
Abstract
Background
Nepal is a South Asian country with a high burden of non-communicable diseases. Electronic health technologies are a promising strategy to mitigate the rising burden of non-communicable diseases by strengthening primary healthcare center service delivery. However, electronic health implementation in Nepal is limited. Furthermore, electronic health use at the primary healthcare center level is chronically understudied. This qualitative study seeks to understand the perceived awareness, benefits, and determinants of electronic health uptake in Nepal, focusing on primary healthcare center-level non-communicable disease management.
Methods
We conducted in-depth interviews with 27 participants including policymakers, health experts, facility administrators, providers, and non-communicable diseases patients in 2019. We selected six urban primary healthcare center facilities via cluster convenience sampling for recruiting facility administrators, providers, and patients, and used convenience sampling to recruit policymakers and experts. We conducted thematic data analysis inductively and deductively using the electronic health readiness assessment framework to understand perceived barriers and facilitators of electronic health implementation.
Results
While there was general awareness and acceptance of electronic health, multiple barriers impede readiness for implementation. These include policy making gaps, language barriers, low user technical literacy, concerns of overreliance on technology, and inadequate training for administrators and providers. Stakeholder suggestions include creating electronic health interfaces that meet the needs of end users (providers and patients), providing training to enable end users to effectively use electronic health technologies, and strong policy support at the national level.
Conclusion
We identify several determinants for effectively promoting the use of electronic health for non-communicable diseases service delivery at the primary healthcare center level in Nepal.
Introduction
The World Health Organization (WHO) estimates that 77% of deaths from non-communicable diseases (NCDs) are in low- and middle-income countries (LMICs) 1 like Nepal, which have extremely limited resources and a rising NCD burden. Primary healthcare center (PHC), as the first point of contact for healthcare services, can provide both preventive care to avoid NCD onset and essential medical management for patients with existing NCDs.2–8 In LMICs like Nepal, however, PHC is often one of the weakest facets of the health system despite its enormous potential to achieve widespread NCD control.9–11
Electronic health (“electronic health”), which the WHO defines as the “use of information and communication technologies (ICT) for health”,12–16 is a potential solution to strengthen NCD care at the PHC level in Nepal. The ability of eHealth to provide prevention-focused, user-centered care underscores a clear opportunity for adoption at the PHC level since management of NCDs requires preventive and long-term patient-centered care strategies. Despite its potential for improving service delivery, however, eHealth take-up in LMICs is limited. 17 Likewise, eHealth literature on PHC services is limited.18,19 When concerned with PHC specifically in LMICs, there is even less available literature. 20 Among the small number of studies that do exist, attention has focused on outcome evaluation at the expense of building an adequate understanding of stakeholder concerns prior to eHealth implementation. For instance, data from Bangladesh, another South Asian LMIC, shows inequity in human resource readiness, inequity in technological capabilities for eHealth, and greater ownership of eHealth technologies among youth, males, and higher socio-economic status individuals. 21 Understanding the concerns of policymakers, experts, PHC staff, and PHC patients is therefore crucial for designing eHealth technologies that truly meet their needs.
This study seeks to add to the evidence base for strengthening urban primary care delivery in LMICs using eHealth technologies. Specifically, we aim to understand stakeholder concerns for eHealth readiness in Nepal, which will contribute to the identification of policy-relevant insights to guide the adoption of eHealth in PHCs.
Methods
Study setting and participant recruitment
In this qualitative cross-sectional study, we conducted in-depth interviews with policymakers, experts in health-related fields, and key informants from urban PHC facilities (includes facility administrators, healthcare providers, and patients who sought care from the facilities) in Nepal.
Our objective was to enroll a balanced group where the number of patient and provider interviewees roughly matched the number of administrators, experts, and policymaker interviewees. Therefore, we used cluster convenience sampling to identify participants based on pre-defined selection criteria (Table 1). PHC participants were selected from three PHC facilities in Kathmandu, Nepal's capital and urban center, and three PHC facilities in Kavrepalanchowk, a district 35 km northeast of Kathmandu with two urban centers and the Kathmandu University Teaching Hospital.
Participant eligibility criteria.
