
Abstract
Background
Patient activation and engagement can improve outcomes of medical and surgical care by increasing involvement of patients in their care plan. We designed a digital engagement tool to improve surgical cancellation and post-surgical outcomes for adult patients undergoing total joint replacements by providing patient education materials via email or text, in small increments throughout the perioperative period.
Methods
We assessed the tool's impact using a quasi-experimental design comparing patients scheduled for surgery January–June 2017 (pre-intervention) versus January–June 2018 (post-intervention). Post-intervention patients with digital contact information in the medical record were automatically enrolled. We extracted de-identified administrative data for all patients during both time periods and utilized an intent-to-treat approach including all post-intervention patients regardless of enrollment. Surgical cancellation and post-surgical outcomes (length of stay, discharge to home and revisits and readmissions) were compared between periods using adjusted regression models. We also examined associations between measures of engagement with the intervention and outcomes.
Results
A total of 2027 joint replacement patients were included (720 hip replacements; 1307 knee replacements). Adjusting for gender, age and insurance type, both hip and knee patients in the post-intervention group were more likely to have a cancelled surgery, but cancellations were less likely to be on the day of surgery compared to pre-intervention patients. Post-intervention patients were also less likely to have length of stay >2 days. Forty- three per cent of hip and 47% of knee patients in the post-period received the intervention and most were highly engaged. Higher engagement was associated with lower odds of surgical cancellation, shorter stays and higher odds of discharge home.
Conclusion
Findings suggest that utilization of a digital patient engagement tool translates into improved hospital efficiency and patient outcomes, particularly for those highly engaged.
Keywords
Introduction
Total joint replacement, specifically hip or knee replacement, is one of the most common adult surgical procedures with over 1 million procedures annually in the United States and increasing volume due to an ageing population and advances in artificial joint technology.1–4 Total joint replacement can be expensive due to long hospital length of stay (LOS), common discharge to skilled nursing facilities (SNFs) and frequent unplanned hospital revisits and readmission.3,5 A 2013 study by Bozic et al. estimated that nearly 40% of total cost for a total joint replacement episode occurs after discharge. 6
Recent studies have demonstrated improved outcomes following total joint replacement when patients are discharged home rather than to a SNF, resulting in additional cost savings as routine home discharges are typically shorter and less expensive.5,7 Additionally, discharge to SNFs has been associated with increases in post-op complications, unplanned readmissions and increased overall costs with discharge to SNFs as one of the strongest predictors of complications within 30 days of discharge. 8 The recent push towards reducing post-operative LOS and increasing discharge home in the era of bundled payments has demonstrated that shorter LOS and increased discharge home do not result in higher readmission rates and can result in significant cost savings.7,9,10
Surgical cancellation is another source of high costs to the healthcare system. 11 A 2011 study from Tulane University found nearly $1.5 million in lost revenue due to cancelled surgeries in a single year. 11 Cancellations are often due to patient-related factors – including illness, failure to comply with preoperative instructions, inconvenient appointments and patients believing they are unfit for surgery – with estimates for patient-related reasons for cancellation as high as 68%.11,12 Because total joint replacement is an elective surgical procedure with potentially long recovery times, these patients may be more prone to cancellation. 12 Though there is not much literature on cancellation in total joint replacement surgeries, Campbell et al. found 3.4% of orthopedic surgeries were cancelled with the highest cost per case for any specialty at $7178 per cancellation. 11
Hospitals are eager to optimize patients efficiently for total joint replacement and other surgical procedures.11,13 This includes communicating with them about how to prepare for surgery and answering questions about the logistics of the surgery, as well as what to expect regarding post-operative recovery and rehabilitation.13–15 To this end, many hospitals prepare printed guides that they give to patients and their families with educational materials and instructions, while some hospitals may combine printed information with in-person classes.13–15 However, patient uptake of printed education and instructions is limited by the fact that the materials are easily misplaced, discarded or simply forgotten about.
Patient activation through education and engagement has been shown to improve the outcomes of medical and surgical care by increasing and sustaining patient involvement in their care plan.15,16 Studies have shown that activation results in patients taking a more participatory role in their healthcare and are thus more likely to engage in healthy behaviours, which can translate to reduced utilization of the healthcare system and cost savings. 16 Improving patient engagement is especially critical in an ageing population with especially low health literacy and patients who are typically not engaged in their own health care for a variety of reasons.13,17,18 Increased patient activation prior to total joint replacement surgery has been shown to improve patient-reported outcomes, including reduced anxiety prior to surgery and improved post-surgical pain relief, as well as increases in patient satisfaction and quality of life.13,14,18–20 A focus on preoperative patient education coupled with other post-operative interventions has also demonstrated shorter LOS without an increase in readmissions.10,14,21
Adoption of digital health tools has been leveraged to improve patient activation and outcomes by increasing patient knowledge, boosting confidence and setting expectations, as well as enhancing healthcare interactions.22–26 Healthcare systems have increasingly begun to offer a range of digital health tools – including patient portals, electronic personal health records (ePHRs), websites and mobile apps – in an attempt to engage and activate patients.22,24–26 Prior studies of digital tools in total joint replacement specifically have demonstrated that even older patients can benefit from direct digital healthcare support.10,23 However, there are often barriers to access, including privacy and security concerns, accessibility and lack of acceptability and perceived value of digital health tools among target populations (e.g. older adults).22,24,25
For total joint replacement patients, we hypothesized that providing patient education materials digitally, via email or text, in small increments pre- and post-operatively timed to the date of surgery, would be a superior way to educate patients and result in higher patient activation and engagement, translating into lower hospital utilization and improved outcomes than traditional educational material given all at one time. We, therefore, designed an easy-to-use digital health engagement tool to deliver patient education and instructions incrementally through the full episode of care with the goal of improving patient engagement and activation perioperatively among adult patients undergoing total hip or knee replacements. Our study used a quasi-experimental design to assess the impact of this digital education tool by comparing surgical cancellation, length of hospital stay, discharge home and readmissions and revisits for all total joint replacement patients over the 6-month post-intervention period to all total joint patients over the same 6-month period of the previous year. We hypothesized that by increasing patient activation and engagement in care perioperatively, use of the tool would be associated with decreased surgery cancellations, increased discharge home, shortened LOS and decreased revisits.
