
Abstract
Objectives
Despite current standard treatments, persons with Parkinson disease (PD) still experience motor and non-motor symptoms that impact daily function and quality of life, warranting the investigation of additional interventions. Holistic complementary interventions such as yoga have been shown to be beneficial for persons with PD. However, there are multiple barriers to in-person interventions such as transportation difficulties and disease-related mobility impairments which may be mitigated by digital health applications. Therefore, this study’s purpose was to assess the safety and feasibility of a synchronous tele-yoga intervention for persons with PD.
Methods
Sixteen participants were enrolled in a single group safety and feasibility trial. The entire study was conducted remotely and consisted of a baseline assessment followed by a six-week waiting period, then a second assessment, a six-week tele-yoga intervention period, a post-intervention assessment, a six-week follow-up period, and lastly a follow-up assessment. During the tele-yoga period, participants completed two one-on-one 30-minute tele-yoga sessions weekly for a total of 12 sessions. Primary outcomes included adverse events, adherence, technological challenges, and usability. Secondary outcomes included enjoyment and clinically relevant outcome measures assessing both motor and non-motor symptoms.
Results
No severe adverse events were attributed to the intervention. Retention was 87.5%, assessment session adherence was 100%, and intervention session adherence was 97%. Technological challenges did not impact feasibility. The intervention was usable and enjoyable. While this study was not powered or designed to assess the efficacy of the intervention, preliminary improvements were shown for some of the clinically relevant outcome measures.
Conclusions
Overall, this study showed that the implementation of a synchronous one-on-one tele-yoga intervention was safe, feasible, usable, and enjoyable for persons with PD. Randomized control trials investigating its efficacy should be initiated. The study was registered with ClinicalTrials.gov (NCT04240899, https://clinicaltrials.gov/ct2/show/NCT04240899).
Introduction
Parkinson disease (PD) is one of the most common movement disorders and its worldwide prevalence is predicted to be between eight to nine million by 2030. 1 It is a progressive neurodegenerative disorder characterized by a deficit in dopaminergic function. It is known for its cardinal motor symptoms including bradykinesia, tremor, muscular rigidity, and postural instability.2,3 Non-motor symptoms such as anxiety, depression, apathy, and sleep dysfunction often accompany these cardinal motor symptoms.3–5 However, current gold-standard treatments such as pharmacological interventions and deep brain stimulation primarily focus on addressing motor symptoms. 6 Additionally, even with these management techniques, people can experience fluctuations in their motor (and non-motor) symptoms without full relief.
While more attention is now being given to the management of non-motor symptoms than in the past; adequate approaches for their management are still lacking. Specifically, anxiety symptoms are sparsely addressed despite having a prevalence of up to 55% 7 in people with PD and impacting daily function, interpersonal relationships, and quality of life.8,9 In fact, a survey of mental health utilization showed that over 25% of persons with PD who expressed a need for mental health care did not receive it. 10 Furthermore, the non-motor psychological symptoms of PD such as anxiety and depression are associated with poor quality of life and in some cases have a greater association than other symptoms.11–16 Due to the fluctuations in motor symptoms and the large impact of non-motor symptoms despite available treatments, there is a need for supplementary holistic interventions that can be added to current plans of care.
Recently, there has been an increased interest in alternative non-pharmacological interventions to manage symptoms of PD. For instance, a variety of exercise approaches have been examined to address gait, freezing, and non-motor symptoms17–19 with mixed results. However, several studies have shown that, in people with PD, interventions should not only attempt to address physical symptoms but also psychological needs and spirituality.14–16 One such approach is the prescription of behavioral exercise intervention which can be defined as “conduct, routines, and habits that promote health and the ability to withstand, recover from, or grow in the face of stressors.” 20 While this encompasses a variety of approaches, complementary mind–body interventions clearly fall within this concept of combining physical, psychological, and spiritual content; and they have been shown to be beneficial for people with PD.18,19,21 Specifically, mind–body interventions can lead to improvements in motor and non-motor symptoms, gait, functional mobility, and quality of life, among others. 21
Yoga, a specific type of mind–body intervention, has the potential to address both motor and non-motor symptoms in people with PD22,23 and has specifically been shown to reduce anxiety symptoms in adult populations 24 and persons with PD. 22 A survey examining the use of complementary therapies for individuals with PD showed that approximately 20% of respondents had tried yoga and over 70% of those who tried it, perceived it as effective. 25 Furthermore, a recent randomized control trial (RCT) showed that yoga yielded significant improvements in anxiety, depression, health-related quality of life, and mobility in persons with PD. 22 Other studies have shown similar benefits for anxiety,26,27 depression,23,27,28 quality of life,28,29 and physical function, 23 indicating that yoga may lead to significant clinical improvements in people with PD. Additionally, yoga has been shown to improve the regulation of the autonomic nervous system 30 and impact the levels of the neurotransmitter GABA. 31 Both autonomic nervous system 32 and neurotransmitter dysfunction 33 are observed in people with PD and have been linked with non-motor symptoms such as anxiety and depression.33,34 Thus changes in these factors may help to explain the potential benefits of yoga in this population. Interestingly, the research to date has focused on in-person yoga. In-person yoga, however, may not be optimally accessible for individuals with PD, especially those with anxiety symptoms who may be more comfortable in their home environment. Notably, individuals with PD have voiced multiple perceived barriers to accessing in-person care including transportation difficulties35,36 and PD-related mobility impairments impacting travel. 10
Delivering yoga remotely over telecommunication networks (tele-yoga) may mitigate these barriers. Furthermore, as mentioned earlier, symptoms of anxiety are prevalent and often unaddressed in people with PD. These symptoms may further impede participation in in-person interventions. A survey of individuals with PD and mental health comorbidities, such as anxiety symptoms, indicated that over 65% of respondents with PD were interested in tele-interventions. 10 Generally, movement-based tele-interventions for individuals with PD including dance, 37 balance training/fall prevention38,39 and exercise40–42 have been shown to be safe and beneficial for this population. However, the safety and feasibility of a tele-intervention specifically for people with PD and elevated anxiety symptoms have yet to be investigated.