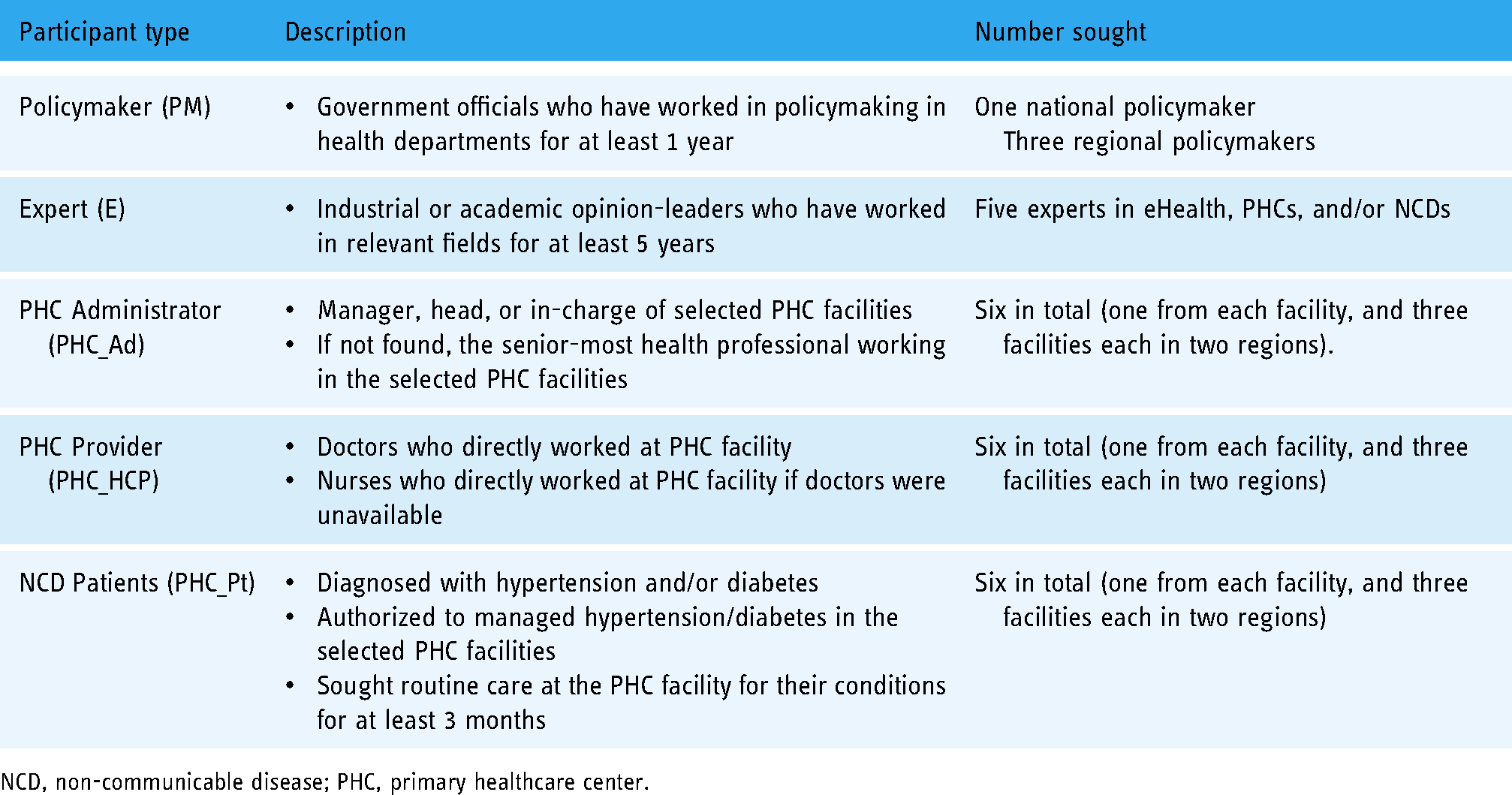
NCD, non-communicable disease; PHC, primary healthcare center.
We included one administrator, one provider, and one NCD patient from each PHC facility in the interviews. We further included national and regional level policymakers and eHealth experts as per the criteria in Table 1. All recruited stakeholders agreed to participate in our study.
Data collection
We designed a semi-structured interview guide based on the scoping review conducted within the multinational “Strengthening Urban Primary Healthcare Service Delivery through the use of eHealth Programs in China, Nepal, the Philippines, and Peru (SUPER)” study, which has been described elsewhere.22,23 The interview guide included (1) general information about the interviewee; (2) interviewee's understanding about the definition of eHealth; (3) interviewee's opinions on the barriers and facilitators for utilization of eHealth; (4) interviewee's opinions on the integration of eHealth technologies with the PHC system, and (5) suggestions and comments about eHealth. The core structure of the interview guide was standardized across the four countries in the SUPER study while allowing for context-based modifications. In Nepal, where eHealth is still extremely limited at the PHC level, most interviews focused on the first four sections of the interview guide. The interview guide for PHC patients was simplified to focus on parts (3) and (4) only.
All interviews were conducted between December 2019 and May 2020 in Nepali by trained researchers in the offices (for policymakers, experts, and administrators) and in the PHCs (for providers and patients). The interviews lasted between 30 and 60 min and were audio-recorded and transcribed in English. The interview questionnaire (standardized version in English) is presented in Appendix 1. We obtained written informed consent with an assurance of data confidentiality from participants prior to any data collection.
