
Abstract
In this study, we use a difference-in-difference approach to explore how physician promotion, the advancement of a physician's offline reputation, affects patient behavior toward physicians in online healthcare communities; this allows us to explore how patients interpret the signals created by physician promotion. The study sample was collected from over 140,000 physician online profiles after 25 months of continuous observation, with 280 physicians who were promoted at month 13 as the treatment group and a control group obtained by propensity score matching. Our results show that a physician's promotion causes more patients to choose that physician, makes patients willing to give more psychological rewards, and makes them tend to give that physician a higher online rating. This implies that patient behavior is susceptible to the signal of physician promotion because the quality of the physician is unlikely to have changed significantly in the short term. These findings extend prior research on reputation in online communities and have crucial implications for theory and practice.
Introduction
Online healthcare communities (OHCs) are emerging online platforms intended to improve people's health status. 1 The functions of OHCs are diverse; for example, OHC managers can aggregate information about doctors and hospitals, patients can share their medical experiences with the public, physicians can write articles to provide medical knowledge, or physicians can answer patients’ questions online. In the OHC explored in this study, in addition to the above-mentioned functions, patients can select a specific physician for online consultation. After a patient interacts with a physician, he or she can provide additional psychological or material rewards to the physician, as well as rating the physician. Although there is a large body of research examining how physician characteristics influence patient behavior, the impact of physician promotion has still not been explicitly discussed due to limitations in data collection. Therefore, the motivation of this study is to reveal what impact physician promotion has on patient behavior, including choosing physicians, giving rewards, and evaluating physicians.
Physician promotion is defined as a change from resident to associate chief physician or from associate chief to chief physician. Since the reputation of an entity (individual or organization) can be defined as the public perception of that entity, usually as a result of some criteria or evaluation of the entity's characteristics, a physician's title can be considered as a kind of reputation, which means a physician's promotion is equivalent to an enhancement of his/her offline reputation. The next question is why reputation is an important influencing factor for OHCs. Due to the highly personalized and strongly emotional nature of an individual's involvement with medical services,4,5 patients frequently face severe information asymmetry and may not be able to discern the true quality of physicians. 6 According to signaling theory, 7 when there is information asymmetry in the market, sellers can send signals to consumers about their quality, thus enabling them to discern the quality of the product. 8 Therefore, observing the reputation of sellers is a common may for consumers to resolve information asymmetry. In this study, physician promotions indicate an increase in reputation, and it is thus useful to investigate behavioral changes in patients when they received this signal.
We considered three common patient-to-doctor behaviors, including whether to choose the doctor, whether to give a psychological/material gift, and whether to give a higher score. We will review the related literature in more detail in Literature review. In short, prior research has focused primarily on physician's online reputation, rather than on offline reputation changes. To the best of our knowledge, this paper is one of the first attempts to shed light on the impacts of physician promotion (offline reputation changes) in OHCs. Specifically, we consider three research questions. First, if physicians are promoted, will this result in an increase in the number of patients they serve online? The number of patients is not only a response to the patient's preference for the physician but also an implicit indication of the physician's performance and the patient's willingness to continue participating in OHCs. Second, if physicians are promoted, will they receive more psychological or material rewards from patients? The psychological and material rewards given by patients can be considered as social and economic returns received by the physician, respectively. Third, if physicians are promoted, will they receive higher ratings from patients? The patients’ ratings can indicate not only satisfaction but also the online reputation of the physician. In other words, attempting to answer this question is equivalent to exploring the impact of a change in a physician's offline reputation on his/her online reputation.
The main innovations and contributions of this study are in two areas. First, to the best of our knowledge, previous studies related to physician reputation have not explored the effects of changes in physician reputation; thus, they have not demonstrated that an effect of physician reputation does indeed exist. For example, when studies have shown that chief physicians are able to attract more patients than attending physicians, this may reflect more the impact of the quality of the physician himself than the impact of physician reputation. For empirical studies, the challenge in addressing this bias lies in the availability of data. Specifically, if we want to know what changes occurred before and after a physician was promoted, we must select a number of physicians to serve as our sample, but it usually takes years for a physician to receive a promotion or even to fail to receive a promotion. This leads to difficulty in collecting a sample large enough for conducting the analysis. Fortunately, OHCs have a large number of physicians that have real public information associated with them, so even if only a small percentage of physicians are promoted, there are still enough physicians who have been promoted during a given period to serve as a sample for our study. Thus, after collecting data from the OHC, this study was able to isolate the effect of physician reputation by using the Difference-in-Difference (DiD) approach with propensity score matching, 9 and we were therefore able to explore whether physician promotion (or a change in physician reputation) really had an effect on the variable of interest in OHCs. From the perspective of signaling theory, 7 because physician quality does not change significantly in the short term, changes in patient behavior must reflect how patients interpret the messages implicit in physician promotions.
