
Abstract
Introduction
Telemedicine is being used in an increasing number of healthy lifestyle intervention studies in preventive cardiology. However, the optimal telemedicine-based approach for patients with cardiovascular disease remains unclear. Therefore, the aim of this systematic review is to identify which design features are associated with the acceptance and efficacy of telemedicine in this specific patient population.
Methods
The databases PubMed/MEDLINE, Embase and the Web of Science Core Collection were searched from 5 October 2010 to 5 October 2020. This systematic review only included randomized controlled or quasi-randomized controlled trials with a comparator to a telemedicine-based intervention group and a designated measure of adherence. We adopted a narrative synthesis approach to define telemedical design features, which were clustered into three main categories (social, exercise related and barrier removal) and compared to adherence (graded as good, medium and bad) and primary outcomes (significant improvement, no significant change).
Results
We screened a total of 865 records, of which 14 were included in this review, containing 13 identified design features. In 8 studies (57.1%), adherence was graded as good (4 studies medium, 2 studies bad). A positive primary outcome occurred in 10 (71.4%) studies. Personal contact showed the most pronounced (while not statistically significant) positive association with adherence and study outcomes.
Conclusion
Given the remote nature of telemedical lifestyle intervention studies, including recurring personal contact in the intervention seems to be a key factor in ensuring that adherence levels remain comparable to those seen in centre-based interventions.
Introduction
There is a growing body of research postulating various potential benefits linked to a healthy lifestyle and specifically physical exercise in the field of preventive cardiology. Studies show that maintaining a healthy lifestyle at midlife is associated with an increased life expectancy, while also reducing the occurrence and progression of major chronic conditions, such as cardiovascular disease (CVD) and type 2 diabetes mellitus (T2DM). 1 In lifestyle intervention research (i.e. interventions focusing on the variables of physical activity (PA) and nutrition), the clinical outcomes regarding the prevention and progression of chronic diseases can be significant when participants closely adhere to the programmes, yet adherence to exercise interventions over an extended period of time is generally low, particularly in older populations with pre-existing health conditions.2,3 This issue is even more pronounced during home-based exercise interventions, where adherence tends to be inferior compared to centre-based interventions. 4
Here, telemedicine offers an avenue of addressing this problem. For home-based interventions, telemedicine has been shown to increase patient adherence when compared to studies not utilizing telemedical concepts. 4 However, the typical patient with CVD is of advanced age and often struggles with telemedical concepts, seeing how technology adoption and willingness to work with new and unknown devices is often low in elderly patient populations. 5 Evidently, the optimal telemedical approach in healthy lifestyle intervention studies focusing on CVD patients remains unclear.
To our knowledge, there are no studies that assess how telemedicine impacts adherence to healthy lifestyle interventions. Therefore, the aim of this systematic review is to address this research gap by identifying design features that are associated with the acceptance and efficacy of telemedicine in CVD patient populations, further evaluating how adherence is being measured in settings, where the participants are not actually on site during the intervention.
Methods
This systematic review follows best practice recommendations from the Cochrane Collaboration
6
and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement.
7
The review protocol was registered in the International Prospective Register for Systematic Reviews with the registration number CRD42020209851. Further, this review employs the definition of telemedicine from the World Health Organization (WHO)
8
: “[Telemedicine is] the delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities”.
Literature search
The search was conducted using three databases: PubMed/MEDLINE, Embase and the Web of Science Core Collection. Results were limited to English journal articles published from 5 October 2010 to 5 October 2020. The applied search terms varied slightly between databases. The exact search term in PubMed/MEDLINE was: ‘(telemed*[Title/Abstract] OR tele med*[Title/Abstract] OR telehealth [Title/Abstract] OR tele health [Title/Abstract] OR mobile health[Title/Abstract] OR mHealth[Title/Abstract] OR eHealth[Title/Abstract] OR mobile med*[Title/Abstract]) AND (lifestyle[Title/Abstract] OR exercise[Title/Abstract] OR physical activity[Title/Abstract] OR training[Title/Abstract]) AND (intervention[Title/Abstract] OR prospective[Title/Abstract]) AND (cardiovascular [Title/Abstract] OR cardiology [Title/Abstract] OR cardia* [Title/Abstract] OR CVD [Title/Abstract] OR heart [Title/Abstract] OR diabet* [Title/Abstract] OR obese* [Title/Abstract] OR overweight [Title/Abstract]) AND (compliance OR adherence OR acceptance OR efficacy OR adoption)’.