Thematic coding
Coding strategy
We used inductive and deductive approaches to analyze the interview transcripts. 24 First, we used deductive coding to map out the interview contents, following the structure and logic of the interview guide, which includes (1) awareness of eHealth, (2) perceived benefits of eHealth, (3) perceived determinants of eHealth take-up, and (4) suggestions for improved take-up of eHealth technologies. Second, we conducted inductive coding to identify emerging specific themes and codes that addressed our research questions. These two steps were completed by two independent coders, with a target inter-rater reliability of 70%. Third, to have more in-depth understanding of the perceived facilitators and barriers of the use of eHealth, a third coder led further analysis of the interview data and aligned the themes and codes with the eHealth readiness assessment (eHRA) framework. 25 Final thematic analysis results were generated through team discussion and verification until group agreement. The primary software used for the coding process was NVivo 12. Tables 3 and 4 present the final thematic coding results.
Stakeholder's perceived concerns and benefits of eHealth technologies.

eHealth, electronic health; PHCs, primary healthcare centers.
Perceived barriers and facilitators to ehealth technologies using eHRA framework .

eHealth, electronic health; eHRA, eHealth readiness assessment.
Framework
The eHRA framework was adopted for its growing use in determining the preparedness of health systems in developing countries “for the anticipated change brought by programs related to ICT use”. 25 It is based on four major domains: (a) governance, (b) stakeholder issues, (c) resources, and (d) access.25,26 These constructs capture a variety of determinants of eHealth readiness, ranging from macro-level policy concerns (governance) to microlevel stakeholder and resource constraints.
The rationale for using the eHRA framework is threefold. First, it allows us to anchor the analysis in an existing eHealth readiness framework, thereby facilitating its use among relevant stakeholders. Second, it provides a framework tailored to the unique constraints of developing countries. Third, it allows us to focus on readiness in response to the anticipated change brought by eHealth, which is more reflective of Nepal's current state of eHealth adoption, as opposed to readiness for its actual implementation phase. The eHRA framework is therefore ideally suited to be integrated compared to other existing frameworks that were either unsuitable for developing country contexts, 27 focused on quantitative evaluative methods28,29 focused on latter stages of eHealth implementation (i.e. on actual uptake and impact), 27 or on business aspects of eHealth. 29
Presentation of findings
The findings of the paper are presented to adhere (to the best of our abilities) to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 30 See Appendix 2 for an overview of our adherence to the COREQ checklist
Findings
We enrolled 27 participants (14 males). Table 2 shows the participant characteristics. Table 3 summarizes our findings at the stakeholder level, including (a) understanding and perception of eHealth, (b) concern about eHealth adoption, (c) perceived benefits of eHealth technologies, and (d) suggestions for eHealth uptake. Table 4 summarizes the eight themes we identified on determinants of eHealth, organized under the four domains of the eHRA framework.
Participant characteristics.

NCD, non-communicable disease; PHC, primary healthcare center.
Stakeholder understanding and perception of eHealth
Most participants agreed with the WHO definition of eHealth. Policymakers and experts had the highest awareness, citing specific examples of eHealth use, while PHC patients were less clear about where eHealth technologies have been deployed. “Even the government of Nepal is trying to put the Electronic Health Record in place in many district hospitals now … for many of the managerial works … There are some good examples of eHealth being used … in Achham … in some of the PHC in Illam district using mHealth … [and] in Dolakha district. (Expert 1) “… Om Hospital which is providing [telemedicine service]. [Someone living] in the rural communities gets in contact with the doctor/specialist in the urban areas …” (Region 2: Facility 6 Administrator). “from the television, there is a TV channel called Om Shanti … which broadcasts a show, Prishak Paen … [which] explains all the details about what diabetic patients should do and should not do …all of these I got it from there.” (Region1: Facility 1 Patient)
Most participants supported the use of eHealth. Some participants, however, showed neutral or negative attitudes toward eHealth adoption. Negative attitudes encompassed concerns that eHealth would be treated as a wholesale, fix-everything strategy and that reliance on technology could undermine the patient–provider relationship.