Our second contribution is to expand the literature on the impact of physician reputation on online communities. Compared to most online community studies that use the term reputation to refer to the “online” reputation of members, this study makes use of the “offline” reputation. Specifically, since members in an online community are usually not required to reveal their real identities, for this study, their reputations were derived from reviews by other members of the OHC or from virtual titles given by the platform. However, in order to avoid the spread of inaccurate medical information, physicians in OHCs are certified by the platform. Therefore, the physician's real identity is known, which makes possible exploration of the impact of the members’ offline reputations on the OHC. The research question for this study was the effect of physician promotion on the number of the physician's online patients, the number of rewards offered by patients, and the physician's online score. It is worth noting that a physician's online score is also a type of online reputation, so we also explored whether offline reputation affects online reputation, a question also unaddressed in previous studies.
Here, we briefly describe the specific work and main findings of this study. After observing more than 140,000 physicians on the Good Doctor website for 25 months, we identified 280 of them who were promoted at month 13 as a treatment group and obtained a control group by propensity score matching. With the use of the DiD approach, our results show that that physician promotions led to more patients choosing the physician, made patients willing to give more psychological rewards, and made them inclined to give the physician a higher online rating. The first finding is not surprising. According to signaling theory, physician promotions can attract more patients. It is worth noting that under our study design, physician quality is unlikely to change significantly in the short term (one year). The latter two findings, however, suggest that patients are still more likely to feel satisfied and therefore give more psychological rewards, or higher ratings, even under conditions where the physician is of the same quality and the patient has already interacted with the physician.
This paper is arranged as follows. We present a literature review related to OHCs and physician reputation in Literature review. Method and dataset briefly introduces the research method, i.e., the DiD approach with propensity score matching, and then we describe the data collection process and explain how the variables were measured. In Results, the results of the relevant analyses, including non-parametric and parametric estimates, are reported. Furthermore, we provide robustness test results for different observed period lengths. Discussion discusses the theoretical meaning and practical implications of these findings, as well as explaining the limitations of this study. Finally, the conclusions are presented in Conclusions.
Literature review
Online healthcare community
An OHC can be viewed as a complex system that contains three elements, namely, platform, information content, and users, all of which are interdependent and interact with each other. Most of the studies from the perspective of platform function have explored the benefits that OHCs can bring such as reducing urban-rural disparities 3 and providing information or emotional support.10–12 The literature related to information content focuses on issues such as mining new knowledge from the content13,14 and ensuring information quality. 15 The last category of literature related to users includes studies of physicians and patients, where the motivation of participation, individual characteristics, and physician-patient interaction are the most frequently discussed topics. For example, Guo et al. 16 explore the impact of status capital and decisional capital on physicians’ social and economic returns based on social exchange theory. Meng et al. 17 find that physicians can recruit more paid patients if they share more knowledge in OHCs. Since physician reputation is closely related to the subject of this paper, we will postpone a detailed discussion of it to the next subsection.
As our primary purpose is to reveal how the promotion of physicians may lead to changes in patients’ behavior toward them, we next review related works on OHCs from the perspective of three aspects of patient behavior. First, understanding how patients choose their preferred physicians is important for the development of OHCs, and this issue is similar to the question of how to increase the number of patients served by physicians. Previous studies have shown that both physician and hospital reputation can have an impact on the number of patients served by physicians.18–20 Recently, Yang et al. 21 have further indicated that the reputation and experience diversities of physicians’ teams have positive influences on team performance, which is measured by the number of patients consulting with physicians. The second issue is how to make physicians more willing to expend greater effort on an OHC. The most common way is to set up relevant reward systems that allow physicians to receive material or psychological rewards from patients, which usually leads to an increase in physicians’ online contributions. 22 Notably for physicians, psychological rewards include not only thank-you letters but also improvements to the social reputation of the physician. 16 Therefore, the number of rewards that patients are willing to give to physicians is also a critical factor influencing the development of the OHC. Third, patient satisfaction with the physician, or the physician's online score, is the most direct indicator of whether the use of the OHC has been beneficial to the patient. Therefore, it is relevant to explore the factors that influence physicians’ online evaluations.13,23 Overall, from the patient's perspective, their preference for what physician to choose, their decision on how much to reward the physician, and their evaluation score of the physician are all closely related to the development of the OHC. The present study's purpose is to examine the impacts of physician promotion on these three variables.
Physician reputation
Reputation is understood as the conditional probability that an individual will behave in a certain way. 24 A common way for individuals to develop reputation is by interacting with others while having these behaviors recorded and available for others to view. Another way is by providing credentials that are recognized as reliable, e.g., a physician's or lawyer's certificate. Potential counterparts use this information to derive conditional expectations of the individual's future behavior. Early studies of reputation generally used experimental designs, but with the growth of the Internet, there have been significant advances in the application or measurement of reputation in e-commerce or online communities. Reputation is one of the most critical factors affecting consumer behavior and seller performance in online marketplaces, 19 and it helps to reduce information asymmetry and uncertainty. 25 The most typical means of reputation measurement is via online customer ratings or satisfaction. However, studies further employ sentiment signals to estimate the reputation polarity of text contents.26,27
The information asymmetry in the healthcare context is exacerbated by the fact that healthcare is a credence product, meaning that physicians know more about the quality of services and the health status of patients than the patients themselves. 6 Therefore, reputation has been identified as an important factor influencing online patient behavior in OHCs. 28 In general, physicians can build up an online reputation through online behavior, as past behavior can be observed by all patients. 29 For example, Wu and Lu 30 found that a physician's reputation positively influenced the likelihood that patients would share their treatment experiences, and Yu et al. 20 noted that physicians receiving virtual honors from the OHC could increase personal page views. Although abundant research has explored the role of online reputation in OHCs, research addressing the role of offline reputation change remains scarce. In particular, little is known regarding how patients’ behavior changes when they learn of physician promotion, which is equivalent to a physician obtaining a better offline reputation.