Methods
Digital health patient engagement tool
The patient engagement tool we used comprised a series of 22 sequenced digital prompts, delivered via email or short message service (SMS) text message. These easy-to-read prompts sought to activate joint replacement patients with timely, concise information delivered from the time the surgeries were scheduled through 6 months of post-operative rehabilitation. There were 9 preoperative prompts, followed by 13 post-operative prompts (Figure 1). The multimedia messages – which included text, videos, slideshows, images and interactive tools – were crafted to engage a variety of learning styles. Examples of the messages can be found in Figure 2. The evidence-based information was sourced from leading medical, academic and government organizations (e.g. the National Institutes of Health, Centers for Disease Control and Prevention, American Academy of Orthopedic Surgeons et al.) and was reviewed and revised by the healthcare system's Joint Council. Content was presented in a concise, simple format with minimal use of medical jargon to enable easy skimming, while also offering access to more details on key topics via links to associated web pages. The digital outreach also included patient-reported feedback via surveys, quizzes and secure one-to-one, patient-provider messaging.

Overview of timing and content of messaging throughout the perioperative period.

Examples of messaging: a – preoperative preparation for surgery pain management (mobile view); b – post-operative pain management (desktop view); c – post-operative infection prevention and blood clot prevention (mobile view).
The information aimed to set patient expectations about the procedure, post-operative recovery and the return to routine activities. It included content to promote pre- and post-operative preparedness, answer frequently asked questions and foster adherence to self-care instructions.
Unlike other digital patient engagement tools (e.g. patient portals, ePHRs, mobile apps and websites),22,24–26 the tool employed in this study (UbiCare's SmarteXp®) was designed for easy patient access and understanding, and minimal effort by the care team. Patients were automatically enrolled to receive the timely prompts via the email or text message channels most of them already used on a daily basis. There were no additional apps that patients had to download or passwords to remember to access the information. This was deemed important due to the widespread perception that many older patients – those who typically undergo total joint replacement – would not be as receptive to digital education if it required using new technologies they had to find, download, set up and learn to use.22,24,25
Study design and participants
This study included patients scheduled for total joint replacement surgery at an 86-bed tertiary care center in the Midwest United States. This study used a quasi-experimental design rather than a randomized controlled trial because the latter was not feasible in the hospital setting at the time of the study. We compared all patients undergoing total joint replacement in the 6-month post-intervention period (January–June 2018) to all patients undergoing total joint replacement in the 6-month period one-year prior to the intervention (January–June 2017).
The intervention tool was connected to the electronic medical record (EMR), allowing for automatic enrollment of all patients with email addresses or SMS text-ready mobile phone numbers recorded in the medical record to receive the educational intervention. All patients scheduled for total joint replacement from January to June 2018 were automatically enrolled to participate in the intervention. Although not all patients received the intervention due to missing or incorrect contact information in the medical record, we considered this an intent-to-treat analysis and conservatively included all total joint replacement patients during the post-intervention period in the post-intervention group. Demographic and clinical information (including surgical cancellation and post-surgical healthcare utilization outcomes) was extracted using administrative data for all total joint patients during the intervention period.
As a comparison group in this quasi-experimental study, data were also extracted for all total joint replacement patients from January to June 2017, prior to the intervention and adoption of the digital health tool when perioperative education and instructions were delivered via a printed guide. To account for seasonal variation and the potential impact of time of year on discharge planning, the pre-intervention group was derived from the same 6-month period one calendar year prior to the intervention.
This study was approved by the healthcare system's interdisciplinary Joint Council. The study was not subject to Institutional Review Board (IRB) approval and patient consent was not required. Ethical considerations were addressed by offering the intervention to all patients – regardless of their level of physical impairment – during the intervention phase.
Outcome measures
The following outcome measures were examined in this study: surgery cancellation, day of surgery cancellation, LOS, discharge home, emergency room (ER) revisit and inpatient readmission. Surgery cancellation was defined as cancellation of joint replacement up to and including the day of surgery. Cancellation on the day of surgery was also examined separately. LOS was defined as the time in days between hospital admission for surgery and discharge. A dichotomous LOS variable was also constructed examining LOS longer than 2 days versus 2 or fewer days. The cutoff was chosen empirically based on average LOS. Discharge disposition was collected in the following categories: home, SNF, acute care hospital or died prior to discharge. Discharge to home was defined as discharged home versus discharged to an SNF or an acute care hospital. Revisit outcome measures included any ER visit within 30 days of discharge, any inpatient readmission within 30 days of discharge and any revisit (either emergency department visit or inpatient readmission) within 30 days of discharge. Patients with cancelled surgeries were excluded from the analysis of all post-surgical outcomes.
