
Abstract
Background
Poor adherence to anti-hypertensive medications leads to poorly controlled blood pressure which is associated with worse cardiovascular outcomes. Emerging technologies may be utilised advantageously in interventions to improve adherence and reduce morbidity and mortality from poorly controlled hypertension.
Objective
To determine the efficacy of technology-based interventions in improving adherence to antihypertensive medications.
Methods
PubMed and EMBASE databases were searched using keywords and MeSH terms. Included studies met the following criteria: randomized controlled trial (RCT); adults ≥ 18 years old taking anti-hypertensives; intervention delivered by or accessed using a technological device or process; intervention designed to improve adherence.
Results
12 papers met inclusion criteria for the current review: 5 studies significantly improved adherence when compared to usual care; of these 5 studies, 2 had corresponding significant improvement in blood pressure. Successful interventions were: electronic medication bottle cap with audio-visual reminder; short message service (SMS) containing educational information (2 studies); reporting of self-measured blood pressure to a telephone-linked computer system; sending a video of every drug ingestion to obtain monetary rewards.
Conclusion
RCTs on technological interventions to improve adherence and those showing significant effect are rare. Some of the interventions show potential to be applied to other populations, especially if targeted at patients with poor adherence at baseline.
INTRODUCTION
Hypertension is the leading preventable risk factor for premature death and disability worldwide, and results in cardiovascular disease and chronic kidney disease. 1 Globally, 31.1% of the adult population had hypertension. 2 Adherence to long-term therapy for chronic diseases averaged more than 50% and poor adherence has been identified as the main cause of failure to control hypertension; improving adherence may result in a reduction of morbidity from poor blood pressure control and hence reduction of healthcare costs. 3
A review by Cochrane in 2014 showed that current methods to improve medication adherence for chronic health problems are mostly complex and not very effective. 4 There are emerging technologies to improve medication adherence such as pharmaceutical database technologies and automated alerts; telemonitoring systems for medication-related self-management, and combination in-person and electronic technology interventions. 5 Electronic systems might inexpensively remind patients and providers about refills. Interactive electronic systems may be used to educate patients about appropriate medication use, and widespread online connectivity should accommodate more sophisticated monitoring, interaction and communication.
Literature review done for technology-based interventions to improve adherence to anti-hypertensive medications (AHM) are rare. At a time when technology plays an important role in every industry as well as in our personal lives, it is appropriate to conduct such a review. The goals are to assess the state of evidence in this field, identify interventions that were successful, and ascertain specific features of interventions that seemed to be most associated with success.
METHODS
Literature review
A search of peer-reviewed journals between 1966 and Dec 2017 was performed using PubMed and EMBASE.
The search terms related to the type of study (ie, randomised OR randomized); adherence (ie, adherence OR compliance); prescription drugs (ie, antihypertensive OR drug OR medication OR agent OR therapy); and medical condition of interest (ie, hypertension). Articles with at least 1 search term in 4 of these main categories (study type AND adherence AND drug AND disease) met the criteria for review. Hand searches of the references of retrieved full text articles supplemented this search.
Search terms and parameters were adjusted for both databases (PubMed and EMBASE) while maintaining a common overall architecture. Search results were then screened for duplicate entries, which were then removed. The search strategies were illustrated in Figure 1.

Search strategies used in PubMed and EMBASE.
Study selection
Studies were included if: the population of interest was composed of adult subjects (aged ≥ 18 years) with essential hypertension; the interventions aimed to improve adherence to medications used for treatment of hypertension; these interventions were either delivered by or accessed using a technological device or process (such as computer or internet, smartphone, short message services (SMS), electronic devices); the intervention group was compared to either no intervention or usual care; a reported outcome (primary or secondary) was adherence to AHM; the type of evidence was limited to randomized controlled trials (RCT). Studies which were non-English, where subjects had secondary hypertension, or which did not define how medication adherence was measured were excluded. Figure 2 presents a flow diagram of the study selection process.

Flow diagram illustrating selection of studies.
Data extraction
Data concerning study design, setting, characteristics of population studied, number of participants, mean age of participants, characteristics of the intervention, methods used to measure medication adherence, medication adherence outcomes, and blood pressure outcomes were extracted. Confidence intervals and p values were reported where available. Means were reported with standard deviations and medians were reported with interquartile ranges where available.
