
Abstract
Background
Due to digitization in the medical sector, many healthcare interactions are switched to online services. This study assessed the acceptance of video consultations (VCs) in cancer care, and determined drivers and barriers of acceptance.
Methods
A cross-sectional online-based survey study was conducted in Germany from February 2022 to February 2023. Recruitment took place at oncology outpatient clinics, general practitioners, oncology practices and via cancer-related social media channels. Inclusion criteria were a cancer diagnosis, cancer treatment and internet access. Sociodemographic, medical data, eHealth-related data were acquired via an online assessment. The Unified Theory of Acceptance and Use of Technology (UTAUT) model was used to determine the acceptance of VC and its predictors.
Results
Of N = 350 cancer patients, 56.0% (n = 196) reported high acceptance of VC, 28.0% (n = 98) stated moderate acceptance and 16.0% (n = 56) indicated low acceptance. Factors influencing acceptance were younger age (β = –.28, p < .001), female gender (β = .35, p = .005), stage of disease (β = .11, p = .032), high digital confidence (β = .14, p = .010), low internet anxiety (β = –.21, p = .001), high digital overload (β = –.12, p = .022), high eHealth literacy (β = .14, p = .028), personal trust (β = –.25, p < .001), internet use (β = .17, p = .002), and the UTAUT predictors: performance expectancy (β = .24, p < .001), effort expectancy (β = .26, p < .001), and social influence (β = .34, p < .001).
Conclusions
Patients’ acceptance of VC in cancer care is high. Drivers and barriers to acceptance identified should be considered for personalized applications. Considering the growing demand for cancer care establishing digital healthcare solutions is justified.
Introduction
Around the world, a rising number of people are developing cancer over the course of their lifetimes. In 2020, the World Health Organization's (WHO) International Agency for Research on Cancer recorded 19,292,789 new cases worldwide, of which 4,398,443 were in Europe and, 628,519 in Germany.1,2 The estimated five-year prevalence of cancer in Germany was 2,188,176 in 2020. 2 This increasing prevalence is connected to the increased life expectancy of patients undergoing optimal care. 3 In light of these statistics, it is clear that the need for treatment and medical consultations will also increase. To be able to treat patients as effectively as possible, it would be prudent to supplement conventional types of examinations and treatment with new forms of care, for example through telemedicine.
Since the WHO declared the COVID-19 outbreak a pandemic in 2020, the nation's healthcare system was confronted with unprecedented difficulties. 4 To contain the virus, all social interactions had to be largely avoided, including nonmandatory visits to physicians. 4 Preventive healthcare appointments and checkups had to be canceled or postponed to adequately protect vulnerable people. 5 As a result, some malignancies were not detected at an earlier stage or not at all. 6 However, the WHO emphasizes the importance of early diagnosis for effective care and an improved prognosis. 7 The WHO noted that the number of cancer diagnoses in some European countries decreased by as much as 40% during the first instances of lockdown. 6 To prevent diagnostic delays during the lockdown and continue providing sufficient health care, many medical fields, including oncology, increasingly focused on telemedicine, such as video consultations (VCs) as a substitute for in-person appointments. 5
Digitalization is continuously making great advances in the global healthcare sector, and in recent years, telemedicine has become an important part of that. In particular, the use of medical VC has become increasingly established in many fields, such as pediatric cardiology, dermatology, palliative care, and other disciplines, especially at times when face-to-face appointments are less widely available, as was the case in the pandemic situation or due to a shortage of doctors.5,8–11 By definition, telemedicine means, “the delivery of health care and the exchange of health-care information across distances.” 12 According to the WHO, it is intended to support and improve healthcare by overcoming geographical barriers and connecting users from various places. 13 Several information and communications technologies (hereinafter referred to only as ICT), such as computers and mobile phones, are used to share information about diagnosis, treatment and prevention. 13
Especially in oncology, wider use of telemedicine would enable patients to see specialists from all over the country or even the world. It could “aid communities traditionally underserved”—especially people in rural or remote regions—to engage with an oncologist to receive adequate care.5,7,14 Furthermore, a consultation by video or telephone could be a considerable facilitation of therapy, when a direct physical examination is not required, especially for older and more restricted patients. 14 Moreover, it is suitable for implementing interprofessional care in multidisciplinary, team-based cancer care. 15 In addition, previous studies have shown that VCs are not only more cost-effective but also reduce waiting times and nonattendance rates.5,16–19
