
Abstract
Background
A high burden of non-communicable diseases (NCDs) is contributing to high mortality and morbidity in India. Recent advancements in digital health interventions, including mHealth, eHealth, and telemedicine, have facilitated patient-centered care for NCDs.
Objective
This systematic review aims to evaluate the current evidence on digital interventions for people living with NCDs in India and the outcomes of those interventions.
Methods
We adopted PRISMA guidelines and systematically reviewed articles from MEDLINE, CINAHL, PsycINFO, ERIC, and Scopus databases with following criteria: journal articles presenting digital intervention(s) used by people with at least one of the NCDs, reporting health outcomes following the intervention, studies conducted in India among Indian population.
Results
Among 1669 articles retrieved from multiple sources, only 13 articles met our criteria. Most (n = 7) studies were conducted in southern states of India; eight studies included patients with diabetes, followed by neuropsychiatric disorders and other NCDs. Five studies recruited participants from tertiary hospitals; six interventions used text-messaging for delivering health services, and 10 studies reported randomized controlled trials. All the studies reported positive health outcomes following the intervention, including better self-management, increased patient–provider communication, improved medication adherence, and reduced disease symptoms. Most studies scored moderate to high in quality assessment checklist of Downs and Black.
Conclusion
Current evidence suggests a low number of interventions with positive outcomes. Future research should explore avenues of advanced technologies ensuring equitable and sustainable development of digital health interventions for people living with NCDs in India.
Introduction
The World Health Organization (WHO) defines non-communicable diseases (NCDs) as chronic conditions of long duration resulting from a combination of genetic, physiological, behavioral, and environmental factors. 1 Nearly 63% of all deaths can be attributable to NCDs, making this the leading cause of mortality in the world. 2 While more than 36 million people die each year due to NCDs, about 80% of NCD deaths occur in low and middle-income countries. 2 India is a highly populous country with a population of more than 1.3 billion which is facing an immense burden of NCDs. 3 Demographic and epidemiological transitions over the past few decades have resulted in a shift in the national burden of diseases from infectious diseases to NCDs.3,4 In 2017, India State-Level Disease Burden Initiative Collaborators reported nationwide variations of disease burden, which highlights that the prevalence of and mortality due to NCDs have increased across all the states between 1990 to 2016. 5 About 8.3% of all deaths and 5% of total disability-adjusted life years (DALYs) in 2016 were due to the contribution of cancer, which has doubled since 1990. 6 In addition to contributing to mortalities and morbidities, NCDs also affect the national economy enormously. For example, the economic losses from heart disease, stroke, and diabetes were estimated to be US$54 billion in 2015. 7 Considering the population health and associated challenges, it is essential to explore potential avenues to alleviate the high burden of NCDs in India. Providing conventional care for NCDs in a large population can be difficult because patients living with chronic conditions need continuous monitoring and prolonged treatment. 8 As the country suffers from a lack of adequate healthcare infrastructure and a severe scarcity of human resources for health, 9 conventional healthcare delivery methods involving face-to-face doctor–patient interactions might not be available to most of the people in India. Moreover, critical challenges such as long distance from the nearest health center, lack of transportation to health facilities, lack of awareness about health services, and high cost of seeking care can affect timely diagnosis and treatment of NCDs. 10 These problems necessitate interventions for making healthcare for NCDs more available, accessible, and acceptable to the patients who need them the most. Furthermore, chronic diseases make individuals vulnerable to mental and physical stress. 11 Empowering patients and their caregivers can help in addressing health problems through enhanced participation and adherence to optimal care at the community level. 12
In the era of digital technologies, many mHealth and eHealth interventions have been developed to provide a wide range of healthcare services to people living with different health conditions.13–15 Different devices and platforms, including mobile phone, website, software, wearable devices, and tablet computers, using online and offline digital technology platforms, are increasingly being used in healthcare; these are collectively termed as digital health.16,17 The WHO recognizes the potential of digital health interventions to achieve universal health coverage and ensure high-quality care to individuals. 17 These interventions can provide preventive, diagnostic, therapeutic, and palliative care using digital platforms such as mobile phone, portable computing devices, internet-based applications, and social media interfaces. 18 Many such interventions are designed and implemented for people living with NCDs. For example, a systematic review by Larson et al. evaluated nine telehealth interventions for patients receiving cancer care. 19 They found telehealth interventions to be similarly effective as usual care in terms of improving quality of life among study participants. This study highlighted opportunities to increase access to effective telehealth services at a lower cost. Another meta-analysis of 35 randomized controlled trials has reported beneficial effects of internet-based interventions for patients with type 2 diabetes mellitus. 20 Similar studies have been conducted among patients with other NCDs, including cardiovascular diseases, 21 stroke, 22 osteoarthritis, 23 depression, 24 and chronic obstructive pulmonary disease (COPD). 25 Such digital interventions facilitate better symptom assessment, self-management, reduction of symptom distress, awareness of health conditions, patient–provider communication, timely care-seeking, follow-up and referral, treatment adherence, and improved quality of living among the patients living with NCDs.26–28