The included RCTs covered a variety of interventions, which were divided into 4 categories: 1. reminder systems only; 2. systems to enhance patient-provider communication; 3. systems that enhance communication and provide a reminder function; 4. interactive systems. I selected these categories to assess how best to deliver interventions to patients. Category 1 featured studies using technology to deliver automated reminders to patients; category 2 had studies that used technology to improve and extend educational information or counselling from the provider to the patients, but without the ability for feedback and interaction; category 3 is a combination of categories 1 and 2; category 4 featured the use of technology to provide a means to allow interaction between patient and provider such that patients may submit additional feedback to the provider, who may then act specifically on the feedback provided.
The studies identified were too heterogeneous in terms of their outcome measures and intervention types to conduct a meta-analysis, so a narrative summary was performed.
Assessment of risk of bias
The risk of bias was assessed using the Cochrane Collaboration risk of bias tool, including the standard domains of random sequence generation, allocation concealment, selective outcome reporting, blinding, and incomplete outcome data.
RESULTS
Characteristics of selected studies
Twelve studies met the criteria for literature review (Table 1). 4 studies used reminder systems only; 3 studies examined the use of systems to enhance patient-provider communication; 1 study tested interventions that combined systems to enhance communication and those that provide reminders; the remaining 4 studies focused on interactive systems.
Characteristics of RCTs of technology-based interventions to improve adherence to anti-hypertensive medication.
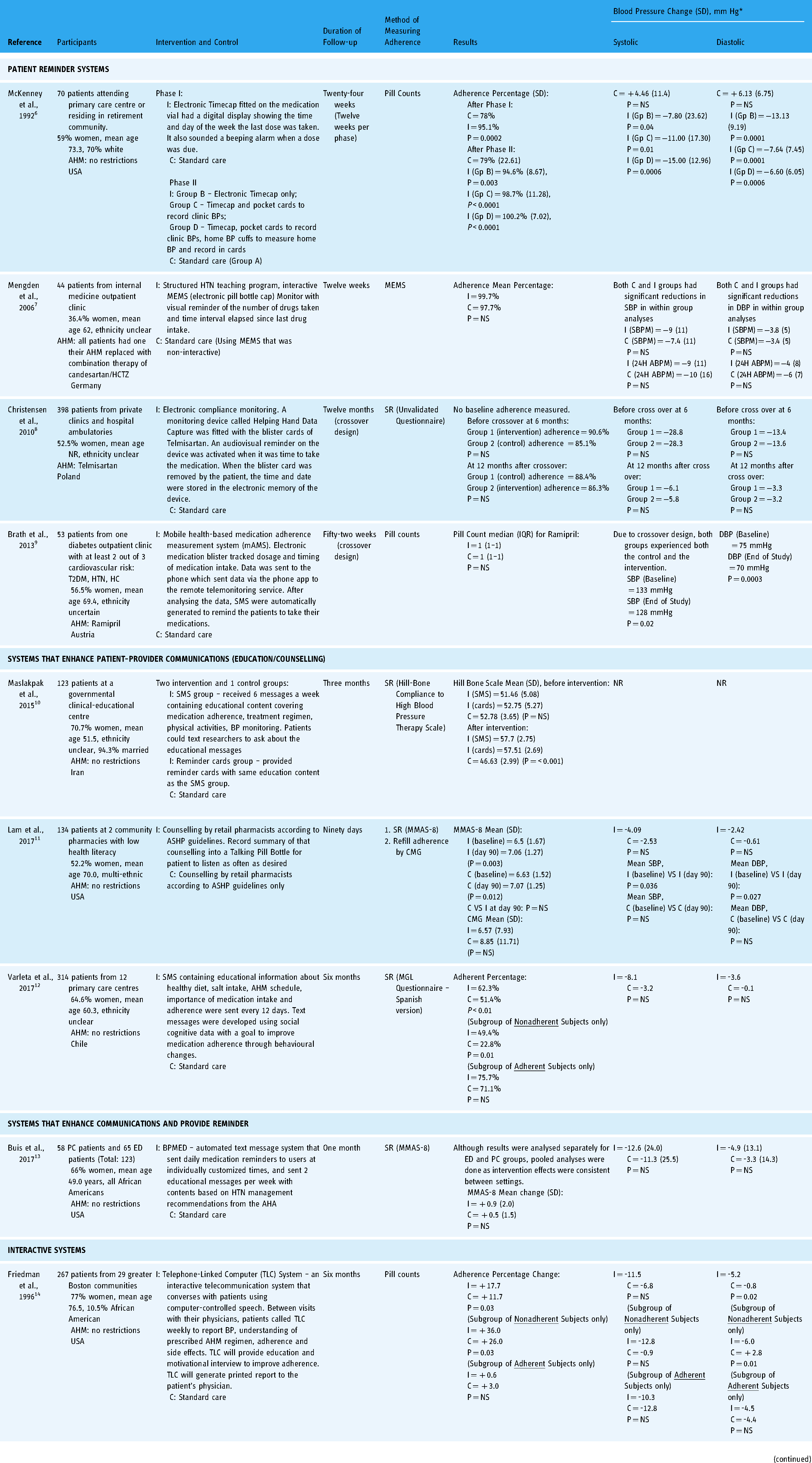
Abbreviation: AA, African American; ABPM, Automated Blood Pressure Monitoring; AHA, American Heart Association; AHM, Anti-Hypertensive Medication; ASHP, American Society of Health-System Pharmacists; C, Control; CMA, Continuous Medication Availability; CMG, Cumulative Medication Gap; DBP, Diastolic Blood Pressure; ED, Emergency Department; EMR, Electronic Medical Record; Gp, Group; HC. Hypercholesterolemia; HCTZ, Hydrochlorothiazide; HTN, Hypertension; I, Intervention; MEMS, Medication Event Monitoring System, MGL, Morisky-Green-Levine; MMAS-8, 8-item Morisky Medication Adherence Scale; NR, Not Reported; NS, Not Significant; PC, Primary Care; SBP, Systolic Blood Pressure; SBPM, Self Blood Pressure Monitoring; SD, Standard Deviation; SMS, Short Message Service; SR, Self-report; T2DM, Type 2 Diabetes; VS, Versus.