Other studies have also been able to highlight the benefits of teleoncology. Shirke et al.'s review of the future effects of VC in oncology for example states that it has the potential to improve cancer care. Besides the time and cost savings, the use of ICT provides improved and more individualized access to care and education for patients. 20 Additionally, Granberg et al. conclude that some patients prefer VC, especially for serious messages, as a way to receive information in a more private setting. 21 Due to the proximity of family comfort and familiar surroundings, bad news may be better processed for some patients. 21 Schade et al. describe how VC may improve mental health and make communication more patient-centered, which can also positively affect the outcome of care. 22
Despite all the benefits of VC, it is also important to consider the limitations. In this context, Shirke et al. cite the limited options for physical examination. 20 Other difficulties might arise from the patients’ respective technical requirements. The availability of technological devices and functioning internet access varies amongst patients and often depends on people's socioeconomic status. 22 A large proportion of cancer patients are among the elderly, which may pose difficulties to the use of VC. 20 In case of technical challenges, phone telehealth could be an alternative to VC. 23 In addition, this form of care may be challenging for people with hearing, vision, or cognitive impairments. Furthermore, lack of trust in technology, fear of misdiagnosis via video or an emotional distance to the provider could also be barriers to the use of VC in oncology. 19 In terms of doctor–patient communication, empathy and nonverbal signs are important factors, and they are likely more difficult to convey and perceive via VC in comparison to in-person consultation. 22
To achieve widespread adoption of telemedicine and accelerate its implementation, the “eHealth law” was introduced in 2015. 24 Information on reimbursement regulation for VC is included in the Supplemental Materials. For the successful use of digital innovations in health care, it is important to measure the acceptance among potential users, as this is a key indicator of actual use. Furthermore, it is necessary to detect influencing factors and possible barriers. 18 A suitable model for predicting the use of eHealth approaches is the Unified Theory of Acceptance and Use of Technology (UTAUT) model by Venkatesh et al. 25 It combines eight user acceptance models which predict the usage behavior of several technologies. 26 Acceptance toward technology is operationalized as behavioral intention (BI) to use a technology. BI results from performance expectancy (PE) as the perceived usefulness and effort expectancy (EE) as the expected ease of use, and social influence (SI).26–28 SI describes the degree to which the user's environment (e.g., doctors) is of the opinion that telemedicine should be used.
In summary, the increasing need for cancer care has led to the demand for additional treatment options. To understand to what extent telemedicine should be offered and to perform evidence-based implementation strategies, acceptance of these new ways of healthcare needs to be examined. VC as care across distances provides certain benefits which may facilitate treatment, especially for more restricted patients from remote regions.5,7,14 Existing barriers to use, such as technical requirements and emotional distance to the physician need to be overcome.19,20 Most qualified for capturing these predictors for acceptance is the UTAUT model. 25
The aim of this study is to evaluate cancer patients’ acceptance and determine drivers and barriers of VC in cancer care as a supplement to personal visits to an oncologist in Germany. For this purpose, additional factors of sociodemographic, medical and ICT-related data were added to the original UTAUT model to form an extended UTAUT version.
Methods
Study design and study population
This study was a cross-sectional online-based survey study. Acceptance of VC in cancer care and its drivers and barriers were assessed among oncological patients. Recruitment was conducted in oncological outpatient clinics of different hospitals in North Rhine-Westphalia, in general practitioner and oncology practices and, as well as via cancer-focused social media channels and blogs. Study information was distributed via flyers, posters, and the study staff. Participation was voluntary, anonymous, and without compensation or financial incentive. Inclusion criteria for study participants were a cancer diagnosis, cancer care (currently or in the past), good knowledge of the German language, majority and internet access. Digital informed consent was given before the beginning of the survey. Data collection took place from February 2022 to February 2023 via the platform Unipark (Questback GmbH). The average completion time was M = 14 min (SD = 9). N = 499 participants started the survey, of which 71.11% (N = 352) completed it. Two participants had to be excluded because they did not fulfill the inclusion criteria. As a result, N = 350 participants were included in the final data analysis. The conductance of the study was approved by the Ethics Committee of the Medical Faculty of the University of Duisburg-Essen (19-89-47-BO).
Assessment instruments
The survey was composed of sociodemographic, medical, psychometric, and eHealth data (including acceptance). Validated assessment instruments and self-generated items were used to collect responses. For the questionnaire, see the Supplemental Materials.
In the first section of the survey, sociodemographic aspects, such as age, gender, marital status, educational background, and occupational status, were assessed. In addition, this part inquired about the distance between their respective place of residence and the location of the oncologist treating them.