However, the application of such advanced technological innovations is relatively low among the low and middle-income countries, who share the major proportion of the global burden of NCDs but have limited resources and opportunities to leverage the benefits of digital health.29,30 In India, the use of digital technologies is gaining momentum in recent years. 31 However, most of these interventions are being implemented within hospitals, where the health workforce has access to them.31,32 One systematic review by Bassi et al. reported the application of mHealth interventions in strengthening the overall health system in India with a primary focus on health service delivery. 33 These applications are mostly used by formal healthcare providers to diagnose diseases, report health conditions to the healthcare institutions, and make decisions for delivering care.
In addition to the available evidence on the systems-level mHealth interventions, it is essential to understand how digitalization is promoting health among individuals suffering from chronic conditions. The use of digital interventions has not been examined at the user level, which highlights a critical knowledge gap about patient-centered applications of digital health technologies for NCD patients in India. Evidence on how digital technologies are being used by people living with NCDs and how such interventions may contribute to health outcomes may inform large-scale adoption of evidence-based interventions among the NCD-affected population. This systematic review contributes to this knowledge gap. The objective of this article is to systematically evaluate the current evidence on digital health interventions used by people living with NCDs in India, and assess the outcomes of those interventions to inform the future development and implementation.
Methods
Search strategy
We conducted this systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 34 We searched published studies in MEDLINE, SCOPUS, CINAHL, PsycINFO, and ERIC databases using specific keywords, both as subject headings and general keywords, with appropriate Boolean operators, as shown in Table 1. These keywords were structured for searching literature on digital interventions for NCDs in the context of India, published since the inception of these databases. Four authors developed the working protocol for review and search strategy. All the databases were searched on 30 May 2019 for the last time.
Keywords for database searching.

Literature screening, inclusion and exclusion criteria
Articles found through database searching and additional sources were screened using Rayaan QCRI and RefWorks tools, which are online platforms for conducting systematic reviews and reference management, respectively.35,36 Three authors independently conducted the screening process. This step was a blinded process; conflicts that appeared in independent evaluations were discussed, and a consensus was made in the presence of two more authors.
We screened the literature and included articles in this review if they were: (a) empirical studies published in a peer-reviewed journal, (b) studies conducted among Indian population living in India, (c) studies presenting at least one health intervention, (d) the intervention was delivered through mobile phone, computer, internet, tablet, social media, and any digital medium, (e) interventions focused on at least one NCD among the intervention population, (f) the intervention was accessible to and utilized by the patients or caregivers, (g) studies which reported any health or health-related outcomes among the participants, and (h) studies published in the English language only.
Articles were excluded from this systematic review if they conflicted with any of the above-mentioned inclusion criteria.
Data extraction
We found 1611 articles through searching five databases: MEDLINE (n = 1072), Scopus (n = 255), CINAHL (n = 93), PsycINFO (n = 127), and ERIC (n = 64). Also, we found 58 additional articles from reference search, consultations with domain experts, hand searching, and other sources (Figure 1). Therefore, the total number of articles primarily considered in this review was 1669. Further, 337 duplicate articles were removed, and the titles and abstracts of the remaining 1332 articles were evaluated based on the described inclusion or exclusion criteria. After this step, we removed 1275 articles that did not meet our criteria. The reasons for exclusion at this stage were not having an empirical design (n = 413), no intervention reported (n = 338), not conducted in India (n = 242), not focused on any NCDs (n = 198), and the reported intervention did not use any digital platform (n = 84). At the next stage we evaluated the full texts of the 57 remaining articles, among which 44 were excluded due to inappropriate study design (n = 19), did not report outcomes (n = 17), and not focused on people living with NCDs (n = 8). Finally, the remaining 13 articles were recruited for this systematic review. Furthermore, two authors re-evaluated the full texts of the finally recruited articles and extracted data in a pre-designed codebook. The codebook included following domains for data extraction: (a) location and time of the study, (b) description and components of the intervention, (c) types of NCDs among the study participants, (d) sampling and recruitment strategies, (e) intervention strategy, (f) design of the evaluation study, and (g) outcomes after the interventions.