Method and dataset
Natural experiment design is one of the most frequently used methods in impact evaluation studies, but due to ethical or cost reasons, it may be difficult to implement, especially for studies relying on observational data. For example, when one attempts to investigate the impact of the implementation of certain policies, one should note that the targets of policy implementation are usually not determined by random assignment, so results obtained by directly comparing differences before and after policy implementation are likely to be biased. In our context, since it is impossible to randomly promote some of the attending physicians to associate chief physicians and then assess the impacts on the OHC, we had to adopt other methods. One of the feasible solutions was using the DiD approach, a quasi-experimental research design for estimating causal effects that is popular in social science fields.20,31,32
Difference-in-difference approach
In general, the DiD approach is used to investigate the effect of a certain intervention on outcome variables. Here, we first introduce its basic terms and concepts. The term “treatment” usually refers to a specific intervention, and a treatment group is defined as all individuals in the group who were exposed to the intervention. For example, in this study, physician promotion was considered a treatment, and the number of patients served in OHC was one of the outcome variables. Since other interventions may have occurred during the study period, such as OHC administrators’ improving the user interface, simply comparing the changes before and after the implementation of treatment in the treated group could not rule out the impact of other interventions. To solve this problem, the DiD approach usually considers another control group, in which individuals have not been exposed to the intervention of interest. The creation of a comparable and balanced untreated group is an important prerequisite. Propensity score matching (PSM) is a common approach that minimizes selection bias in an observational study. We first focus on the DiD approach and then introduce PSM in Physician reputation.
To formalize the concept described above, following,
33
the basic DiD approach uses data from two groups (the treatment and control groups) and two time periods (the pre- and post-treatment periods). With a sample of data, the DiD estimate (

To obtain the significance level of the DiD estimate, we adopt a regression model of the general form


Propensity score matching
The main benefit of using randomized experiments to investigate causality is that, because both the treatment and the control groups are randomly assigned, the covariates or characteristics of the sample are not usually significantly different from each other. This ensures more efficient estimates of treatment effects. To achieve the same objective in observational studies, researchers have proposed several matching methods to balance (or equate) the distribution of covariates in the treatment and control groups. 34 Among them, propensity score matching is a standard one and was first introduced by Rosenbaum and Rubin. 35 The propensity score is defined as the probability of receiving the treatment, conditional on observed covariates. 36 Although some nonparametric methods such as generalized boosted models or boosted CART usually show good performance, 37 using logistic regression to estimate the propensity score is still the most common approach. In practice, these matching methods are becoming easier to implement due to advances in software tools. 38 In this study, we adopted the package MatchIt in R to implement the related PSM estimations. 39
Data collection and measures
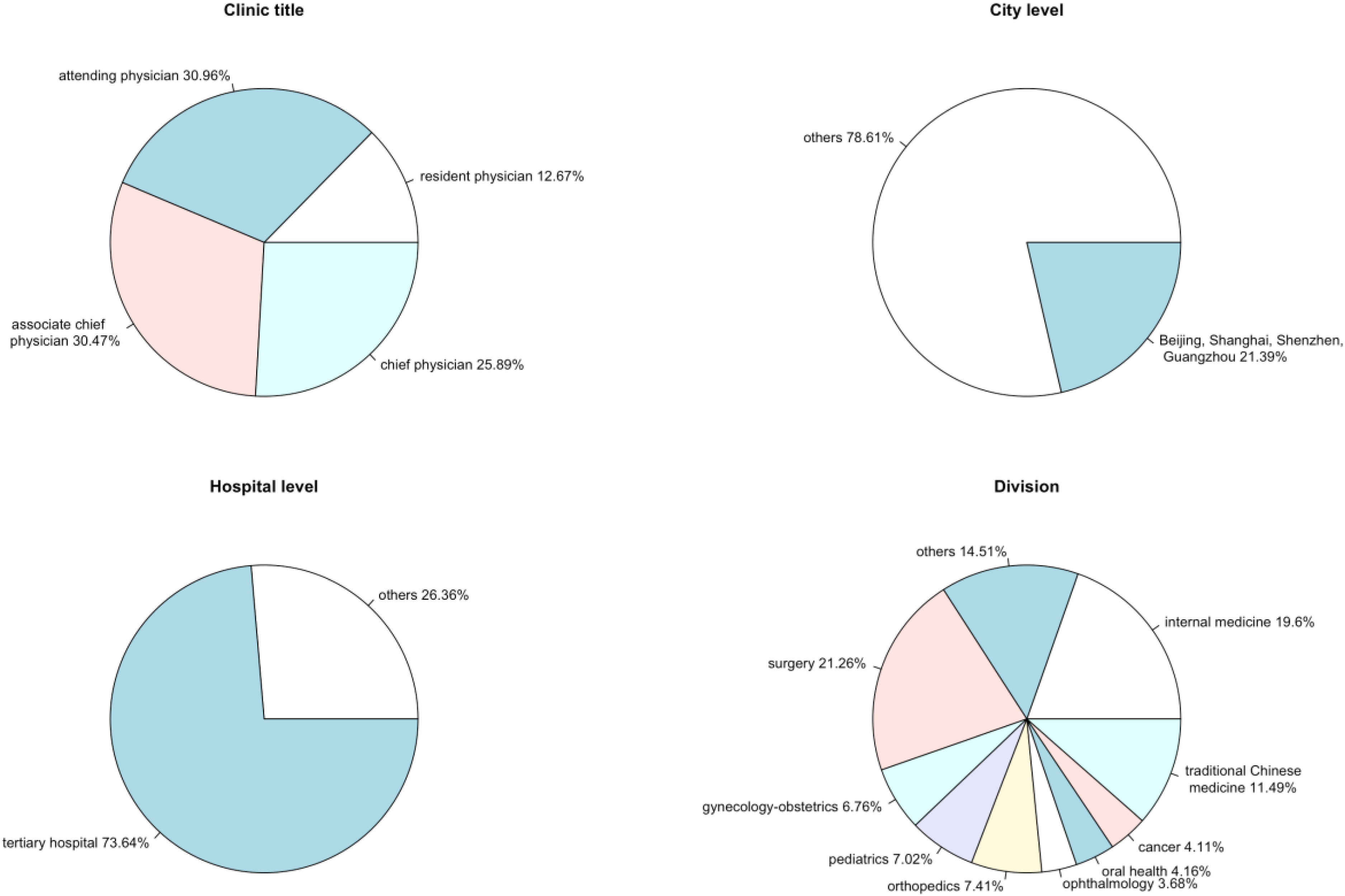