Now more than ever, following the presence of the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) pandemic, attention is being given to digital health applications including tele-interventions.43–45 However, a recent systematic mapping of review studies identified several gaps in the literature related to the use of digital health for quality healthcare. 46 Among the gaps identified, most of the information to date involves the application of digital health for psychiatric care predominantly through mobile health applications for mental health and behavioral therapies. 46 The review showed that there is an overall paucity of information related to the application of digital health for rehabilitation purposes and movement-based interventions, 46 such as tele-yoga.
Due to the benefits of in-person yoga and the benefits of tele-interventions, tele-yoga may be especially useful for individuals with PD and elevated anxiety. Yet, neither asynchronous tele-yoga (instruction delivered via pre-recorded materials) nor synchronous tele-yoga (instruction delivered in real-time with live interaction) has been robustly investigated for individuals with PD. These approaches have, however, been successfully implemented for other populations with health conditions.47–60 Most of these existing studies implemented asynchronous delivery of tele-yoga interventions.47–49,53,55–60 Yet, they did not include individuals with extensive mobility deficits or impaired balanced. Individuals with PD commonly experience these symptoms and may therefore benefit from a one-on-one synchronous tele-yoga intervention which allows for live individualized interaction and feedback. The few existing studies that have implemented synchronous tele-yoga delivery, including one especially for individuals with PD, 61 have shown general safety and feasibility along with some preliminary benefits.51,54,62
In summary, typical treatments for persons with PD often leave non-motor symptoms, such as anxiety, unaddressed in this population. Tele-yoga may be a beneficial supplementary intervention to address non-motor symptoms for this subset of persons with PD. However, before the efficacy of tele-yoga for this population can be examined, the safety and feasibility of this approach need to be established. As such, the objective of this study was to investigate the safety and feasibility of a synchronous tele-yoga approach in persons with PD exhibiting symptoms of anxiety. Feasibility trials capture both feasibility and preliminary efficacy outcomes useful for planning large RCTs. Here, it was hypothesized that the synchronous tele-yoga intervention would be safe and feasible for those individuals.
Methods
Study design and timeline
This was an unblinded non-randomized single group safety and feasibility study conducted entirely remotely via videoconferencing from January 2020 to July 2021. For a detailed study timeline see Figure 1. While this was a safety and feasibility study, it was designed such that future RCTs assessing motor and non-motor symptoms could be conducted using a similar timeline. Therefore, a six-week waiting period was included at the start of the study prior to the intervention period to assess the participant-specific stability of symptoms over time with their standard of care. Similarly, a six-week follow-up period was added after the intervention-period to see if changes observed following the intervention, if any, would be maintained over time. Ethics approval was obtained from the Institutional Review Board at Rutgers University and the study was registered with ClinicalTrials.gov (NCT04240899). The results of this study are reported in accordance with the CONSORT Extension for Pilot and Feasibility trials.63,64

Illustration of the study timeline. *After reviewing and singing the informed consent participants completed the Parkinson’s Anxiety Scale (PAS) to confirm baseline symptoms of anxiety. If participants did not reach the eligibility score (≥ 14), responses were destroyed, and participation ceased. If eligibility scores were met participants completed T0 and continued study participation (see Figure 3).
Participants
Individuals were recruited from ClinicalTrials.org, as well as from other websites and social media pages relevant to individuals with PD, using an online study information flyer. A convenience sample of 16 individuals was recruited This sample size corresponds to recommendations for pilot efficacy and feasibility trials stating that a minimum of 12 participants be recruited for this type of study. 65 Furthermore, previous studies were reviewed to determine whether this sample size was adequate. Our sample size fell within the range of sample sizes found in the tele-yoga literature (N = 3 53 to N = 98. 59 ) Furthermore, a previous study that successfully investigated the safety and feasibility of a synchronous tele-yoga intervention for individuals with chronic health conditions had a smaller sample size (N = 15 and ntele−yoga = 7). 54
Individuals were included if they (1) had a diagnosis of PD, (2) had anxiety symptoms (indicated by a score of ≥ 14 on the Parkinson’s Anxiety Scale (PAS) 66 (See below for how this cut-off score was determined.), (3) were able to communicate such that they could indicate pain, answer questions, and provide feedback, (4) were English-speaking, (5) had access to WiFi and an applicable technological device (e.g. laptop, tablet, smartphone, etc.), and (6) were willing to be video recorded and use Zoom. Individuals were excluded if they (1) had unmanaged major depressive disorder (self-reported) (Individuals were excluded if they reported having a diagnosis of major depressive disorder from a relevant medical professional that was currently not well managed using, for example, medication or cognitive behavioral therapy), (2) had a condition that prevented them from engaging in yoga postures (such as a musculoskeletal injury limiting the ability to bear weight on a limb or a recent surgery such as a joint replacement), (3) had major cognitive impairments, (4) had a past yoga experience exceeding five or more times within the last two month, or (5) were pregnant. During the initial videoconferencing session (T0), informed consent was obtained, and eligibility was confirmed. As per the inclusion criteria, individuals were included if they experienced anxiety symptoms as indicated by a score of ≥ 14 on the PAS. 66 While the PAS is not a diagnostic tool and does not have a severity scale indicating mild, moderate or severe anxiety, the cut-off score of 14 has been shown to discriminate between people with and without clinically relevant anxiety symptoms. 66
Intervention
The yoga intervention protocol was developed by two licensed physical therapists who were also certified yoga instructors. One of the physical therapists who developed the program was a newly licensed physical therapist with clinical exposure to individuals with PD, primarily in outpatient settings, from her academic clinical rotations. During that time, she integrated her knowledge as a yoga instructor of five years into her plans of care. The other physical therapist was board certified geriatric specialist with 40 years of experience. She routinely worked with older adults including those diagnosed with PD, predominately in sub-acute rehabilitation and long-term care settings. In 2003, she began to integrate breath work and yoga postures into her clinical practice using her clinical reasoning skills, which were rooted in Motor Learning and Control for people with PD and other neurological conditions. Together, the two physical therapists used their knowledge of yoga, their clinical experience, and the scientific literature to develop the yoga intervention protocol implemented in this study.