Engagement measures
Among patients enrolled and participating in the intervention during the post-intervention period, engagement with the prompts (i.e. opening the messages and clicking links for more information) was tracked. The spread in days between enrollment in the engagement tool and the surgery date was collected along with the following measures of engagement with the educational prompts: per cent of prompts opened, per cent of prompts clicked and a three-level categorical engagement classified as ‘high’ (opening ≥50% of the prompts delivered), ‘medium’ (opening 25%–49%) and ‘low’ (opening <25%). The number of prompts opened was not collected for a small number of patients receiving the intervention by SMS text message because there is not a text message ‘open’ equivalent to email opens.
Statistical analysis
The primary analysis utilized a quasi-experimental intent-to-treat design comparing all total joint replacement patients in the post-intervention period to all total joint replacement patients in the pre-intervention period. Given clinical differences between total knee replacement and total hip replacement, all analyses are stratified by joint replaced.
Mean (SD) is reported for continuous variables and frequency (per cent) for categorical variables. The pre- and post-intervention periods were compared on demographic factors (gender, age and insurance) using two-sample t-tests for continuous age and chi-square tests for all other variables (gender, age category, insurance).
Intervention time periods were compared on surgical cancellation and post-surgical outcomes using two-sample t-tests for continuous LOS and chi-square tests for all other variables (surgical cancellation, LOS longer than 2 days, discharge home and readmissions or revisits within 30 days). We examined adjusted associations between the intervention period and outcome measures using multivariable regression analysis. Models adjusted for gender, age category and insurance. We used logistic regression models to examine associations between intervention period and surgical cancellation, LOS longer than 2 days, discharge home and readmissions or revisits within 30 days while continuous LOS was examined using linear regression. We report odds ratio (OR) and 95% confidence intervals (CIs) for logistic regression models and parameter estimate (β) and 95% CIs for linear regression models. Estimates from logistic regression models were used to construct a forest plot with OR and 95% CIs for post-intervention period versus pre-intervention period, stratified by joint replaced.
We examined associations between measures of engagement with the intervention and patient demographic characteristics using chi-square tests (or Fisher's exact test, where appropriate) for categorical measures (level of engagement) and two-sample t-tests or one-way ANOVA for continuous measures (prompts clicked, prompts opened). Unadjusted logistic regression models were used to examine the association between measures of engagement (level of engagement, prompts opened, prompts clicked) and outcome measures (surgical cancellation, LOS >2 days, discharge home and readmissions or revisits within 30 days).
All analyses were performed in SAS (v9.4; Cary, NC, USA) at an alpha level of 0.05. We accounted for multiple comparisons across a number of outcomes by adjusting the family-wise error rate using the Holm–Bonferroni correction to maintain a family-wise type I error rate of 0.05. In tables and figures examining associations with our primary outcome variables, we report uncorrected p-values and indicate which comparisons remained statistically significant after post-hoc adjustment.
Results
Overall, 2027 patients scheduled for total joint replacement were included: 720 (36%) hip replacement patients and 1307 (64%) knee replacement patients. One-thousand eight-hundred and seventy eight (93%) scheduled surgeries were completed and completion did not differ by joint replaced (p = 0.47). In the post-intervention period, 474 (46%) patients with email addresses or text-ready mobile phone numbers in the EMR were enrolled in the intervention. Participation did not differ by joint replaced (p = 0.23). Among patients in the post-intervention period, there were no differences in participation by gender (p = 0.43), age category (p = 0.72) or insurance (p = 0.91) overall.
Hip replacement patients
Demographic and clinical characteristics
Of the 720 scheduled hip replacement surgeries, 383 (53%) patients were in the pre-intervention period and 337 (47%) were in the post-intervention period. Table 1 presents demographic and clinical characteristics by intervention period. Patients were comparable in terms of gender and age distributions but differed significantly by insurance (p < 0.001). Post-intervention patients were more likely to have private insurance and less likely to have Medicare.
Patient demographic and clinical characteristics by intervention group and joint replaced (n = 2027; n = 720 hip replacements; n = 1307 knee replacements).