*Net blood pressure change from baseline to follow-up.
Seven studies used self-reported adherence such as the 8-item Morisky Medication Adherence Scale (MMAS-8) as an endpoint whereas 6 studies used pill count or pill cap monitoring such as the Medication Event Monitoring System (MEMS) to determine adherence.
Seven studies were conducted in North America, 3 in Europe, 1 in the Middle East, and 1 in South America. The sample sizes ranged from 29 to 398. All but 2 studies had women as the majority sex represented; and while ethnicity was unclear in 7 studies, 1 study had a sample of 100% African Americans, 1 study reported only 10.5% African Americans, and 2 studies had at least 70% European Americans. The mean age of patients in different studies ranged from 49 years to 76.5 years. 10 studies had at least 3 months for duration of follow-up including 3 that had 12 months of follow-up. All except 1 study reported blood pressure as one of the outcomes investigated.
Risk of bias
All studies had high risk for performance bias as patients cannot be blinded to the interventions and all studies were deemed low risk for reporting bias as there was no evidence that they tried to describe only outcomes with positive results or which favored the studied interventions. Selection bias was low for half the studies while the other half did not elaborate on either random sequence generation or allocation concealment. The majority of the studies did not describe blinding of the outcome assessors. Attrition bias was high in some studies which had a higher rate of drop out. There was a risk of referral bias in two studies because patients were referred by or recruited from 2 different methods or sources. Table 2 summarized risk of bias for the selected studies.
Quality assessment of included trials and potential sources of bias using cochrane risk of bias tool.

Abbreviation: ED, Emergency Department; NA, Not Applicable; PC, Primary Care.
Patient reminder systems
Of the 4 studies featuring reminder systems, only McKenney et al. had a significant favorable effect on both adherence and blood pressure outcomes. The other 3 did not demonstrate significant improvements in adherence and only 1 of them (Brath et al.) showed improvement in blood pressure.