Eligibility criteria
Eligible studies involved participants with or at risk of CVD (as defined by overweight or T2DM). We included only randomized controlled or quasi-randomized controlled trials which had to include a comparator to the telemedicine-based intervention group and a measure of adherence. Studies were excluded if they focused on children and adolescents, pregnant women or other special populations, non-lifestyle-related factors such as medication adherence, or if the chosen adherence measure could not be graded. Furthermore, we excluded studies if part of the intervention occurred after 11 March 2020, the date on which the WHO declared COVID-19 a pandemic, to eliminate the influence that the pandemic ensued on the adherence of ongoing interventions.
Study selection and data extraction
Two authors independently screened titles and abstracts, rating them with either ‘yes’, ‘no’ or ‘unsure’ regarding their potential inclusion in the review. The authors were blinded to each other's decisions, articles only being excluded if both rated them with ‘no’. Both authors then read the remaining articles in full and screened them in detail for the described eligibility criteria. Consensus between authors had to be reached for an article to be included in the review.
For each included study we then extracted descriptive data regarding methodology and study design, patient population, intervention components, adherence measures as well as the identified design features. We further extracted specific secondary outcomes, regarding weight loss, PA and exercise capacity.
Data synthesis and risk of bias assessment
This review adopted a narrative synthesis approach as described by Popay et al.
9
to define telemedical design features which are associated with patient adherence and consequently intervention success, following the recommendations by the Synthesis Without Meta-analysis reporting guideline.
10
For further explorative analysis and to allow better quantification of the impact that these design features had on primary study outcomes and adherence, risk ratios (RR) were calculated and tested for significance via two-tailed Fisher exact probability test Meta-analysis was deemed as unfitting due to data heterogeneity. Two authors independently evaluated each individual study and rated the adherence as good, medium or bad. Given the wide range of reported adherence measures and their consequently difficult comparability, the grading process itself was qualitative in nature. However, to be graded as good at least 67% of the utilized adherence measure had to be reached (a cut-off established in prior lifestyle intervention studies.11,12
Results
Study selection
A PRISMA flow diagram is shown in Figure 1. The deployed search strategy yielded 865 records, of which 591 remained after the removal of duplicates. After title and abstract screening, 77 articles were read in full, of which 14 [n = 1284, mean number (range) of participants 92 (36–171)] were included in this review (Table 1). Furthermore, we conducted a post hoc literature search adding ‘cholesterol [Title/Abstract]’ and ‘hypertens* [Title/Abstract]’ to the initial search terms (both for Title/Abstract). This yielded an additional 15 articles (11 on hypertension, 4 on cholesterol), of which none would have been included in this review (due to either not meeting the inclusion or meeting our exclusion criteria).

Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram.
Included studies.