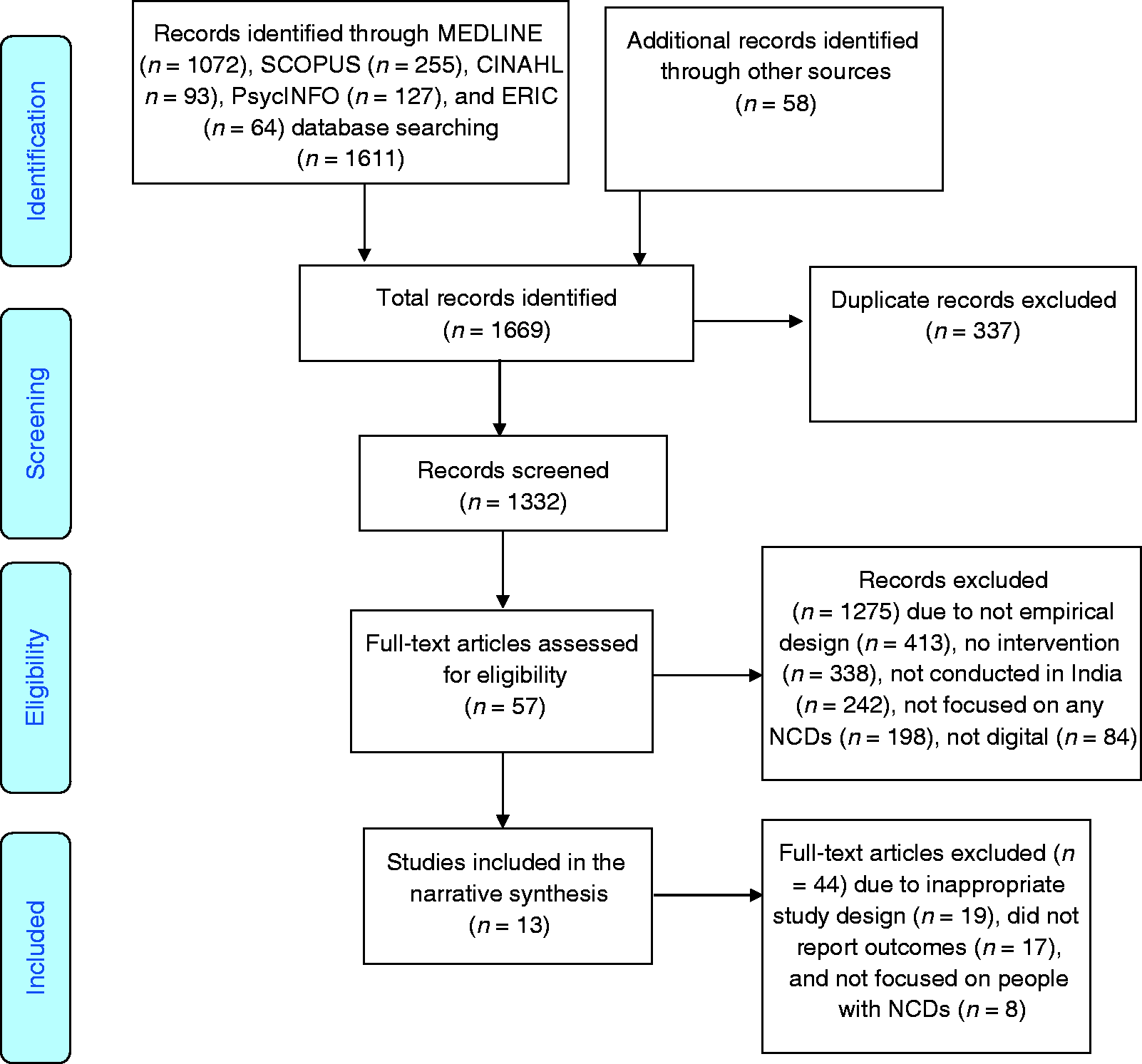
PRISMA flow diagram of the systematic review.