In McKenney et al.'s study, those randomized to intervention arm used medication vials that were fitted with novel electronic caps – called the TimeCap – that displayed the time and day of the week when the cap was last open. An alarm sounded off from the TimeCap when a dose was due; if the alarm was ignored, the digital time face flashed to provide a visual reminder of a missed dose. There were 2 phases of 12 weeks. After phase 1, intervention arm had adherence of 95.1% versus 78% in the control arm (P = 0.0002). After phase 2, intervention arm had adherence of 94.6% versus 79% in the control arm (P = 0.003). After 24 weeks, systolic (SBP) and diastolic (DBP) blood pressures did not change significantly in the control arm; in the intervention arm both SBP and DBP improved significantly.
Mengden et al. studied patients with uncontrolled hypertension despite being on more than 2 AHM. 7 All patients had 1 AHM replaced by candesartan/hydrochlorothiazide (16/12.5 mg). Patients randomized to intervention arm received hypertension teaching and an interactive Medication Event Monitoring System (MEMS) cap affixed to the medication bottle. The MEMS cap was able to tell the number of drugs taken and the time elapsed since the last dose. Patients in the control arm had usual care as well as the use of the MEMS cap except that it was not interactive and had no visual reminder. Adherence was tracked by the MEMS cap. There was no significant difference in adherence levels by the end 12 weeks. SBP and DBP had significant reductions in within group analyses for both the control arm and intervention arm; however, when comparing the mean change in BP between control and intervention arms, there was no significant difference.
Christensen et al. designed a 12-month crossover study on patients taking telmisartan, randomized to either use an electronic monitoring device called the Helping Hand Data Capture (HHDC) or usual care without the use of HHDC. 8 Crossover occurred at 6 months. HHDC was operated with blister cards of telmisartan, so that it recorded the time of each blister removal; and an audio-visual reminder on the HHDC gave the time to take the next dose of medication. Baseline adherence was not measured at the start of the study. At time of crossover, adherence was not significantly different between the intervention arm and the control arm. At 12 months, adherence between both arms was also not significantly different. While patients had notable improvements in their BP by the end of the study (SBP was lowered by up to 34.1 mmHg and DBP up to 16.8 mmHg), improvements were not significant between the randomized groups.
Brath et al. recruited patients with at least 2 of 3 conditions (diabetes, hypertension or hypercholesterolemia). 9 They were randomized to use a mobile health-based medication adherence management system (mAMS) or usual care. mAMS made use of electronic medication blisters for the medications being studied; breaking the blister and ingesting the medication resulted in data on the dosage and timing of the medication-taking being sent to a remote telemonitoring service via the handphone app and aided by RFID technology. After analyzing the data, SMS reminders were sent to the patients to take their medication. When considering only patients with hypertension, adherence was not different between intervention and control arms. At the end of the crossover phase, BP improved significantly for both groups which underwent both intervention and control arms.
Systems that enhance patient-provider communications
Three studies tested interventions using technology to enhance communications in educating and counselling patients – of which 2 achieved some success in improving adherence.
Maslakpak et al. randomized patients into equal groups to receive educational SMS, reminder cards, or to just have usual care respectively. 10 The SMS group was sent 6 messages a week with content covering the domains of medication adherence, treatment regimen, physical activities and BP monitoring. The reminder cards group were trained in the usage of the cards which contained similar educational content as the SMS messages. At baseline, adherence was not significantly different between the 3 arms. At 3 months, adherence was significantly better for the intervention arms compared to the control arm. Blood pressure outcome was not reported.
Lam et al. subjected all patients to receive counselling from the pharmacists at point of dispensing. The intervention arm received an electronic device called Talking Pill Bottle (TPB) that recorded a summary of the same counselling that can be replayed by the patient multiple times. This was compared to usual care without TPB. Adherence was measured by the 8-item Morisky Medication Adherence Scale (MMAS-8). Within-group analyses at 90 days showed significant improvements in adherence within the intervention and control arms compared to baseline; but there was no difference in adherence level when comparing intervention arm to control arm. The situation was similar when comparing blood pressure outcomes – no difference was found in the DBP and SBP between intervention and control groups at the end of the study.
