
Abstract
Objective
To explore the feasibility of a randomised controlled trial of a multiple sclerosis online course (MSOC) via qualitative analysis of participant semi-structured interviews.
Methods
The MSOC was developed in two arms: intervention arm which contained evidence-based lifestyle modification recommendations, and standard-care arm which delivered information from MS websites reflecting standard advice. Participants were recruited via online advertisements, completed a baseline questionnaire, and randomised. Seven modules were delivered over six weeks. Course completers were invited to participate in semi-structured interviews. Within a qualitative paradigm, interviews were analysed using reflexive thematic analysis.
Results
Fourteen of the 17 course completers were interviewed: 86% (12/14) female; mean age 50 years; residing in Australia, New Zealand, and the USA, predominantly had relapsing-remitting MS, mean time from diagnosis 9.5 years, and patient-determined disease steps disability assessment distributed evenly across all three categories. Four themes were identified: 1) “Hearing our stories” (hope for the future, feeling represented, exploring the journey of others with MS, learning from diversity, and wanting to connect with others); 2) “Taking the plunge” (not wanting to be first, feelings of nervousness or reluctance and feeling confronted); 3) “The accessibility and safety of being online” (ease of access, going at your own pace, making it work and not letting others down); and 4) “unpacking the course” (ease of navigation, visuals, understandability, and length and timing).
Conclusion
Participants felt represented, found the course accessible and content was easy to understand. These experiences provide important insights and considerations for this digital health intervention.
Keywords
Introduction
MS is a chronic autoimmune disorder of the central nervous system characterised by demyelination that can lead to physical and cognitive disability. 1 It is estimated that there are almost 3 million people with MS (pwMS) globally, 2 and a combination of genetic and lifestyle factors are hypothesised to contribute to its pathogenesis.3,4 MS management involves a coordinated approach to managing symptoms, relapses, and disease progression, which primarily occurs through the use of pharmacological disease-modifying therapies (DMTs). 5 Despite the acceptance of DMTs and their effectiveness, pwMS have demonstrated a desire for greater access to self-management programs that use lifestyle modification to manage known risk factors for disease progression. 6
One such lifestyle modification program has been delivered face-to-face internationally as a five-day residential workshop to pwMS over many years and accumulated an evidence-base for improving health outcomes. 7 This educational program has been associated with improved health-related quality of life up to 5 years post-attendance 8 and reduced relapse rate three years post-attendance. 9 Importantly, pwMS attending these workshops found the lifestyle modifications both feasible and sustainable. 9 However, there are multiple barriers for attendance at face-to-face workshops including cost, time, resource limitations, accessibility, and potentially MS-specific issues such as cognitive impairment and disability.
The multiple sclerosis online course (MSOC) was developed by researchers, in conjunction with pwMS, to transform the face-to-face educational lifestyle program into a digital health intervention (DHI). The process of digitalising the face-to-face educational lifestyle program is a means to overcome access barriers identified with the physical mode of delivery for pwMS. The feasibility of the MSOC was then evaluated in a small randomised controlled trial (RCT), the MSOC-feasibility RCT, using both quantitative and qualitative methods, to determine the acceptability of the MSOC in a representative sample of pwMS. Acceptability is a key concept for DHIs as it mediates a user's engagement with a program. 10 Engagement is similarly vital in that it facilitates the acquisition of knowledge and learning of skills that aid in the behaviour change necessary for improving health outcomes. 11
The results of this MSOC-feasibility RCT will inform redevelopment of the course, with the ultimate aim being to deliver the MSOC to a larger audience of pwMS to facilitate effectiveness testing with respect to improved health outcomes through behavioural change. The aim of this study was to explore the acceptability of the MSOC using qualitative methods, which allow for the exploration of the perspectives of participants 12 and provides an in-depth exploration of the depth and breadth of experience with the MSOC in an international sample of pwMS.
Methods
Ethical approval and informed consent
This study was approved by The University of Melbourne Human Research Ethics subcommittee (ID: 1851781.2). Written informed consent was obtained from all participants prior to inclusion.
Study design
The MSOC-feasibility RCT study design and course contents have been previously and comprehensively described 13 ; however, briefly, this study was run over six weeks from April 2021 to June 2021. Participants were recruited online via MS societies in the USA, Canada, and New Zealand, and a peer-support Facebook group for pwMS in Australia. Consenting participants completed a screening questionnaire within the study website to confirm eligibility: a diagnosis of MS confirmed by a physician; at least 18 years of age; living in Australia, Canada, United States, New Zealand, or the United Kingdom; fluent in English. A baseline survey consisting of questions on sociodemographics, lifestyle habits, and health status was sent to eligible participants after completing this screening (Figure 1).

Consort flow diagram of study participants.
