
Abstract
Background
While telehealth utilization has decreased following the COVID-19 pandemic, the incorporation of remote visits into ambulatory cardiology practice guidelines remains a necessity. The aim of this study was to survey cardiologists’ perceptions on telehealth practices post-pandemic, and to propose clinical workflow models for remote visit types.
Methods
A 25-item survey was distributed to 481 American College of Cardiology CardioSurve panelists from 14 April 2023 through 11 May 2023. Descriptive analyses were conducted to evaluate provider demographics and reported percentages of responses to opinions and statements in the questionnaire. Chi-square and Fisher's exact tests were performed to determine statistically significant associations between categorical variables. Kruskal–Wallis H tests were performed on telemedicine visit frequency offered before, during, and after the pandemic.
Results
Seventy percent of respondents continue to offer telemedicine visits post-pandemic. Early career cardiologists were more likely to offer telemedicine visits compared to later career colleagues (p = 0.004). The odds ratio for offering telemedicine visits for early career compared to late-career was 5.56 (95% CI [1.910, 16.277]) and 1.394 (95% CI [0.594, 3.269]) for mid-career compared to late-career. Sixty-three percent of respondents reported that lack of reliable internet access posed challenges for outpatient visits, and approximately one-third believed that the risk for malpractice increased when providing care remotely. Only 22% of cardiologists reported the use of telepresenters. Three clinical workflow models were then constructed to address potential barriers to telehealth implementation.
Conclusions
Cardiologists continue to offer telehealth visits, but concerns persist regarding the feasibility and appropriateness for a variety of ambulatory encounter types. To address these concerns, we have proposed several models for telehealth integration into various outpatient settings to optimize access to care and lighten the burden placed on an already diminishing cardiology workforce.
Introduction
Widescale use of telehealth in cardiology became a necessity during the COVID-19 pandemic as we needed to continue to deliver care despite social distancing requirements. Prior to this, telehealth had been used in ambulatory cardiology settings, particularly in patients with heart failure, arrhythmias, and ischemic heart disease, but its use was limited given reimbursement and insurance restrictions and overall lack of infrastructure to provide remote services, among other reasons.1–4
However, during the pandemic, the use of digital tools to safely deliver care exponentially increased from <1% to over 70%. 5 Since then, studies have investigated the implementation of telehealth services in ambulatory cardiovascular care and identified feasibility of use in various cardiology subspecialties during and after the pandemic.3,5–7 These studies have demonstrated that combining telemonitoring and guideline-directed therapy can improve quality of life for a multitude of patients with various disease profiles, including, but not limited to, peripheral vascular disease, atrial fibrillation, heart failure, and treatment-resistant hypertension.6–9 Additionally, the notable increase in the use of wearable devices, including mobile cardiac telemetry, enabled wireless communication to supplement remote monitoring in otherwise resource-limited settings.3,9
The cardiology workforce has been shrinking due to training shortages and retirements, resulting in a net loss of 547 cardiologists per year and increasing attrition of physician-extenders, including nurses and advanced practitioners. 10 Thus, there is an urgent need to restructure current clinical practice in the digital age to meet the demands of an ever-complex, increasingly older and sicker population of patients in a system already burdened by rising health care costs.
This study aims to evaluate cardiologists’ perceptions on telehealth practices after the pandemic and characterize ongoing barriers to broader implementation. Based on these findings, we propose several models for the integration of telehealth into various outpatient settings in an effort to provide additional guidance on ways to triage outpatient encounters in a digital age, identify vulnerable populations, improve access to care using telepresenters and attainable medical supplies, and optimize workflow to lighten the burden placed on an already diminishing cardiology workforce.
Methods
This was a cross-sectional, online, anonymous 25-item survey that was distributed to 481 cardiologists meeting the following inclusion criteria: CardioSurve panelists were American College of Cardiology (ACC) members and Fellows ACC who were actively practicing in the United States. Cardiologists who were not part of the CardioSurve panel were excluded. Panelists were selected using a stratified random sampling technique to ensure accurate demographic representation of U.S.-based cardiologists, and they voluntarily agreed to participate in monthly ACC research surveys for a two-year term. The survey was conducted from 14 April 2023 through 11 May 2023. The online survey is available for review under Supplemental files.