The sample for this study was taken from the Good Doctor website (https://www.haodf.com), which is one of the most popular OHCs in China. To explore the impact of physician promotion on the OHC, we conducted four rounds of data collection, over more than two years. In July 2017, at the time of our first data collection, more than 140,000 physicians had already created individual profiles (personal pages) on the website, in which the variables we needed could be observed. At the next three points in time, July 2018, August 2018, and August 2019, we performed the same data collection procedure. If a physician missed any of the variables in these four collections, that physician was excluded from the study sample. In this way, our sample eventually covered 111,742 physicians from 3718 hospitals. As shown in Figure 1, these physicians had different clinic titles and came from different cities, different levels of hospitals, or different divisions, so this sample is not limited to a specific field. The four rounds of data collection allowed us to divide the study period into three time periods, with the first one used to record changes in various physicians’ characteristics, the second, shorter, period used to determine which physicians were promoted during this period, and the third one used to observe how physician promotion affected the OHC. For convenience, we refer to these three periods as the pre-treatment, treatment, and post-treatment periods.
Sample characteristics.
Two points about the data collection procedure deserve further explanation. First, due to the fact that we could not readily observe whether a physician was promoted, or a physician may not have updated her or his latest clinic title immediately, we set up a treatment period to determine whether a physician was promoted. During the entire study period (25 months), a total of 280 physicians were promoted during the treatment period (1 month), 7715 were promoted at other times (24 months), and the remaining 103,747 physicians were not promoted. These 280 physicians formed the treatment group, while the control group members were selected from among 103,747 physicians through PSM. Second, it would have been inappropriate to explore the impact of promotion on OHC over a short period of time (e.g. 1–2 weeks) based on the treatment group obtained over a 1-month length of the treatment period. Therefore, we set the length of both the pre-treatment and post-treatment periods to 1 year, and this setup allowed us to explore the long-term effects of physician promotion. For example, we were able to compare the number of patients served online 1 year before and after physician promotion. Next, we explain in detail how the variables used in this study were measured after 4 rounds of data collection.
Table 1 summarizes the definitions and measures for all variables. First, a physician's clinic title (CT) is the key variable in this study and was used to determine whether a physician was promoted. In general, after a certain number of years of practice, each physician can be promoted within his or her clinic after the government assesses whether his/her competencies meet certain requirements; the formal clinic titles from lowest to highest are resident physician, attending physician, associate chief physician, and chief physician. Then four outcome variables were considered. The Good Doctor website allows physicians to provide online consultation services for patients, and the total number of patients receiving such online services was recorded on the physician's individual web page. We define the number of patients served by the physician online as PT. After a patient chooses a physician, he/she can rate the physician online and even write a thank-you letter or provide a token gift to the physician. Based on these patients’ behavior towards physicians, we defined three other outcome variables: online score (SCORE), psychological reward (PR), and material reward (MR). SCORE was calculated based on the average of the online scores (from 1 to 5), where 5 was the highest score. PR and MR were measured by the numbers of thank-you letters and token gifts received by the physician from patients, respectively. Since the token gift can be converted into cash and deposited into the physician's personal research fund, which can bring some economic benefits to the physician, we regarded it as a kind of material reward.
Variable definitions and measurements.