Intervention and standard-care courses
Participants were randomised to either an intervention course or a standard-care course using a computer-generated randomisation sequence implemented within the course website. These courses were codesigned with four pwMS from Victoria, Australia, while the research team also drew on behaviour change intervention design frameworks such as the Behaviour Change Wheel 11 and the Theoretical Domains Framework. 14 Both courses contained seven modules, which followed the format of introduction, diet, vitamin D, physical activity, stress reduction, family and prevention, and a concluding module. Content in the intervention arm was adapted from an evidence-based lifestyle modification program for pwMS, The Overcoming Ms program, 15 previously presented in a face-to-face format. Specifically, the content included an introduction to pathophysiology of MS followed by the evidence underpinning the lifestyle recommendations: dietary modification to a plant-based whole food diet plus seafood with omega 3 polyunsaturated fatty acid supplementation; physical activity 20–30 min approximately five times per week suited to ability; vitamin D supplementation; stress reduction via meditation; education regarding prevention in family members, smoking cessation, and alcohol moderation; and concluding remarks. Content in the standard-care arm mirrored the intervention course with respect to module topics but the content was sourced entirely from MS society websites in the public domain. These domains were Multiple Sclerosis Australia, Multiple Sclerosis Research Australia, National MS Society, Multiple Sclerosis Society UK, Multiple Sclerosis Society of Canada, and the choice of content was designed to reflect the standard information provided by heath care practitioners and MS societies.
Modules contained text, video, images, and interactive quizzes related to the topic at hand, with progress bars included within the modules to ensure participants knew at what point in the module they were at. There was forum access for participants with each course having its own, isolated forum for asking questions or responding to other questions. Participants were able to build a profile of themselves including photo, bio, and social media links if they desired. Two presenters, researchers GJ and SN, introduced and concluded every module with a video, discussing the module outlined within both courses. In particular, one of the presenters with MS (GJ) specifically discussed what to expect from having MS and described his personal experiences of incorporating the content of individual modules into his daily life. Modules were released sequentially twice per week, Monday and Thursday 12AM AEST, and participants were required to complete each module before advancing to the next. After the final module was released in week 4, further two weeks were allowed to complete outstanding modules.
Qualitative recruitment
Participants were invited to participate in a semi-structured interview if they had fully completed either the intervention or standard-care course. The possibility of an invitation to participate in an interview post-study period was outlined in the study consent form and plain language statement, and therefore, participants were prepared to be contacted once more. Participants were emailed an invitation to participate in the semi-structured interview, which outlined the time commitment and process that would take place during this interview. For participants that did not respond by email to this invitation, a follow-up phone call was made. Of the nine participants who completed the intervention course and eight who completed the standard-care course, 8 and 6, respectively, agreed to participate in a semi-structured interview (Figure 1). One participant declined the email invitation to participate and two did not respond to any contact attempts.
The interviewers
Interviews were conducted by SN, JR, and PJ, with clinical and epidemiological backgrounds. SN was involved with the design and development of the MSOC and has extensive clinical and qualitative interviewing and research experience. PJ is a general practitioner with experience in clinical interviewing, and JR is a public health researcher. All three researchers had access to the course materials and were not blinded to which course the participants had been randomised, so that they could understand participants’ views on content.
The interview
The interview questions were developed by WB, SN, PJ, and JR to explore participants’ expectations and experiences with the course to ultimately assess feasibility. Interviews were conducted via telephone or videoconference. The first three interviews were conducted with a lead interviewer and two observers, with the permission of the interviewee, for interviewers to assess the interview schedule and to assist consistency in the approach between interviewers. Following the first three interviews, the interview schedule was minimally revised, based on researcher observations, to reduce repetition. Further interviews were then conducted with one or two interviewers depending on the availability of researchers. Interviews were digitally recorded and transcribed verbatim by voice recognition software (temi.com). 16 Interview transcripts were subsequently edited by the interviewers while concurrently listening to audio recordings to correct transcription errors produced by the software. These transcripts were then imported into NVivo software for data management. NVivo software outputs were maintained, along with researcher meeting memos, to document coding development and theme evolution. 17
Acceptability
For this study, feasibility is assessed in terms of acceptability according to the domains: learnability, desirability, and accessibility. These indicators of feasibility have been used previously to explore the feasibility of mobile and web-based self-management intervention in a population of outpatients with cancer pain. 18 Learnability refers to how easy it was for participants to learn how to navigate the course; accessibility refers to the ease of participant interaction with the course, specific to their physical or cognitive ability; desirability refers to the enjoyment participants derived from the course and its components. These domains are not explicitly queried, they informed the development of questions and broadly guided interviewers during the interviews.