The study protocol was reviewed by the Advarra Institutional Review Board (IRB) Services and deemed to be exempt from IRB oversight. Survey respondents were provided with introductory language explaining the survey and informed that their individual responses would be kept confidential.
Provider demographic information was collected, including sex, race, years in practice, primary specialty, types of outpatient visits offered in person and through telemedicine encounters, payer mix, and whether telemedicine visits were used prior to, during, and after the COVID-19 pandemic. Survey questions also included the following: (1) provider telemedicine visit practices, including use of telepresenter services, (2) provider responses to statements regarding technological advancements and possible limitations in the age of telehealth, and (3) summary of perceptions, including provider assessment of subspecialties best suited for telemedicine visits, risk for malpractice with telemedicine visits, and whether providers are continuing to offer telemedicine visits after the COVID-19 pandemic. Survey participants answered questions comprised of the following formats: single-answer multiple-choice, dichotomous, open-text entry, and Likert scale questions. Open-text entries were excluded from statistical analysis.
An analysis of responses was performed using the Statistical Package for the Social Sciences (SPSS) version 27 (Armonk, NY, USA). Descriptive analyses (frequency and percentages) were conducted to evaluate provider demographics and reported percentages of selected responses to opinions and statements based on the questionnaire. Chi-square and Fisher's exact tests were performed to determine statistically significant associations between categorical variables. For the subgroup analyses, Fisher's exact tests were used to report significance for a cell of fewer than n = 5. Kruskal–Wallis H testing was used to analyze significance for ordinal values and performed on telemedicine visit frequency offered before, during, and after the pandemic. A p-value <0.05 was indicative of statistically significant differences between variables. To calculate effect size, univariate logistic regression was performed between cardiologists offering telemedicine visits based on career stage, with late-career stage as the reference category. Advarra IRB Services reviewed the study protocol and, using the Department of Health and Human Services regulations found at 45 CFR 46.104(d), 2 the IRB determined that the research project was exempt from IRB oversight.
Results
Respondent demographics
The survey total response rate was 31% (148 out of 481 responders). Among the 148 participants, a majority were male (85%), and 61% identified as White (Table 1). There was a largely even distribution of participants in various career stages with 30% early career, 26% mid-career, and 38% late-career (Table 1). The three most common specialty certifications were general cardiology (57%), interventional cardiology (29%), followed by electrophysiology (6%) (Table 1). Additional clinical practice information, including procedural volume and type of practice, is listed in Supplemental Table S1.
Participant demographic table.

Changes in utilization of telemedicine with COVID-19
Prior to the COVID-19 pandemic, 14% of cardiologists performed telemedicine visits (Figure 1). This practice pattern shifted notably during the pandemic, with 94% offering telemedicine visits, and remained common post-COVID-19, with 70% of participants still adhering to telehealth practices. Among those currently providing telemedicine visits, most (79%) replied that they should continue to offer these services. However, the frequency of telemedicine visits significantly declined following the pandemic (p

Telemedicine visit frequency comparisons at various times surrounding the pandemic.
Provider perceptions of use of telehealth in cardiology
Perceptions on the use of telehealth varied based on career stage. Early career cardiologists (89%) were more likely to provide telemedicine visits compared to their mid- (67%) and late-career (59%) colleagues (p = 0.004) (Figure 2). The odds ratio for offering telemedicine visits for early career compared to late-career was 5.56 (95% CI [1.910, 16.277]) and 1.394 (95% CI [0.594, 3.269]) for mid-career compared to late-career.

Distribution of providers currently offering telemedicine visits based on tenure level.
Early career participants were more likely to report feeling that they should offer telemedicine visits post-pandemic, and that telehealth technology improved their ability to perform cardiology care compared to mid- and late-career cardiologists (82% vs. 59% vs. 55%, p = 0.012; 67% vs. 36% vs. 46%, p = 0.015, respectively, see Table 2). Only 9% of early career cardiologists perceived that telehealth was not a suitable way of practicing cardiology compared to their mid- and late-career colleagues (9% vs. 46% vs. 34%, p
Perceptions on telemedicine practices stratified by tenure level.