The coded data were reviewed by the other three authors to identify conflicts and resolve these based on consensus. Further, we included the key findings in the respective domain extracted from individual studies in a tabulated format. Finally, a brief narrative description of the interventions, characteristics of the study population, study or evaluation design, and the outcomes following the interventions are presented in the results.
Study quality assessment
In this systematic review, we used the Downs and Black checklist for assessing the methodological quality of both non-randomized and randomized intervention studies. 37 Three authors evaluated the studies independently. The results were further reviewed, and an agreement was made in the presence of three more authors. This checklist has a total of 27 items in five sub-scales for evaluating different methodological domains of the published studies. The first sub-scale has 10 items for assessing the quality of reporting (e.g. “Are the main findings of the study clearly described?”). The second sub-scale has three items for checking external validity (e.g. “Were the subjects asked to participate representative of the entire population from which they were recruited?”). The third and fourth sub-scales examine internal validity by assessing biases in three items (e.g. “Were subjects randomized to intervention groups?”) and confounding in six items. The fourth sub-scale evaluated confounding in six items (e.g. “Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population?”). The last sub-scale evaluates the power of the study on a range of 0–5 (e.g. “Did the study have sufficient power to detect a clinically important effect where the probability value for a difference being due to chance is less than 5%?”) Most items can be scored as “0” for “no” or “unable to decide” or “1” for “yes”, except one item in the reporting sub-scale (which can be score between 0 to 2) and the last sub-scale for power (scoring ranged between 0 to 5). Therefore, a study can receive a maximum score of 32 in this 27-item checklist.
Results
Out of 1669 studies derived from multiple databases and additional sources, 13 articles met our inclusion criteria (Table 2). Key findings from these studies are discussed below.
Overview of digital interventions for people living with NCDs in India.

Study period and location
Among the 13 studies included in this review, nine studies mentioned the study period during which they were conducted. The first study reporting digital intervention for NCDs was conducted by Patnaik et al. in 2012. 38 Most of the studies (n = 5) were conducted around 2015.39–43 The most recent study, by Goruntla et al., was conducted in 2017. 44 Studies were conducted in different states of India; however, most studies (n = 7) were from southern states. The highest number of studies (n = 3) were conducted in Bengaluru city of Karnataka state.38,40,45 There were two studies each from Tamil Nadu39,46 and Andhra Pradesh,44,46 and one each from Kerala, 47 Himachal Pradesh, 41 Punjab, 48 Puducherry, 42 Gujarat, 39 and Delhi. 43
Study design, recruitment strategy, and participants
There were only two cohort studies,43,47 and one pre–post study. 45 All the remaining studies (n = 10) were randomized control trials. In most of the studies (n = 5) the participants were recruited from tertiary care hospitals.38,42,43,48,49 The study conducted by Kleinman et al. recruited participants from multiple diabetes clinics and secondary care hospitals. 39 In the rest of the studies, participants were recruited from various sources including primary care hospital, mental health clinic, community outreach program, diabetes research center, and industrial workplace.
Among the included studies, the sample size ranged from 29 to 1000 participants. The majority of them (n = 8) recruited patients with diabetes. Three studies recruited patients with mental health disorders.40,42,45 One study recruited children with cerebral palsy, 50 and another recruited participants with metabolic syndrome. 49 In most of the studies (n = 9) the majority of the participants were males, in the middle age group (n = 11), with minimal literacy level to understand instructions related to the interventions (n = 10). More than half of the studies (n = 7) included participants with access to mobile phones.
Quality assessment of the included studies
Methodological quality was assessed for all the recruited studies (Table 3). Scores in five sub-scales were added to calculate the total score in the scale of 32. The mean score of the studies was 22.76 (range 19–26). The mean score for randomized controlled trials and studies with non-randomized designs were 23 and 22, respectively. The studies were further evaluated and labeled in three groups: low quality (score 18 or below, n = 0), moderate quality (score 19 to 22, n = 5), and high quality (score 23 or above, n = 9). Among the studies recruited in this review, four studies40,47,49,50 had moderate quality and the remaining nine studies had high quality.38,39,41–46,48
Quality assessment of the intervention studies.