Qualitative analysis
Within a qualitative paradigm, interviews were analysed using reflexive thematic analysis, 19 a revised version of thematic analysis. This approach to analysis was chosen as it is an open-ended and flexible process that encourages depth of engagement and exploration while emphasising researcher subjectivity and reflexivity 20 and is appropriate for healthcare research. 21 Researchers acknowledged their depth of involvement in the project and their perspectives and the influence this may have had on their interpretations.
Immersion in the data was assisted by researcher data collection and listening to interview recordings while amending transcripts for accuracy. Initial codes were determined, and all data extracts were collated under the relevant codes (SN). The analysis team (SN, WB, PJ, and JR) met to examine the codes.
At this point, the entire dataset was divided into two data subsets as it was evident that the dataset contained two larger themes that required separate analyses. One data subset contained codes that related to course feasibility with respect to content, structure, and function, which formed this study. The other data subset contained codes related to participant motivations to undertake the course and their experiences of participation which fell outside the scope of this analysis. Data immersion, familiarisation, and re-coding were then undertaken on this dataset by WB. The research team met to identify broader patterns of meaning. An inductive approach was used, where initial themes were identified from within the data. The data were collated under each proposed theme and reviewed to ensure the themes reflected the data and contained a central organising concept. An iterative process of reviewing and renaming themes was undertaken before final themes were decided upon (Figure 2).
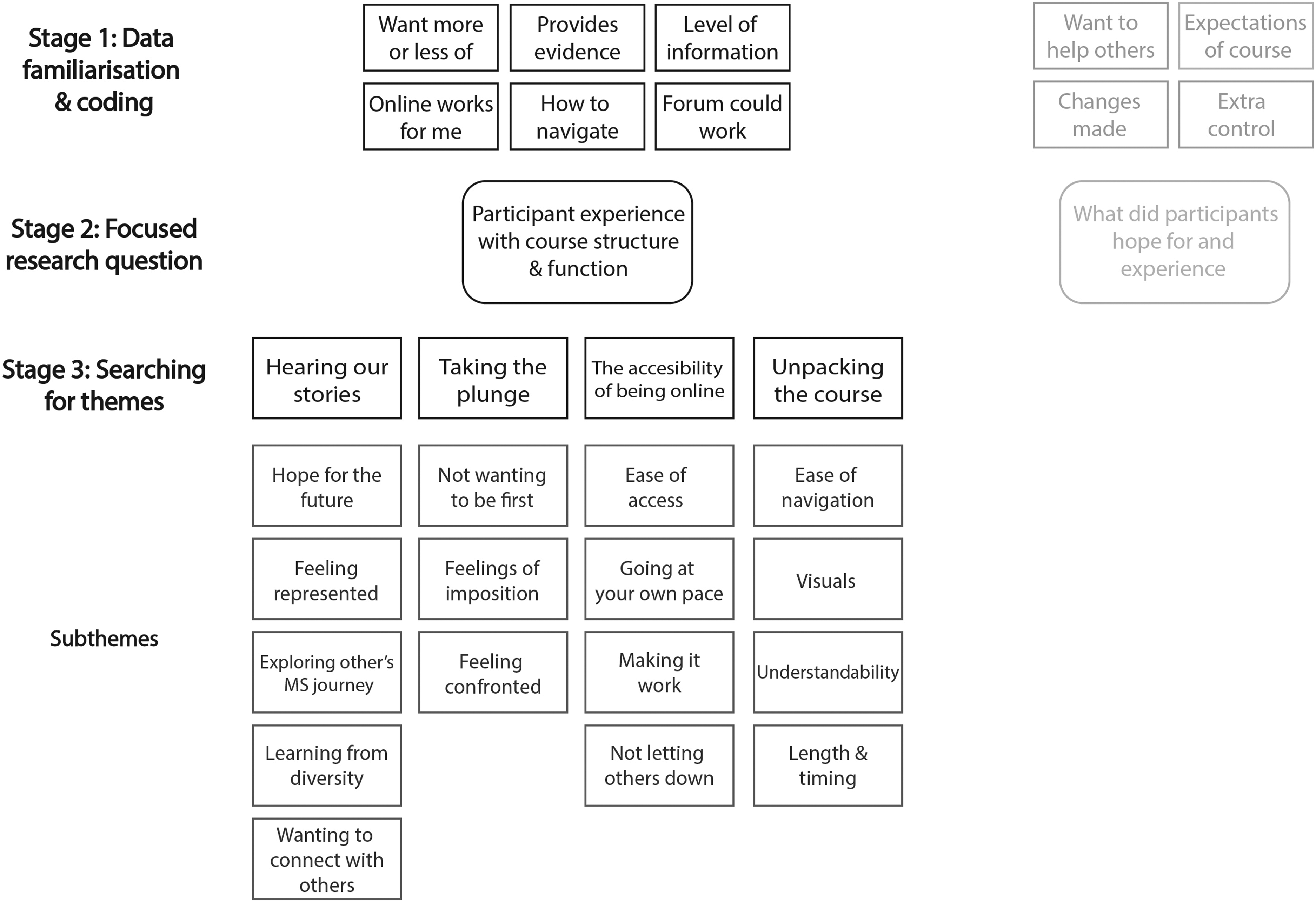
Thematic analysis development.