The yoga intervention protocol was developed with the intention of optimizing safety and facilitating the implementation of tele-yoga. To do this, the protocol was developed using the “Guidelines for developing yoga interventions for randomized trials.” 67 Careful attention was given to each of the eight domains discussed in the guideline (See Supplementary Materials Table S1 for more details about each domain). The intervention was implemented by one of the individuals who developed the yoga protocol.
The yoga intervention was delivered one-on-one, remotely, and synchronously through the videoconferencing platform Zoom for 30-minutes two times a week for six weeks. The intervention dose of 30 minutes twice weekly for six-weeks was chosen because it fell within the rage of doses described in the existing tele-yoga literature (7.5 to 90-min sessions, once weekly to daily, for 2 to 12 weeks).47–50,53–60 Furthermore, a study that compared tele-yoga intervention doses showed greater adherence to the intervention with the lower dose (60-minutes per week). 49 This further supported our intervention dose of 60 minutes per week. Thus, the delivery method and dose were intended to enhance adherence and consequently, implementation of the intervention.
Sessions were individualized to fit the participants’ needs but always included three key yogic elements in the following sequence (1) breathing exercises (first five to seven minutes), (2) yoga postures (middle 14 to 20 minutes), and (3) relaxation exercises (last five to seven minutes). A set list of breathing exercises, postures, and relaxation exercises along with levels for progression and suggestions for modifications were developed prior to the start of the study. The individualization and predetermined plan for progressions and modifications were intended to enhance safety prior to the implementation of the intervention.
For the breathing and relaxation exercises, participants were taught an exercise in the first weekly session and that exercise was reviewed and progressed as applicable in the second weekly session. For the postures, the interventionist did not have to teach all postures from the list in each session and was able to teach multiple levels of a single posture within one session. The interventionist followed a suggested script when teaching each breathing and relaxation exercise and a list of cues to use when teaching the physical postures. Figure 2 provides a brief overview of the exercises taught using their English names. Another strategy used to enhance safety, was the implementation of specific safety precautions including, encouraging another adult to be present at the residence while yoga sessions occurred and implementing modifications that facilitated balance and optimized safety. If another adult could not be present at the residence during the time of the intervention, the study team was given the name and number of a “safety” contact who was reachable during the time of the intervention. The instructor’s expertise and the participants’ comfort level were used to gauge posture levels and modifications. See the Supplementary Materials for more details regarding the yoga intervention.
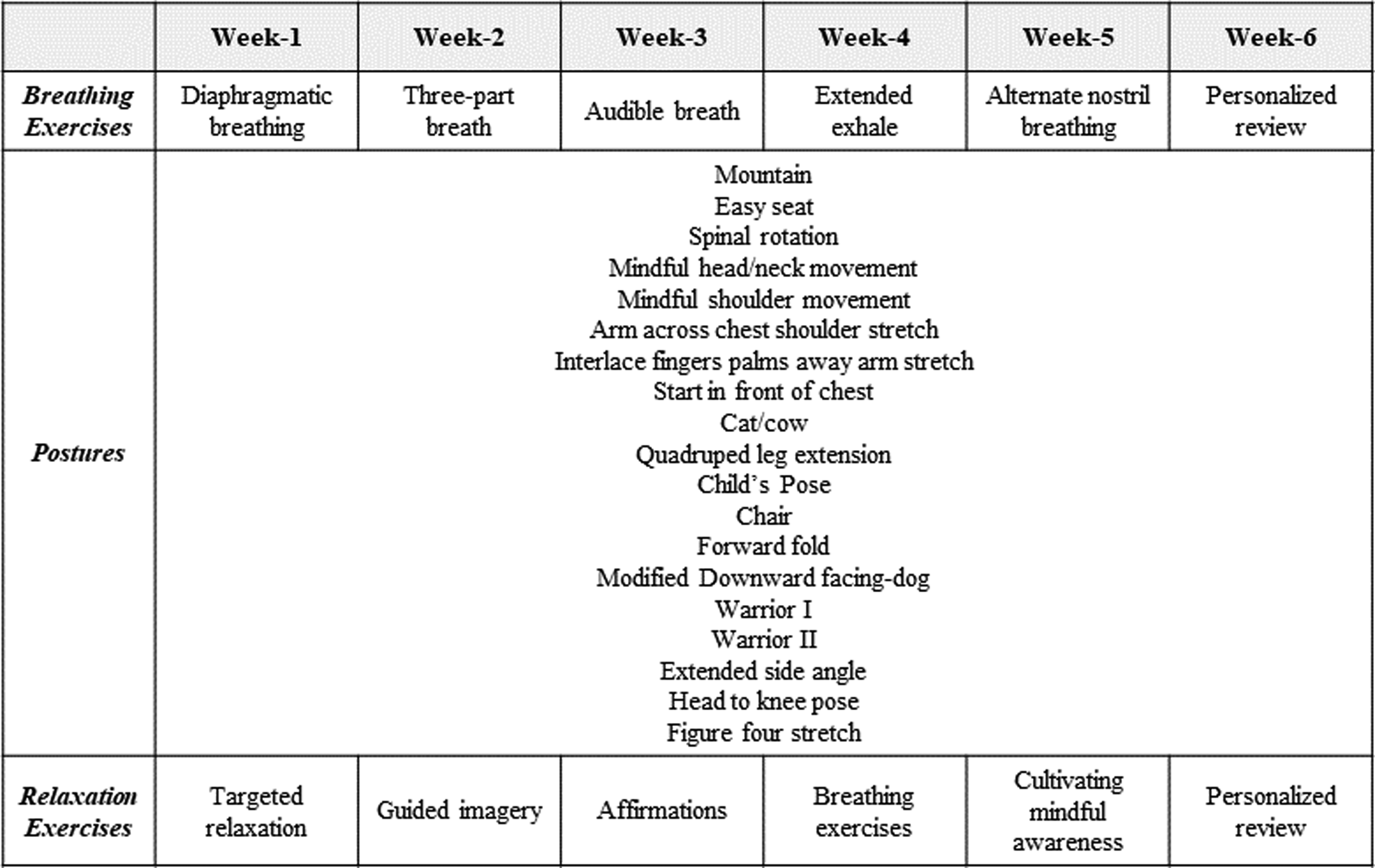
The breathing exercises, postures, and relaxation exercises taught in the yoga intervention period.