“There are additional benefits of eHealth, but it cannot totally replace our conventional services … Everything is not possible through eHealth.” (National Policymaker)
“e-prescribing, online medicine should not be brought into existence. If brought, then there will be a lot of dependence [on] eHealth. How [can we follow up with the patients about how they are doing]? [It is only] good to talk to him [in person]. eHealth will increase the gap between doctors and the patient.” (Region 2: Facility 6 Health Care Provider)
Stakeholder concerns about eHealth
Respondents mentioned technological concerns (data security issues, lack of standardization and compatibility, user-centeredness of interface), organizational concerns (legal issues, funding, and overall sustainability), and stakeholder-specific concerns (lack of digital literacy, low public acceptance, lack of direct communication between provider and patient, compliance issues among providers, and inappropriate utilization among patients). Across the board, stakeholders expressed concerns about the potential harm of inappropriate utilization of eHealth technologies. This included patients using information they could not adequately understand and interpret to self-diagnose and self-treat symptoms, and mistrusting physicians’ advice. “eHealth strategies should be made in such a way to minimize the chance of self-medication. We may be in danger if practice of self- medication is promoted.” (National Policymaker)
Another reported concern was the lack of direct communication between providers and patients. This concern assumes that eHealth technologies and face-to-face communications are substitutes in provider–patient communications, and that the adoption of one could come at the expense of the other. As such, the adoption of eHealth technologies could result in the depersonalization of healthcare, culminating in mistrust between care providers and patients in long-term care. “There may be no trust regarding patient care among the consumers as well as they might think that there is no physical contact with providers.” (National Policymaker)
Stakeholder's perceived benefits of eHealth
Perceived benefits are straightforwardly grouped into supply-side benefits (e.g. improved work efficiency, data storage, and diagnostic accuracy) and demand-side benefits (improved patient health outcomes, enhanced patient–provider communications, and reduced costs). Benefits noted by the most types of respondents include (1) improved work efficiency, (2) improved patient health outcomes, and (3) reduced costs.
Most participants noted the administrative benefits of adopting eHealth technologies at the PHC level. The potential for streamlining and speeding up tedious tasks made eHealth an attractive option for supply-side stakeholders in PHC service delivery. “Previously a hard copy was used for reporting which would take a month for reporting. But now, with a click we can do monitoring and give the quick feedback.” (National Policymaker)
“… there is the chance that we forget something while we do [it] manually. But if we do works from eHealth we can be certain on things like “patient has arrived in that day,” “we had prescribed certain medicine while coming on that day,” “His blood sugar level and blood pressure was…..on that day,” “ After 2–4 months of follow-up, his blood pressure was on decreasing pace or increasing pace,” “Sugar level is decreasing or increasing,” “Whether he was benefited by a certain medicine or not,” “If there was any side effects of medicine, which medicine we prescribed again?” So, it would help patients for lifelong follow-up.” (Region 2: Facility 5 Administrator).
Participants also mentioned cost reduction as a crucial benefit of adopting eHealth technologies in PHC service delivery in Nepal. The argument is that eHealth technologies can reduce costs for patients (reduced travel costs) and for healthcare facilities (reduced overcrowding in tertiary-level institutions), two extremely common problems in low-resource settings. “It was initiated by Dr Bhola Rijal.
a
There are two or three reasons for its success. Not everyone from Humla [and] Jumla
b
[can] afford for the checkups, [and] a doctor like Bhola Rijal couldn't be available at Humla, Jumla for his service. [After being checked by a doctor in urban areas], the health workers there can have [discussions] with the doctors/specialist here about the patient's condition. Due to this, [patients] [need] not be present physically in the hospitals; he can get good services being there. This saves his time as well as money. It has also been a success as the patients could be directly consulted by the specialist for the treatment.” (Region 2: Facility 6 Administrator)
Stakeholder suggestions for eHealth uptake
Political support and coordination
Most stakeholders agreed that changes at the policy level are crucial for eHealth technologies to be accepted and used on the ground. These changes included designing policies that were (1) clear for all stakeholders, (2) signaled the government's financial and principled commitment, (3) standardized eHealth technologies across sectors, and (4) facilitated cross-sector collaboration within the health sector and with other related sectors. “… if there would be guideline of everything so that there would not be difference in treatment. Everyone would have similar type of treatments. Like the level of treatment that I do in the Jumla and the Kathmandu, could remain the same.” (Region 2: Facility 6 Provider)
“… to mobilize the provincial government for long term by the central government could be beneficial because every provincial government wants to keep their people healthy but talking about current situation, they are still confused about what and how to do …” (Region 2: Facility 6 Administrator)
Technology development
Stakeholders emphasized building an interface that is functional, user-friendly, affordable, secure, and interoperable across different technologies that makes multiple systems compatible with one another. Additionally, given low digital literacy in Nepal, stakeholders emphasized improvements in user-friendliness of eHealth technologies. Some suggested pilot research to determine the optimal design and integration strategies. “First of all, we should know whether it can be done in this clinic or not? Yes, whether it is needed here or not. Yes, need identification should be done first Once it is confirmed that the people here require such services, then we should be provided the related training.” (Region 2: Facility 5 Provider)
PHC facilities
Stakeholders offered several recommendations aimed at strengthening the implementation of eHealth technologies at the facility level. The foremost suggestion was to conduct a local needs assessment before implementing and scaling up eHealth. Barriers that were identified earlier, like those of language, would fall under this category. Moreover, stakeholders also recommended that eHealth technologies be institutionalized instead of being project-based, which encourages users to participate in a long-term service. Stakeholders also recommended that this institutionalization be accompanied by rigorous and continuous evaluations to assess how well eHealth technologies are addressing local needs. Finally, they recommend including human resources that are more adept at handling eHealth technologies.