Verbatim data extracts to illustrate themes were chosen. Frequent rereading of transcripts, thematic development by multiple researchers, and researcher reflective discussions enhanced credibility. 22 Verbatim quotations are used to illustrate themes. Deletions of words that did not add meaning are indicated as “…”. Participants are indicated as intervention course participants “ICn” or standard-care course participants as “SCCn”. The COnsolidated criteria for Reporting Qualitative studies (COREQ): 32-item checklist was utilised. 23
Results
Participant characteristics
The mean age of participants was 49 and 51 years in the intervention arm and standard-care arm respectively. The majority in the intervention arm and standard-care arm were female (88% and 83%, respectively) and diagnosed with relapsing-remitting MS (75% and 67%, respectively). Fifty percent of participants in the intervention arm were from the USA, 38% New Zealand, and 13% Australia. In the standard-care arm, participants were from Australia (50%) or NZ (50%). Mean time since diagnosis was 8 years in the intervention arm and 11 years in the standard-care arm (Table 1). There were no significant differences in characteristics examined between the participants in the intervention and standard-care arms, nor between the qualitative participant cohort (N = 14) and the initially randomised cohort (N = 31).
Participant characteristics.

n: number; PDDS: patient-determined disease steps; SD: standard deviation.
Themes
There were four themes identified from the data: 1) “Hearing our stories” discussed the role of feeling represented within the course; 2) “Taking the plunge” explored participants” motivations or apprehension with engaging in the course; 3) “The accessibility and safety of being online” described participants’ preferences for an online course as well as their experience with this particular course; and 4) “Unpacking the course” explored the pros and cons of the course functionality across three broad groups: accessibility, usability, and enjoyability. From each theme, several subthemes were identified.
Hearing our stories
The theme “hearing our stories” contained subthemes of hope for the future; feeling represented; exploring the journey of others with MS; learning from diversity; and wanting to connect with others. The theme explored a central concept of the importance of representation within the course. Representation meant varying things to participants, including seeing themselves reflected in the presenters. This meant seeing and listening to presenters with MS within the course, including physicians, allied health professionals, or people from the general public who shared their experience with the disease. Further, it was seen as important to have information presented in a positive way, as opposed to the negative outlook many participants described they were frequently exposed to online and through their clinical experiences.
Hope for the future
Participants within the intervention arm described a more positive tone of this course compared with the information they have previously read online, which had been more fatalistic and emphasised long-term negative outcomes. It was more positive. Whereas a lot of the other stuff I’ve heard online is basically this is what you’ve got, and you’ll just get worse. (IC7)
It's always nice to hear other people saying, “that's the way you should be doing it” and not be negative about it just because you have MS. Not say “you need to just need to kind of lay there and just wait til your day comes.” (IC8)
One participant from the standard-care arm remarked that they were apprehensive about participating in the course as they had previously experienced negativity and wanted to filter information received to avoid an environment that emphasised negativity. I sort of don't necessarily want to put myself into that environment where I’m constantly reminded about disability and loss of function. (SCC6)
Feeling represented
Many participants across both arms described the importance of feeling represented by having presenters with MS within the course. Having this representation gave the course a relatable, credible feel whereby participants could see themselves in the stories described. It's nice to hear from someone who personally has experienced MS and then learn from their ways that they’ve dealt with the disease. I thought that that was very effective. (IC4)
It was good hearing from somebody who had experience with MS, you know, and that it's just not a doctor telling you this. (IC6)
One participant in the standard-care arm discussed the value of the authenticity of the people that were featured in videos. The videos of real people who you can relate to who know what you’re going through… I thought that was quite relatable and that was quite good. (SCC5)
A desire articulated within the standard-care arm was to see regionally appropriate representation. It would have been really nice to have videos that were actually New Zealanders or Australians talking about their lifestyle. (SCC6)
Exploring the journey of others with MS
The ability to create a public biography that described participants” life and story was seen positively by participants within the intervention arm but not mentioned by the standard-care arm. Intervention arm participants described enjoyment from being able to see and hear other people's experiences with MS. It's always interesting to hear someone else's story and how MS has affected them. (IC4)
You also got an idea of the range of their symptoms and their illness. (IC8)
It was noted that since there was no template, different people focused on different aspects of their lives when writing their profiles, adding variety and interest. Different people writing different things. So that part was good…that way I get to know a little bit about people. (IC7)
It was interesting because people talked about where they were from and there were people from all around the world. (IC8)
Learning from diversity
The opportunity to meet others with MS was a motivating factor for participation in the course for participants in both arms. Understanding how people from other countries dealt with MS, to see how their experience living with MS differed from their own, was important. I thought it might be a good opportunity to connect with other people with MS. (IC6)
I had never met anybody obviously from Australia or anywhere else besides the US with MS. And so, in some ways I wanted to ask, “was it any different having it over there?” (IC4)
Wanting to connect with others
Participants from both arms described wanting to communicate with their peers through the forum and expressed disappointment when that did not eventuate. I was like always ready to go on, but I was like, I’m not going to be the first to say, even if it was something little, I was really surprised that nobody had gone on. (IC8)
I was just a little disappointed that I couldn't interact more with the other course members. The forums could be valuable because you could find people who had similar problems and hear about their solutions. (IC4)
I guess what surprised me was that no one was involved in any of the community feedback on any of the modules. (SCC1)
Taking the plunge
Taking the plunge contained the subthemes of not wanting to be first; feelings of nervousness or reluctance and feeling confronted. Participants talked about feelings of nervousness and apprehension with respect to participating in some aspects of the course, in particular the peer-support aspects of the course, such as forums. The idea of “being the first” to engage in conversation or to ask a question appeared to be a barrier to participation for many, while the ease of access due to the course being online also meant less pressure to engage for some.