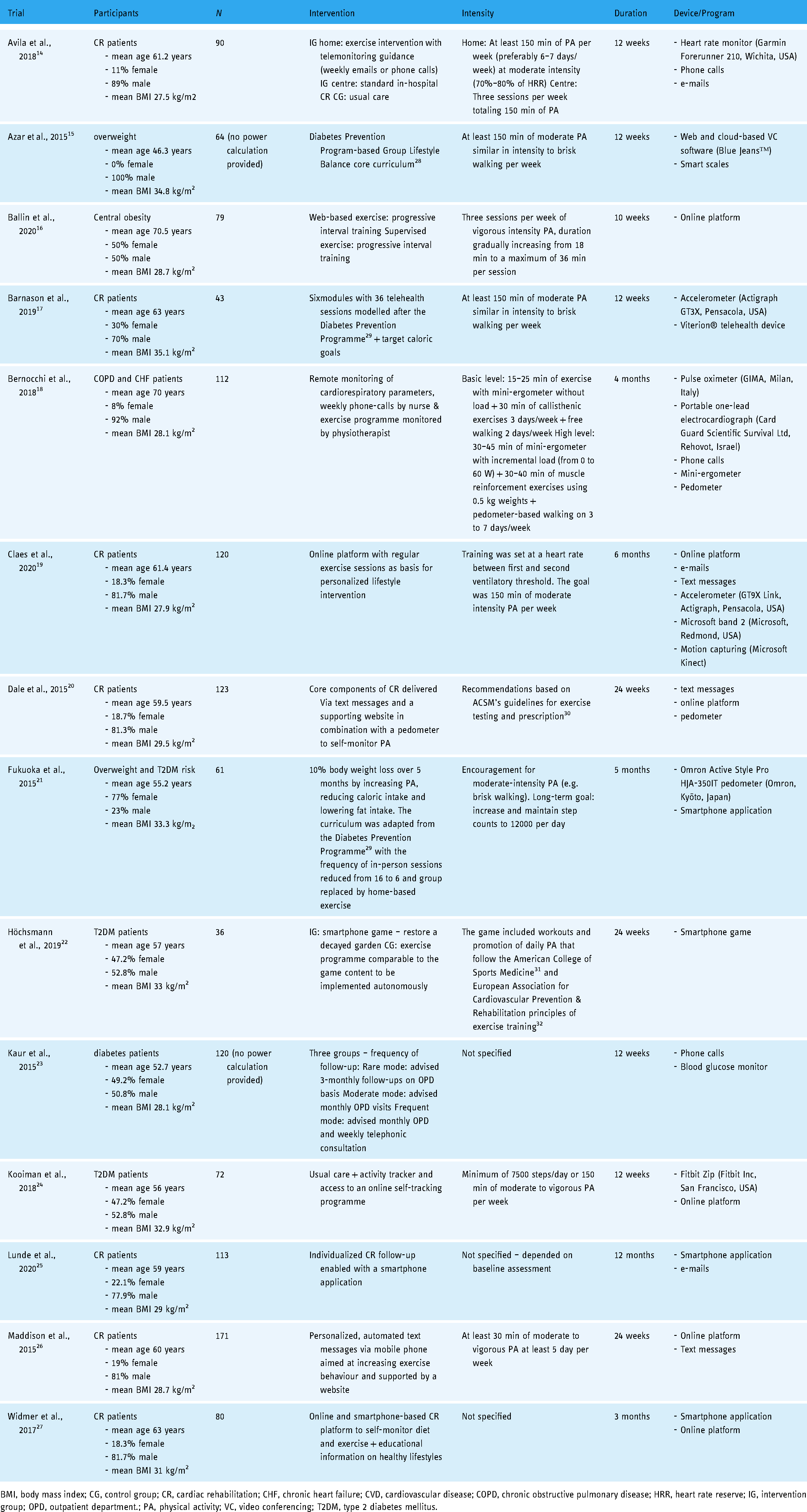
BMI, body mass index; CG, control group; CR, cardiac rehabilitation; CHF, chronic heart failure; CVD, cardiovascular disease; COPD, chronic obstructive pulmonary disease; HRR, heart rate reserve; IG, intervention group; OPD, outpatient department.; PA, physical activity; VC, video conferencing; T2DM, type 2 diabetes mellitus.
Risk of bias
The results of the quality assessment are highlighted in Table 2. All of the included randomized controlled trials were assessed as high risk of bias regarding the lack of blinding of participants and personnel. This is however a common problem and difficult to achieve in the field of exercise interventions. The other cases of high risk were assessed in the domain of other biases, where four studies did not register their trials in any online registry and one study only did so retrospectively.
Risk of bias assessment using version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB2).

+ , low risk; ∼, some concerns; - , high risk and ?, uncertain risk.
Contents and outcomes of telemedical interventions in preventive cardiology
Table 1 offers a brief description of the main intervention contents of the included studies. Overall, it is evident that telemedicine is a very heterogeneous concept ranging from simple text messages to complex motion capturing. The most common intervention components were:
online platforms (6 out of 14 studies), activity trackers (6 out of 14 studies), smartphone applications/games (4out of 14 studies), text messages (3 out of 14 studies), e-mails (3 out of 14 studies) and phone calls (3 out of 14 studies).