Outcome measures
Safety and feasibility benchmarks for the primary study outcomes were set a priori using the literature.
Safety. Safety was assessed through the recording of adverse events, their severity, and their relationship to the study. The severity of each adverse event was defined as (A) mild if the event resulted in no limitation of usual activities; (B) moderate if the event resulted in some limitations of usual activities; and (C) severe if the event resulted in the inability to carry out usual activities. The relationship to the study was defined as (I) not related if there was no possible relationship between the event and the relationship; (II) unlikely if the relationship between the event and the study was not reasonably related, but a causal relationship could not be ruled out; (III) possible if a causal relationship between the event and the study was uncertain; (IV) probable if there was a high degree of certainty for a causal relationship between the event and the study; and (V) definite if the causal relationship between the event and study was certain. For the intervention to be deemed safe, no severe adverse events could be attributed to the intervention (i.e. no severe events could have a possible, probable, or definite relationship to the tele-yoga intervention) and no moderate events could have a definite relationship to the tele-yoga intervention.
Recruitment rate. The recruitment rate was defined as the number of individuals who were enrolled in the study compared to the individuals who initially contacted the study team. It was reported as a percentage along with the absolute values. Because the study was a safety and feasibility trial with a sample of convenience, an a priori benchmark for an appropriate recruitment rate was not defined.
Retention rate. The retention rate was defined as the number of participants who completed the study compared to the number of individuals who were enrolled. It was reported as a percentage along with the absolute values. For a participant to be counted as completing the study they needed to engage in the tele-yoga intervention period and complete all of the four assessment sessions. Retention was deemed acceptable if 85% or more of the participants completed the study based on standards established in the literature. 68
Adherence. Adherence was divided into two categories: (i) assessment adherence and (ii) intervention adherence. Assessment adherence was defined as the number of assessment sessions completed compared to the number of assessment sessions scheduled. Intervention adherence was defined as the number of tele-yoga sessions completed compared to the number of tele-yoga sessions scheduled. Both were reported as a percentage along with the absolute values. Mean tele-yoga session attendance and percent of sessions canceled or rescheduled by all participants were also reported. Adherence was deemed acceptable if 85% or more of assessment sessions 68 and 80% or more of the yoga sessions23,69,70 were attended. These benchmarks are based on standards established in the literature 68 and the range of intervention adherence reported in previous intervention studies for similar interventions (physical activity and yoga) and populations (chronic health conditions and PD).23,69,70
Technological challenges. Technological challenges were documented, and their severity was measured by time disrupted as follows (A) mild (time disrupted 1–3 minutes), (B) moderate (time disrupted 3–10 minutes), and (C) severe (time disrupted >10 minutes). For the intervention to be deemed feasible, an a priori threshold of no more than 20% of the intended yoga dose could be missed due to technological challenges. This benchmark was determined because it aligns with the target intervention adherence of 80%23,69,70 as noted above but it is important to note that no previous studies have reported technological challenges in this way.
Usability. Usability was assessed through the Systems Usability Scale (SUS). 71 A score higher than 68 indicated adequate usability as established by the literature. 71 The participants were instructed that questions pertaining to “this system” was referring to engaging in the tele-yoga sessions over videoconferencing using Zoom.
Enjoyment. Enjoyment (secondary outcome) of the tele-yoga intervention and each component of the intervention (breathing exercises, postures, and relaxation exercises) was assessed using a 11-point scale (0–10; where 0 indicates no enjoyment and 10 great enjoyment) during the T2 assessment session. To be deemed enjoyable, a threshold of mean enjoyment scores equal to or greater than 7 was determined a priori.
Relevant clinical outcomes. Relevant clinical outcomes (secondary outcomes) were also assessed to compute effect sizes to help power future RCTs. To do this, relevant clinical outcome measures were administered at all assessment timepoints (T0, T1, T2, and T3). These outcomes included the PAS, 72 the Parkinson’s Disease Questionnaire-39, 73 the Beck Depression Inventory-II (BDI-II), 74 the PD Sleep Scale-2 (PDSS-2), 75 the Unified Parkinson’s disease Rating Scale (MDS-UPDRS) 76 (excluding rigidity and postural stability), and the five times sit to stand (FTSTS) as a measure of physical function. 77 All of these measures were standardized self-report questionnaires with the exception of the motor examination subdomain of the MDS-UPDRS and the FTSTS. All measures were administered during the live videoconferencing sessions with a study team member.