Not wanting to be the first
One common theme from both arms was wanting to participate but not wanting to be the first to comment in the forum. I almost did a couple of times just to sort of think maybe if I do, I’ll start it up. (IC7)
I think seeing maybe one other person start it up, I think back and I think, “oh, I should have just gone at it.” That was kind of silly trying to wait for somebody else to start something. (IC8)
Nobody likes to be the first person it's like speaking up first in class… Oh, I don't want to be the first dork. (SCC1)
Feelings of nervousness or reluctance
Participants in both arms described their reason for not participating being due to feeling nervous or like they have nothing to contribute to discussion. I just don't feel that I’ve got anything interesting enough to say. (SCC3)
I’m still kind of, a little bit of a shell myself, so it may have been an opportunity to engage more. (SCC5)
Others felt reluctant to engage as, after having MS for many years, they felt other participants would not have answers to their questions. I feel like I didn't really have any questions that I thought other people would have the answers to. (IC2)
Feeling confronted
Participants in the standard-care arm described a sentiment of feeling confronted by difficulties faced by others with MS; having to navigate one's own challenges living with MS was enough. I don't want to listen to other people saying, “Oh wo wo.” It's bad enough having to deal with it yourself. (SCC2)
When you’re first diagnosed, you’re already really vulnerable and when you’re reading about how hideous it's going to get it can be absolutely devastating. And so, the forum side of things this is good and bad. (SCC5)
The accessibility and safety of being online
The theme of accessibility and safety of being online contained subthemes of ease of access; going at your own pace; making it work; and not letting others down. This theme explored participants” views on delivering the course online compared with face-to-face, both the benefits and challenges. There were many factors identified by participants that influenced their ability to participate in an intervention. Importantly, the ramifications of the COVID-19 pandemic are mentioned by some with specific reference to the diagnosis and management of their MS.
Ease of access
Participants from both arms discussed a range of accessibility benefits to the course being taught online. For people who have mobility problems, it might be very difficult for them to get to an in-person event. So, I probably would prefer the online part of it. (IC4)
It's the availability and the sheer fact that because I’m in a wheelchair with only the use of my left hand, it made complete and utter sense to do it online. (SCC2)
Feeling comfortable in one's own home was important to people. The really good bits were the fact that I could do it from the comfort of my home and not go anywhere because I was so unwell. (SCC1)
Being able to do it in your own time and not having to go to a central point and just do it literally in your pyjamas at home. (SCC5)
One participant from the intervention arm mentioned the desire for the course to be made accessible through mobile devices. The only other thing is that I wish it was mobile friendly because I do feel like I would have preferred to just be laying on my couch. (IC2)
Going at your own pace
Participants within the intervention arm described that it was appealing to be able to stop and start the course when needed, which is not possible when delivered face-to-face. It was good to know that I could do it, press pause, take a break, go back. That was quite attractive to me. (IC7)
Those with work and family responsibilities found the online format especially useful. Obviously, it was convenient to be able to do it whenever you wanted. You didn't have to do it at a set time, so that suited my needs because I’ve got four children and a busy business and stuff like that. (IC6)
Making it work
Some participants from both arms described frustration behind having to complete a video or the technology did not recognise they had completed the video before progressing to the next stage of the course. You couldn't sort of pause [the videos] halfway through. You would have to watch the whole video in one setting or you couldn't progress. (SCC5)
I was watching the video, got to the end of it, went to click next, and the arrow to go to the next bit, and it wouldn't work. (IC3)
Another intervention arm participant described feeling forced to work through content that was not applicable to them and would have liked to have the option to skip parts of the course not relevant to them. I felt like I was having to watch a whole lot of slides about pregnancy when I’m not pregnant or plan on becoming pregnant anytime soon. (IC2)
Not letting others down
One participant from the standard-care arm described a feeling of potentially letting others down if they had committed to attending a face-to-face course and were suddenly unable to attend. If I had to attend a course and it was between certain hours, I’d feel very badly about letting other people down, signing up and committing to something, and not being able to fulfill that commitment. (SCC1)
The online course provided a way to ameliorate that feeling. I need a course like that, so if I was sick, I wouldn't be letting anyone down and I could work through it at my own pace. (SCC1)
Unpacking the course
Unpacking the course contained the subthemes of ease of navigation; visuals; understandability and length and timing. This theme explored participants” perceptions of which features of the course affected its accessibility, usability, and enjoyment. The ability to move through the course easily whilst understanding the important content was remarked upon, while some people talked about the visual style and presentation of the content itself. The length of the course itself was generally enjoyed by participants, and the frequency of module release was considered appropriate.