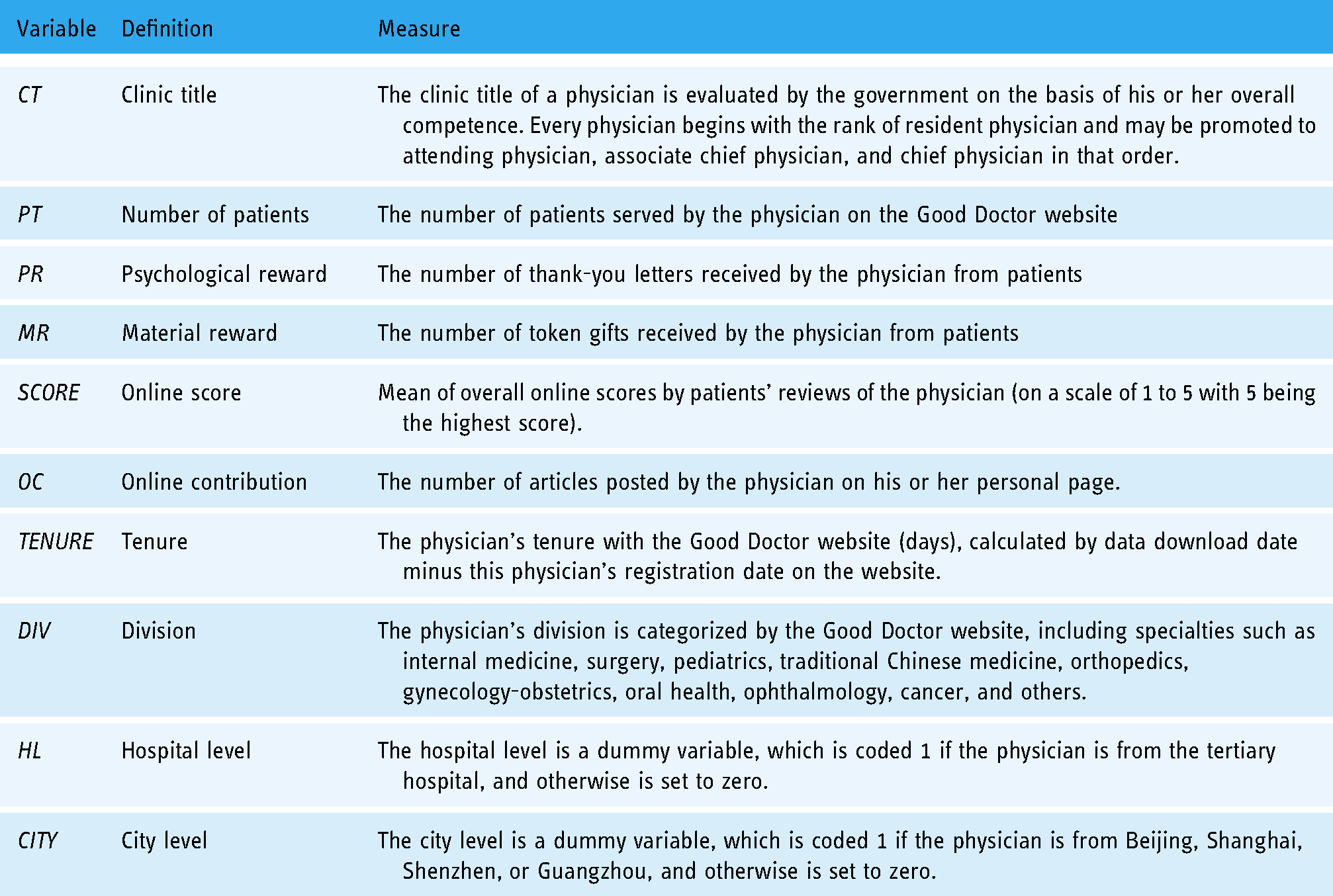
In addition to the outcome variables mentioned above, five variables related to physician characteristics were collected from the Good Doctor website and used as covariates to match the control group. The first covariate was the online contribution (OC), which is used to evaluate how much effort a physician expends on work in the OHC. In this study, we measured a physician's OC as the total number of articles published by him/her. The second was the physician's tenure on the Good Doctor website (TENURE), which was determined by the number of days the physician had been registered on the website. The importance of both OC and TENURE to the OHC has been verified in recent literature.20,22 The remaining three covariates are all related to the offline characteristics of the physician, i.e., division (DIV), hospital level (HL), and city level (CITY). DIV is a categorical variable, which is divided into 10 groups by the Good Doctor website according to the physician's specialty, which might be internal medicine, surgery, pediatrics, traditional Chinese medicine, orthopedics, gynecology-obstetrics, oral health, ophthalmology, cancer, or others. HL is a dummy variable for hospital level, set to 1 if the physician was from a tertiary hospital and zero otherwise. Finally, CITY a dummy variable for city level, set to 1 if the physician was from Beijing, Shanghai, Shenzhen, or Guangzhou and zero otherwise.
Complete analysis process
Figure 2 shows the four rounds of the data collection process and indicates how the variables of interest were used in our empirical analysis. It should be noted that the variables have the subscript i for physician i and the subscript t for different periods, with 

Data collection and processing.

Research framework.