Anxiety. The 12-item self-report PAS was used to assess anxiety symptoms. It takes approximately 2-minutes to complete and is a 12-item scale with three sub-scales assessing persistent anxiety, episodic anxiety, and avoidance behavior. The questions are on a scale from "not or never" (0) to "severe or almost always" (4) with a potential score range of 0–48. Higher scores indicate greater symptoms of anxiety. This scale is valid and reliable for persons with PD.66,72
Depression. The 21-item self-report BDI-II was used to measure symptoms of depression. For each item, the participants choose one out of four statements of increasing severity regarding a specific symptom of depression. It takes about 5–10 minutes to complete. Potential scores range from 0–63 with higher scores indicating greater severity of depressive symptoms. The BDI-II has good psychometrics properties 74 and has been shown to be acceptable for assessing depressive symptoms in PD. 78
Quality of life. The 39-item self-report questionnaire was used to assess the quality of life. It has 8 domains (e.g. mobility, emotional well-being, stigma, social support, cognition, communication, and bodily discomfort) and contains questions asking how often certain difficulties/problems have occurred within the last month with answers ranging from "never" to "always." Each dimension’s total score ranges from 0 (never have difficulty) to 100 (always have difficulty). With higher scores indicating poorer quality of life. The PDQ-39 is valid and reliable for persons with PD. 73
Sleep. The 15-item self-report PDSS-2 measure was used to assess sleep dysfunction. It contains questions about the participant's sleep experience during the past week with answers on a Likert-scale of 0-"very often" to 4-"never." Scores can range from 0 to 60 with higher scores indicating greater sleep impairment. It is a valid and reliable tool for persons with PD. 75
Motor and non-motor symptoms of PD. A modified version of the MDS-UPDRS (excluding examination of rigidity and postural instability) was used to assess motor and non-motor symptoms of PD. It contains four sections 1. Mentation, Behavior, and Mood; 2. Activities of Daily Living; 3. Motor Examination; and 4. Complications of Therapy. Higher scores indicate greater symptoms/disability. The modified version excludes the hands-on components such that the measure can be administered over videoconferencing. This modified version of the MDS-UPDRS excluding rigidity and postural instability completed virtually has demonstrated high levels of agreement with the complete in-person MDS-UPDRS. 79 Additionally, inter-rater reliability of video-based assessment showed moderate to high agreement between raters. 80
Physical Function. The FTSTS was administered to assess physical function. It was administered using a chair in the participants’ homes. Participants were encouraged to have another adult present during this portion of the data collection in case there was any loss of balance. The time, in seconds, that it took participants to raise from the chair 5 times was recorded. Longer times indicate poorer physical function. The FTSTS has shown adequate psychometric properties for persons with PD. 77
Data and statistical analysis
R and R studio81,82 were used to complete score computation and statistical analyses for all outcome measures. Percentages were computed as applicable. Available subdomain scores and total scores were computed as applicable. Item mean imputation was used to address missing items (i.e. the mean of the specific missing item for the relevant assessment session across all subjects was imputed for missing values). This was primarily used to impute missing items from the two participants who withdrew from the study and necessary for the calculation of the effect sizes. Missing items were distributed across T0 (n = 25), T1 (n = 185), T2 (n = 314), and T3 (n = 331) (see Table S2 in the supplementary materials for more details regarding missing items). Descriptive statistics of all measures were determined. For the clinically relevant outcomes used to compute effect sizes, normality was determined using the Shapiro Wilk Test. Then, repeated measures analysis of variance (rmANOVAs) or Friedman tests were completed for normally distributed data and non-normally distributed data respectively. Post-hoc analysis was conducted as applicable. The Bonferroni correction with an adjusted p-value for multiple comparisons (α = 0.0083) was used following statistically significant results of rmANOVAs. The Nemenyi-Test was used following statistically significant results of Friedman tests. The effect sizes, partial eta squared or Kendall’s W, were calculated as applicable.
Results
Participants
Initially, 54 individuals contacted the study team displaying interest in the study. After learning more about the study including eligibility requirements and the study time commitment 34 individuals decided to engage in the telephone-based screening session. Twenty-three of the 34 individuals who engaged the phone screen completed the PAS to confirm eligibility. The other eleven individuals who completed the phone screen were either ineligible or decided not to participate in the study (see Figure 3). All individuals (n = 16) who demonstrated baseline levels of anxiety (mean score of 19.9 ± 4.9) were enrolled in the study. Therefore, the recruitment rate was 29.6% (16 participants enrolled out of 54 participants who initially contacted the study team). Fourteen participants completed the study. One participant withdrew after the T0 assessment due to a family emergency and another participant withdrew after the fourth yoga session, reporting that they felt the yoga sessions were below their ability level. Therefore, the retention rate was 87.5%. See Figure 3 for the Consort flow chart illustrating participant recruitment and retention.

The recruitment and enrollment CONSORT chart.
The individuals enrolled were people with mild to moderate PD (Hoehn and Yahr stages 1–3). Disease management strategies at the time of enrollment varied across participants: carbidopa-levodopa (n = 10), carbidopa-entacapone-levodopa (n = 1), levodopa and benserazide (n = 1), rotigotine (n = 1), deep brain stimulation (n = 1), and physical activity (n = 10). Some participants were also managing symptoms of anxiety (n = 4) and depression (n = 8) with medication. Participants were recruited regardless of medication status and four participants experienced changes in medication over the course of the study. See Supplementary Materials for details regarding medication changes. Notably, participants were not all located within the United States, with one participant living in Canada and another living in the United Kingdom. See Table 1 for participant baseline demographics.
Participant demographics.
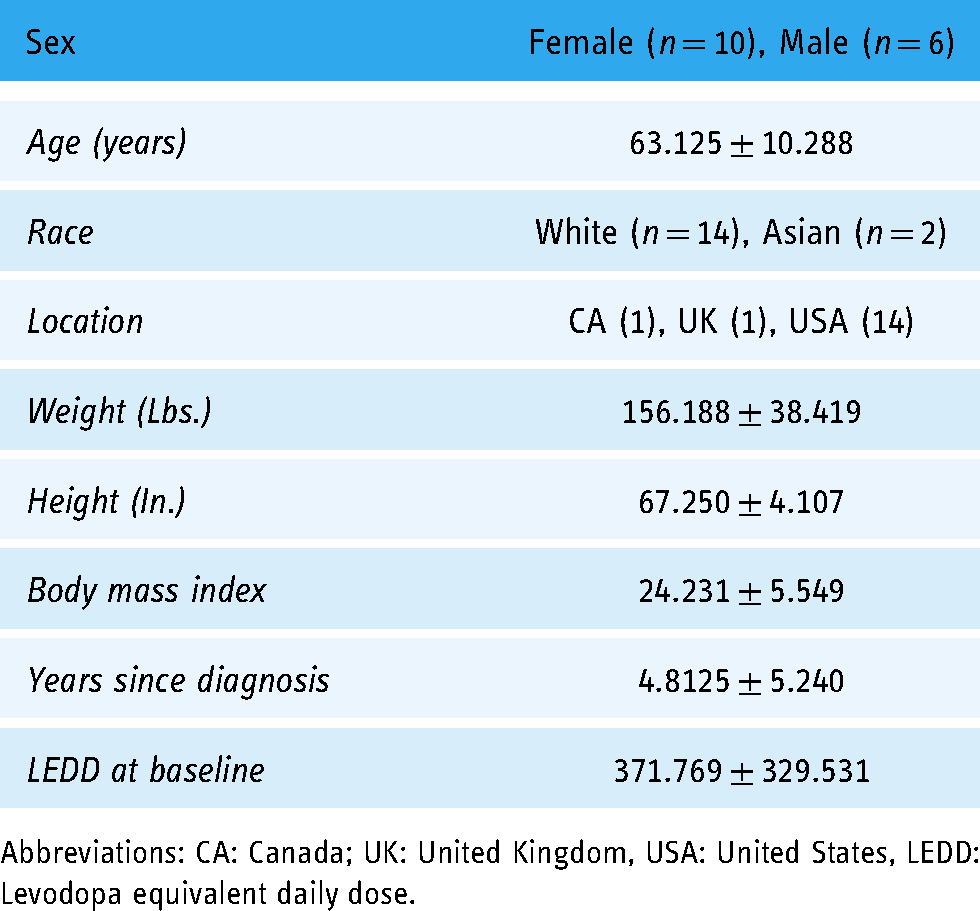
Abbreviations: CA: Canada; UK: United Kingdom, USA: United States, LEDD: Levodopa equivalent daily dose.