This was followed by a medical anamnesis including an oncological history, which included an assessment of the time of diagnosis, tumor localization, and current therapy. Further, the participants were asked about recurrences, metastases and the current stage of their disease (in accordance with the definition of the National Cancer Institute29,30). Depressive symptoms over a two-week period were assessed with the Patient Health Questionnaire Scale-8 (PHQ-8), which is scaled on a four-point Likert scale (0 = “never” to 4 = “almost every day”). A cutoff score of 10 or more indicates current major depression symptoms. 31 Internal consistency was high (Cronbach's α = .85). Distress was assessed via the visual scale of the distress thermometer (DT 32 ), ranging from 0 = “no distress” to 10 = “extreme distress.” Furthermore, a history of mental illnesses was examined.
In the next part of the survey, participants were asked about their use of ICT in general, on a five-point Likert scale (digital confidence,33–37 internet and VC use for private and professional purposes, 38 digital overload, and internet anxiety33–37). Digital confidence could be indicated for digital media and end devices, as well as for internet platforms in general and for VC (1 = “very uncertain” to 5 = “very safe”). Internal consistency was excellent (Cronbach's α = .94). With regard to previous user behavior, the cancer patients were asked for their daily private and professional internet use (1 = “not at all” to 5 = “more than five hours a day”). Internet anxiety and digital overload were each assessed via three items, for example, whether the participants have concerns about using the internet or are worried by it and if they feel burdened by permanent accessibility (1 = “strongly disagree” to 5 = “strongly agree”). Internal consistency was high (Cronbach's α = .85 and .76, respectively). Knowledge of digital health support in oncology was also assessed by three items (1 = “strongly disagree” to 5 = “strongly agree”). 38 Internal consistency was high (Cronbach's α = .88).
Using the revised German version of the eHealth Literacy Scale, GR-eHEALS, eight further items were used to measure the respondents’ digital health literacy. 39 On a five-point Likert scale (1 = “strongly disagree” to 5 = “strongly agree”), respondents could indicate, for example, their knowledge of where to find helpful health information online and their ability to use and critically evaluate it. The sum score ranges from 8 to 40, whereby a higher score indicates a higher level of eHealth literacy. Internal consistency was excellent (Cronbach's α = .95).
Participants were asked whether their oncologist already had the capabilities to offer VC and whether they already made use of it. Participants were asked for which medical problems they would potentially use VC (e.g., minor medical problems) and for indicated barriers of VC use (e.g., lack of technical requirements). On a five-point Likert scale (1 = “very important” to 5 = “not important at all”), participants were further asked to indicate how important it is to them to have previously met the physician in person and to have previously established a relationship of trust. Further, patients were asked about prior use of other digital services in health care (e.g., online pharmacy).
The UTAUT model was used to assess oncological patients’ acceptance toward VC in cancer care. Acceptance, operationalized as BI, was determined via three items (“I would like to try oncological VC,” “I would use oncological VC if it were offered to me,” “I would recommend oncological VC to my friends”). Internal consistency for this scale was excellent (Cronbach's α = .93). Further, the three core predictors of the UTAUT model were assessed. SI (by physicians, friends, and family) was preceded through items such as “People close to me would approve of the use of the oncology VC.” Internal consistency was high (Cronbach's α = .83). EE was assessed using five items, such as “The use of oncological VC would not be an additional burden for me.” Internal consistency was high (Cronbach's α = .81). Three items were used to measure PE, including “The use of oncological VC could improve my health condition.” Internal consistency was good (Cronbach's α = .78). Responses were given on a five-point Likert scale (1 = “strongly disagree” to 5 = “strongly agree”).