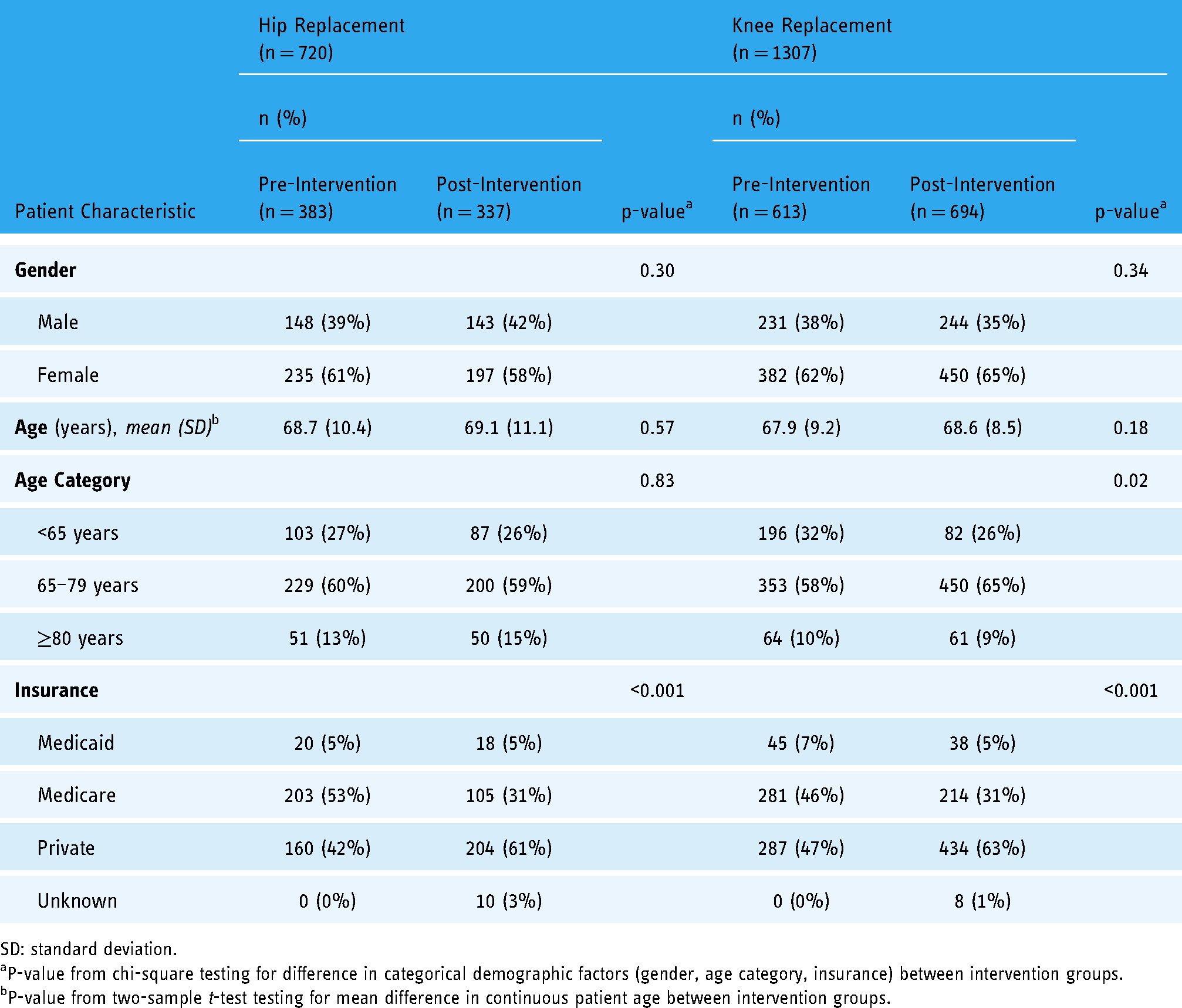
SD: standard deviation.
P-value from chi-square testing for difference in categorical demographic factors (gender, age category, insurance) between intervention groups.
P-value from two-sample t-test testing for mean difference in continuous patient age between intervention groups.
Surgical cancellation and post-surgical outcomes
Table 2 presents unadjusted comparisons between pre- and post-intervention periods on surgery cancellation and post-surgical outcomes. A total of 57 (8%) scheduled surgeries were cancelled, of which 24 (42%) were on the day of surgery. The post-intervention period had more overall cancellations (5% pre vs. 11% post; p = 0.001), but proportionally fewer cancellations were on the day of surgery (76% pre vs. 22% post; p < 0.001). Average LOS was 2.35 (SD = 0.89) days pre-intervention compared to 2.16 (SD = 0.95) days post-intervention (p = 0.007), and patients in the post-intervention period were less likely to stay longer than 2 days (37% pre vs. 28% post; p = 0.02). There were no differences between the periods with respect to discharge disposition or destination, or revisits and readmissions.
Surgery cancellation and post-surgical outcomes by intervention group and joint replaced (n = 2027; n = 720 hip replacements, n = 663 completed surgeries; n = 1307 knee replacements, n = 1215 completed surgeries).

ER: emergency room; LOS: length of stay; SD: standard deviation.
Uncorrected p-values are reported. An asterisk (*) indicates tests that remained statistically significant after accounting for multiple comparisons.
P-value from chi-square testing for difference in cancellation and post-surgical outcomes (LOS>2 days, discharge disposition, discharge destination and readmissions or revisits) between intervention groups.
Among cancelled surgeries (n = 57 hip; n = 92 knee).
P-value from two-sample t-test testing for mean difference in LOS between intervention groups.
Note: One hip patient who died prior to discharge excluded.
Note: One knee patient discharged to acute care hospital included with skilled nursing facility (SNF).
Within 30 days of discharge.
Figure 3 shows adjusted associations between intervention period and surgery cancellation and post-surgical outcomes from logistic regression models adjusting for gender, age and insurance. Post-intervention patients were more likely to have a cancelled surgery compared to pre-intervention patients (OR = 2.42; 95% CI: 1.35, 4.33; p = 0.003). However, among the cancelled surgeries (n = 57), patients in the post-intervention period had much lower odds of cancellation on the day of surgery (OR = 0.07; 95% CI: 0.02, 0.33; p < 0.001). Post-intervention patients were less likely to stay longer than 2 days (OR = 0.65; 95% CI: 0.45, 0.92; p = 0.017) and less likely to have an ER visit within 30 days compared to pre-intervention patients (OR = 0.45; 95% CI: 0.20, 1.00; p = 0.05). Adjusted linear regression analysis indicated that post-intervention patients had LOS 0.22 days shorter compared to pre-intervention patients (95% CI: −0.36, −0.09; p = 0.001; data are not shown). There were no differences between pre- and post-periods on discharge to home, inpatient readmission or any revisit.