Safety
There were no severe adverse events with a possible, probable, or definite relationship to the intervention and no moderate events with a definite relationship to the intervention. Some mild and moderate adverse events did occur.
Mild adverse events not related to the intervention included baseline pain, new pain related to outside activity, not feeling well, unrelated losses of balance, and medication side effects. Mild adverse events not likely related to the intervention included temporary pain occurring prior to yoga sessions and participant-reported increased awareness of PD symptoms such as tremor. Mild adverse events with a possible relationship to the study included transient increases in existing pain attributed to participants’ typical patterns of wellness, and transient new pain noticed outside of the intervention sessions. Mild adverse events with a possible relationship to the study included transient increases in existing pain or transient occurrences of new pain noticed during the yoga sessions but attributed by the participants to their typical patterns of wellness or outside physical activity. Mild adverse events with a probable relationship to the study included temporary increases in pain and temporary bouts of dizziness noticed during the yoga sessions. Mild adverse events with a definite relationship to the intervention included transient pain coinciding with specific yoga postures such as knee pain in the easy seat and inner thigh pain during seated number four. These increases in pain ceased when the postures were stopped.
Moderate adverse events not related to the intervention included illness that resulted in the rescheduling of yoga sessions and falls that led to modifications of the yoga postures including the elimination of kneeling postures in the session following the fall. One moderate adverse event with an unlikely relationship to the intervention was prolonged dizziness between intervention sessions that resolved with a few hours of rest One moderate adverse event with a possible relationship to the intervention was an exacerbation of low back pain over the course of the study, however the participant did not attribute this pain to the intervention.
Two severe adverse events not related to the intervention occurred and included an emergency room visit for a urinary tract infection during the follow-up period and reoccurring bouts of insomnia that impacted the participant’s usual activities but was reported as a typical pattern of wellness. For more details about the occurrence of adverse events see Table 2.
Adverse events .

Feasibility
Adherence to assessment sessions was 100% (59 assessment sessions completed out of 59 scheduled). Yoga intervention adherence was 97% (167 tele-yoga sessions completed out of 172 scheduled). Mean tele-yoga session attendance at 11.13 ± 2.10 sessions out of the 12 intended sessions. It is important to note that for the two participants who formally withdrew from the study, the assessment sessions and yoga sessions after the participants withdrew were not included in the adherence calculations because the sessions were not scheduled. Eleven participants completed all 12 intended yoga sessions. Of the yoga sessions attended, 33 sessions (20%) were rescheduled due to participants’ requests, five sessions (3%) were rescheduled due to the interventionist’s request, and five sessions (3%) were canceled for participant-related reasons.
Technological challenges. Technological challenges occurred and this despite the fact that some of the participants (n = 3) had family members assist them in setting up the videoconferencing platform each session. Of those, 78.9% were mild (71/90), 11.1% were moderate (10/90), and 10.0% (9/90) were severe. The most common challenge was video/audio delay. The delay did not often disrupt time but impacted the overall quality of the session in which it occurred. For more information about technological challenges see Table 3. In addition to technological challenges, there were also other challenges that occurred during the intervention. These included disruptions, such as familial or pet interruptions, and difficulty reaching the participants’ safety contacts. Overall, of the challenges that occurred, 83.3% were technological in nature (90/108) and 16.7% were not related to technology (18/108).
Technological challenges during yoga sessions.

Usability. Usability was good as evidenced by the mean score on the SUS of 81.3 ± 17.1. As such, despite the technological challenges, the participants’ experience in engaging in the intervention through the videoconferencing platform was good.
Enjoyment. Enjoyment scores were high for the complete yoga intervention (9.0 ± 1.0), breathing exercises (8.3 ± 1.0), postures (9.1 ± 1.0), relaxation exercises (9.3 ± 0.6), and the overall remote study experience (8.9 ± 1.0).
Clinically relevant outcome measures demonstrated a range of effect sizes (ηP2 = 0.019 (UPDRS-total) to ηP2 = 0.417 (PAS total) and K = 0.053 (PD symptoms subdomain of the PDSS-2) and K = 0.609 (BDI)) with four measures (anxiety, quality of life, depression, and motor-experiences of daily living) demonstrating preliminary improvements. For descriptive statistics and effect sizes of each clinically relevant outcome measure see Table 4 and for the results of the rmANOVAs, Friedman Tests and post-hoc analyses see Table 5.
Descriptive statistics and effect sizes for relevant clinical outcome measures.