Results
Treatment and control groups
To match the 1:1 balanced control group, we estimated propensity scores using a logistic regression model, as shown in equation (3). According to the fitted model, we obtained a control group sample with a sample size of 280, identical to that of the treatment group. By determining whether the distribution of propensity scores was similar between the different groups, we were able to discover whether or not the matching performance was good. Figure 4 is a jitter plot where each circle indicates a physician's propensity score. The uppermost stratification includes no cases, indicating no mismatched treatment units. The middle two stratifications show that the treatment group and the matched control group had similar distributions in their propensity scores. The final stratification shows unmatched control units and was not used in any subsequent analysis. Obviously, PSM is useful for constructing a well-balanced control group. In addition to the jitter plot, we also looked at the sample characteristics of the treatment and control groups as shown in Figure 5. In terms of the physician's clinic title, since chief physician is the highest rank, it was impossible for chief physicians to be present in the treatment group. While chief physicians were still 8.21% of the control group, compared to 25.89% in the whole sample (see Figure 1), the matching process ameliorated this part of the difference. For the city level, in which 21.39% of all physicians were from large cities and accounted for 32.86% of the treatment group, the control group obtained through PSM improved this proportion to 28.57%. A similar phenomenon was observed in the hospital level. Of the total number of physicians, 73.64% came from tertiary hospitals, while these accounted for 86.78% of the treatment group and 89.64% of the control group. As for the percentage of physicians belonging to different divisions, there was no significant difference among the whole sample, the treatment group, and the control group.

Distribution of propensity scores.

Sample characteristics of treatment and control groups.
Impacts of physician promotion
This study investigated the impact of physician promotion on the OHC. Specifically, four outcome variables were used to determine whether promoted physicians were able to attract more patients online, whether promoted physicians received more psychological or material rewards from patients, and whether promoted physicians were more likely to receive higher ratings. A nonparametric method was adopted to investigate these issues. Specifically, for the treatment and control groups, the data were divided into pre- and post-treatment periods; then the averages in these four groups were used to calculate the double difference as in equation (1). Table 2 reports the related results. For instance, for the outcome variable patient, the average values in the four groups are
Nonparametric estimation results.

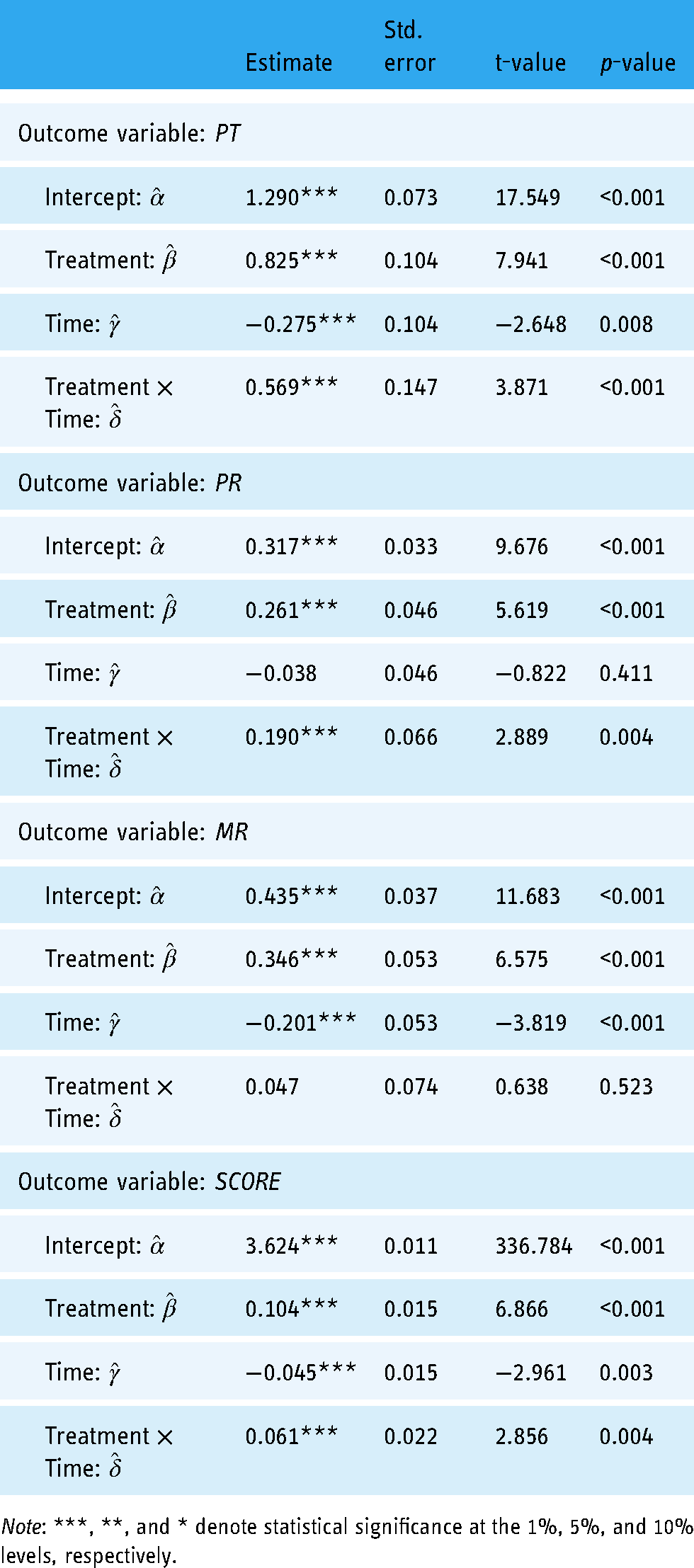
Table 3 displays the parametric estimates of DiD effects for each outcome variable according to the regression models as shown in equation (2). The DiD estimates (
Parametric estimates of DiD effects.