Adjusted day of surgery cancellation and post-surgical outcomes for post-intervention versus pre-intervention patients by joint replaced. (n = 2027; n = 720 hip replacements, n = 663 completed surgeries; n = 1307 knee replacements, n = 1215 completed surgeries).
Engagement and outcomes among the intervention participants
Among post-intervention hip replacement patients, 146 (43%) participated in the intervention. Patients participating in the intervention did not differ from those who did not participate with respect to gender (p = 0.07), age category (p = 0.32) or insurance (p = 0.75).
Patients were enrolled in the intervention as early as 131 days before surgery to as late as 36 days after surgery, with the average enrollment occurring 24.3 (SD = 28.7) days prior to surgery. Twenty-four (16%) patients were enrolled in the intervention on the day of surgery (n = 6) or after. Engagement characteristics and surgical cancellation and outcomes among the intervention participants can be found in Table 3. Nearly all participating patients received the intervention via email and 71% were highly engaged (opening more than half of the delivered messages). On average, 67.9% (SD = 33.9) of the prompts were opened and 52.5% (SD = 34.3) were clicked.
Patient engagement, surgical cancellation and post-surgical outcomes among the intervention group by joint replaced (n = 474; n = 146 hip replacements, 133 completed surgeries; n = 328 knee replacements, 303 completed surgeries).

ER: emergency room; SD: standard deviation; SMS: short message service.
Data are not collected for SMS text message subscribers.
Among cancelled surgeries (n = 13 hip; n = 25 knee).
Note: One knee patient discharged to acute care hospital included with skilled nursing facility (SNF).
Within 30 days of discharge.
There were no differences in subscriber type (email or SMS text message) by gender (p = 0.99), age category (p = 0.52) or insurance (p = 0.66). Patients aged 65–79 years were more likely to be highly engaged with the intervention (p = 0.002). Per cent of prompts clicked did not differ by gender (p = 0.10) or insurance (p = 0.49) but did differ by age category (p = 0.04). Patients 65–79 years old clicked the most prompts on average (mean = 57.5%, SD = 32.4), while patients under 65 years old clicked the least prompts on average (mean = 40.5%, SD = 40.5). Per cent of prompts opened did not differ by age (p = 0.08), gender (p = 0.43) or insurance (p = 0.16). Additionally, there was no difference in the days between enrollment and surgery by age (p = 0.55), gender (p = 0.80) or insurance (p = 0.06). Enrollment on or after the day of surgery was not associated with gender (p = 0.27) or age (p = 0.26); however, there were differences by insurance with the majority of late enrollees on private insurance (54%; p < 0.001).
Associations between measures of engagement, surgical cancellation and post-surgical outcomes from unadjusted logistic regression analyses can be found in Table 4. High engagement was associated with lower odds of surgery cancellation (OR = 0.18; 95% CI: 0.05, 0.61; overall p = 0.016), higher odds of discharge home (OR = 16.3; 95% CI: 4.05, 65.4; overall p < 0.001) and lower odds of inpatient readmission (OR = 0.10; 95% CI: 0.02, 0.64; overall p = 0.047) compared to patients with low engagement. There was no association between level of engagement and day of surgery cancellation, long LOS, ER visit or any revisit within 30 days. Per cent of prompts opened was associated with lower odds of surgery cancellation (OR = 0.98; 95% CI: 0.96, 1.00; p = 0.01) and slightly higher odds of discharge home (OR = 1.04; 95% CI: 1.02, 1.05; p < 0.001). Per cent of prompts clicked was associated with lower odds of surgery cancellation (OR = 0.97; 95% CI: 0.95, 0.99; p = 0.001).
Unadjusted association between patient engagement and surgical cancellation and post-surgical outcomes among intervention participants by joint replaced (n = 474; n = 146 hip replacements, 133 completed surgeries; n = 328 knee replacements, 303 completed surgeries).