Statistical analyses
Statistical analysis was conducted using SPSS 26 (IBM, New York) and R (4.1.2). Sum scores were calculated for GR-eHEALS and PHQ-8 and categorized according to the cut-off value. Mean scores were calculated for the scales of digital confidence, digital overload, internet anxiety, and prior knowledge of digital health support in oncology. Mean scores for acceptance (= BI) and its three predictors PE, EE, and SI were calculated. The mean score of acceptance was divided into three categories in accordance with previous research.35,40 Scores from 1 to 2.34 indicate low acceptance, scores from 2.35 to 3.67 indicate moderate acceptance, and scores from 3.68 to 5 indicate high acceptance. Sociodemographic, medical, psychometric and eHealth data were examined using descriptive statistics. Independent t-tests and ANOVAs with post-hoc tests were used to compare differences in acceptance between groups (gender, education, cancer recurrence, and mental illness). Bonferroni correction was used to adjust p-values for multiple comparisons. Levene's tests indicated homoscedasticity. Normal distribution of residuals was assumed due to the given sample size. To examine the drivers of acceptance toward VC in oncology, multiple hierarchical regression analysis was applied. Drivers were included blockwise: (1) sociodemographic data, (2) medical data, (3) eHealth data, (4) internet and VC-related data, and (5) UTAUT predictors. The absence of multicollinearity was verified by the variance inflation factor (VIF), all VIF values were < 3.3. qq-plots of the residuals were visually inspected and showed no signs of violations against normality. Therefore, normal distribution of the residuals was assumed. Homoscedasticity was verified based on a scatter plot of the standardized residuals and the adjusted predicted values. The level of significance was set to α < .05 for all tests. Effect sizes were reported and interpreted according to Cohen, with values around 0.2, 0.5, and 0.8 being considered as small, medium-sized, and large effects, respectively. 41
Results
Study population
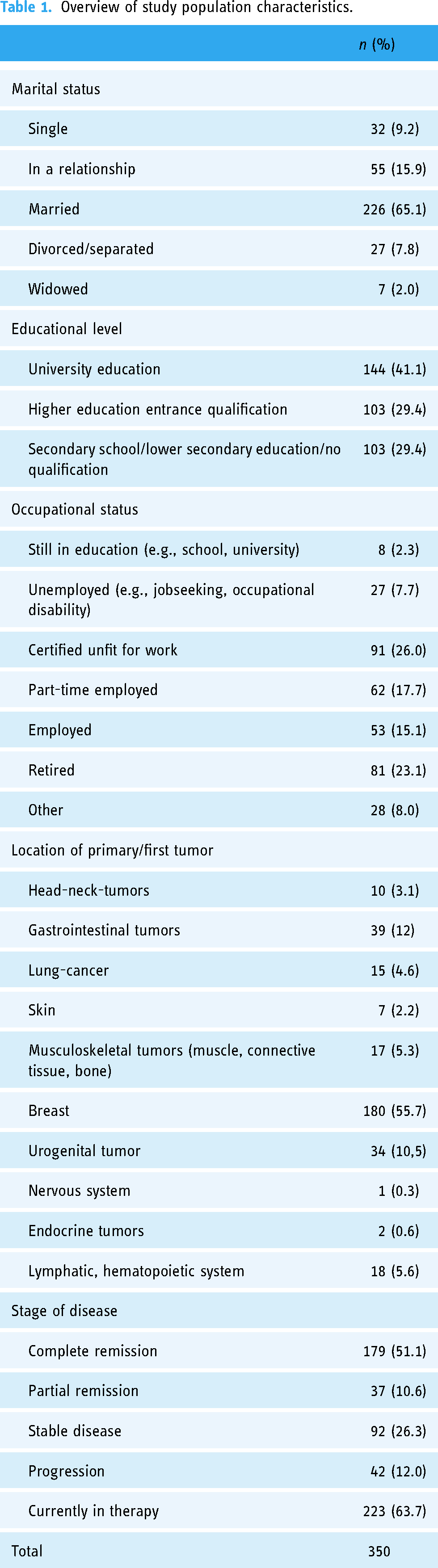
In this population of N = 350 patients with cancer, the mean age was M = 48.96 (SD = 13.72) years. The youngest participant was 19 years old and the oldest was 87 years old. The majority of participants were female (n = 261, 74.6%; male: n = 88, 25.1%; diverse: n = 1, 0.3%).
The mean distance to the attending oncologist was M = 28.52 (SD = 26.18) km. On average, the first cancer diagnosis was received M = 4.66 (SD = 5.48) years ago, ranging from 1.36 months to 46.94 years. 22.9% (n = 80) reported a recurrence of cancer and 40.9% (n = 143) stated metastases of their cancer. 22.29% (n = 78) of the participants were affected by mental illness. PHQ-8 scores, indicating major depressive symptoms, were M = 7.79 (SD = 4.68) on average among cancer patients. 32.6% (n = 114) reached levels above the cutoff score. Cancer patients reported elevated distress levels of M = 6.78 (SD = 2.39). Table 1 gives an overview of the population characteristics.
Overview of study population characteristics.
eHealth-related data and responses toward video consultation
Cancer patients reported high digital confidence (M = 3.81, SD = 1.05), low internet anxiety (M = 1.60, SD = 0.80) and moderate perceived digital overload (M = 2.28, SD = 0.88). Prior knowledge of digital health promotion in oncology was moderate (M = 2.85, SD = 1.08). Table 2 gives an overview of cancer patients’ responses toward VC. eHealth literacy was high among cancer patients (M = 31.12, SD = 6.95). Figure 1 shows the use behavior of the internet and VC for private and professional purposes.