The reported outcomes of the included studies are presented in Table 3. Notably, 10 out of 14 studies (71.4%) reported a significant difference in the primary outcome between groups. Regarding the chosen secondary outcomes, 9 studies reported on changes in weight and of those, 5 (55.6%) reported significant between-group differences. Daily PA was reported by 10 studies, six (60%) reporting a significantly higher change in the intervention group. Lastly, changes in cardiovascular fitness, as assessed by peak V˙O2, were reported by five studies of which two (40%) reported significant between-group differences.
Included studies – outcomes.

+ , significant improvement; ∼, no significant change; CVD, cardiovascular disease; ED, emergency department; PA, physical activity; V˙O2, oxygen uptake; 6MWT = 6-min walking testand.
Adherence measures and design features of telemedical interventions
Table 4 shows how adherence was measured in the included studies and the different design features which could be identified. In eight studies (57.1%), adherence was graded as good, in four (28.6%) as medium and in two (14.3%) as bad. Of the included studies, 10 (71.4%) utilized an objective measure of adherence while 4 (28.6%) relied on self-reported measures. Further, only 2 (14.3%) of the included studies took into account some dimension of intensity when analysing adherence, whereas the remaining 12 (85.7%) contented with what could more aptly be described as measures of attendance.
Design features and adherence of telemedical intervention studies.

CG, control group; CR, cardiac rehabilitation; CPET, cardiopulmonary exercise test; HRR, heart rate reserve; IG, intervention group; OPD, outpatient department; PA, physical activity.
Regarding the impact of adherence on primary study outcomes, out of the 10 positive studies, 7 (70%) was graded as good, 2 (20%) as medium and 1 (10%) as bad with respect to the reported adherence levels. For the four neutral studies, one was graded as good (25%), two as medium (50%) and one as bad (25%).
How the various design features impacted the reported adherence levels can be seen in Table 5. Based on the extracted data, we divided design features into three categories:
a. social, b. exercise related and c. barrier removal.
Design features and adherence of telemedical intervention studies – data synthesis. Two-tailed Fisher exact probability test was utilized to calculate p-values for the observed risk ratios (RR).
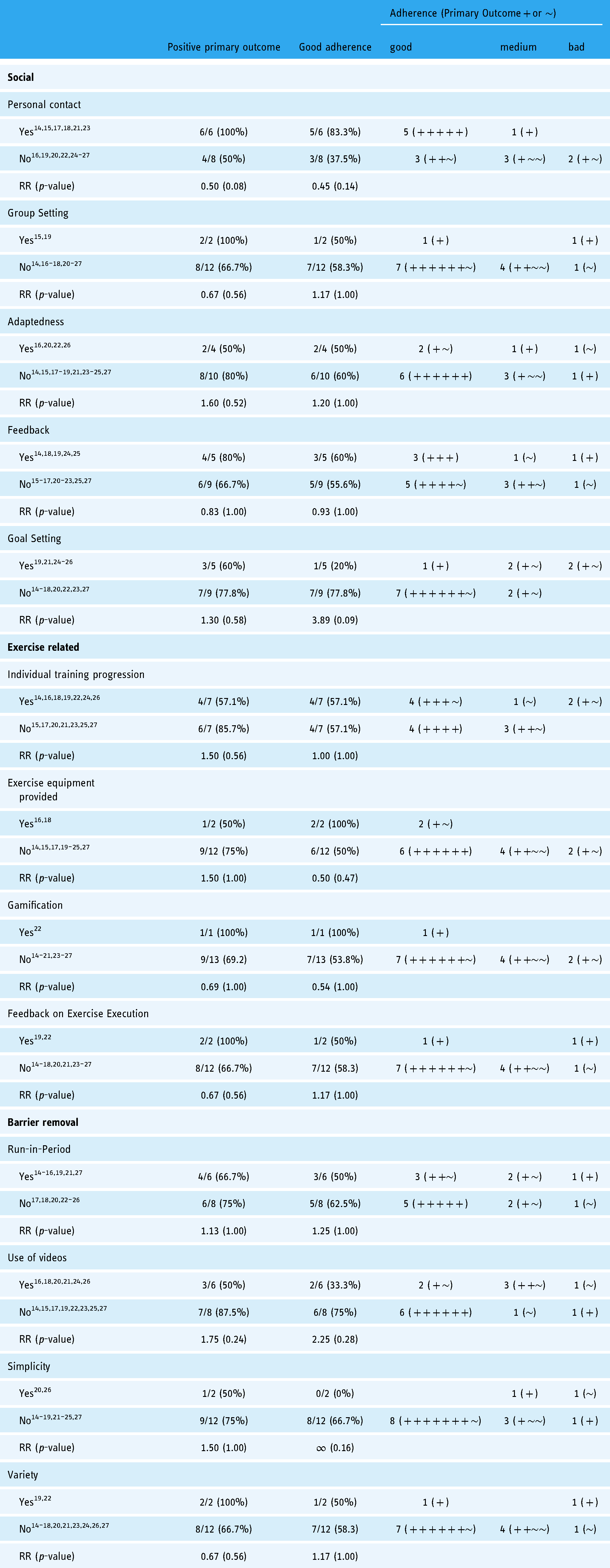
The most pronounced positive association between identified design features and adherence could be observed if the intervention included ‘personal contact’ with the study personnel (i.e. not only communicating via text but also implementing in-person sessions, phone calls, video chats, etc.). Studies that included personal contact reported good adherence levels in five out of six cases (83.3%) compared to three out of eight (37.5%) in the studies which did not include this design feature. Receiving regular feedback on the individual progress during the intervention was associated with good adherence levels in three out of five (60%) studies compared to five out of nine (55.6%) in the remaining studies. On the other hand, allowing participants to set their own goals and thereby independently track intervention progress seemed to be inferior in improving adherence [one out of five (20%) compared to seven out of nine (77.8%) studies].
