a health threat. For this sample, the children who believe that they have high vulnerability to experiencing cancer treatment side effects viewed the use of daily self-care as an effective way to manage the side effects and also believed in their self-efficacy to perform these daily self-care activities. This indicates that both the threat appraisal, which includes the PMT factors of threat severity, intrinsic rewards and extrinsic rewards, and the coping appraisal, which includes the PMT factor of response efficacy, play a role in encouraging the use of daily self-care.
According to the thematic analysis of the caregivers’ and children's feedback regarding Pets vs Onco, the virtual pet game positively impacted children with cancer. Qualitative feedback from caregivers indicated that the children had become more motivated for cancer treatment and daily self-care, in addition to learning about their illness and treatment through playing the game. The children became more eager to undergo cancer treatment and were keener about knowing more about their treatment plans and progress, and were also more self-disciplined and punctual about their daily self-care. The benefits depicted are in line with the results of the quantitative analysis and is supportive of the three hypotheses of this study which theorized that the game can increase childhood cancer patients’ intention to adhere to their treatment plans to fight cancer (H1), increase childhood cancer patients’ intention to perform daily self-care to manage treatment side effects (H2) and educate childhood cancer patients about their illness and treatment (H3).
Feedback showed that the game was well accepted, with an average rating of M = 4.125 out of 5 stars by the 24 children. When divided by age, young children (M = 4.357) rated the game higher than older children (M = 3.875). This could imply that the game is better suited for younger children and that more content is needed to appeal to older players. This is in line with the findings of the thematic analysis, where it was highlighted that the game is not challenging enough, especially for older children. Both children and caregivers liked the game for various reasons, including providing various benefits to children with cancer, such as cheering them up, opening up communication about cancer, and providing the children with a virtual companion.
However, the game was not without weaknesses and would require improvements to enhance the overall appeal of the game. Suggestions for improvements include having more content such as new items to interact with the pet, for example, new clothes, new kinds of food and drink, more activities to do with the pet, a storyline, the depiction of exercise and additional mini-games. The game can also be more suitable for the wide age range of 6–17 years old by having two versions of the educational content. One version would be written for younger children's reading levels, while the other would be for adolescents.
Conclusions
In conclusion, both children with cancer and their caregivers, in general, enjoyed Pets vs Onco. The findings suggest that childhood cancer patients became more motivated to adhere to their cancer treatment after playing the game. The game also showed potential in encouraging childhood cancer patients to practise daily self-care, especially for younger children. In addition, the study's findings revealed that the game was educational, particularly for older children. Furthermore, both the children and caregivers in the study agreed that the game provides various benefits to children with cancer. These results align with the preliminary findings of the pilot study 47 conducted with a smaller sample of children, which indicated the intervention's potential to support childhood cancer patients.
This study has several limitations. Due to the difficulty in finding enough children with cancer to participate, it was determined that everyone would be assigned to the intervention group to obtain more data. However, this study used a pre-test–post-test methodology, allowing the post-test survey responses to be compared to the pre-test survey results obtained before the participants had played the game. Participants and their families that are recruited from the boarding homes of the two cancer organizations are mostly from low-income families who require financial assistance. Furthermore, although Malaysia consists of multiple races such as Malays, Chinese and Indians, 66 most of the research participants and their families are Malays or Indigenous people. Due to a lack of diversity, we could not generalize the findings to a larger group of children with cancer. Because of the pandemic, this study could not be conducted in person with childhood cancer patients vulnerable to contracting the virus. While the digital surveys and online contact allowed for safety, contacting caregivers for the study can be challenging, resulting in some data collection delays.
Future work should address the study's limitations by having a control group and recruiting from more locations to expand the sample size, diversify the sample and generalize the findings to a broader population of children with cancer. Firstly, future research should increase the sample size and diversity of the participants to generalize the findings to a broader population of children with cancer. This can be accomplished by evaluating the game on a larger scale with other collaborators over a longer recruitment period, as well as by recruiting people from different socioeconomic backgrounds and races. Future research should also include a control group, whether a waitlist control group or allowing control group participants to play a commercially available game similar to a serious game. By using a control group, the researchers can establish that the study outcomes are due to the manipulation of independent variables rather than extraneous variables. Additionally, surveys should be performed face to face wherever possible to allow for smoother data collection and more consistency in survey-filling methods. Face-to-face surveys would also allow the researchers to provide extra guidance to the children while they fill in the surveys.
Besides that, the game prototype can be improved based on the feedback participants and their caregivers provided in this study. Finally, the game is found to be beneficial to children with cancer, based on the results of this study; the file can be made freely available and distributed to hospitals and cancer organizations so that children and adolescents with cancer can play it once an improved version of the game has been developed.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the children and families from Sarawak Children's Cancer Society (SCCS) and the National Cancer Society Malaysia (NCSM) who took part in this study. We also want to express our gratitude to the amazing individuals at SCCS and NCSM for their assistance with the recruitment process.
Conflict of interest
The authors have no conflicts of interest to declare.
Contributorship
CCWE, LBT, MTKT, and AA researched literature, conceived the study, developed the protocol and gained ethical approval. CCWE oversaw participant recruitment and wrote the first draft of the manuscript. All authors were involved in data analysis, reviewed and edited the manuscript, and approved the final version of the manuscript.
Ethical approval
This work was approved by the Swinburne Human Research Ethics Committee (SUHREC) (Ref: 20202689–3990).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swinburne Sarawak HDR scholarship.
Guarantor
CCWE
Appendix 1. Thematic analysis evidence and quotes for each sub-theme
Participants in this section will be referred to by their participant number to maintain their anonymity. For example, Participant 1 or P1 for short.
The game teaches about cancer and/or treatment
33
More motivation for treatment
19
More motivation for daily self-care
24
The game teaches about daily self-care
11
Becoming more punctual/self-disciplined (about daily self-care & medication, or in general)
9
The game cheers child up
19
The game opens conversation about illness
15
Improving the child's outlook, attitude or behaviour
11
The game helps to pass the time (during treatment and in general)
9
Playing the game eases stress (from illness and other stressors)
7
The child learns how to take care of a pet
3
The pet is a good role model for daily self-care
3
Alarm helps to remind for treatment and daily self-care
2
The game teaches problem-solving skills
2
The game can be beneficial for children with cancer
13
The game has attractive graphics/ character
4
The child enjoys taking care of the pet
4
The game is easy to play
4
The game provides a virtual playmate
3
The child enjoys virtually treating and fighting cancer
3
The game reminds the child of a popular mobile game
1
The child likes writing in the diary
1
The game is not interesting/challenging enough (lacking content)
8
The game is boring or gets boring later
6
The game is difficult to understand for younger children
3
Waiting time for pet to sleep for energy is too long
2
The game lags or delays
1
Improve the game by adding more content
8
Improve the game by having more mini games
6
Other suggestions for improvement
6
The child is curious about cancer and treatment-related information
2
The child misses having a pet
2
The child had problems putting the game down
1
The child wants to dress better now
1
The game is full of love
1
The child is proactive about daily self-care even before having cancer
1
Parents of young children with cancer do not talk to them about cancer
1