Characteristics of the interventions
Among the included studies, six studies focused on self-management of the disease.38,39,41,43,45,50 For example, Mehrotra et al. focused on self-management of depression using the principles of cognitive behavioral therapy (CBT). 45 Moreover, four studies focused on increasing patient–provider communication.39,43,47,48 For example, Kesavadesv et al. provided three options (email, telephone calls, and a secured website) for the patients to communicate with a team of healthcare providers. 47 Five studies focused on educating the participants about their disease.38,43,44,46,47 Kesavadev et al. and Goruntla et al. provided face-to-face educational session alongside digital interventions,44,47 whereas Jha et al. provided educational videos for the participants. 43 Studies conducted by Ramachandaran et al. 46 and Patnaik et al. 38 reported SMS-based intervention to educate the participants about lifestyle modification. Furthermore, three studies focused on increasing follow-up.40,43,47 For example, Sing et al. provided reminders before the scheduled appointment for follow-up. 40 They also called the participants who had missed their appointments, requested for follow-up, and noted the reasons for missing the same. Two studies offered counseling services to patients.38,44 For example, Goruntla et al. provided face-to-face counseling regarding knowledge, education, and non-pharmacological strategies related to diabetes mellitus management for the participants. 44 Two interventions sent reminders to increase medication adherence among the patients including SMS reminders prior to their medication intake.42,44 Moreover, two interventions focused on increasing physical activity among the participants.44,49 For example, Radhakrishnan et al. encouraged participants to engage in aerobic exercise and sent reminders to exercise biweekly. 49
Although majority of the studies (n = 10) used one digital medium to deliver the intervention, the remaining studies (n = 3) used multiple methods to deliver the interventions to the participants. Among the interventions with a single component, the majority (n = 6) used SMS to deliver the intervention.38,41,42,44,46,49 For example, Kumar et al, sent biweekly SMSs to participants in the intervention group containing messages regarding self-management of diabetes. 41 Two interventions were delivered via mobile apps to send reminders, address patients’ problems, and increase communication with the providers.39,45 Kaur et al. was the only study to use telephonic consultation as the only component to increase the follow-up visits by the patients. 48 Another intervention by Sharan et al. used a virtual reality-based training program to help children with cerebral palsy to receive rehabilitation training at home. 50 There were a few (n = 3) studies with multiple modes of delivery.40,43,47 For example, Kesavadev et al. 47 provided three options for reporting the blood glucose level—phone, email and a secure website—and Jha et al. provided the facility for telephonic follow-up, SMS reminders, and access to educational videos. 43
The characteristics of the intervention studies were diverse irrespective of the study design. The non-randomized studies used telemedicine technologies to promote symptom management and follow-up.43,45,47 Similar contents and approaches to promote healthier behavior, lifestyle modification, management of health conditions, medication adherence, and communication with providers were reported among intervention studies that used a randomized controlled trial design.38–42,44,46,48–50
Outcomes of the interventions
All the studies reported outcomes specific to the NCD of interest in the respective studies. These outcomes included changes in biomarkers for specific diseases, improvements in follow-up and adherence to medication, improved health conditions in terms of patient-reported symptoms, satisfaction and increased participation in the offered health services. Reduction in the HbA1c level and improvement in the lipid profile was reported by most of the studies (n = 5).39,43,44,47,48 For example, Kesavadev et al. reported a significant decrease in the HbA1c level and decrease in low-density lipoprotein. 47
Five studies reported improvement in disease symptoms.38,45,46,49,50 For example, Sharan et al. reported improvement in balance, manual ability, and Pediatric Balance Score among the children in the intervention group. 50 Mehrotra et al. reported a reduction in the depression symptoms among the participants who completed all essential sessions. 45 Three studies reported improvement in medication adherence.39,42,44 For example, Menon et al. reported improvement in medication adherence and positive change in attitude among the participants in the intervention group. 42
Moreover, two studies reported improvement in the follow-up.40,47 For example, Singh et al. reported that the rate of reaching the appointment was significantly higher in the intervention group and 75% patients who missed previous appointments came back for follow-up. 40 Furthermore, three studies mentioned that participants were highly satisfied with the interventions.39,48,50 For example, Sharan et al. reported that level of participation, motivation, and satisfaction were significantly higher among children in the intervention group. 50