Mean scores, standard deviations, and applicable effect sizes (ηP2-for normal distribution) and W-for non-normal distribution for clinically relevant outcomes. Symbols: α15 participants completed timepoint-2 assessment and β14 participants completed post-intervention and follow-up; item mean imputation was used to include the missing participant in analysis, *statistically significant effect for an outcome
BDI: Beck Depression Inventory-II; EWB: emotional wellbeing; FTSTS: Five Times Sit to Stand; ME: Motor Experiences of Daily Living; NME: Non-motor Experiences of Daily Living; PAS: Parkinson’s Anxiety Scale; PDSS-2: Parkinson’s Disease Sleep Scale-2; Parkinson’s Disease Questionnaire- 39; UPDRS: The MDS-sponsored Revision of the Unified Parkinson’s Disease Rating Scale.
Additional results for relevant clinical outcome measures.

Results of repeated measures ANOVAs, Friedman Tests and post-hoc analysis. Symbols: α15 participants completed timepoint-2 assessment and β14 participants completed post-intervention and follow-up, item mean imputation was used to include the missing participant in analysis, +Friedman Test results, *statistically significant (α = 0.05-rmANOVAs, α = 0.016-post hoc analysis (corrected for multiple comparisons)
BDI: Beck Depression Inventory-II; Comm.: communication; EWB: emotional well-being; FTSTS: Five Times Sit to Stand; ME: Motor Experiences of Daily Living; NME: Non-motor Experiences of Daily Living; PAS: Parkinson’s Anxiety Scale; PDSS-2: Parkinson’s Disease Sleep Scale-2, Parkinson’s Disease Questionnaire-39; UPDRS: The MDS-sponsored Revision of the Unified Parkinson’s Disease Rating Scale.
Discussion
While there is an existing body of literature supporting the use of in-person yoga for persons with PD,22,23,28,29,70,83–89 this is one of the first studies to investigate the safety and feasibility of a synchronous tele-yoga intervention for this population. Feasibility trials are important to ensure that larger RCTs are rigorous, feasible and economically justifiable. 90 This study found one-on-one synchronous tele-yoga to be safe and feasible for 16 individuals with mild to moderate PD (Hoehn and Yahr stages 1–3) and elevated anxiety symptoms. These findings may help to facilitate the use and implementation of digital health to improve the access to yoga and facilitate the integration of holistic interventions into plans of care for persons with PD.
This study provided information about the safety of a home-based synchronous one-on-one tele-yoga intervention for people with PD. Our findings showed that there were no severe adverse events attributed to the intervention and no moderate adverse events with a definite relationship to the intervention. Thus indicating that home-based one-on-one synchronous tele-yoga was safe for individuals with PD and anxiety. This is in line with the general yoga literature, 91 as well as the literature specific to yoga for persons with PD22,23,61,85,92 which have all shown yoga to be generally safe in a variety of settings. Additionally, the existing tele-yoga literature has shown both synchronous54,61 and asynchronous47,59,93 tele-yoga to be safe for adults with different physical and mental health conditions. It is important to note however, that most previously published studies demonstrating the safety of tele-yoga have not specifically included individuals with postural instability and balance impairments. These symptoms are commonly experienced by people with PD 3 and may increase safety and fall risks, especially when implementing a tele-intervention. While tele-yoga has only once been previously investigated in people with PD, 61 the safety of other remotely delivered movement-based interventions has been more robustly investigated.41,94–97 These interventions were shown to be safe however, specific inclusion criteria 61 and safety precautions were often implemented. These included encouraging another adult to be present if needed,61,97 instructing the participant to complete the exercises in a seated position, 41 or instructing the participant to have a wall and sturdy chair nearby. 61 In the current study, similar safety precautions were also implemented including encouraging another adult to be present at the residence (or at least being reachable by phone) during the yoga session and modifying postures to facilitate balance including having a sturdy piece of furniture nearby. So, while this study demonstrated the safety of the intervention, there are multiple factors that could have contributed to this finding.
First, based on our findings and previous literature, the synchronous delivery may have positively influenced safety. For example, a previously conducted study that involved an asynchronous tele-exercise intervention for people with PD resulted in one adverse event that was severe enough to result in withdrawal from the study. 98 This serves as an example of why synchronous live-monitoring may help to optimize the safety of tele-interventions for this population. Adding to this, a scoping review of home-based physical therapy for people with PD highlighted the importance of personal guidance and immediate feedback for optimizing safety for this population. 99 Furthermore, a cross-sectional survey investigating the safety of yoga showed that practicing yoga by self-study without live feedback was associated with a higher risk of injury. 100 Taken together, these findings show that the synchronous application of digital health may help to explain our results and optimize the safety of tele-yoga interventions in people with PD. We suggest that for individuals with potentially severe balance and mobility impairments, a synchronous approach should be prioritized.
Second, the one-on-one aspect of delivery and expertise of the interventionist may have also contributed to our findings. The individual delivery allowed the interventionist to observe and react in real time to each participant’s needs, which also addressed this population’s need for personal and immediate guidance (as mentioned above). 99 While individual delivery is different from the common delivery method for in-person yoga, which is often delivered to a group, it more closely resembles how typical rehabilitation interventions are delivered. We think that the fact that the intervention was designed and instructed by a physical therapist may have also facilitated safety. The physical therapist employed knowledge of movement disorders and clinical practice, which was used to individually adapt each session for each participant. The cross-section survey investigating the safety of yoga mentioned above also indicated that the risk of adverse events was reduced when the intervention was provided by qualified, experienced instructors. 100 This indicates that one-on-one delivery by a knowledgeable professional may have also facilitated safety. While individual delivery by knowledgeable professionals can be conducted in-person, the addition of the digital application may have increased access to the intervention to individuals who otherwise may not have access to it. However, the practical application of such interventions may be limited, and future work should focus on determining whether home-based synchronous group interventions are as safe as our protocol.
In addition to providing information about intervention safety, this study also provided information about the feasibility of the approach. Participant retention was 87.5%, assessment adherence was 100%, and intervention adherence was 97%. Additionally, while technological challenges occurred, they did not disrupt the amount of yoga received and the participant-reported usability showed a mean score of 81.3 ± 17.1. This demonstrates that a home-based one-on-one synchronous tele-yoga for people with mild to moderate PD and elevated anxiety symptoms was feasible. Similar to the safety of the intervention, the feasibility of the intervention may have been facilitated by multiple factors.