Note: ***, **, and * denote statistical significance at the 1%, 5%, and 10% levels, respectively.
The robustness tests
The previous study design used a 1-month period to see which physicians had promotions. The advantage of doing this is that the physician promotions count be concentrated within 1 month, which allowed the true difference in the length of each physician's pre-treatment period or post-treatment period to be within 1 month. The disadvantage, however, is that the number of physicians in the treatment group was small, a sample of only 280. We thus extended the observation period to 3 months to increase the sample size of the treatment group and then carried out the same analysis procedure to verify the robustness of the previous results. Specifically, the four rounds of data collection were July 2017, June 2018, September 2018, and August 2019. In other words, the lengths of the pre-treatment, observation, and post-treatment periods were 11 months, 3 months, and 11 months, respectively. In this case, the sample size of the treatment group was expanded to 737, and the control sample was matched according to the same PSM method. In this subsection on the robustness test, we omit the discussion of PSM results and present the results of the DiD estimates directly in Table 4. Overall, all results are consistent with the previous finding of a significant positive effect (at a less than 1% significance level) of physician promotion on patient numbers, psychological rewards, and online scores.
Robust tests with a longer observed period.
Note: ***, **, and * denote statistical significance at the 1%, 5%, and 10% levels, respectively.
Discussion
Main findings
This study observed 111,742 physicians’ profiles on the Good Doctor website over a 2-year period. The sample ultimately included physicians from 10 medical specialties, 3718 hospitals, and 31 provinces in China, so the diversity of the data ensured the representativeness of the empirical results. We then used the DiD approach with PSM to verify the causal relationship between physician promotion and several outcome variables of interest. Based on the empirical results, we can clearly answer the three research questions raised in Introduction. Physician promotion leads to more patients choosing promoted physicians, making patients willing to give more psychological rewards, and making them tend to give promoted physicians higher online ratings. Next, we discuss further the theoretical and practical implications.
Theoretical implications
Intuitively, physician titles can indicate to patients the true quality of their physician, which helps patients make better medical decisions. However, are patients really interpreting the physician title correctly? Suppose a physician's true qualities do not change significantly in the year before and after a promotion; then any change in patient behavior toward the physician when a higher title is obtained may be due to the patient's misinterpreting the signals conveyed by the original or new title. For example, patients prefer highly qualified physicians, and if there is a significant increase in the number of patients after a physician is promoted, that means patients may have underestimated the significance of the original title or overestimated that of the new title. Although many studies have taken physician title into account, it is usually set as a control variable with no significant effect on outcome variables such as patients’ trust in physicians or patient satisfaction. 23 However, this study looked at patient behavior toward physicians before and after physician promotion in an effort to better understand the impact of physician title (reputation) change. Thus, we provide clear evidence for the importance of physician promotion in explorations of OHC topics.
Physician reputation can be divided into online and offline reputation, with the former usually measured by online scores and the latter measured by physician title or hospital level. Although both online and offline reputation have been considered in past research models, 19 the relationship between the two has not been considered. To our knowledge, no one has explored whether the physician's offline reputation affects his or her online reputation in the past, and the current study fills this gap. By comparing online scores one year before and after a physician's promotion, we find that a physician's promotion (offline reputation) results in a significant increase in online scores (online reputation). Indeed, healthcare services are often viewed as a credence commodity, 6 characterized by the fact that the physician knows better than the patient what he or she needs, and it is difficult for the patient to even judge the effects of receiving the service. Thus, if patients had more prior trust in their physicians, they would be more likely to improve their ratings of the care they received, even if the medical procedure were no different. If physicians have better online scores in the OHC, it will both encourage physicians to continue their activities and attract more patients to the platform. Based on the above results, OHC managers or physicians themselves should pay more attention to finding ways to increase patient trust in physicians. While physician titles cannot be arbitrarily changed, other information such as awards, journal publications, or professional certificates can be provided to aid in achieving a similar goal.
Practical implications
We provide two practical implications. First, via a comparison of the number of new patients added in the OHC one year before and after the physician's promotion, the empirical outcomes significantly support the conclusion that a physician's promotion leads to an increase in the number of patients served online. In other words, patients are not willing to choose a lower-title physician even if the physician's quality is not significantly different. This phenomenon reveals a disadvantage faced by younger physicians in the OHC, who typically take years to qualify for higher titles, but this does not mean that they cannot provide the same medical service. The over-concentration of patients with higher-title physicians points to an uneven distribution of health care resources, which can leave higher-title physicians with too much work and result in lower-title physicians’ no longer participating in the OHC because they have no patients; thus, OHC managers should seek to solve this problem. However, it is not reasonable to hope that patients will completely change their minds about physicians’ titles. We suggest that OHC managers refer patients to younger, lower-title physicians when they have low-risk illnesses such as colds or tooth decay. In the short term, this would reduce the burden on higher-title physicians while providing lower-title physicians the opportunity to prove their competence. In the long term, this practice would have a good chance of changing patients’ physician-selection habits.