According to the study design, both randomized and non-randomized studies reported effectiveness in terms of health outcomes of interest in respective studies. Three non-randomized studies reported improved adherence, psychosomatic health outcomes, and better quality of living.42,45,47Among the randomized studies, the study participants reported varying levels of improvements in physical abilities, 50 management of impaired glycemic profile and diabetes,41,44,46,48,49 adherence to therapies and more frequent follow-up visits,39,42,44 and reduction in chronic physical and mental health conditions.38,40,49
Discussion
To our knowledge, this is the first systematic review of digital interventions for people living with NCDs in India. In this review, we found studies presenting different digital interventions for varying diagnoses of NCDs, ranging from cerebral palsy among children to diabetes among adult participants. A majority of the studies (n = 10) were randomized in design, two were cohort studies, and one used pre–post design. The target population, NCDs of interest, design and content of the intervention, and outcomes following the intervention were diverse across the included studies. Such heterogeneity in the interventions studies does not allow us to draw inferences on comparative outcomes between the studies. However, within-study variations in terms of outcomes of interest can provide analytical perspectives on how those interventions contributed to better health outcomes. Both among the randomized and non-randomized studies, the interventions attempted to increase access to different health services and deliver health-related information or self-management instructions to the participants. In these processed, digitalization played a pivotal role in establishing unidirectional and bi-directional communication between the providers and people living with NCDs. For example, the randomized clinical trial study by Kleinman et al. recruited patients with diabetes and the intervention group was offered mobile app to communicate with the providers, which allowed them to adopt self-management and lifestyle modification. 39 This study found a marked increase in medication adherence and self-testing of blood glucose, highlighting how strengthened communication and care through the digital platform resulted in better health outcomes. Similarly, the mobile-based digital intervention by Goruntla et al. found higher adherence and improved outcomes in blood glucose level, blood pressure, and lipid profile. 44 This evidence highlights that frequent reminders, instructions, and counseling may enhance treatment consumption and health outcomes among the study participants. While all the interventions in this review resulted in varying improvements in different health outcomes, none of them reported any adverse effect or unintended consequences following the implementation of the interventions. Despite the low number of studies, the current evidence shows various benefits of using digital health interventions among people living with NCDs. Furthermore, these interventions provide several critical insights on how India is leveraging the avenues of digital health and how future directions can be adopted to improve population health outcomes in the realm of NCDs.
First, the number of digital health interventions for NCDs is relatively low for India, which shares a major proportion of the global burden of NCDs. Like many other low- and middle-income countries, digital health interventions for NCDs have not reached their fullest potential in India, as seen in many developed nations. 51 However, investing in digital health can reduce the cost of direct care, enhance access to health services, and improve health outcomes for resource-constrained countries. 52 Future policymaking, research, and implementation should seek opportunities to adopt more evidence-based digital approaches to improve NCD care in the context of India.
Second, most of intervention studies were conducted in southern states of India, whereas we did not find any study from north-eastern states. These states share a similar burden of NCD compared with the national scenario. 5 Therefore, unequal distribution of studies highlights potential disparities in the development and implementation of digital health interventions across Indian states. This necessitates careful attention from researchers and practitioners to consider the adoption of evidence-based interventions and development of culturally tailored digital interventions for those states where digital health is in a developing stage.
Third, most of the studies recruited participants from hospitals, clinics, research centers, and community sources located in urban areas. Such urban-centered growth of digital interventions for NCDs may not help to improve population health outcomes, as 68.84% of India’s total population live in rural areas. 53 Moreover, the rural population in India often suffers from a lack of health infrastructure, scarcity of expert physicians, and lack of access to health services. 10 These places may have a higher need for technological advancements like digital health services to bridge the gaps of healthcare. In recent years, mHealth interventions have been implemented for community health services; for example, maternal and child health services by “Accredited Social Health Workers (ASHA)” in many states in India. 54 However, the benefits of the digital revolution in healthcare remain beyond the reach of the rural population suffering from NCDs. This is an area where future research and interventions should be focused, to alleviate the urban–rural health disparities in the digital era.