Descriptive analyses were conducted to report provider percentages to selected statements in the questionnaire. P values were obtained using Chi-square and Fisher's exact tests.
Amongst all cardiologists surveyed, those who continued to offer telemedicine visits were more likely to believe that telehealth technology improved their abilities to perform cardiology care, and that technological advancements have leveled the field for patient access to quality cardiology care, compared to those who were not offering telemedicine post-pandemic (61% vs. 23%, p
They were also more likely to report that even if payors decreased reimbursement rates for telemedicine visits, they would continue telemedicine appointments, compared to those who were not offering telemedicine visits post-pandemic (47% vs. 16%, p
Lastly, those who continued to offer telemedicine visits after the pandemic were more likely to report that patient workflow remained the same, regardless of in-person or telemedicine visits, compared to those who did not offer telemedicine visits post-pandemic (33% vs. 11%, p
Provider perceptions on types of visits best suited for telemedicine encounters
While most cardiologists (90% of total participants) preferred in-person office visits for managing complex cardiac patients, 85% of respondents believed that offering telemedicine visits to at least some of their patients would be appropriate (Figure 3(A)).

(A). Perceptions on appropriateness of telemedicine visits based on patient populations according to tenure level. (B). Perceptions of telepresenter utilization in telemedicine visits. RN indicates registered nurse; LPN indicates licensed practical nurse; CMA indicates certified medical assistant; CA indicates certified assistant. (C). Likert scale responses to statements on telemedicine and patient care.
Early career cardiologists were more likely to perceive follow-up visits and general cardiology consults as appropriate for telemedicine visits, compared to mid- and late-career cardiologists (91% vs. 77% vs. 71%, p
Types of visits appropriate for telemedicine encounters stratified by tenure level.
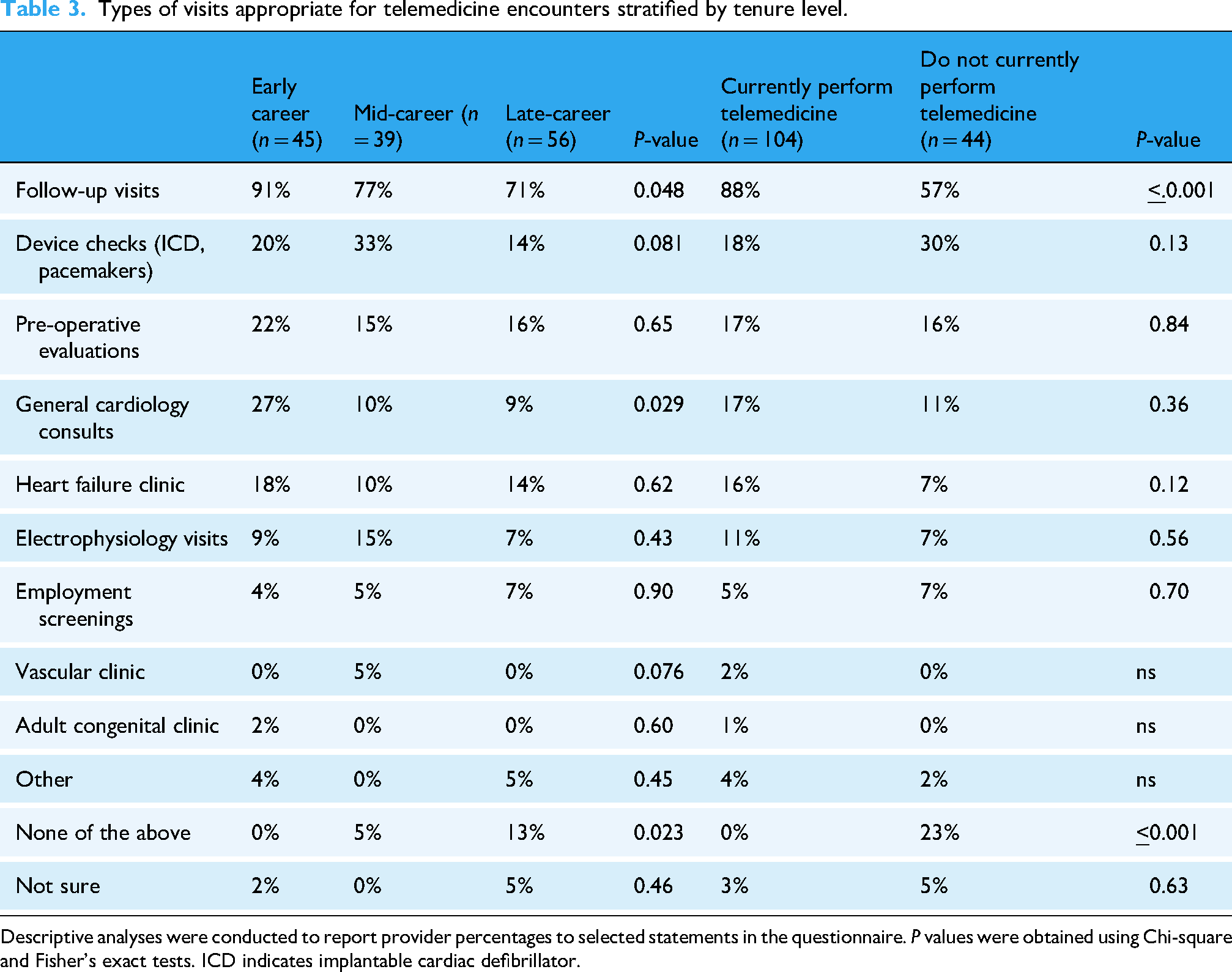
Descriptive analyses were conducted to report provider percentages to selected statements in the questionnaire. P values were obtained using Chi-square and Fisher's exact tests. ICD indicates implantable cardiac defibrillator.
Use of telepresenters
Few cardiologists (22%) reported using telepresenters in clinic (Figure 3(B)). Of those cardiologists who utilized telepresenters, 72% believed that this improved their efficiency. In comparison, only 1 in 3 cardiologists who had not used a telepresenter thought it would be of any benefit.
Barriers to telehealth in cardiology
Among the cardiologists currently providing telemedicine visits, 63% reported that lack of reliable access to high-speed internet posed a challenge for outpatient cardiology visits (Figure 3(C)). For 82% of cardiologists surveyed, the typical age range for their patient population fell between 65 and 80 years of age, regardless of career stage (Supplemental Figure S1). Additional patient cardiovascular disease profile and payor distribution characteristics are listed in Supplemental Table S3.
Over half of cardiologists believed that risk for malpractice in providing cardiology care via in-person versus telemedicine visits has neither increased nor decreased. Around one-third of cardiologists surveyed believed that the overall perceived risk for malpractice when providing care remotely was increased, without differences noted by career stage.