Second, under the incentive system set up on the Good Doctor website, physicians can receive thank-you letters and token gifts from patients, which can be considered as psychological and material rewards, respectively, for physicians’ participation in the OHC. These incentives have been shown to increase physician engagement and thus contribute to the development of the OHC. 22 This study explores how physician promotion affects patients’ reward behavior. Comparing the number of thank-you letters or virtual gifts received by physicians in the year before and after their promotion, we found that patients were more likely to write thank-you letters to physicians after the physicians’ promotion but did not show increased willingness to give token gifts. The latter outcome diverges from our expectations. Past studies based on the social exchange theory 40 have pointed out that a physician's status capital such as his/her clinic title can bring him/her more economic or social returns. 16 However, our results only partially support the findings of the above-mentioned study. Both non-parametric and parametric results show that there is no causal relationship between a physician's promotion and the number of virtual gifts she/he receives. A possible reason is that when patients pay for a token gift, they might think more carefully than they do when writing a thank-you letter about whether the cost is worthwhile. In other words, when patients no longer base their decision to give a token gift only on a simple impression of the physician, basing it rather on an assessment of the physician's overall performance, the effect of physician promotion ceases to exist. This implies that patients would be equipped to accurately interpret the signal of a physician's title, if only they would take the time needed to make the assessment accurately. Thus, the amount of material rewards a physician receives is more reflective of an accurate evaluation of him or her than is the number of psychological rewards. For OHC managers, finding ways to make patients willing to carefully evaluate physician performance before offering rewards will help the platform retain more good physicians.
Limitations and future work
As with many OHC studies, because our sample was collected from a specific OHC platform, we must acknowledge that it was difficult to include additional variables due to limitations in data availability. The adoption of more physician-related variables can be expected to reduce the potential bias in the selection of the control group with PSM. Moreover, several other limitations may point to future research themes. First, it is known that people's online behavior is influenced by cultural differences such as individualism-collectivism or long-term orientation.41,42 However, all samples in this study were from the Good Doctor website in China, so cultural or healthcare system differences may lead to conclusions from this study different from those that would be found in other countries. In addition, the promotion systems or titles of physicians in different countries are also interesting topics in terms of their impact on patient behavior. Second, due to academic ethics and cost considerations, this study did not collect variables related to personal patient information, such as education and income. However, we believe that some characteristics of patients might be critical variables moderating physician promotion that then influence their behavior. Future studies including such variables should be conducted in collaboration with the OHC platform with the permission of the patients. Finally, since OHC records often contain large amounts of textual data about physician-patient interactions, many studies have attempted to obtain more useful information from these materials. For example, researchers have used text-mining techniques to measure how much emotional and informational support physicians provide, and these variables have been found to have a significant effect on patient satisfaction 13 ; other studies have used topic models to automatically extract hidden topics from reviews and explore whether there were differences by area of expertise. 43 While this study explored the impact of physician promotion on the number of patients, the number of awards, and online scores using a number of established metrics from the OHC, a careful analysis of the text of patient reviews may answer to other meaningful questions related to physician promotion.
Conclusions
Information asymmetry is a common problem in OHCs, and conveying the true quality of physicians to patients through reputation can be a way to alleviate this problem. Employing a large amount of real-world data from the Good Doctor website, this study used the DiD approach with PSM to verify the causal relationship between physician promotion (improvement in physician offline reputation) and certain variables of interest that are useful for measuring changes in patients’ behavior toward physicians. We concluded that a physician's promotion results in an increase in the number of patients served online, an increase in the psychological rewards received by the physician, and an increase in the physician's online score. In other words, when patients have realized that a physician has a higher title, they are more likely to choose that physician, give that physician more psychological rewards, and even give that physician a higher online score. Because the true quality of a physician does not change significantly in a short period of time, changes in patient behavior are likely to come from patients’ underestimating (overestimating) the quality of the physician as represented by the original (new) title. In addition, we found that patients do not give more material rewards as a result of physician promotions, suggesting that patients are more likely to perceive the true quality of physicians if they think more carefully before deciding whether or not to reward a physician. Based on these results, we suggest that OHC managers should provide more incentives to young physicians with lower titles to make them more likely to remain on the platform. While physician reputation can send a message to patients, it is also important to ensure that patients are able to discern such messages. Physicians in OHCs, whose offline reputation affects their online reputation, should provide more detailed personal information to reinforce patients’ trust in their professional competence, thereby enhancing their online reputation. In summary, this study provides empirical evidence of the impacts of physician promotion on the online healthcare community and extends prior research on reputation, with implications for theory and practice.
Footnotes
Acknowledgements
Yuan-Teng Hsu gratefully acknowledges financial support from Shanghai Business School.
Author contributions
All authors contributed equally to this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the People's Republic of China (grant number 20YJCZH199).
Ethical approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial registration
Not applicable, because this article does not contain any clinical trials.
Guarantor
Yuan-Teng Hsu.