Fourth, most of the interventions were designed and implemented for diabetes, followed by neuropsychiatric disorders, whereas none of the included studies focused on cancer, cardiovascular diseases, or COPD, which constitute a large proportion of NCDs in India.6,55,56 People living with these diseases would need varying support which can be delivered successfully through digital interventions. For example, many studies have shown how mHealth and telemedicine interventions can help cancer patients or survivors.57–59 Moreover, studies have also shown that the use of digital self-management and exercise-based interventions can improve health outcomes among patients suffering from COPD. These opportunities should be explored in the context of India to improve patient-centered care in those unexplored areas of NCDs.
Fifth, most of the included studies discussed the implementation of digital interventions for localized patient populations in the respective study locations, whereas none of the studies have shown a large-scale adoption of the interventions at the community, state, regional, or national level. Moreover, little is known about the sustainability of the interventions presented in this review. Most studies reported health outcomes at the follow-up evaluations; however, it cannot be concluded that the interventions have brought sustainable health practices and outcomes among the participants. Moreover, digital interventions would require availability and accessibility to digital devices and services such as internet and messaging. 60 It cannot be assumed that the participants will continue to use the interventions once the study has ended. Future research in digital health in India should overcome such challenges and expand the outreach of health services for NCDs in a sustainable manner. A few potential strategies to do so may include subsidizing digital health devices and services for large-scale and sustainable adoption, 61 incentivizing healthcare providers to encourage digital health interventions complementing conventional care, 62 and development of low-cost and culturally appropriate digital interventions for different NCDs, ensuring optimal compliance among the users. 63
Sixth, NCD multimorbidity is an emerging global health challenge in which individuals suffer from co-existence of more than one NCD. 64 Earlier studies conducted in India have shown a high prevalence of multimorbidity,65,66 which needs extensive planning and optimal management of the patients. Studies conducted in other countries have shown that digital interventions can help in managing multimorbidity among NCD patients.67–69 However, most of the studies in this review had participants with diabetes, among which the burden of multiple morbidities was not evaluated explicitly. Only one study has reported an intervention for addressing psychological stress among diabetic patients. 38 This evidence highlights the need for examining how multimorbidity exists among people reporting one NCD, and how multiple digital health services can be delivered for those patients more efficiently. Such development of multifaceted digital interventions would require interoperability among healthcare providers offering specialized services in multiple domains of NCDs.70,71 As the burden of NCDs has been increasing in India, scholars and practitioners should consider such strategies to ensure optimal, multipronged, and holistic NCD care in the future.
Seventh, technological aspects of digital interventions should be evaluated in the context of global advancements. Artificial technologies such as machine learning and deep learning are increasingly being used for optimizing the performance of digital health interventions and customizing health services as per the unique requirements for individual patients.72–74 Such personalization of health services may facilitate precision healthcare delivery for patients with NCDs. While such innovations are contingent upon availability of big data including genomic, behavioral, epidemiological, and environmental data on a given population, these advancements in digital health should be acknowledged to unlock the potential of precision public health in resource-constrained contexts. 75 Current evidence in our review has shown text-messaging and internet-based applications in most of the studies in India. Understanding global trends in health information technologies may help in developing digital health interventions with advanced technologies in the future.
Eighth, the safety and security of personal health data is a major concern in the age of digitalization. In developed countries such as the United States, protected health information stored or exchanged through electronic systems is secured under regulatory measures such as the “Health Insurance Portability and Accountability Act - HIPPA.” 76 Despite such measures, breach of protected health information is a public health challenge in the United States. 77 In India, Clinical Establishments (Registration and Regulation) Act – 2010 and the Clinical Establishments (Central Government) Rules 2012 have been instituted to regulate health information services across the nation; 78 however, little is known about the scope of these measures in the era of rapidly evolving digital health. As electronic health records and other digital health applications are still under development, future innovations in digital health in India should be conceptualized maintaining compliance with legislative and regulatory measures. Although such measures would help digitalized health systems in general, they are likely to provide more protection to people with NCDs with a higher risk of data breaches, as they are more likely to use digital health services for managing chronic conditions across their lifespan.