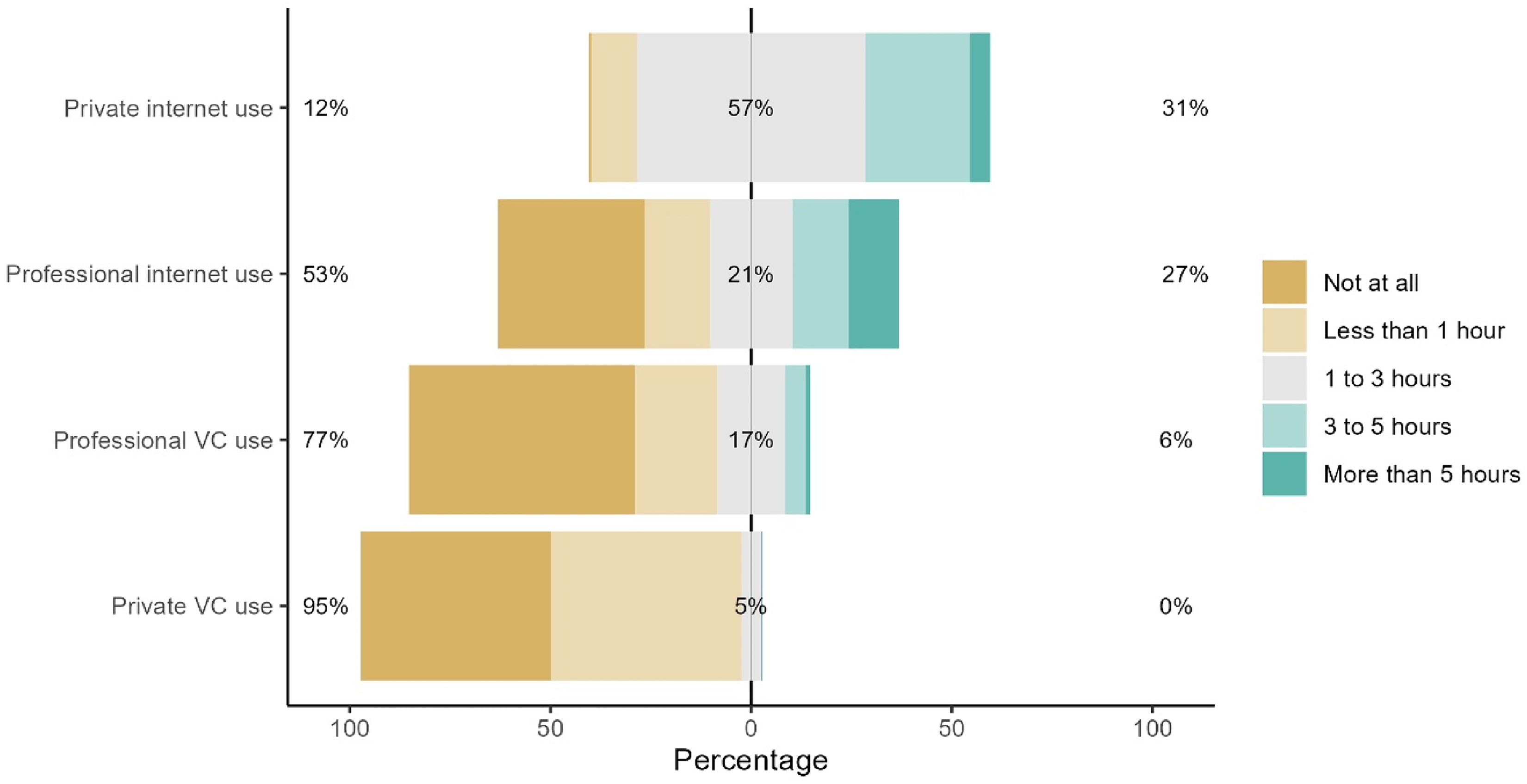
Cancer patients’ use behavior of the internet and VC for private and professional purposes
Cancer patients’ responses toward video consultation in cancer care.

VC: video consultation.
Acceptance of VC in oncology
Overall, acceptance of VC in oncology was high among cancer patients (M = 3.78, SD = 1.18). 56.0% (n = 196) of the population reported high acceptance, 28.0% (n = 98) stated moderate acceptance, and 16.0% (n = 56) of cancer patients indicated low acceptance toward VC.
Female participants reported a significantly higher acceptance toward VC than male participants, t(347) = −4.82, padj < .001, d = .59. Acceptance did significantly differ between different levels of education, F(2,347) = 6.02, padj = .013. Post-hoc tests revealed that participants with no to lower secondary education/other reported significantly lower acceptance than patients with higher education entrance qualification, padj = 0.038, or university education, padj = .002. There was no difference in acceptance between individuals with a mental illness and without a diagnosis, or between patients with cancer recurrence and those without, all padj > .05.
Predictors of acceptance of VC in cancer care
Predictors of acceptance of VC in oncology were determined by multiple hierarchical regression analysis. One participant who reported a diverse gender had to be excluded to ensure the necessary participant number per category.