Varleta et al. randomized patients to receive or not receive SMS. 12 The text messages were developed by a multi-disciplinary team using social-cognitive theory data and contained educational information touching multiple domains such as healthy lifestyle and medication adherence; they were sent every 12 days over 6 months. Mean percentage of adherent patients was significantly higher in intervention arm versus the control arm. On subgroup analysis, the improvement was only found in patients who were non-adherent at baseline; adherent patients at baseline did not seem to benefit from the intervention. There was no significant difference in the change in SBP or DBP when comparing intervention arm to control arm.
Systems that both enhance communications and provide reminder
One study was identified in this category.
Buis et al. randomized patients with uncontrolled hypertension to receive text messages from an automated text message system called BPMED while the other arm received usual care. 13 BPMED sent 2 educational messages per week with content based on hypertension management recommendations from the American Heart Association; it also sent daily medication reminders customized to the patient's medication regimen. After 1 month, mean change in adherence was not significantly different in both arms. Mean changes in SBP and DBP were also not significantly different in both arms.
Interactive systems
These 4 studies, in general, described interventions that required substantial patient involvement and participation to interact with their providers with the aid of technology. 2 of the studies showed improvements in adherence and blood pressure outcomes.
Friedman et al. randomized patients with uncontrolled hypertension to usual care while the other arm had to call a Telephone-Linked Computer (TLC) every week to report their blood pressure taken at home for 6 months. 14 TLC group patients also had to report to TLC their anti-hypertensive regimen, adherence to their medication, and side effects to the AHM. TLC would, during the same call, provide education and motivational counselling. TLC spoke to patients using computer-controlled speech. At the end of the call, a report was generated, printed and given to the patient's physician. Mean percentage change in adherence at 6 months was significantly better in the intervention arm than in the control arm. Subgroup analyses showed that significant difference in change in adherence between groups only occurred in patients who were not adherent at baseline, but not in those who were. SBP change was not significantly different between arms; DBP change was significantly different between arms – this difference, again, was significant in patients who were not adherent at baseline but not in patients who were.
In Rinfret et al.'s study, patients on intervention accessed telephone-linked IT-supported management program weekly to report their home blood pressure and self-assessed adherence (validated self-report questionnaire). 15 The program merged these data with actual pharmacy refill data, and generated reports that were faxed monthly to physicians, pharmacists and study nurses. For patients with poor BP control, additional emails were sent to study nurses to inquire about their difficulties in BP control or adherence, and deal with them or refer to the pharmacist or doctor as specified by the study algorithm. At the end of one year, there was no significant difference in adherence between intervention and control arms. Despite that, change in SBP and DBP had significantly greater improvements for the intervention arm compared to control.
For 12 weeks, Petry et al. randomized patients to usual care and intervention which involved patients recording the taking of medications and sending the record to study personnel. If they were sent within 2 h of their actual dosing time, patients were rewarded with $0.50; bonuses can go up to $5 a day for a full day of adherence; missed or late sending incurred resetting of bonuses. Only during week 1, the research assistant phoned and reminded the patients who did not submit their recordings within one hour of dosing time. At week 12, adherence, was significantly greater in intervention arm than control arm. Both arms reported better SBP but the change in SBP was not significantly different between intervention arm and control arm. DBP was not reported.
Kim et al. conducted a 6-month study in which the control group received standard disease management program while the intervention group received wireless monitoring program on top of standard disease management program. 17 Patients in the intervention arm received an iPhone with the necessary apps and were enrolled in the HealthyCircles Platform – an online disease management program featuring educational materials and a dashboard to link with the patient's family, caregiver and healthcare professionals. Measurements of BP were made 3 times per week 2 measurements per day with the home BP device provided and readings were wirelessly uploaded to the HealthyCircles Platform. The patient's healthcare providers had access to the BP readings. The platform sent reminders to the patients if BP monitoring became less frequent; it also had information about disease condition and provided general health behavior recommendations. Adherence did not have significant improvements within the intervention arm or control arm. Changes in SBP and DBP were not significantly different between intervention arm and control arm.
DISCUSSION
This review identified 12 RCTs of technology-based interventions to improve AHM adherence. There was considerable variation in the types of interventions, with small numbers of studies grouped together. Overall, only 1 of 4 reminder-only interventions reported an improvement in adherence compared to control. Of the 3 studies that enhanced communications for counselling and education, 2 had good effect on improving adherence. The 1 study combining reminders and enhancing communication showed no effect on adherence. 2 of the 4 studies on interactive interventions succeeded in improving adherence.