Discussion
This study identifies several findings regarding cardiologists’ perceptions toward the use of telehealth. While in-person cardiology visits remained the preferred type of clinical encounter for most, 70% of surveyed cardiologists continued to offer telemedicine visits in the post-COVID-19 era. Most cardiologists (regardless of career stage) deemed follow-up visits to be the most suitable type of encounter to be offered remotely. Early career cardiologists were more likely to offer telemedicine visits compared to later career colleagues, a finding that has previously been demonstrated amongst primary care physicians and potentially explained by younger physicians’ higher levels of comfort with technology and digital platforms. 11
Potential barriers to successful implementation of telemedicine visits as demonstrated by this survey included perceived malpractice risk in providing remote visits and lack of reliable access to high-speed internet, particularly for older patients. These concerns highlight the importance of utilizing and documenting informed consent for remote visits with specific parameters addressed prior to the start of virtual encounters. 12 These barriers also emphasize the crucial role telepresenters have in facilitating remote visits with equipment set-up, orientation, and test-runs beforehand, and having providers or companies assist with loaning equipment such as tablets and software, arranging a backup telephone conversation, or using a three-way telemedicine platform in the event of connection difficulties, which have previously been considered for patients with hearing and/or cognitive impairment. 13
This study demonstrated that the typical age range for patients seen by outpatient cardiologists was 65–80 years of age, highlighting an important population of patients who would benefit from further optimization of remote health services. This has been previously identified by the National Health and Aging Trends Study, in which 72% of adults aged 85 years or older experienced difficulty with telehealth video visits due to a variety of reasons, including hearing or visual impairment, difficulty speaking, cognitive impairment, and unfamiliarity with internet-based or wireless technology. 14 These observations reinforce the importance of acknowledging existing inequities to telehealth services for older patients less familiar with internet-based and wireless technologies. Similar findings were observed in a veteran population, where navigating technology was a primary barrier for both providers and patients. 15
Importantly, existing inequalities such as those observed for patients living in rural areas and those with lower socioeconomic status without reliable broadband and internet access, as well as significant language barriers and physical and cognitive impairments, can pose significant barriers to widespread adoption and use of telehealth in resource-limited settings. 14 Clinical teams need to consider appropriate selection of bandwidth-efficient, device-compatible technologies, and developing patient-inclusive workflows (language interpreter, onboarding visit assistance) if telehealth visits are to be incorporated into their practices. 5 Although telehealth has the possibility to decrease inequalities, care needs to be taken to consider ways in which existing inequalities could be addressed prior to offering remote encounter visits.