Regarding the design of the exercise part of the intervention, one feature was providing participants with individual progression instead of using a ‘one size fits all’ approach. This feature took into account the results of baseline assessments (e.g. CPET, 6MWT) to plan incremental exercise adjustments over the course of the intervention. However, this was not associated with an increased adherence. Regardless of whether this design feature was applied, adherence levels were graded as good in four out of seven studies (57.1%). Offering alternatives to standard cardio exercises or strength training with the own body weight via the provision of exercise equipment was a further design feature implemented in two of the included studies. In both studies, adherence levels were graded as good. Another design feature related to the form in which the exercise intervention was delivered. Here, a newly developed smartphone game was implemented in one study, resulting in good levels of patient adherence. Additionally, utilizing phone sensors allowed to deliver specific feedback on exercise execution – a feature that one more study implemented via external hardware. However, in the latter case, the adherence levels were subpar.
Removing common barriers towards adherence was another group of identified design features. The implementation of a run-in period was associated with good adherence levels in three out of six studies (50%). Yet, these levels were inferior when compared to studies that did not include this design feature, where we graded five out of eight (62.5%) with good adherence levels. Another identified design feature was the use of educational videos to deliver intervention content, this, however, yielded positive adherence levels in only two out of six (33.3%), compared to six out of eight (75%) studies that did not implement this feature.
Patient and study design characteristics and association with adherence and primary outcomes
Participants weighted mean age and body mass index (BMI) were 59.9 years (range of mean age 46.3–70.5) and 29.8 kg/m2 (range of mean BMI 27.5–35.1), respectively. Given the limited sample of 14 studies, testing for association or correlation between the dependent categorical variables adherence and study outcome as well as the independent continuous variables sample size, age and BMI would not yield meaningful results. However, dividing the included studies into two groups according to sample size, age and BMI allows for a qualitative description of how the adherence levels and primary outcomes are distributed (Table 6). Additionally, we also divided the included studies into two groups regarding their duration, CVD status of the included patients as well as their biological sex distribution.
Patient and design characteristics of included studies and association with adherence and primary outcomes.

BMI, body mass index; CVD, cardiovascular disease.
Adherence was graded as good in five out of seven studies (71.4%) in the lower compared to three out of seven (42.9%) in the higher BMI group. Regarding primary outcomes, significant effects were reported by four out of seven studies (57.1%) in the lower compared to six out of seven (85.7%) in the higher sample size group, the contrary being true for age (85.7% lower compared to 57.1% higher). For BMI, no differences could be observed regarding the significance of primary outcomes. Looking at duration, adherence levels were higher in shorter interventions (71.4% compared to 42.9%), while primary outcomes were positive in 85.7% of the longer compared to 42.9% in the shorter studies. Similarly, while primary outcomes were positive in six out of eight (75%) studies with CVD patients compared to four out of six (66.7%) studies with at-risk patients, adherence was higher in the at-risk (66.7%) than in the CVD (50%) patient studies. Regarding the biological sex distribution, both primary outcomes and adherence were positive (respectively rated as good) in 60% of the not predominantly male studies. For the predominantly male group, positive outcomes were reported by seven out of nine (77.8%) and adherence was graded as good in five out of nine (55.6%) studies.