Ease of navigation
Participants from both arms described that navigating the course was straightforward. They knew what they were supposed to do and where they were within the modules of the course at any given moment. It was very simple, very straightforward. And you could see what stage you’re at all times. (IC1)
Once you started navigating your way around the technologies, it's quite clear, quite straight forward. (SCC2)
Some participants from both arms described their ability to use a computer in relation to their age/generation, and the implications of this in navigating an online course. I found as, you know, I CAN use a computer, but for me it was a little bit, um, confusing. (IC3)
Being of the just post baby boomer era, I’m not as computer savvy as others and navigating around the technology can cause issues, but it was quite straightforward. (SCC2)
Visuals
The ability to see material in the online course was raised by participants in both arms. Some related font size and other visuals as challenging issues for those with sight problems. Any of the stuff that I had to try to zoom in and read it where it was small print, I found it difficult personally. (SCC1)
When you’ve got issues with your eyes, it's really hard to read masses of information sent out to you. (IC7)
Understandability
Participants from the intervention arm described the level of course content as being at a comprehensible level that the majority of people would understand and expressed that this was a desirable feature. I feel like I could show my husband and be like, “this is actually what MS is” because it's really been hard to describe to other people. (IC2)
It might seem that you were talking to somebody in layman's terms; weren't talking to a medical person, which made it really good, and it made it easy to understand. (IC3)
Some from the standard-care arm also mentioned that the content was too basic and that having lived with MS for so long, they had heard all the information before. I have done a lot of reading and I’ve experienced a lot of it so I’m probably not the best person for an introductory course. (SCC2).
I thought that it would inform more about MS. I just thought it would give me some new information. And some new ways of understanding the disease. (SCC1)
Certain participants in the intervention course expressed they would have liked more information or information in greater depth across several topics. I just remember thinking I wish there was a little bit more about like the physical activity. (IC1)
I probably would love to have a little bit more information, now that I know about the diet stuff, that kind of thing. (IC6)
Length and timing
Some participants in the intervention arm described the modules as running shorter than they would have preferred and were seeking more information that might expand their knowledge further.
The modules in the course, I actually thought were a little bit short from my perspective. (IC4)
Others focused on the frequency of the modules and length of the course in its entirety. I don't know if I could have handled every day, but like twice a week. I think it's very fair. (IC2)
It was a good length in the sense that there wasn't too much in each one, and it wasn't too overwhelming because again, with illness and concentration and needing to go to the toilet and all those things, you don't want anything to be too long. (SCC1)
It was a very short and quite basic to what I thought it would be, but probably really, really good for people dealing with MS issues because you can't have concentration for long periods of time. (IC7)
Discussion
To date, no RCTs performed to test the feasibility of an educational lifestyle DHI for pwMS have included a qualitative analysis of participants’ experiences. Exploring participants’ experiences through thematic analysis complements qualitative data as thematic analysis captures implicit meaning beneath the surface, uniting data that at first sight might seems disparate. 24 The present study sought to fill this gap in the literature by examining the experiences of participants enrolled in the MSOC-feasibility study. Semi-structured interviewing of participants in both the intervention and standard-care arms revealed a wide range of experiences, both positive and negative, linked to peer support, relating to the presenters, and technical aspects of the course itself.