Based on the survey results, engagement of telepresenters for telemedicine visits remained low, with only 22% of cardiologists reporting the use of telepresenters. Telepresenters may mitigate existing inequities as they can help navigate technological issues, obtain basic clinical data (such as electrocardiograms and vital signs), and assist with basic physical exam findings over video conference, which has previously been shown to be feasible and effective. 16 In this present study, the cardiologists surveyed who worked with telepresenters believed this partnership improved their overall efficiency during these remote visits. Telepresenters play a crucial role in increasing patient involvement remotely, which may mitigate the existing inequities observed in rural, underserved, and Medicaid-dominant communities. 17 Barriers to a broader utilization of telepresenters include, but are not limited to, lack of formally trained staff or laypersons in the community, lack of a formal telepresenter curriculum, and lack of a standardized and well-defined role of a telepresenter in clinical practice. 18 Addressing the underutilization of these important health professionals may improve coordination of telehealth care.
Based on this survey, providers who continued to offer telemedicine visits post-pandemic were more likely to report that even if payors decreased reimbursement rates for telemedicine visits, they would continue telemedicine appointments. This acknowledges the potential benefits that telehealth can provide not only for patients and providers, but also for healthcare systems and payors, in which long-term use of telehealth platforms may decrease overhead costs, increase capacity for inpatient care, and decrease overall payments due to a decline in facility fees. 19 Yet, telemedicine usage has declined nationwide post-pandemic, partly due to uncertainties regarding its financial sustainability. 20
This raises important questions around how telehealth and digital technologies should be integrated into routine ambulatory care moving forward and brings into question telehealth sustainability. Smaller-scale surveys assessing provider opinion on telehealth after the pandemic have been conducted in other specialties, such as oncology and orthopedics, but little remains known about the future of telehealth practice in cardiology.21,22 Strategies to mitigate these concerns have been proposed in several studies. These proposed interventions may include limiting coverage to certain conditions or telemedicine visit modalities, further defining types of visits suitable for telephone versus video encounters, or adopting value-based financing models, which may be especially relevant for patients with heart failure.19,20
Given the findings of this survey, we propose three model visit types for optimization of ambulatory cardiology telehealth visits, based on patient location (home-based or office-based), availability of digital health tools, and availability of telepresenters (Figure 4(A) to (C)). For home-based visits, it is important to consider the visit goal, as well as pre-existing barriers to reliable internet, patient technological literacy, and ongoing speech, hearing, or visual impairments. This can help to inform whether a video visit or phone visit would be more appropriate. For visits requiring electrocardiogram (ECG) performance or visits that require remote transmission of patient data (i.e. mobile cardiac telemetry, daily weights, and blood pressure readings), telemedicine visits may be appropriate. For ambulatory settings with video conference capabilities in which the patient is accompanied either by an individual familiar with his or her health status or medically trained personnel with access to a blood pressure cuff and/or scale, routine follow-up visits in general cardiology, interventional cardiology, heart failure, adult congenital heart disease, and electrophysiology may be considered. In circumstances for which a detailed cardiac physical exam is needed (i.e. new valvular disorders, follow-up visits for patients with bioprosthetic or mechanical valves, and new heart failure symptoms), in-person visits should be performed.