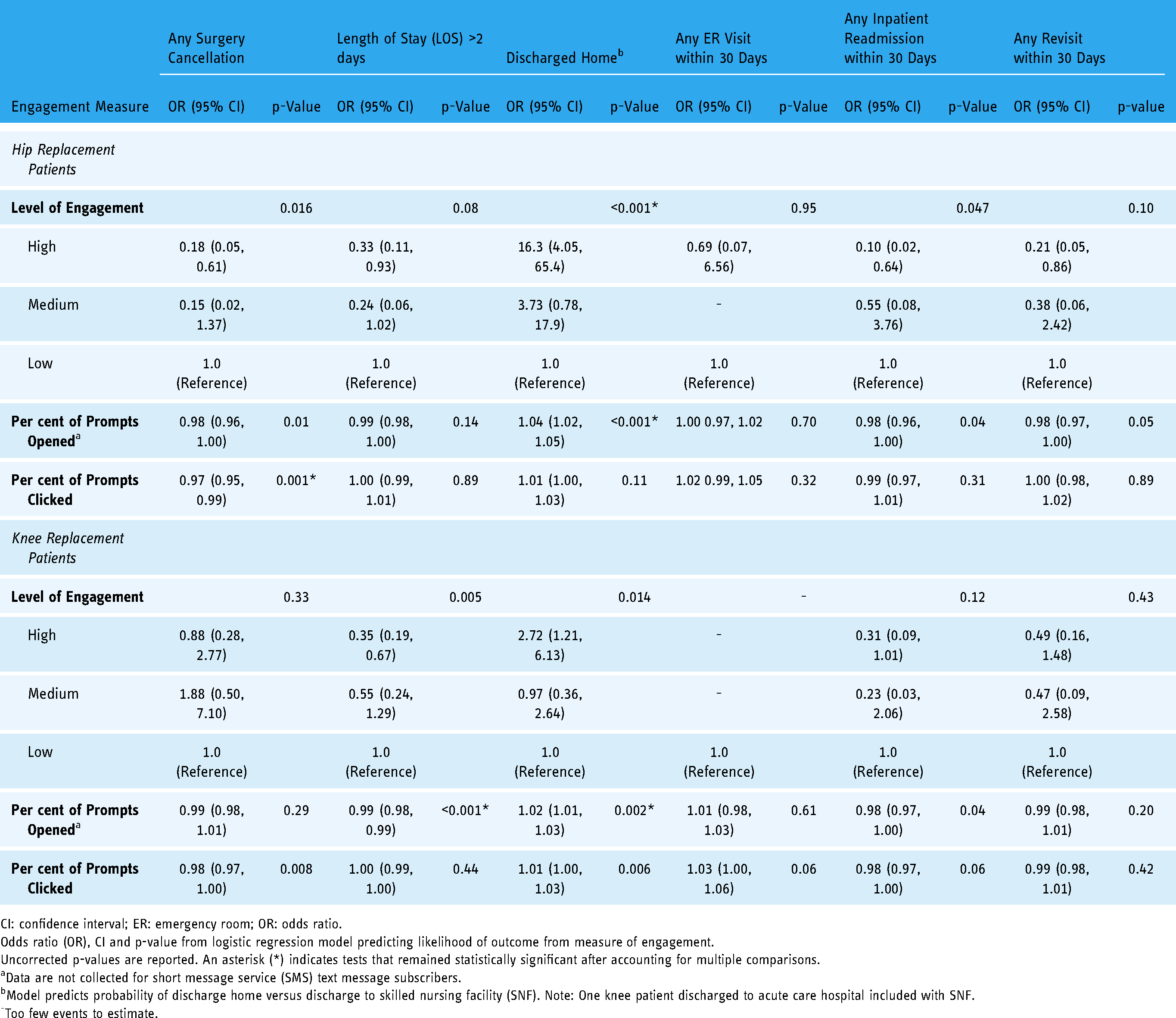
CI: confidence interval; ER: emergency room; OR: odds ratio.
Odds ratio (OR), CI and p-value from logistic regression model predicting likelihood of outcome from measure of engagement.
Uncorrected p-values are reported. An asterisk (*) indicates tests that remained statistically significant after accounting for multiple comparisons.
Data are not collected for short message service (SMS) text message subscribers.
Model predicts probability of discharge home versus discharge to skilled nursing facility (SNF). Note: One knee patient discharged to acute care hospital included with SNF.
Too few events to estimate.
Knee replacement patients
Demographic and clinical characteristics
Overall, 1307 scheduled knee replacement patients were included; 613 (47%) in the pre-intervention period and 694 (53%) in the post-intervention period. Demographic characteristics by time period can be found in Table 1. The periods were comparable in terms of gender and age distributions but differed significantly by age category and insurance (p = 0.02 and p < 0.001, respectively). Post-intervention patients were slightly older, more likely to have private insurance and less likely to have Medicare.
Surgical cancellation and post-surgical outcomes
Unadjusted comparison between pre- and post-intervention patients on surgery cancellation and post-surgical outcomes can be found in Table 2. Overall, 92 (7%) scheduled surgeries were cancelled, of which 35 (38%) were on the day of surgery. Post-intervention patients had more overall cancellations (5% pre vs. 9% post; p = 0.001) but fewer of the cancellations were on the day of surgery (71% pre vs. 23% post; p < 0.001). Post-intervention patients were less likely to stay longer than 2 days (44% pre vs. 37% post; p = 0.007), though average continuous LOS did not differ significantly (mean = 2.43 pre vs. 2.39 post; p = 0.34). There were no differences between the periods with respect to discharge disposition or destination, or revisits and readmissions.
Adjusted associations between intervention period and outcome measures adjusting for gender, age and insurance from logistic regression analysis can be found in Figure 3. Patients in the post-intervention period were more likely to have a cancelled surgery compared to pre-intervention patients (OR = 2.15; 95% CI: 1.35, 3.44; p = 0.001), but among cancellations (n = 92) post-intervention patients were less likely to cancel on the day of surgery (OR = 0.10; 95% CI: 0.03, 0.29; p < 0.001). Post-intervention patients were also less likely to stay longer than 2 days (OR = 0.74; 95% CI: 0.58, 0.94; p = 0.01). There were no differences between pre- and post-periods on discharge to home or readmissions and revisits.
Engagement and outcomes among the intervention participants
Forty-seven per cent of post-intervention knee patients (n = 328) participated in the intervention. Patients participating in the intervention did not differ from those who did not participate with respect to gender (p = 0.83), age category (p = 0.10) or insurance (p = 0.62).