In the first step, sociodemographic data were included (R2 = 0.135, R2 adj = 0.127, F(3,345) = 17.88, p < .001). Age (β = –.28, p < .001) and Female gender (β = .35, p = .005) were revealed as significant predictors of acceptance. The explained variance was 13.5%.
Medical data were included in the second step (R2 = 0.148, R2 adj = 0.133, F(6,342) = 9.91, p < .001), which significantly increased the explained variance to 14.8% (ΔR2 = 0.13, F(3,342) = 6.47, p < .001). The stage of disease was a significant predictor of acceptance (β = .11, p = .032).
eHealth data, included in the third step (R2 = 0.296, R2 adj = 0.275, F(10,338) = 14.23, p < .001), significantly increased the explained variance to 29.6% (ΔR2 = 0.148, F(4,338) = 71.14, p < .001). All of the included variables were significant predictors of acceptance (Digital confidence: β = .14, p = .010; Internet anxiety: β = −.21, p = .001; eHealth literacy: β = .14, p = .028; Digital overload: β = −.12, p = .022).
In the fourth step, VC and internet-related data were included (R2 = 0.375, R2 adj = 0.352, F(12,336) = 16.78, p < .001), which significantly increased the explained variance to 37.5% (ΔR2 = 0.079, F(2,336) = 45.14, p < .001). Internet use (β = .17, p = .002) and personal trust (β = −.25, p < .001) were significant predictors of acceptance.
In the final step, the three UTAUT predictors were included (R2 = 0.711, R2 adj = 0.698, F(15,333) = 54.49, p < .001). Explained variance of the final model was significantly increased to 71.1% (ΔR2 = 0.336, F(3,333) = 128.78, p < .001). EE (β = .26), PE (β = .24), and SI (β = .34) were significant predictors of acceptance of VC in oncology (all p < .001). Table 3 contains the final UTAUT model of acceptance and its predictors.
Results of the multiple hierarchical regression analysis of acceptance toward VC in cancer care.

Note. N = 439. To examine the drivers of acceptance toward VC in oncology, operationalized as behavioral intention, multiple hierarchical regression analysis was applied. Drivers were included blockwise in five steps. In steps 2, 3, 4, and 5 only the newly included variables are presented. B: unstandardized beta; β: standardized beta; T: test statistic; R²: determination coefficient; ΔR2: changes in R2; PHQ-8: Patient Health Questionnaire Depression Scale; VC: video consultation.
Discussion
The purpose of the study was to determine the acceptance of VC and influencing factors among patients in cancer care. While other studies have portrayed utilization and acceptance of VC among cancer patients in general and during the COVID-19 pandemic, there have been few regarding drivers and barriers of acceptance to date.19,42–46 Moreover, this issue has not been considered from the perspective of the UTAUT model. To our knowledge, no valid information regarding the acceptance and influencing factors is existing.
Overall, acceptance of VC was high among cancer patients. More than half of the participants indicated high acceptance, and nearly a third reported moderate acceptance. These findings correlate with previous studies of telehealth in oncology.42,47 At the onset of the COVID-19 pandemic, Wehrle et al. observed a higher preference for in-person visits among cancer patients. 48 The contrast to the results of this study, which were collected rather later in pandemic, may be due to initial uncertainty with this type of eHealth intervention. Similarly, other research suggests a positive impact of the pandemic on improving the uptake of telehealth and VC. 21 Moderate to high acceptability to eHealth interventions has also been demonstrated among other medical fields like cardiology, psychodiabetology, in patients with chronic pain, at general practitioners’ offices, among patients with obesity and with post-COVID-19 syndrome.33,35–38,40,42,47,49 Different drivers and barriers for acceptance could be identified, which are discussed below.
Sociodemographic parameters could be determined as having an impact on the acceptance of oncological VC. Female participants exhibited a significantly higher acceptance rate compared to males. By contrast, in a cross-sectional study that examined the experience of teleoncology, willingness to use VC was lower among women, especially breast cancer patients. 42 Whether gender, in general, is an influencing factor is discussed controversial in literature.37,38,50–52 Some studies suggest that women are more willing to use eHealth services, while others report this to be more applicable for men.
The results indicate a significantly higher acceptance toward VC among participants with higher educational backgrounds, as shown in prior studies.50,51,53 This could be due to a greater familiarity with eHealth interventions and ICT, both in terms of knowledge and experience among people with higher levels of education. 50 In addition, eHealth literacy is often lower for less educated patients which could also be associated with lower adherence to telehealth.50,54 This may indicate that patients with higher educational levels are generally more likely to take part in online research and are therefore more willing to use ICT and VC.55,56
In contrast to other research, mental illness was not found to be a driver of acceptance.35,38 In the context of e-mental health programs, the strong association between mental illness and acceptance may be explained by the fear of stigma for attending psychotherapy, which can be reduced using eHealth offerings.51,57,58 With regard to cancer care, stigmatization may have been a less influential factor for the participants.