PHC providers and patients
Stakeholders offered suggestions for improved acceptance of eHealth technologies and their subsequent implementation. To improve acceptance, they recommend education and training programs and increase awareness of eHealth and its potential benefits. This awareness would need to be paired with incentive mechanisms at earlier stages to encourage adoption. For providers, this can also mean evaluating their performance in ways that would encourage them to use eHealth technologies. As such, stakeholders supported behavioral interventions that would achieve this goal. “The main point is that the implementor or the service provider should be convinced first Unless they are convinced, the eHealth program cannot be implemented. This is the first thing.” (Regional Policymaker 1) “The first and foremost thing is [patients] need to know how to use it.” (Region 1: Facility 3 Provider) “If training can be provided according to the education level of the people then we can implement eHealth.” (Region 2: Facility 6 Provider)
eHRA framework theme 1: Governance
Sub-theme 1.1: Lack of a conducive regulatory environment
For many respondents, policy gaps in eHealth use (caused by a lack of political will and a legal framework) were a major barrier to eHealth uptake. This highlights insufficient organizational and policy readiness in response to eHealth. “The foremost thing right now is, there is no regulatory body for this. Yes, not from the government side.” (Region 1: Facility 2 Administrator)
Sub-theme 1.2: Lack of implementation plan
Several respondents specifically cited the lack of a comprehensive plan for implementing eHealth as a major barrier. This includes strategies for facilitating the interoperability of eHealth services within the PHC system and ensuring the security of the eHealth technology infrastructure. The main readiness themes highlighted included core readiness and technological readiness. One respondent mentioned that the plethora of eHealth systems could be a barrier if data entered in one of these systems cannot be easily used in another. “In fact, an information system to track NCDs might be developed by 10 different companies in 10 different ways and if the data operability is not ensured then a particular data entered into a system cannot be accessed.” (Expert 5)
eHRA framework theme 2: Stakeholder issues
Sub-theme 2.1: Limited public awareness and preparedness
Sixteen respondents cited public knowledge as a strong barrier for the implementation of eHealth technologies. Within this issue, some respondents focused on the issue of a generational gap, whereby the older generation is not literate and does not have enough information related to digital technologies to utilize eHealth altogether. This lack of knowledge, for some respondents, could result in hesitation to adopt new trends and techniques for offering healthcare services. “The foremost thing, fundamental thing is… lack of knowledge regarding this among the health care consumers. They are not aware that such services exist” (Region 1: Facility 2 Administrator)
“I have already told you that in many places, many people belong to old generation and they don't have enough information related to computer. They may not be technology friendly so that they might not accept it that [easily] …” (Regional Policymaker 2)
Sub-theme 2.2: Insufficient provider training and acceptance
Beyond public knowledge and acceptance, several respondents highlighted a lack of provider training as a significant barrier to the implementation of eHealth technologies. Provider training was the most-cited determinant in the study, with 49 references to the topic across 15 respondents. Respondents remarked that even if the necessary infrastructure is available, a healthcare workforce that does not know how to deploy eHealth technologies properly would impede their adoption. “There will be a lot of challenges during the development phase. Such as…in our place, computer is brought, there will be barrier if no one can use it despite having facilities of computer and internet both. If that person doesn't know how to use it, it is a barrier in itself.” (Region 2: Facility 4 Provider)
An expert extended this problem to argue that providers who are not well trained in the use of eHealth technologies would be unable to understand how it would be beneficial to their everyday work. Consequently, such providers would not comply with guidelines and best practices in eHealth use, resulting in poor implementation. Altogether this evidence highlights a potential lack of provider readiness. “The concern that I have is poor compliance from the health care provider side. People are not ready to learn yet and put them to the best use, to make the best use of eHealth and trying to get the best results.” (Expert 1)
eHRA framework theme 3: Resource
Sub-theme 3.1: Poor infrastructural readiness
Respondents pointed to financing as a major challenge, citing that eHealth must compete with other public health interests for funding. Prioritization of other public health needs may result in less or insufficient resources committed to eHealth technologies. “… budget is very low. Yes, reports point out that it is a priority but there may be no budget or they can find something else more important and say that let's not do it this time.” (Regional Policymaker 2)
Likewise, severe infrastructure constraints make it difficult for eHealth technologies to be meaningfully deployed in the first place. This includes a reliable power supply, sufficient network reach, and internet facilities. “At the center, if he/she is well known to everything but there are [no] equipment, no computer, no electricity or no internet, then how he/she will open the data and formats and how he/she will use that, right? This can be a problem.” (Regional Policymaker 2)
“We aren't using electronic devices now. We don't have a computer here. We aren't even provided with laptop. That's why we don't have that.” (Region 2: Facility 4 Provider)
Sub-theme 3.2: Limited human resources