Our study provided critical insights into the desire for representation within DHI for pwMS. Participants clearly place importance on feeling represented by both presenters and within the course content. Many discussed the benefit of pwMS delivering content within the course as it made the course more “believable”. It also made participants feel understood and gave them an opportunity to learn from the personal experiences of others. This sentiment was noted across both intervention and standard-care arms, indicating the importance of representation regardless of the specific content. Participants from Australia and New Zealand who undertook the standard-care arm, in which the content drew largely from US sources, described their wish for representation that was more specific to their countries. The importance of representation when receiving health information has been observed in other DHIs for pwMS. 25 This may relate to the importance of perceived authenticity in governing online relationships, which has previously been explored through the use of social media by pwMS. 26
People within the intervention arm commented that the “positive tone” was important to them, especially since their experience with other courses and websites/forums had described MS journeys in a fatalistic way. Presenting health information, particularly for progressive chronic conditions such as MS, presents a common dilemma of finding a balance between optimism and realism. Similar to these results, pwMS within an educational program for MS emphasised that a “warm, good natured” tone was important to them. 27 Other work with focus groups found negative information presented online with regards to poorer health outcomes in MS could negatively impact emotional or psychological well-being. 28 Importantly, the very nature of being exposed to health information within DHIs can unintentionally generate negative feelings for pwMS by being exposed to “negative” information. 29 A DHI of distress management in people with implantable cardioverter defibrillators (ICD) described similar results where negative content made participants feel worse and therefore decided not to proceed in the program. 30 Tone remains an under-explored element in delivering educational material and it is clear across studies that it remains an important consideration for pwMS.
In relation to the use of the forums within the courses, participants expressed feelings of apprehension and nervousness. Themes of uncertainty and reluctance to engage in the forum to avoid embarrassment were described across participants in both arms and it is likely that this is a generalisable problem to DHIs with “community” elements. The aspect of “not wanting to be the first” appears to be a problem that may be overcome with more direction from moderators, whether by researchers prompting conversations or by including interactive and real-time seminars between practitioners and participants. Previous research has discussed barriers for pwMS engaging in face-to-face courses such as distance, cost, and health-issues related to their disease. 31 In the present study, one participant highlighted not wanting to feel “confronted” by others with MS that may have more significant symptoms when they were feeling well themselves, which led to them avoiding peer-support entirely. However, it is unclear how common these sentiments are. Given that peer support is understood to enhance engagement in digital health behaviour change interventions32,33 and online discussion forums have demonstrated benefit for pwMS seeking health information, 34 further research to promote participation in online peer support settings for pwMS is important.
People in both arms found the course easy to navigate, even those that identified their age as a potential barrier to using computers. The design process for this course emphasised a straightforward and easy-to-navigate interface specifically to address the possible needs of pwMS. Conversely, some participants in both arms remarked on the difficulty of being able to see text or visual information presented within the online course. Both navigation and visual acuity are vital considerations for designing DHI for pwMS explored in other contexts previously.29,35 Participants in this study noted that they always knew where they were within the course, an important consideration in the design process.29,36
Across both arms the course content was perceived as easy to understand, a crucial aspect of disseminating health information to people with varying health literacy. 37 Many participants commented that the information appeared almost too easy and was suitable as introductory material, which is consistent with similar DHIs for pwMS. 29 Considering the mean duration from diagnosis was eight and eleven years, for intervention and standard-care courses respectively, some participants may have felt some information was not relevant to them, such as “What is MS?”. Relatedly, some participants wished for more depth in certain topics and regarded the length of the course and frequency of the modules as shorter than they would have liked, wishing to expand upon and deepen their knowledge and understanding. This is possibly a by-product of the researchers attempts to make the content as accessible as possible. Other participants appreciated that modules were short but of a suitable length, identifying that concentration and health concerns can make staying attentive in courses difficult, particularly for some pwMS. This relates to the desire for “personalisation” within DHIs, which pwMS consider an important factor for remaining engaged with interventions online. 36 Personalisation is an important consideration for DHIs whereby an individual's needs, experiences, sociodemographics, and health status should be tailored to ensure the information is relevant to participants, which in turn promotes engagement and retention.38,39 This has previously been achieved by building digital platforms that are responsive to users’ input.40,41 For our purposes, personalisation may mean the “dose” of content received by participants varies widely from person-to-person. This is a challenge for a future effectiveness study where improvements in health outcomes for participants exposed to the intervention program content are to be evaluated against those receiving standard-care program content.
Further to the concept of personalisation, being able to navigate the course in one's own time and at one's own pace was appealing to many, especially those with work and family commitments. Understandably, many participants experienced frustration with being required to watch a video to completion without the option to skip. The decision to make watching all the videos compulsory (including modules that may not be relevant to all participants such as the pregnancy-related module) was a study design decision to ensure a standard “dose” of the intervention was received. 42 This will need to be balanced against the evidence that it was a source of frustration for many participants and may drive attrition in a future study with larger sample size.