The findings of this review suggest that the use of patient reminder system alone may not be useful in improving adherence. Only one study (Mckenney et al.) using electronic Timecap with visual display and audible alarm showed significant improvement; the other 3 studies using electronic pill cap with visual reminder (Mengden et al.), electronic blister pack with SMS reminder (Brath et al.), and blister pack device that provided audiovisual reminder (Christensen et al.) had no significant improvements. Buis et al.'s study, analyzed in the third category, used SMS reminders too but with no significant effect on adherence. Despite using audiovisual reminders, Mckenney et al.'s study was successful while Christensen et al.'s study was not. One possible reason could be the differences in the design of the device – such as the prominence of the display and the volume of the audio reminder – may play a role in the intervention's success. Also, adherence was measured by self-reported questionnaire in Christensen et al.'s study which may overestimate adherence. The effectiveness of the SMS reminders lies on the premise that patients actually read it at the time it is sent; should the mobile phone be away from the patient or put on silent mode, SMS reminders will lose their intended effect.
There are other reminder systems that have been used to target medication adherence in other studies. In a meta-analysis by Fenerty et al. on reminder systems for chronic diseases, 18 other interventions that had found success included the use of video-telephone call reminders and programmed electronic voice reminders. These have not been tried for adherence to AHM.
This review showed that technology-based interventions to educate or counsel patients can be promising. In contrasting fashion, an old Cochrane review done in 2004 19 on interventions to improve adherence to AHM showed that patient education and counselling using non-technology-based interventions were largely unsuccessful except for one study which, unlike the other 6, included studies which had only one interventional encounter, did follow-up group education sessions at 1, 3 and 5 months after enrolment. Perhaps the use of technology makes follow-up education sessions easier and more sustainable. Maslakpak et al. and Varleta et al. sent education SMS to their study subjects persistently and at regular intervals, and achieved positive effects on adherence. For Varleta et al.'s study, it is to be noted that SMS education intervention had the most effect on patients who were already non-adherent at baseline. Although Buis et al. employed the same SMS strategy to educate their patients, adherence did not improve; this may reflect the variation in the content and language style used in SMS messages. However, SMS has the advantages of being able to be sent to anywhere at any time, cheap and not data-intensive, customizable and modifiable in terms of content, and easily accessible and private as it is sent directly to the patient's personal mobile communication device. Lam et al.'s use of “Talking Pill Bottle” may have been unsuccessful since patients may not take the initiative to replay the counselling recorded by pharmacists.
The causes of AHM non-adherence are multifactorial. 20 Therefore, a multi-faceted approach may be needed to address poor AHM adherence. Systematic review of medication adherence in other chronic diseases such as diabetes mellitus also suggested that multifaceted interventions are more effective than single intervention in improving adherence. 21 In this review, technology-based systems appeared to be great facilitators to multi-faceted interventions. Interactive systems mandated the need for patients to take the first step to collect and send personal data. These data were then analyzed by the study coordinators or healthcare providers and a certain predetermined action was then carried out based on the result of the analysis. Technology certainly made this interaction more efficient with automated telephone responses, ability to send videos instantly miles apart, and dedicated smartphone apps. With reference to interventional tools to improve medication adherence, 22 Friedman et al. and Rinfret et al. touched on the domain of self-management by requiring their patients to monitor their own BP at home and reflect on their own level of medication adherence. Friedman et al.'s study succeeded in improving adherence while Rinfret et al.'s did not; this could be attributable to Friedman et al.'s impressive multi-tasking computer system that even delivered motivational interview; both studies generated reports to patients’ healthcare provider. In fact, Friedman et al. found that the interventions were the most effective in the subgroup of patients who were non-adherent at baseline.