Another resource constraint is the shortage of skilled human resources. Some respondents make the distinction between human resources directly involved in healthcare service delivery (coded as human health resources) and human resources directly involved in eHealth service delivery (coded as human ehealth resources), with the latter focusing on skilled technicians and developers who can optimize, troubleshoot, and maintain the eHealth technology interface and infrastructure. “Sometimes there may be all of these equipment but scarcity of human resources. There might be only one or two personnel. Sometimes due to the overflow of patient, he/she mayn't give time to all of those patients. There are a lot of obstacles which may be difficult for eHealth.” (Regional Policymaker 1)
eHRA framework theme 4: Access
Sub-theme 4.1: Poor access to eHealth technologies
Interview respondents frequently cited low affordability and accessibility of eHealth technologies as strong barriers to implementation. In a multilingual country like Nepal, the availability of technologies in local languages is a fundamental aspect of accessibility. One PHC administrator noted how eHealth technologies might be inaccessible to those that primarily communicate in their ethnic languages. “In a simple language, I talk in Nepali Language and the video made in Nepali language is useful for me but a person who understands Maithili couldn't get the Nepali language properly. In Nepal, we have diversity of languages used. There can be barrier due to language. So, it should be made in 2–4 languages.” (Region 2: Facility 6 Administrator)
Facilitators
Respondents named only a few facilitators. In the domain of stakeholder issues, seven respondents cited provider incentives as an important facilitator for the uptake of eHealth technologies. Ensuring that providers see the benefit of eHealth technologies is crucial to ensuring its utilization in the supply side. Meanwhile, in the domain of access, a notable facilitator is the user-friendliness of eHealth technologies. Ensuring that service deliverers and recipients alike can easily navigate through the interface of eHealth software was considered crucial to improving uptake. “The apps which are easier to use, which are similar to what we seek, if we find such apps, then only we would use them right? In health too, like you said, (clears throat) if you want to target the clients having cardio-metabolic diseases, if your target is to get the tool used by them, then it should be considered whether the tool has been made according to those target users, right?” (Expert 2)
“So if they feel that life will be easier by using this … less time will be spent in patient recording. It will give them a long-term benefit because the information will be accurate.” (Expert 1)
Discussion
With 374 urban care centers operating in Nepal, effective eHealth implementation holds immense potential for improved healthcare service delivery. c This study explored stakeholder's perspectives on the adoption of eHealth initiatives for strengthening urban primary care in Nepal. We found that although there is general acceptance of eHealth, multiple barriers impede readiness and implementation. These include policymaking gaps, data security concerns, conflicts of interest, language barriers, low user technical literacy, and inadequate training. These findings are consistent with a systematic review of studies in developing countries, which identified lack of infrastructure, lack of equipment, and technological gaps as the top three barriers to eHealth implementation. 33 . We also observed a better understanding of eHealth at the administrative and policymaking level than with end users such as providers and patients. Stakeholder interviews suggest possible solutions, ranging from proper regulatory frameworks at the national level, to designing eHealth interfaces that cater to the unique needs of PHC personnel and patients on the ground, to equipping end users with the knowledge and training to effectively utilize these technologies.
Among our sample of interviewees in Nepal, administrators and experts view eHealth as a way to provide better care at reduced costs. d As such, there was generally a positive perception of eHealth technologies among our respondents. Some stakeholders, however, also presented neutral and negative opinions of eHealth. Skeptics argued that eHealth could be inappropriately pursued as a catch-all solution, that poorly designed eHealth systems could be detrimental to service delivery, and that heavy reliance on technology could undermine patient–provider relationships. Further, skeptics were concerned about possible self-diagnosis and self-medication, especially given Nepal's low digital literacy rates. Moreover, stakeholders are concerned about a lack of political will, the unavailability of infrastructure, inadequate provider training, and low public awareness as barriers that must be overcome before eHealth technologies can be deployed effectively.
These concerns highlight several opportunities for enhanced eHealth readiness. First, policies that clearly signal government buy-in/support would allow for technical standardization of eHealth technologies and likely boost eHealth acceptance among PHC providers and patients. Second, a younger, more tech-savvy PHC workforce could improve supply-side acceptance, including involvement of community health workers in the implementation of eHealth. Third, user-friendly technological development can ensure that eHealth technologies are mindful of and responsive to local contexts and constraints, improving their usefulness to end users. Finally, changing provider and patient incentives to (1) make them aware of eHealth technologies and (2) to induce them to shift to eHealth technologies, could encourage eHealth adoption. Since well-designed eHealth technologies can be “experience goods,” e changes that encourage the use of these technologies in the short run may promote more sustained participation in eHealth longitudinally instead of as one-off projects.