First, the ability to reschedule the tele-yoga sessions may have positively contributed to the intervention’s feasibility. People with PD often experience fluctuations in symptoms101,102 and busy schedules attributed to multiple healthcare appointments. This can result in variable availability. Therefore, providing flexible scheduling and the ability to reschedule may have helped participants maintain high adherence to the intervention sessions. In fact, a systematic review of physical activity interventions for older adults showed that convenient scheduling helped to improve intervention adherence. 103 With this, the one-on-one delivery of the intervention may have facilitated flexibility in scheduling. While one-on-one delivery does not necessarily mean that rescheduling will occur, it is easier to offer flexible rescheduling options with one-on-one delivery compared to group delivery. An example of this is shown in a previously conducted group tele-yoga study that demonstrated feasibility challenges due to scheduling difficulties. 51 Another study showed that a participant had to miss a group tele-yoga session due to a doctor’s appointment. 61 Thus, the one-on-one delivery and flexible scheduling may have facilitated the high adherence demonstrated here.
Second, the implementation of synchronous delivery may have helped to facilitate adherence. Synchronous delivery provided the opportunity for social interaction with the interventionist, individualization, and feedback. Feedback has been shown to motivate people with PD to start and continue exercise programs. 104 Furthermore, a study comparing asynchronous and synchronous telerehabilitation for individuals with spinal cord injury showed higher adherence to the synchronous delivery method compared to the asynchronous delivery method. 105 This supports the idea the synchronous delivery may have positively influenced adherence and feasibility here.
Third, the high levels of enjoyment shown by participants for the intervention and its various components may also help to explain the high adherence and related feasibility. Higher enjoyment has been shown to be associated with higher intervention adherence. 106 All participants reported that they liked engaging in the yoga sessions one-on-one in their own homes. This may be because people with PD can experience stigma which often results in anxiety, fear, or discomfort when being watched by/engaging with others. 107 People with elevated anxiety and PD may experience this even more and may especially benefit from one-on-one remote delivery as implemented here. All participants also mentioned that they found the instructor helpful, and some explained that they liked the intervention because of the instructor’s style and demeanor. Other studies have shown that satisfaction with an instructor may be a contributing factor to exercise enjoyment. 108 Therefore, the high levels of enjoyment may be attributed to the one-on-one remote home delivery and instructor characteristics. This may have subsequently impacted adherence and feasibility.
In addition to the safety and feasibility of the intervention our findings demonstrated preliminary improvements in anxiety and depressive symptoms, as well as in quality of life. These results are in line with previously published studies for people with PD that have shown similar benefits for anxiety, depression, and quality of life following in-person yoga22,109 and group-based tele-yoga. 61 These outcome measures also demonstrated moderate to large effect sizes which can be used to help power future RCTs.
There are limitations to the current study. First, it was a small unblinded, single group, non-randomized study. People were recruited regardless of disease severity, disease duration, and medication status. These broad inclusion criteria could impact the ability to interpret the efficacy of this intervention. However, the participants’ heterogeneity helped to demonstrate the safety and feasibility of the tele-yoga intervention for a variety of individuals with PD. Second, participants self-reported all information related to the inclusion and exclusion criteria. Reliance on self-report for most of the eligibility criteria may have resulted in the inclusion of individuals who did not accurately meet the criteria. Third, due to the novel nature of this study, some of the measures, including the rating of the severity of technological challenges, do not have established validity and reliability. With this, some of the benchmarks were established using the expertise and clinical reasoning of the study authors. However, our methods and rationale are clearly described in this paper. Fourth, because the study started slightly before the SARS-CoV-2 pandemic, there were circumstances that could not be controlled that may have impacted adherence and mental health throughout. Specifically, the global SARS-CoV-2 pandemic has been shown to impact mental health and quality of life in persons with PD. 110 Fifth, selection bias may have occurred, as participants were a self-selected cohort, such that people familiar with yoga and/or already involved in physical activity may have been drawn to participate in the study more than other individuals. Lastly, it is important to note that as this study was a safety and feasibility study, assessing efficacy was not its main purpose. Consequently, the study was not designed or powered to assess the efficacy and those results should be interpreted cautiously. While these factors should be taken into consideration when interpreting the study results, the results are promising and can be used to inform future RCTs.
Conclusions
Previous work has shown in-person yoga to be a beneficial22,23,28,29,70,83–89 and safe complementary intervention for persons with PD. Barriers, however, may limit access to this approach especially for individuals with PD and elevated anxiety symptoms. A digital health or tele-delivery approach may help to attenuate those barriers. Prior to the current study, the safety and feasibility of this type of approach were unknown for this specific subpopulation of individuals with PD. Therefore, we showed here that one-on-one synchronous tele-yoga is safe and feasible for individuals with mild to moderate PD and elevated anxiety symptoms. With the results of this study confirming the safety and feasibility of this approach in this sub-population of persons with PD, future RCTs should be initiated.
Footnotes
Acknowledgments
We would like to acknowledge the participants and their families, whose time and participation were invaluable. We would also like to thank laboratory volunteers, Shannon Crehan, Miriam Pomerantz, and Sanya Ravoori who assisted in recruitment efforts. We would also thank Dr Ellen Z. Anderson for her help in developing the yoga intervention and Dr Judith E. Deutsch for her insight and feedback regarding the study design. We also acknowledge Drs Carrie Esopenko and Samantha Farris for their guidance in navigating mental health comorbidities and the related outcome measure selection.
Author Contributions
AMJP and JFD participated in the research project conception, design, and organization and were involved in gaining ethical approval. AMJP was involved in participant recruitment and conducted assessment sessions and implemented intervention sessions under the supervision of JFD. AMJP and JFD were involved in statistical analysis design and execution. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Institutional Review Board at Rutgers University, The State University of New Jersey approved this study (Protocol ID number: Pro2018002758).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.