Discussion
Telemedicine is likely to play a key role in future healthcare provision, allowing an avenue to supervise patients at home and thereby not only reducing the burden on study participants but also physicians and scientists.
33
Numerous studies show that telemedicine can significantly reduce both the cost related to upholding an intervention programme, as well as reducing the travel time which is often linked to the participation in intervention studies and especially important for rural patient populations
Looking at the identified design features, it is noticeable that there is a deviation when it comes to the impact they had on adherence when compared to the main study outcomes, as highlighted in Table 5. The RR reveal noticeable divergences – and while none of them were statistically significant (due to the limited study sample), they allow for an explorative comparison of the individual design features. While for features such as personal contact (RR – primary outcome = 0.50, RR – adherence = 0.45) and regular feedback (RR – primary outcome = 0.83, RR – adherence = 0.93) a reduction in risk for a non-significant primary outcome and bad adherence can be observed, other features such as group setting (RR – primary outcome = 0.67, RR– adherence = 1.17) and individual training progression (RR – primary outcome = 1.50, RR – adherence = 1.00) show more inconsistent effects.
This could indicate four things:
The intervention had no effect on the primary outcome or the latter was not suitable to detect relevant changes over the observed time period. There were methodological limitations that prevented the detection of statistically significant differences between groups (e.g. the study was underpowered). Adherence did not play a major role in the effect of the intervention, that is, even a low adherence rate was sufficient to induce significant effects. Some adherence measures were chosen in a way, that they did not sufficiently capture the relevant dimensions of participating in the interventions.
One apparent limitation of commonly used adherence measures in telemedical interventions is that they are often self-reported by study participants.16,18,20,23 Additionally, most objective measures only evaluate patient attendance without including any measures of intensity or effort.15–21,23–27 In most cases they capture if interventions are being used, but not to which extent regarding duration, intensity, total energy expenditure or other variables. Additionally, there are studies where adherence measures did not seem to be pre-specified and sometimes arbitrarily chosen.
24
Consequently, there is an apparent need to establish gold-standard adherence measures which are objectively collected and consider variables such as duration and intensity towards the exercise part of the intervention.
Looking at the reported adherence levels of the included studies, especially when taking into account the corresponding primary intervention outcomes, the variable of personal contact emerged as the most important design feature in telemedical interventions. While telemedicine can be very practical and facilitate many processes, especially elderly patients, who are often not too familiar with the use of novel technologies, can perceive telemedical intervention concepts as impersonal. 35 This is especially relevant for this review, seeing that the mean age of all participants was 59.9 years. In this age group, having recurring interactions with a dedicated contact person can counteract this problem, serving as a reminder for the patient that even while at home, their progress is continuously monitored.
Finding the balance between a simple yet engaging intervention design presents an important challenge. When presented with a choice, patients often prefer receiving intervention content by simple means such as text messages rather than having to learn how to utilize an online platform or a smartphone application.26,27 Similarly, interventions becoming almost
When designing a telemedical intervention for a specific population, the technology-focused form of delivery needs to be balanced by trying to keep the contents as age-adapted and appropriate as possible. Currently, a lot remains to be learned on this topic, which is reflected in the results regarding the identified design feature of ‘adaptedness’. Here, studies not including any aspects of adaptedness performed better regarding both primary outcomes and patient adherence, when compared to the studies that did include this feature. Yet, as only four studies even took into consideration any dimension linked to adaptedness (e.g. using age-appropriate actors for educational videos) these results have to be interpreted with caution, given the apparent amount of unexploited potential. Conversely, we argue that there remains huge potential to improve adaptedness in future telemedical intervention studies. For example, one study 22 chose a gardening setting for their smartphone game to improve PA since this activity is among the favorite in the participating age group – and this choice proved to be very successful.