The foundation of clinical care is trust built upon strong patient–provider relationships, so the concern that inappropriate technology use may depersonalize care is valid. Other studies in Nepal have found that the patient–provider relationship is fundamental to successful delivery of primary care services for NCDs such as hypertension and diabetes. 31 It is unclear, however, whether and to what extent adoption of eHealth might affect this facet of primary care. Kohrt et al. developed a Nepal-specific tool for rating communication skills and scoring the patient–provider relationship, as well as patient-rated interactions with providers in the setting of mental health visits.32,33 The use of this or similar tools within a study on eHealth initiatives could provide more rigorous evaluation of the potential effect(s) on the patient–provider relationship, potentially offering better insights into this aspect of eHealth. We, therefore, suggest this as a valuable direction for future research.
Our study possesses several strengths. We approach eHealth from an understudied angle, exploring stakeholder perspectives on eHealth readiness in Nepal to strengthen primary care services for combatting the rising burden of NCDs. Our sample size of 27 interviewees was more than sufficient to achieve saturation, and we included a diverse range of stakeholders, from policymakers and experts to facility administrators and end users (i.e. clinicians and patients). Our methods and reporting adhere closely to the COREQ guidelines. 30 Overall, our findings provide a preliminary guide for policymakers and other stakeholders to strengthen primary care delivery in urban areas via eHealth. Finally, this study was conducted immediately before the first COVID-19 wave in Nepal. On one hand, it is possible that the concerns about political inertia and stakeholder surrounding eHealth implementation, which were raised by many stakeholders in this study, may have been addressed by the exogenous pandemic shock. On the other, the enormous strain COVID-19 imposed on Nepal's health system may have further stalled efforts to strengthen NCD care and eHealth implementation. Our study provides a clear baseline upon which further studies in a post-COVID-19 context may compare whether stakeholder readiness has meaningfully changed.
In doing so, our findings contribute to the literature on eHealth readiness in South Asia, and broadly concur with findings in neighboring countries with similar healthcare systems. The optimism of stakeholders in Nepal is well supported by evidence of improved PHC-based service delivery in India34–36 and Bangladesh. 37 Further, while stakeholders seem aware about potential benefits in terms of time savings and access to medical history in other South Asian contexts, 35 they mention concerns about provider readiness35,38,39 and lack of adequate ICT infrastructure, and organizational effectiveness.38,40
Moreover, our findings corroborate with previous studies on eHealth readiness in other developing countries outside South Asia, such as Iran, 41 Botswana, 25 and South Africa. 42 Specifically, stakeholder concerns over training, resource access, and user-friendliness of technologies are consistent with a large body of existing literature addressing the use of mobile health technologies in primary care services. 43 The similarity in findings across different geographical contexts is likely because these countries are also in nascent stages of eHealth adoption and face similar infrastructural stakeholder constraints as our stakeholders in Nepal.
Likewise, our study carries several limitations. These include the use of only two districts in Nepal, convenience sampling, and findings that are limited in scope. With respect to study sites, Nepal is a small yet extremely diverse country, where rural regions and the corresponding populace far outnumber urban centers and residents. Within the limitation of being only two study sites, Kathmandu and Dhulikhel do portray characteristic urban centers within Nepal and serve our purposes as an exploratory study. Second, the use of convenience sampling can potentially bias sampling. This sampling method was necessary, however, provided our objective to enroll a balanced group of policymakers, experts, and facility administrators, who often have limited availability/willingness to participate in research as an interviewee. We attempted to partially mitigate this issue by creating a balanced sample where the number of patient and provider interviewees roughly matched the number of administrator, expert, and policymaker interviewees. The low levels of eHealth awareness among PHC patients in our study, however, meant although they comprised 6 out of 27 participants, their responses do not meaningfully feature in our main analysis on the determinants of eHealth readiness. Finally, while our study generates insights for implementing better eHealth technologies, it does not adequately focus on the specific problems faced by NCD patients and PHC providers, which will be instrumental to designing systems that cater to end user needs. A more robust needs assessment of both providers and patients must be the focus of future studies in this field.
The results of our study are crucial because eHealth technologies have large potential benefits in Nepal. First, Nepal's high mobile phone penetration rates suggest that eHealth technologies can be effective outreach and communication strategies for PHCs. 44 Further, previous studies on eHealth use in CMD control have demonstrated encouraging results in Nepal,13,14 offering precedence for the efficacy of eHealth technologies in this context. However, previous studies in Nepal suggest that eHealth implementation suffers from poor integration with the existing healthcare system and limited scale of implementation. 17 Crucially, our findings suggest that some of the perceived benefits of eHealth implementation appear with greater integration and scale. As such, investing more resources in digital infrastructure development and stakeholder readiness can allow urban PHCs to explore the untapped potential of eHealth technologies in supporting patients with NCDs.
Conclusion
eHealth is a nascent field and requires careful attention from all stakeholders. We found that while administrators and experts view eHealth as a way to provide improved care at reduced costs, numerous barriers continue to impede eHealth readiness. These include lack of political will, unavailable infrastructure, inadequate provider training, low digital literacy, and concerns that further digitization of healthcare will undermine the patient–physician relationship. These challenges underscore major opportunities to improve eHealth readiness. Potential solutions include user-friendly tech development that is mindful of and responsive to local contexts, cultivating a tech-savvy healthcare workforce including community health workers, and policies that clearly signal government buy-in to eHealth strategies. The emphasis placed by our respondents on addressing local needs indicates the need for a more robust needs assessment of both providers and patients must be the focus of future studies in this field.