Ninth, the participation of the patients and their informal caregivers is critical for effective development and successful implementation of digital interventions for NCDs.79,80 Many factors, including literacy about digital health and activation of the users, are essential for increasing adoption of digital health interventions.61,81 In most of the studies included in this review, the participants were recruited through direct communication, which may be expensive and time-consuming. Also, the findings of successful interventions should be widely communicated with people living with NCDs for better adoption of such interventions. The researchers and healthcare strategists should consider e-recruitment strategies, with culturally appropriate and context-specific behavior change communication approaches to increase participation in and adoption of such interventions among NCD patients.
Lastly, addressing the above-mentioned challenges and advancing digital health for NCDs would require collegial efforts of key stakeholders including physicians, other healthcare professionals, researchers working on NCDs, specialists working on health information technologies, health services organizations, and policymakers.61,82 The National Health Policy 2017 recognized the role of digital health technologies and envisioned establishing National Digital Health Authority to develop, deploy, and regulate digital health across the continuum of care. 83 It is critical to acknowledge the high burden of NCDs in India and incorporate specific provisions in these policy discourses to create an enabling environment within which multiple stakeholders can collaborate and work together to promote digital healthcare for NCDs.
Limitations
This systematic review has several limitations. First, this systematic review carries the limitations within the included studies. We acknowledge that there are publication biases within the studies as our team could see only the published studies with positive findings in most cases. This limits the process of learning about those interventions which did not work or were not published in the journals. Second, there could be limitations within the process of conducting the systematic review. We searched major databases with a plausible search strategy, and searched further to obtain more articles from additional sources. Therefore, we could not retrieve any literature stored in databases we did not search, which may be another limitation of this review. Third, the number of studies and sample sizes within those studies are relatively low, which may limit generalizing the findings for wide range of NCDs in a large country like India. However, we strictly followed the PRISMA guidelines and conducted each phase of the review in the presence of two or more reviewers to eliminate potential biases as well as other limitations in the process of conducting this systematic review. Future evidence synthesis should maintain strict methodologies and address the limitations of this review to better inform evidence on digital interventions for people living with NCDs.
Conclusion
To conclude, our systematic review shows a low yet gradually increasing number of digital health interventions for people living with NCDs in India. Most of the intervention studies have shown a wide range of positive health outcomes following the interventions, which highlight the potential for alleviating health problems among individuals suffering from different NCDs. Nevertheless, our review also presents the gaps alongside the current evidence, which may affect the overall development of digital health interventions for NCDs in the context of India. These gaps and challenges are critical for the large-scale adoption of evidence-based interventions, as well as for developing and implementing newer interventions for people living with NCDs. Future research and practice should engage key stakeholders and address issues highlighted in this review to advance patient-centered NCD care in the digital age in India.
Supplemental Material
DHJ896153 Supplemental Material - Supplemental material for Digital interventions for people living with non-communicable diseases in India: A systematic review of intervention studies and recommendations for future research and development
Supplemental material, DHJ896153 Supplemental Material for Digital interventions for people living with non-communicable diseases in India: A systematic review of intervention studies and recommendations for future research and development by Md Mahbub Hossain, Samia Tasnim, Rachit Sharma, Abida Sultana, Araish Farzana Shaik, Farah Faizah, Ravneet Kaur, Madhuri Uppuluri, Mitali Sribhashyam and Sudip Bhattacharya in Digital Health
Footnotes
Acknowledgements
We would like to thank Shah Akib Sarwar, Md Nazmus Sakib, and Arif Arman for their kind support in conducting this study.
Contributorship
MMH and ST conceived the study. MMH, RS, AS, and SB developed the review protocol and search strategy. MMH, RS, and AS conducted the primary screening; which was further reviewed by AF and FF. ST and RK conducted the data extraction from screened literature; which was further reviewed by MMH and RS. Quality assessment was conducted independently by AF, MU, MS; which was finally reviewed by MMH, ST, and FF. RK, MU, and MS conducted the background literature review. The first draft of the manuscript was written by MMH, ST, and AS. Further, it was further critically reviewed and edited by RS, AF, FF, and SB. All the authors reviewed and finalized the submitted version of the manuscript.
Conflicting interests
The authors have no conflicts of interest to declare.
Ethical approval
Not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MMH
Peer review
This manuscript was reviewed by reviewers, the authors have elected for these individuals to remain anonymous.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.