Ultimately, the findings of this research support that this course is acceptable to pwMS. These data are consistent with the broader research into digital health behaviour modification interventions while elucidating specific design considerations for pwMS. Our findings suggest: content should be delivered by people that represent the diverse MS community; the tone of the course content should be positive yet honest; people may not automatically participate in peer support activities and engagement may need to be cultivated by those overseeing the course delivery. Personalisation may be important in ensuring engagement with and retention in the course. This must be considered against the need to ensure a standard dose is received by participants to allow for accurate comparisons in effectiveness studies.
This study presents several significant implications for future effectiveness study. Building a community within a new RCT proved difficult and many participants reported feeling nervous and apprehensive to engage with the forum as it existed in this feasibility study. A revamping of the forum system within the effectiveness study is necessary to promote engagement, and it may be necessary to incorporate more guided opportunities to interact or involve researchers/practitioners to facilitate engagement. The representation of presenters and of MS more generally within the courses was described as limited and therefore, redesign of content within the courses should involve a more diverse population of people across a range of demographics. Finally, personalising the course for individuals is an attractive function for the course, which could occur through tailoring content for specific individual characteristics or through the ability for participants to determine what content they wish to access.
Strengths and limitations
Participants were a small sample of pwMS recruited online through MS societies and one Facebook group. Recruitment achieved a conversion of only 35 allocated participants from 84 invitations sent out. However, participation rate was high with 14/17 (76%) people who completed the online course agreeing to be interviewed, with similar rates of participation across both arms. Participants that agreed to participate in the research project are likely to be a highly motivated cohort of pwMS. This cohort may have thus been more likely to complete the course than other pwMS. Researchers conducting the interviews were not blinded to the participants’ group allocation, which may have biased the semi-structured interviews; however, being unblinded was considered necessary so that interviewers understood what course content interviewees had been exposed to and were discussing. Researchers (WB and SN) were involved in the development of the MSOC course, so their views of participants’ reflections may be biased by their perspectives.
Both the program delivery and qualitative follow-up occurred during the COVID-19 pandemic. This may have a yet unmeasured impact on the mental or physical health of this sample of pwMS, which in turn may have affected their perceptions of the online course more broadly. Additionally, areas with COVID-19-associated restrictions that required people to isolate within their homes likely saw a higher rate of people using computers, which may have also influenced people's perception of the online course.
The strengths of the study lie in the richness of the data obtained from these semi-structured interviews with participants and by the interviewers’ in-depth understanding of the course and their immersion within the study, both of which add depth and breadth to the feasibility data.
Conclusions
This study provides crucial context to the experiences of pwMS who completed the MSOC -feasibility trial. Important findings included the desire for DHIs to have a positive tone, have relatable and credible presenters of content within the course, and to be provided with the opportunity to understand the experiences of others with MS. This study provides important insights into the acceptance of this online educational course in its feasibility phase to guide course redevelopment and provide vital information to other researchers when developing DHIs for pwMS.
Footnotes
Acknowledgments
The researchers acknowledge the very generous contribution of the community advisory group, the participants in this MOSC-feasibility trial and those who took part in the qualitative interviews who gave so willingly of their time and providing their considered reflections. The authors gratefully acknowledge the assistance of our industry partner JMA Creative for course development.
Authors’ Note
This study was approved by The University of Melbourne Human Research Ethics subcommittee (ID: 1851781.2). Written informed consent was obtained from all participants prior to inclusion. Anonymised transcript data may be available upon request from corresponding author via email. All authors contributed equally to critical revisions of the article and all authors accept final responsibility for the decision to submit for publication. WB, TW, GJ, and SN were responsible for conceptualisation of the web-based course. WB, TW, GJ, SN, and KG were responsible for overall design considerations of the web-based course. WB, GJ, and SN were responsible for course content development such as videos, text, and figures. WB, TW, GJ, SN, KG, NN, and SSY were responsible for feasibility study design. WB was responsible for project administration and investigation while SN and KG were responsible for supervision during the feasibility study period. WB, SN, PJ, and JR were responsible for the development of the semi-structured question prompts. SN, PJ, and JR were responsible for conducting the semi-structure interviews. SN was responsible for transcription. WB and SN were responsible for condensing and organising data. WB, SN, PJ, and JR were responsible for identifying themes and analysis. WB, SN, and KG were responsible for writing the original draft.
Declaration of Conflicting interests
Professor Jelinek and Dr Neate have previously received remuneration for facilitating lifestyle modification workshops. Professor Jelinek receives royalties from his book “Overcoming multiple sclerosis: the 7 step recovery program.”
Funding
The Overcoming Multiple Sclerosis Charity provided financial support for the technological development of the course via JMA Creative. The Neuroepidemiology Unit receives funding from Mr Wal Pisciotta and other anonymous philanthropic donors.
Guarantor
WB accepts official responsibility for the overall integrity of the manuscript (including ethics, data handling, reporting of results, and study conduct).