(A). Proposed telehealth visit encounters suitable for home-based visits. (B). Proposed telehealth visit encounters suitable for facility-based visits, based on medical staff and medical supply availability. BP indicates blood pressure; GDMT indicates guideline-directed medical therapy. (C). Proposed telehealth visit encounters suitable for rural clinics. BP indicates blood pressure; ECG indicates electrocardiogram; GDMT indicates guideline-directed medical therapy.
At a minimum, remote visits would require either broadband and/or mobile hotspot access for video-facilitated encounters, accessible patient transport to a local facility for visits requiring a physical exam and/or ECG monitoring, and access to a device capable of accessing the Internet or a telephone landline, all of which may pose barriers to the most remote regions within the United States. 23 Additionally, the hiring of telepresenters will require training in at least three critical areas: understanding the technological platform and devices to be used, adapting clinical skills to facilitate virtual encounters, and learning to conduct physical exams on a video conference. 24
For many patients, the pandemic compromised equitable and timely access to medical care, delayed necessary treatments, and led to poorer clinical outcomes, particularly amongst patients presenting with myocardial infarction or heart failure. 10 Telehealth may provide an opportunity to reduce no-show rates for vulnerable patient groups and mitigate existing disparities.25,26 It is important to identify best practices for telehealth depending on patients’ needs, limitations, and visit types.
Limitations
This study has several limitations. The online survey was only distributed to cardiologists participating as CardioSurve panelists with an overall response rate of approximately 31%. However, this response rate is typical for those seen in prior CardioSurve surveys, and the overall n-size provided for the interpretation of the data was sufficient for the required statistical testing. Additionally, most respondents were white and male, practicing in suburban or urban settings, which potentially limits the generalizability of these findings, especially when considering barriers to improving telehealth access for patients and providers within rural settings. Lastly, the study was limited to physicians and may not be entirely representative of perceptions on telehealth practices from other allied healthcare professional groups, including, but not limited to, physician assistants, nurse practitioners, and registered nurses. Future studies will be needed to include more diverse provider demographics when distributing surveys (such as allied health providers in rural communities for broader applicability), with emphasis placed on remote practice regions, and to evaluate longer-term outcomes on virtual cardiovascular care, especially for complex patient populations requiring hemodynamic evaluations, telemetric data, and serial physical exams.
Conclusion
Cardiologists continue to offer telehealth visits, but concerns persist regarding its feasibility and appropriateness for an array of ambulatory encounter types, and the longer-term implications of telemedicine delivery post-pandemic remain unknown. The proposed clinical workflow models in this study may offer additional guidance on triaging the appropriateness of telemedicine visits, potential resources required, and the feasibility of remote visits for a variety of clinical encounters within the spectrum of outpatient cardiovascular care. The thoughtful integration of telehealth and use of e-health tools may help to address current and projected workforce shortages within cardiology, and alleviate the rising cost of healthcare delivery with the implementation of standardized remote visits into reimbursement models in order to meet the demands of an ever-growing population of patients with chronic, complex disease profiles, especially within limited resource settings.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251364928 - Supplemental material for Cardiologists’ perceptions on telehealth practices and limitations during and following the COVID-19 pandemic
Supplemental material, sj-docx-1-dhj-10.1177_20552076251364928 for Cardiologists’ perceptions on telehealth practices and limitations during and following the COVID-19 pandemic by Jennifer Miao, Claire S Duvernoy, Paul D Varosy, Paul Theriot, Anne Rzeszut and S Elissa Altin in DIGITAL HEALTH
Footnotes
Ethical approval
Ethical approval was not required for this study.
Author contributions
The author contributions (indicated by initials) are listed as follows. Conceptualization: EA, CD, PV, PT, and JM; formal analysis: PT and AR; writing-original draft: JM and EA; writing-reviewing and editing: JM, EA, CD, PV, PT, and AR.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Paul Varosy was a member of the writing group for the HRS/EHRA/APHRS/LAHRS/ACC/AHA worldwide practice update for telehealth and arrhythmia monitoring during and after the pandemic. Paul Varosy also received research funding from the VA HSR&D, NHLBI, PCORI, and the ACC Foundation, and has a small ownership stake and unpaid medical advisor role for HRCRS/3PH Alliance, a clinical research organization.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.