Another driver of acceptance was age. Younger participants demonstrated higher acceptance than those who were older. A similar association can be found in several other studies of general acceptance of digital health services.37,42,53 Potential reason for lower uptake could be a requirement for greater support in using VC. 50 Older age is also related to less widespread internet access, lower eHealth literacy, and fundamentally lower usage of online services in general.43,59 This relationship may be based on greater doubt about privacy issues and data security.59,60 In an aging society, these barriers have to be reduced to make VC more accessible to become a successful enhancement to cancer care.
In terms of patients’ medical data, the stage of the disease was also a significant driver of acceptance. Half of the participants were in complete remission of their disease, which may indicate that cancer survivors in particular have a high acceptance to use of VC. A systematic review by Cox et al. also shows a preference to use telemedicine for further care in order to minimize the burden of treatment and disruption to daily life after fighting cancer. 44 In addition, this type of care has the potential to save time and costs for patients. Both in view of the completed treatment, but also a current therapy, which is often considered a very distressing time, these patients may then prefer care that can also be carried out at home.
eHealth-related data were also identified as significant drivers of acceptance. Internet anxiety describes general concerns or fears about using the internet. 61 Participants reported low internet anxiety and high digital confidence. Digital overload represents a form of technology overload, which can be considered a general overwhelm due to digital availability and was reported as moderate, matching the high level of private and professional internet use reported. 62 Obviously, this basic approach to internet usage already has a significant influence on acceptance. High digital overload might lead patients to avoid spending more time than necessary with technical devices related to health care. However, considering that it was revealed as moderate, this possibly indicates a higher willingness to use VC. Other studies have previously shown that higher internet anxiety is associated with lower acceptance and that confidence in digital media provides another key factor for acceptance.34–36,42,63 In this context, high internet anxiety may lead to increased uncertainty about eHealth interventions and thus negatively affect acceptance. A systematic review of VC in oncology suggests that patients’ unease about new technologies is a relevant hindrance to the introduction of new online services. 19 Video utilization might represent additional technical difficulties compared to a telephone-only consultation.23,64 Further, digital overload and technology fatigue may have a negative impact on the acceptance of online services.35,53,65 Simultaneously, participants’ high eHealth literacy as another significant driver might be used to enhance their confidence and belief in VC. The ability to find, use and evaluate health information on the internet could improve digital confidence and reduce internet anxiety, and therefore directly influence the acceptance of VC. 38
High general internet use among the participants and personal trust in this form of physician contact present themselves as significant drivers of acceptance. Regarding internet and VC-related data, respondents would be most likely to use the VC for minor, unproblematic concerns, the issuance of a prescription or to discuss diagnostic findings. The willingness to attend an initial consultation via VC was rather low. This suggests that this form of medical interaction in oncology is not suitable for all concerns, but can serve facilitating purposes. 42
Similar to previous studies, the UTAUT model has shown a high value for predicting the acceptance of eHealth interventions.33–36,53 The UTAUT model with its three factors PE, EE, and SI demonstrated a significant impact on acceptance, explaining a high level of variance. Other studies present PE as the strongest core predictor matching the high influence of PE on acceptance as found here.27,34,35,37,53 By contrast, SI appeared to be the predictor with the highest effect in this study. A large proportion of cancer patients stated that they would be more likely to use VC if important caregivers recommended it. However, these divergent results might be explained by all core predictors showing a strong effect in this study. The high influence of effort expectancy shows again the importance of easy usability and low effort in daily routine.38,53 This would be especially beneficial for patients with limited experience using ICT.