Studies showed that financial incentive may be an effective intervention for encouraging healthy behavior change. 23 Akin to directly observed therapy (DOT) used to ensure drug ingestion in the treatment of tuberculosis, 24 Petry et al. cleverly got patients to send videos of medication ingestion to the study coordinator and rewarded them financially for good adherence, resulting in significant improvement in adherence. This can be seen as a form of behavioral intervention with patients associating good adherence with a positive experience of receiving monetary rewards. However, using financial incentives in this aspect may lead to moral concerns and unintended consequences 25 because they hold potential to be applied unfairly and encourage people with good adherence to have poor adherence just so they can be enrolled to this program. Using such intervention to “jumpstart” optimal decisions and create an ingrained behavior pattern of adherence at the beginning only could reduce ethical and practical concerns. Kim et al. was the only study among the 12 to use a phone app to aid adherence; again, his study entailed the need for patients to report self-measured BP. However, no impact on adherence was found.
Comparing results between studies is difficult because there is a great variety of interventions; studies often use multi-faceted approaches; and do not use the same method to measure adherence. Just looking at self-report adherence scales that were validated, at least 43 of them were uncovered by a review by Nguyen et al. 26 Unfortunately, self-reported adherence may lead to inaccurate estimates with internal validities (Cronbach's alpha) ranging from 0.61 to 0.91 and specificity generally below 75%. Other methods listed by Gupta et al. included indirect methods such as pill counting, electronic monitoring devices, review of pharmacy database records, and direct methods such as DOT, digital pills and biochemical detection of medications in urine or blood. 27 8 methods to measure adherence were found in the 12 cases reviewed.
Of the 5 studies showing effectiveness of their intervention for adherence, only 1 study (Mckenney et al.) had significant improvement in both SBP and DBP; Friedman et al.'s study had significant improvement in DBP but not SBP. Previous literature showed that good adherence was associated with better BP control and reduction of cardiovascular outcomes. A retrospective population-based study showed that patients with high adherence were 1.45 times (P = 0.026) more likely to be associated with good BP control; 28 using urine analysis to detect non-adherence to AHM, the group with inadequate blood pressure control had the highest prevalence (28.8%) of patients with total or partial non-adherence. 29 In a retrospective cohort study in Korea, patients with poor adherence to AHM were significantly more likely to suffer all-cause mortality, acute myocardial infarction, ischemic heart disease and stroke compared to those with good adherence. 30
Strengths and weaknesses of this review
The search was done on 2 of the largest databases, PubMed and EMBASE. A wide search strategy was cast using MeSH terms and keywords to reduce the chance of missing relevant articles. The selection of articles was done by one person.
The definition of technology-based intervention was liberal, and the review included interventions with any electronic components. Despite that, only 12 studies were found using technology-based interventions to improve adherence. Limiting to only RCT designs allowed the presentation of more robust evidence.
Most of the studies had small sample sizes with only 6 of them exceeding 100 patients. Only 3 studies (Maslakpak et al., Lam et al., Varleta et al.) were found to have described the calculation of their sample sizes.
Comparison of the outcomes between the studies was challenging because the interventions, the measurements of adherence and the durations of follow-up had not much consistency. The patient populations were also highly variable and conclusions from them may not be applicable to the local population of interest
CONCLUSIONS
Although there is a paucity of evidence arguing for technology use in improving adherence, some of the interventions reported here have the potential to be used again in other populations, especially if the interventions are targeted at a specific group of patients with higher risk of poor adherence. As such, it may be more efficacious to find out the factors associated with patients with poor adherence and study the effect of interventions on these patients.
In the future, lead investigators should try to improve on those technology-based interventions found in these 12 studies, mix in artificial intelligence and the use of phone apps, and continue to use it to help remind medication ingestion, counsel and educate patients about hypertension and medication adherence, and create opportunities for the provider and patient to interact. There is also a need to ensure the calculation of appropriate sample size, a longer duration of follow-up, objective measurement of adherence and proper reporting of the blood pressure outcomes.
Of course, objective measures of the cost of using technology-based interventions should be done too. Sending out SMS as reminders or for education purposes does not seem expensive but creating a phone app or employing staff to review data sent by the patients require substantial investment. Cost-effectiveness can vary greatly between interventions, and it is a very important consideration in any budget-conscious healthcare system.
Footnotes
Acknowledgements
The author would like to thank Dr CS Lee of SingHealth Polyclinics for proof-reading the manuscript.
Contributions
GCY Kang researched literature, conceived the study, analysed the data, wrote the first draft of the manuscript, reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not required for the review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
GCY Kang.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.