On average, patients were enrolled in the intervention 25.9 (SD = 30.5) days prior to surgery (range: 208 days prior to 37 days after). Fifty-two (16%) patients were enrolled in the intervention on the day of surgery (n = 9) or after. Table 3 presents engagement and outcome measures among the intervention participants. Most patients received the prompts via email and the majority were highly engaged. An average of 65.9% (SD = 32.7) of prompts were opened and 51.0% (SD = 33.6%) were clicked.
Subscriber type (email vs. SMS text message) did not differ by age category (p = 0.99), gender (p = 0.81) or insurance (p = 0.95). Level of engagement did not differ by gender (p = 0.49) or insurance (p = 0.06), but did differ by age category (p = 0.01) with patients aged 65–79 years most likely to be highly engaged. There were no differences by gender (p = 0.19), age (p = 0.09) or insurance (p = 0.09) in per cent of prompts opened. Per cent of prompts clicked differed by age category (p = 0.03) and gender (p = 0.01), with no difference by insurance (p = 0.21). Patients 65–79 years old clicked the most prompts (mean = 53.8%, SD = 33.3), while patients 80 years or older clicked the least on average (mean = 35.5%, SD = 35.5). Females clicked on average 54.3% (SD = 34.1%) of the prompts compared to 44.7% (SD = 31.9%) for males. No differences were found in the time between enrollment and surgery by age (p = 0.94), gender (p = 0.57) or insurance type (p = 0.16). Enrollment on or after the day of surgery was not associated with gender (p = 0.20), age (p = 0.28) or insurance (p = 0.07).
Associations between measures of engagement, surgical cancellation and post-surgical outcomes from unadjusted logistic regression analyses can be found in Table 4. Patients who were highly engaged had lower odds of LOS longer than 2 days (OR = 0.35; 95% CI: 0.19, 0.67; p = 0.005) and higher odds of discharge home (OR = 2.72; 95% CI: 1.21; 6.13; p = 0.014) compared to patients with low engagement. There was no association between level of engagement and surgical cancellation or readmissions and revisits within 30 days. Opening a higher percentage of prompts was associated with lower odds of LOS longer than 2 days (OR = 0.99; 95% CI: 0.98, 0.99; p < 0.001), higher odds of discharge home (OR = 1.02; 95% CI: 1.01, 1.03; p = 0.002) and lower odds of inpatient readmission (OR = 0.98; 95% CI: 0.97, 1.00; p = 0.04). Clicking on a higher percentage of prompts was associated with lower odds of surgical cancellation (OR = 0.98; 95% CI: 0.97, 1.00; p = 0.008) and higher odds of discharge home (OR = 1.01; 95% CI: 1.00, 1.03; p = 0.006).
Discussion
We found that utilization of a digital health patient education and engagement tool prior to and following total joint replacement was associated with shorter LOS for both hip and knee patients and lower odds of ER revisits for hip patients. While there were more cancelled surgeries in the post-intervention period, there was a substantial reduction in the proportion of cancellations on the day of surgery for both hip and knee patients. These findings were robust even with non-participants included in the post-intervention group. Among patients who received the intervention, higher engagement was associated with improvements in surgical cancellation, LOS and discharge home.
Although patients in the post-intervention period had more overall cancellations, proportionally fewer were on the day of surgery, therefore impacting efficiency and revenue less than day-of cancellations.11,12 Prior to the intervention, nearly three-quarters of the cancellations were on the day of surgery, while post-intervention fewer than one-quarter were day-of cancellations. Importantly, we did not collect information on the specific reason for cancellation and whether it was patient-related (e.g. illness, decided to delay) or hospital or clinic-related (e.g. staffing, scheduling). We hypothesize that being more educated about the surgery and potential complications allowed patients to cancel earlier since they knew what to watch for but might have had more cancellations overall also due to better knowledge about good reasons to cancel, though we were unable to explore this in detail. Due to the potential for a secular trend in cancellation rates, we compared patients enrolled in the intervention to all other patients (including post-intervention patients who were not enrolled and all pre-intervention patients) in an adjusted model that also accounted for year. We found a strong effect of year with scheduled surgeries in 2018 over 2.5 times the odds of cancellation compared to 2017 for both hip and knee patients (OR = 2.84; 95% CI: 1.48, 5.44; p = 0.002; and OR = 2.51; 95% CI: 1.51, 4.20; p = <0.001; respectively). These findings indicate the increase in overall cancellations was likely due to an overall trend and unrelated to the intervention.
Prior studies have demonstrated that shortened LOS and shifting discharges from SNFs to home can be accomplished without impacting readmissions while potentially saving thousands of dollars per total joint patient.6,7 Similar to findings by others, we found shorter LOS and more frequent home discharges in the post-intervention period did not have a negative impact on revisits.7,9,21 As the most common inpatient adult surgical procedure, improvements in total joint replacement has the potential to save the healthcare system millions of dollars per year, in particular Medicare, as one of the largest joint replacement payors in the United States.3,5 Recent advances in total joint replacement have allowed for outpatient surgery, which presents another opportunity for cost savings and improved outcomes, although adequate patient selection and preoperative education and preparedness may be even more important for these patients. 27 In this study, all patients included were inpatient; however, the engagement tool has been adopted for outpatient surgeries in other facilities as practices shift towards more ambulatory surgery, particularly for younger, medically suitable patients. Application of our engagement tool in an ambulatory surgery setting is an important area of future study.