Another design feature that requires further attention is the application of a run-in period into the study. Even though we expected this feature to increase adherence levels, this was not confirmed in the present review (RR = 1.25). Again, this might be linked to the limited number of included studies – yet, we argue that similar to designing a successful intervention study, designing an adequate run-in-period requires additional attention and might be more complex than a simple one-off explanation of a technical device to a patient. Therefore, the mixed results in adherence levels of studies that applied this design feature might be explained by the actual procedures of the deployed run-in-periods. Consequently, how to design run-in-periods could be an interesting topic of future research.
Looking at the patient and design characteristics of the included studies, there emerge some notable points. Only one study on patients with manifest CVD did not have a majority of male participants, while in at-risk patient populations most studies were balanced regarding the biological sex distribution with only one study being 100% male and another being predominantly female. This further highlights the problem of the generalizability of findings in CVD studies, where included patients are often predominantly male. According to a recent review, adherence to lifestyle intervention trials is higher in males compared to females. 36 In contrast, in the present review, adherence levels were similar between studies with and without predominantly male patient populations. For the primary outcomes, on the other hand, 77.8% of the predominantly male studies reported a positive primary outcome compared to only 60% in the no-predominantly male group. Given the limited number of female participants and the lack of direct comparisons in the included studies, it is not possible to draw meaningful conclusions regarding differences in primary outcomes between men and women. However, it emphasizes the need to consider and evaluate potential gender differences in telemedical interventions.
Regardless of sex, long-term adherence is a typical problem in lifestyle intervention trials, which requires further investigations to induce sustainable changes in clinical outcomes. Interestingly, even though adherence does seem to decrease with increased length of the intervention, primary outcomes were positive more often in longer duration studies. This underlines that for many study endpoints (e.g. weight reduction) there is minimum amount of time needed to achieve significant results. On the other hand, the deviation between adherence and outcomes emphasizes the question of whether currently utilized and reported adherence measures are suitable to capture the extent to which interventions are being used.
Lastly, due to the exploratory nature and the non-significant findings of this review, no clear conclusion can be drawn about which aspects of a study design are most important. However, we would strongly recommend the implementation of personal contact in every telemedical intervention. Other design features should be considered based on the population and aims of the trial.
Limitations
Due to the limited number of published studies and the large variety of reported adherence measures, it was not feasible to perform a meta-analysis. Therefore, the results should be interpreted as exploratory findings. Also, it was not possible to clearly rank the importance of the identified design features as most studies included more than one feature. It is unclear whether design features really had a causal impact on adherence or outcomes. It is possible that some design features were coincidentally associated with adherence and outcomes or that other factors played a more important role (e.g. methodological limitations). Moreover, this review did not include any studies which focused primarily on the topics of alcohol and smoking cessation, since those face their own and very specific challenges when it comes to patient adherence. Yet, since alcohol consumption and smoking represent two key factors in healthy lifestyle research, results regarding these variables would be of great interest for future research. Additionally, while all included studies pertain to the field of preventive cardiology, differences between the reported primary outcomes and observed patient populations add additional difficulty in analysing intervention adherence levels. Same is true regarding the heterogeneity of the included telemedical interventions. Furthermore, given the qualitative approach as well as the exploratory nature of this review, the limited number of included studies and the non-significant results, all of the reported results have to be treated with a certain degree of caution. Lastly, while we excluded studies if part of the intervention occurred after the beginning of the COVID-19 pandemic to eliminate the influence that it ensued on the adherence of ongoing interventions, the pandemic has also caused a dramatic increase in the use of telemedicine, which led to severe changes in CVD patient care. Analysing how the pandemic impacted the development and implementation of telemedicine in patient care might be of great interest for future research.
Conclusion
Even (or especially) in telemedicine, recurring personal contact seems to be a key factor in ensuring that adherence levels remain comparable to those seen in centre-based interventions. Yet, much remains to be done in the area of adaptedness (i.e. adapting the intervention for a particular target population), where an optimal intervention design for a CVD patient population remains to be established. Lastly, gold standard adherence measures in telemedical interventions need to be established, so that study outcomes are more comparable and meta-analyses can be conducted.
Footnotes
Acknowledgements
NA.
Contributorship
NA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
No ethical approval was needed to conduct this review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Guarantor
Felix Gass.