Footnotes
Acknowledgments
We appreciate the support of and guidance in protocol development from Professor Shenglan Tang (Duke University), Professor Truls Ostbye (Duke University), and Professor Abu Abdullah (Duke Kunshan University). We acknowledge and appreciate the support from our research assistants/coordinators/project manager in fieldwork research, including Namuna Shrestha, Dr Rajani Shakya, Sulata Karki, Saurya Dhungel, Nikita Shakya, Roshan Kasti, Anusha Humagain, and the Dhulikhel Hospital Family. Finally, we gave our sincerest thanks to all the study participants for sharing their valuable insights to our research questions.
Conflict of interest
The author(s) declare that there is no conflict of interest.
Contributiorship
P.B. contributed to data analysis and writing of the article. A.S. contributed to study design and data collection. S.X. contributed to conceptualization, study design, data analysis, and critically revised the article. N.P. critically revised the article. C.R. contributed to data analysis, and critically revised the article. S.S. contributed to study design and data collection. R.Y. contributed to study design and data collection. B.K. contributed to conceptualization, study design, and data collection. L.Y. contributed to conceptualization, study design, and critically revised the article. T.J. contributed to data analysis and critically revised the article.
Ethical approval
The SUPER study was approved by the Duke Kunshan University Institutional Review Board (IRB No. 2019YANL015) and Nepal Health Research Council. (IRB Ref No. 1341) Local IRB approvals were obtained in Nepal with support from our local collaborators at Kathmandu University School of Medical Sciences (KUSMS) (IRC Ref No. 257/19). We obtained written informed consent with an assurance of data confidentiality from participants prior to any data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the funding support from the Asia Pacific Observatory on Health System and Policies, and additional financial support from Duke Kunshan University. P.B. acknowledges funding from Yale-NUS College to support the writing process.
Guarantor
L.Y. is the guarantor for this article.
Notes
Appendix 1: Semi-structured interview guide
What is your professional background? What are your current responsibilities? How many years have you been working in this field? The number of doctors, nurses, and other personnel The number of beds The number of residents covered The number of daily/annual outpatients The number of annual discharged inpatients
The definition of eHealth given by the WHO is “the use of information and communication technologies for health.”
Based on your understanding and work experience, do you agree with this definition? If not, please give us your modified definition of eHealth.
What eHealth technologies are available in your facility? What are the purposes of using those eHealth technologies? (e.g. reducing workload burden, improving efficiency/accuracy) Currently, what is the role of PHC facilities in the whole life cycle of eHealth technologies, from initiation, design, uptake, to maintenance? What do you think SHOULD be the role? What are the factors that influence the uptake of the eHealth technologies? (Can use some specific examples of the existing eHealth technologies) What are the facilitators and barriers for the use of eHealth in your facility? (e.g. financial, technical, and personnel factors) Are there issues in maintaining using eHealth in your facility? What are they? (e.g. financial, technical, and personnel factors)
What do you think is an ideal situation where eHealth technologies are well integrated in the PHC practices for NCDs?
In what aspects of your job responsibilities involve eHealth technologies? What are the effects of using these eHealth technologies on your work? Both positive and negative effects. How do you think eHealth can better fit in your responsibilities? (e.g. better design and functions) Based on the considerations above, what is your overall attitude toward the use of eHealth technology? If any, what are your concerns for using eHealth technology in NCD management?
Is there any connection between the different eHealth technologies used in your facility? (e.g. in some medical facilities, diagnosis, medical reports, information archives, and medical insurance data, are all based on one integral system.) How do you think the different eHealth technologies in your facility can be better integrated and compatible with each other? To your knowledge, what are some typical/distinctive cases of successful uses of eHealth for NCD in other PHC facilities? Are the eHealth technologies in your facility different from other PHC facilities in the same city? What are the differences? If any, what are the effects of these differences in the collaboration and communication among different facilities? (e.g. patient referrals, information sharing) How to enhance the integration of eHealth technologies among different primary healthcare facilities? According to your knowledge, are there other non-PHC facilities that use eHealth technologies? What are they like? (e.g. secondary/tertiary hospitals, companies, disease control centers, and governmental departments) Can the eHealth applications in your facility be integrated with these other departments? (e.g. patient referrals, and information sharing) How do you think we can enhance the integration of eHealth technologies among PHC facility and non-PHC facilities? What is the future development strategy in your facility regarding the use of eHealth technologies, especially for hypertension and diabetes management? What are your other suggestions to better integrate eHealth to the PHC system for NCD service delivery?