Practical implications
Based on the identified drivers and barriers of acceptance, valuable information for the clinical application of VC in cancer care is obtained. Initially, according to the high level of acceptance found here, VC appears to be an appropriate supplement for clinical practice in oncology and should be offered more comprehensively. Since acceptance was higher among women, male patients should be approached in a targeted manner in order to familiarize them with the service. This also applies to elderly patients as well as those with lower levels of education. Barriers arising from age, education, and lower eHealth literacy require special consideration and might be improved with specific support, for example, in the format of guided tutorials and promotion of eHealth literacy. Here, providers should ensure easy access and provide clear instructions in advance to keep EE as low as possible and not impose an additional burden on patients’ daily lives. In order to make the VC service user-friendly, further studies should examine which framework conditions and preferred modalities of usage such as timing, duration and frequency are required to facilitate usage and overcome technical barriers. This may also address possible hindrances such as internet anxiety or digital overload. If problems are encountered with video usage, it may be useful to offer a telephone consultation as an alternative for VC. Attention should also be paid to the great influence of the SI. Strategies to further increase acceptance might start here, for example, with providers directly suggesting the use of VC to their patients.36,53 Furthermore, the benefits and advantages of VC could also be highlighted along with this to simultaneously address PE as a significant predictor. Subsequently, the findings should be used to examine how this new approach can be optimally integrated into everyday clinical practice in order to improve patient-centered cancer care. Following the establishment of VC, its acceptability should be reexamined. Lastly, teleoncology and VC may not only benefit patients in Germany but also provide several opportunities to improve and support cancer care all over the world, especially in countries with structurally weaker healthcare system.66,67 eHealth offerings like VC have already been implemented in cancer care in several other countries and are growing, especially since the pandemic.21,42,66–70
Limitations
Due to the online implementation of the survey, sampling bias needs to be considered, as individuals who lack internet access or the necessary devices might have been excluded. Previous studies have found that this mainly applies to elderly people and those with a lower level of education.71,72 In addition, people with higher levels of digital confidence and less fear of the internet were approached in this way. As a result, they may have been more willing to use the VC. Besides that, the proportion of female participants, and in turn breast cancer patients, predominates. This unequal gender distribution could restrict the evaluation of a gender effect. 37 Consideration must be given to the fact that the mean age of participants was younger than the average age of the first diagnosis. The exact place of residence of the patients was not queried in this study to guarantee anonymity and should be considered again in subsequent studies. Overall, the generalizability of the results may be limited by these sampling biases. However, since the study examines sociodemographic influences on acceptance, the present results also provide an indication of which subgroups need to be approached more strongly for new eHealth offerings. Since acceptance was operationalized as the intention to use VC, the intention-behavior gap needs to be considered.73,74 This phenomenon shows that the mere intention to do something does not necessarily result in actual behavior. However, it should be taken into account that more than half of the participants were previously uninformed about VC in oncology and how to use it. Therefore, the examination of the actual usage behavior and adherence is still outstanding. Furthermore, the collected data are self-reported and susceptible to common method variance.75,76 This should be mitigated by assuring the anonymity of the survey and the sufficient internal reliability of the items. To overcome these limitations, future studies on VC in cancer therapy should survey a higher number of elderly people and people with lower education levels, as well as more male patients. Whether there is a difference in acceptance among patients with visual or hearing impairment has not been assessed in this study. This could be a relevant barrier and should also be investigated in future studies. Moreover, in the context of the intention-behavior gap, the actual usage patterns of telemedicine should be investigated in the future. Ideally, such research should be conducted after the COVID-19 pandemic in order to look at acceptance outside of this exceptional situation and its impact on ICT usage behavior.
Conclusion
To conclude, the study revealed a high acceptance among cancer patients towards VC as a viable supplement to personal visits to an oncologist. With regard to the present findings, it is clear that a wider implementation of VC as a complement in cancer therapy should be considered. For that, existing barriers, especially for the elderly, need to be improved to accommodate the needs and abilities of all patients. In the context of the high impact of SI demonstrated here, it becomes apparent that caregivers can have a direct influence on acceptance. This could improve and facilitate future forms of therapy, especially when in-person contacts need to be limited.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231222108 - Supplemental material for Drivers and barriers of patients’ acceptance of video consultation in cancer care
Supplemental material, sj-docx-1-dhj-10.1177_20552076231222108 for Drivers and barriers of patients’ acceptance of video consultation in cancer care by Angelina Nurtsch, Martin Teufel, Lisa Maria Jahre, André Esber, Raya Rausch, Mitra Tewes, Christoph Schöbel, Stefan Palm, Martin Schuler, Dirk Schadendorf, Eva-Maria Skoda and Alexander Bäuerle in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgments
We thank the Open Access Fund of the University of Duisburg-Essen for supporting the publication of our article. We thank Deborah Friedman for proofreading and linguistic assistance.
Author contribution
conceptualization: A.B., A.N., and M.T.; data curation: L.M.J.; formal analysis: L.M.J.; methodology: A.B. and L.M.J.; project administration: A.B. and A.N.; supervision: A.B., E.-M.S., and M.T.; visualization: L.M.J.; writing—original draft: A.N., L.M.J., and A.B.; writing—review and editing: A.N., M.T., L.M.J., A.E., R.R., M.T., C.S., S.P., M.S., D.S., E.-M.S., and A.B. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Medical Faculty of the University of Duisburg-Essen (19-89-47-BO). Electronic informed consent was mandatory.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.