In the post-intervention period, 70% of patients who participated were highly engaged, opening more than half of the prompts, while few patients had low engagement. Higher engagement was associated with even greater improvement in surgical cancellation, LOS, discharge home and revisits. We did not measure patient activation directly, but these findings may indicate that the tool had an impact on patient activation, which we hypothesize was due to keeping patients better informed leading up to surgery along with setting expectations about post-operative recovery, thereby making them better prepared. These findings are similar to others demonstrating the positive impact of patient education and activation to improve outcomes and post-operative utilization.7,13,14,18–21
Though patient perception or acceptability of the tool was not assessed, we found no difference in demographic factors between patients who opted to participate in the intervention compared to those who did not. In addition, level of engagement with the intervention did not differ by gender and insurance. Interestingly, patients aged 65–79 years old had the highest level of engagement, while younger patients had the lowest engagement. These findings suggest the tool was generally acceptable across a range of demographics, including older adults who may be less receptive to digital tools. Relative to other tools which are often fraught with barriers to access,22,24,25 our tool was designed to be easy to access, use and understand. User perception and experience are important areas of future study to identify opportunities to further improve the usability and content of this digital health engagement tool.
Limitations
This study has several limitations. First, patients at this health system may not be generalizable to total joint replacement patients at other institutions given the tertiary care setting. Future work should examine the tool across a variety of settings and patient populations to ensure validity and generalizability of our findings. Second, the ideal methodology would have been a randomized trial of the intervention; however, that was not feasible. Therefore, we used a quasi-experimental intent-to-treat design and compared patients undergoing joint replacement surgery during the intervention period to those 1 year prior during the same time of the year to account for potential seasonal differences. Although slightly less than half (46%) of the post-intervention patients were actually enrolled to receive the intervention messaging (due to lack of an email or text-ready mobile number in the patient record), we still found significant improvements in a number of outcomes. Additionally, this study relied on administrative data and no additional information was collected, including demographic or socioeconomic factors (e.g. race or ethnicity, income, living situation, marital status), timing of surgery (i.e. month) or comorbidities that may contribute to surgical cancellation or post-surgical outcomes. As discussed above, we did not formally measure patient activation, patient perception or user experience with the tool, though our findings indicated the majority of patients who used the tool were highly engaged, which may be a useful proxy for both activation and acceptability. We hope to directly assess user experience and acceptability across a diverse patient population in the future.
To the best of our knowledge, there were no other ongoing improvement initiatives during the study time periods that would have impacted the results. As a sensitivity analysis, we compared patients enrolled in the intervention to non-enrollees in the post-intervention period only to eliminate the potential effect of any secular trends or other improvement efforts. These analyses indicated no difference in surgical cancellations for either hip or knee patients (p = 0.30 and p = 0.21, respectively) and a significantly shorter LOS in knee patients participating in the intervention (β = −0.16; 95% CI: −0.28, −0.03; p = 0.01).
Conclusions
Our findings suggest that the use of a similarly designed patient engagement tool could be helpful in improving hospital efficiency and patient outcomes for total joint replacement by reducing day-of cancellations, shortening LOS and increasing discharge home by better preparing patients for surgery. The readily scalable digital engagement tool used in this study could be easily adopted and educational messaging tailored for specific patient populations (e.g. those at higher risk for complications). It could also be adapted for other surgical procedures, including those in an ambulatory setting, or for chronic disease management (e.g. COPD, heart disease or diabetes). In the future, we aim to study the impact of the patient engagement tool across a variety of settings and in a randomized, controlled clinical trial versus the standard of care for total joint replacement.
Footnotes
Acknowledgements
The authors would like to thank Leonard A. Rappaport, MD, MS, Chief Emeritus, Division of Developmental Medicine, and Mary Deming Scott Professor of Pediatrics at Harvard Medical School, for his guidance and assistance with this research and the write up of the study findings.
Contributorship
BW conceived the study, and along with TAS identified the key metrics to be evaluated. BW, BL and CEM completed the literature review. BL oversaw the development of the intervention tool, with input from BW and TAS; and with TAS, coordinated the synthesis of the patients’ engagement data with their outcomes data, as well as doing final edits on the manuscript. TAS directed the implementation of the study intervention in the healthcare system, including getting Joint Council approval, establishing the technical interface between HIT systems and overseeing the integration of the patient outcome data with the engagement data. LB provided input on key metrics, reviewed data and provided input on the study's context and presentation. CEM conducted the statistical analysis, created the data tables and wrote the initial draft of the study manuscript. CEM and BL revised the manuscript in response to reviewers’ comments. All authors reviewed and edited the manuscript and approved its final version.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: BW and BL are employees of TPR Media LLC (d.b.a. UbiCare), the company that created the digital patient intervention tool used in this study.
Ethical Approval
This quasi-experimental, intent-to-treat study was not subject to IRB approval. There was no intervention in patients’ care and no requirement for patient consent. Relevant engagement and de-identified outcome data was collected and reviewed retrospectively. The project and study method was reviewed and approved by the hospital system's orthopedic Joint Council.
Funding
The study was funded by the healthcare system, which licensed the digital patient intervention tool and put staff time toward its technical implementation and toward data collection; and by UbiCare, which provided additional data compilation and statistical analysis services.
Guarantor
CEM.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.